
Abstract
Background:
Worldwide, there is an increase in the incidence of suicide each year. Suicide attempts are estimated to be more frequent than actual suicide mortality. One potential contributor to suicide risk is the presence of sensory impairments (visual or hearing impairments). The present review aimed to assess the direction and strength of the association between visual impairment (VI) and the risk of suicidal behavior.
Methods:
A systematic search was carried out on the literature published up to July 2021 in PubMed, Embase, Cochrane Library, and clinicaltrials.gov. The association between VI and suicidal ideation/attempt was summarized by pooled odds ratio with 95% CI.
Results:
Six studies with a sample size of 1,64,752 were included in the final quantitative synthesis. The pooled odds ratios (95% CI) for suicidal ideation and attempt among persons with VI were 1.53 (1.30–1.79) and 4.55 (2.39–8.67), respectively. On subgroup analysis, the odds of suicidal ideation were higher in persons with additional sensory impairment, 2.07 (1.21–3.53), than in the group with VI only, 1.63 (95% 1.34–1.98).
Conclusion:
This study found a significant association between suicidal behavior and VI, more so in persons with dual impairment. Structured assessment for psychological health and appropriate management should be an integral part of managing people with visual and other sensory impairments, to prevent this serious adverse consequence.
Visual impairment (VI) is a condition of reduced visual performance that cannot be remedied by refractive correction (spectacles or contact lenses), surgery, or medical methods. 1 In general, sensory impairment leads to poorer mental health and reduced quality of life. 2 World Health Organization (WHO) estimated that globally at least 2.2 billion people have an impairment in near or distance vision. 3 More than 90% of individuals with VI live in developing countries, and this geographical disparity may be attributed to a higher prevalence of conditions related to poverty or environmental conditions and poor access to health care services. 4 It has been well documented that vision loss may result in varying degrees of psychic suffering, which is greater than the distress resulting from other forms of sensory impairment, irrespective of age. 5 The association between VI and depression has been investigated by several studies, and the majority of these studies found a significant association between VI and depression.6–8 In some cases, this is complicated to the point of precipitating suicide.
Suicide is one of the major causes of premature and preventable mortality globally.9,10 The causes of suicide are multifactorial and inadequately understood. Risk factors such as social deprivation, physical and mental illness, and financial and social factors alone or in combination may contribute to a variable extent. 11 A link exists between suicide ideation (SI) and behaviors leading to suicide attempts. 12 Therefore, it is crucial to understand the risk of SI among people with VI. Many studies have attempted to evaluate the relationship of visual and other impairments to quality of life as measured on scales of depression and life satisfaction.12–14 Although a substantial number of studies have been done on the risk of suicidal behavior among sensory impaired people, data are less consistent regarding their association.
Given the global prevalence of VI, determining whether it is linked to an elevated risk of SI and suicide attempts is critical public health research that could improve suicide prevention strategies. We conducted a systematic review and meta-analysis of studies focusing on VI and suicidal behavior. We aimed to clarify the direction and strength of the association and potential sources of heterogeneity between studies. Concurrently, we also attempted to understand the other potential influencing factors through subgroup analyses by age and type of sensory impairment.
Material and Methods
Design and Registration
We followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) checklist for reporting systematic reviews incorporating meta-analyses for reporting our review. We have also registered our study protocol on the “International Prospective Register of Systematic Reviews” and the registration number for the study is CRD42021268087.
Search Strategy
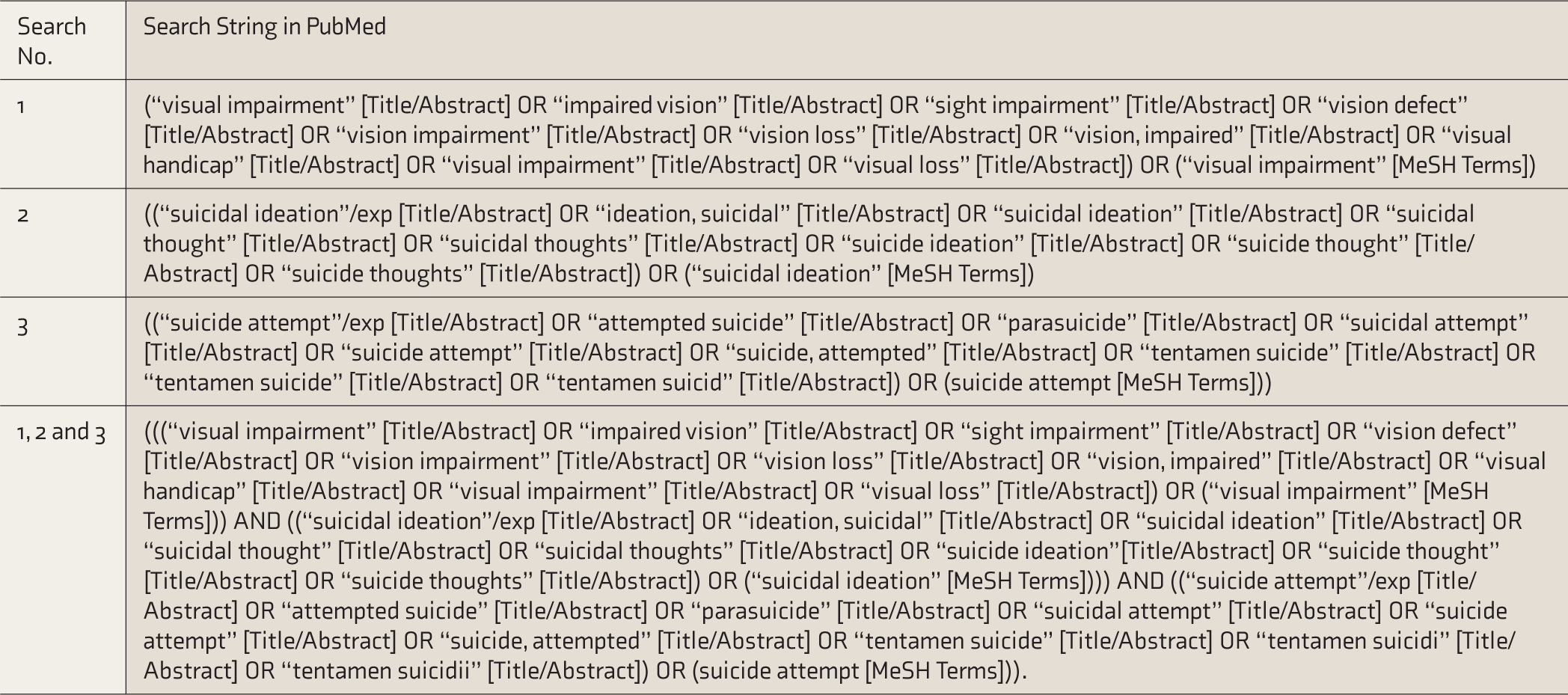
A systematic search was carried out on the literature published up to July 2021 in PubMed, Embase, Cochrane Library, and clinicaltrials.gov. We included only English-language studies published in peer-reviewed academic journals. In the first step, free text searching of keywords of population, intervention, control, and outcome (PICO) components of the research question was performed. All possible synonyms were included in the free text search. Database-specific subject headings (MesH, Emtree, etc.) were also included in the search. The detailed search strategy was constructed using appropriate Boolean operators, search field tags and punctuations, and other advanced features specific to each database (Table 1). Appropriate filters were used to make the search strategy further specific. In addition to the electronic searches, a manual search was also performed on the reference lists of the included articles, systematic reviews, and related literature. Finally, all included articles were retrieved from each database and imported into reference management software.
Search Strategy
Inclusion Criteria
Primary studies that evaluated SI/attempts in adolescent or adult samples (>12 years of age) with any type of VI (loss of peripheral vision, blurred vision, generalized haze, extreme light sensitivity, glaucoma, low visual acuity, night blindness, blindness, or legal blindness) were included. Studies in persons with additional sensory impairment were also included. All types of observational (cross-sectional, cohort, and case-control) and experimental studies, including randomized controlled trials (RCTs), were included. Only English language studies published until July 2021 were included. Studies on persons with additional physical impairments or preexisting psychiatric disorders, on children <12 years of age, or focusing on VI occurring after a suicidal attempt were excluded.
Study Selection and Data Extraction
Results of the electronic and manual searches were assessed based on the above inclusion/exclusion criteria. After removing duplicates, articles were included or excluded at different levels, starting at the level of title and abstract screening, followed by full-article screening. Two reviewers were involved in each process, and disagreement between them over the eligibility of a particular study was resolved through discussion with a third reviewer. These screening and selection processes were represented in a preferred reporting items for systematic reviews and meta-analyses flowchart. The reviewers independently extracted and plotted the data for each included article (two reviewers per article), based on the data extraction template from Cochrane Consumers and Communication Review Group. 15 Data on demography, study characteristics (first author, publication year, country of origin, and sample size), type of VI (and other sensory impairment), proportion of SI/attempts, tools used to measure VI and SI, proportion of death, measure of association (odds ratio [OR]), and mortality hazard ratio were extracted. Entered data were double-checked by second reviewer for correctness of the entry.
Risk of Bias (Quality) Assessment
The methodological quality of the included studies was assessed for all individual elements of the study, including the selection of participants, outcome assessment, adequacy of follow-up, and completeness of the data. The quality of evidence was evaluated in accordance with the Newcastle-Ottawa Scale (NOS). 16 The quality of the studies was then scored on the scale, from “lowest” to “highest” possible quality, where the highest quality is considered the strongest possible level of proof for an association.
Data Synthesis and Subgroups Analysis
In accordance with the statistical guidelines recommended in the latest version of the Cochrane Handbook for Systematic Reviews of Interventions, 17 statistical software R was used to calculate the combined outcome effect. 18 The association between VI and SI/attempt was summarized by pooled OR with 95% CI for dichotomous outcomes and represented as a forest plot. Evidence of between-study variance because of heterogeneity was assessed through the following methods: chi-square test for heterogeneity and I2 statistics to quantify the inconsistency. I2 < 25%, 25% to 75%, and > 75% are considered mild, moderate, and substantial heterogeneity, respectively. Subgroup analysis was performed based on co-exposures (other sensory impairments), to investigate sources of heterogeneity. We performed a sensitivity analysis to check the consistency of the pooled estimates.
Results
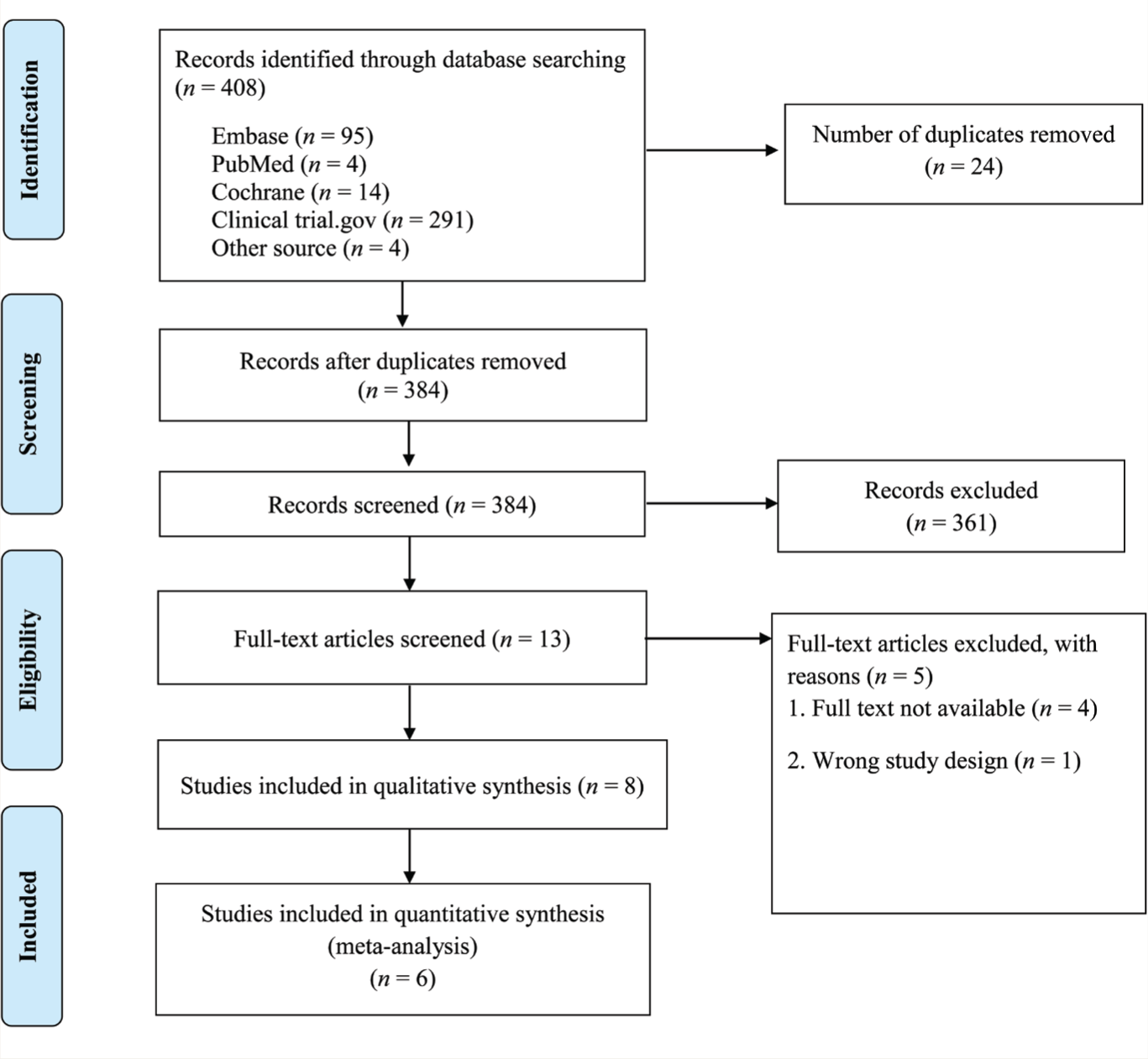
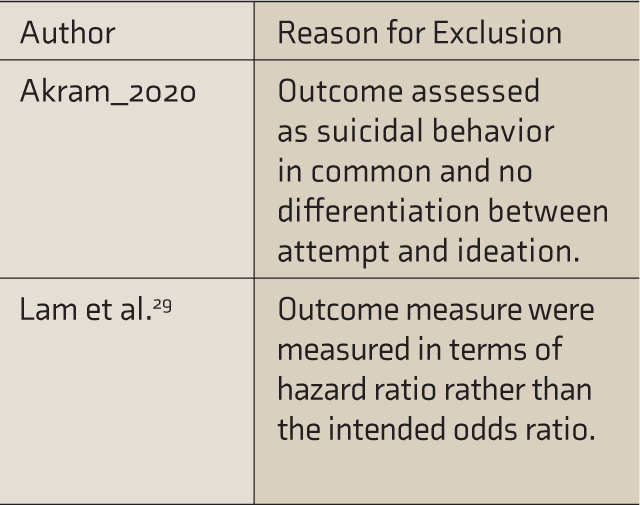
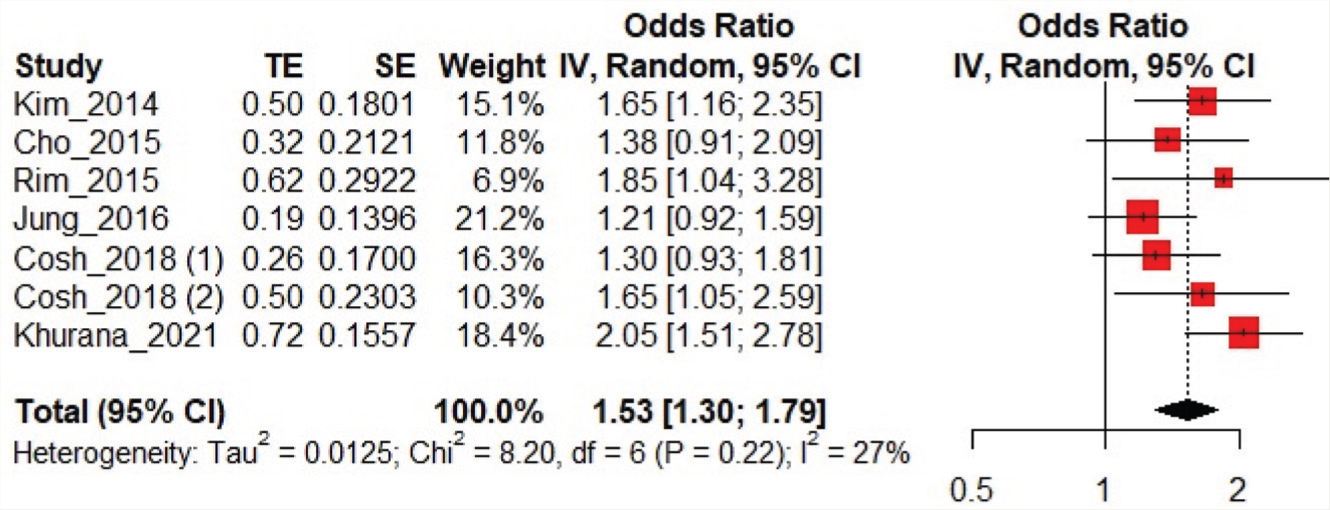
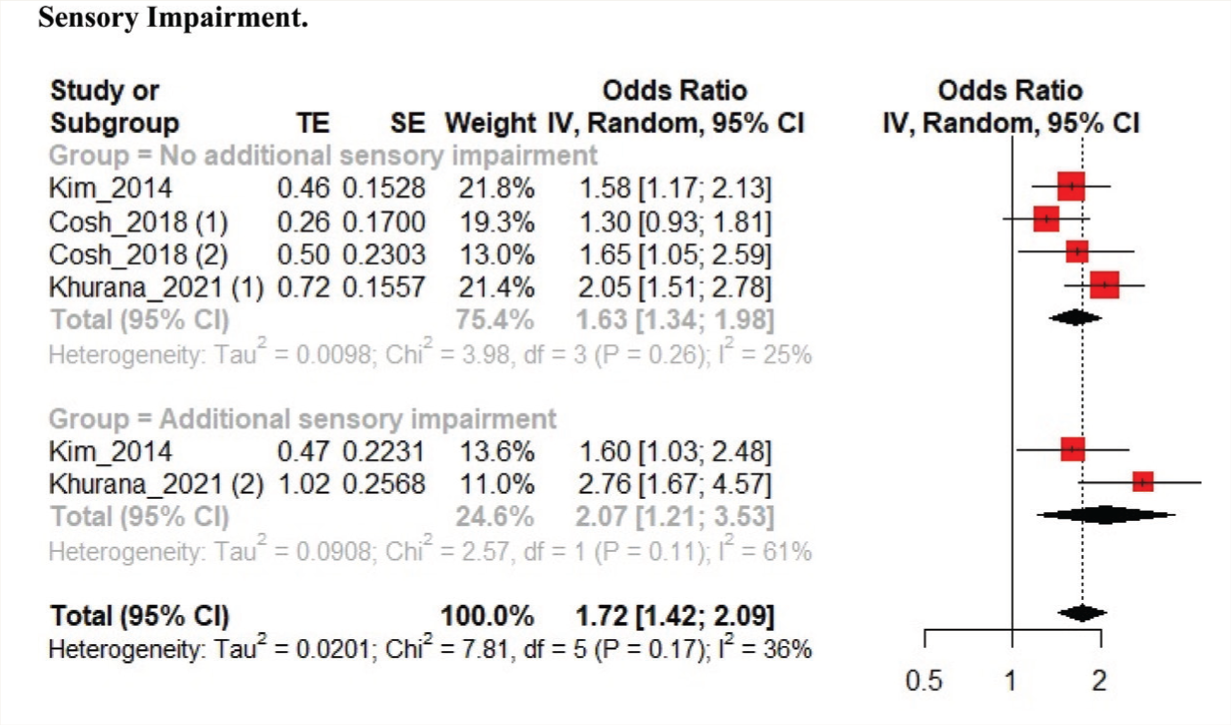
Eight studies were included in the qualitative synthesis, out of which six were included in the meta-analysis (Figure 1, Table 2).12,19–23 The two studies not included in the quantitative synthesis are described separately in the exclusion table (Table 3). Four studies were from Korea, and the other two were from UK and France. Association between SI and VI was reported by six studies, and the pooled sample size was 81,171. The pooled OR (95% CI) for SI was 1.53 (1.30–1.79). Moderate heterogeneity was found among the studies (I2 heterogeneity 27%, P = 0.22; Figure 2). We performed subgroup analysis based on the presence of additional sensory impairment (VI only: three studies; with additional sensory impairment: two studies). The odds of SI were higher in the group with additional sensory impairment 2.07 (1.21–3.53) than in the group with only VI 1.63 (1.34–1.98, Figure 3).
PRISMA Flow Diagram
Inclusion Table
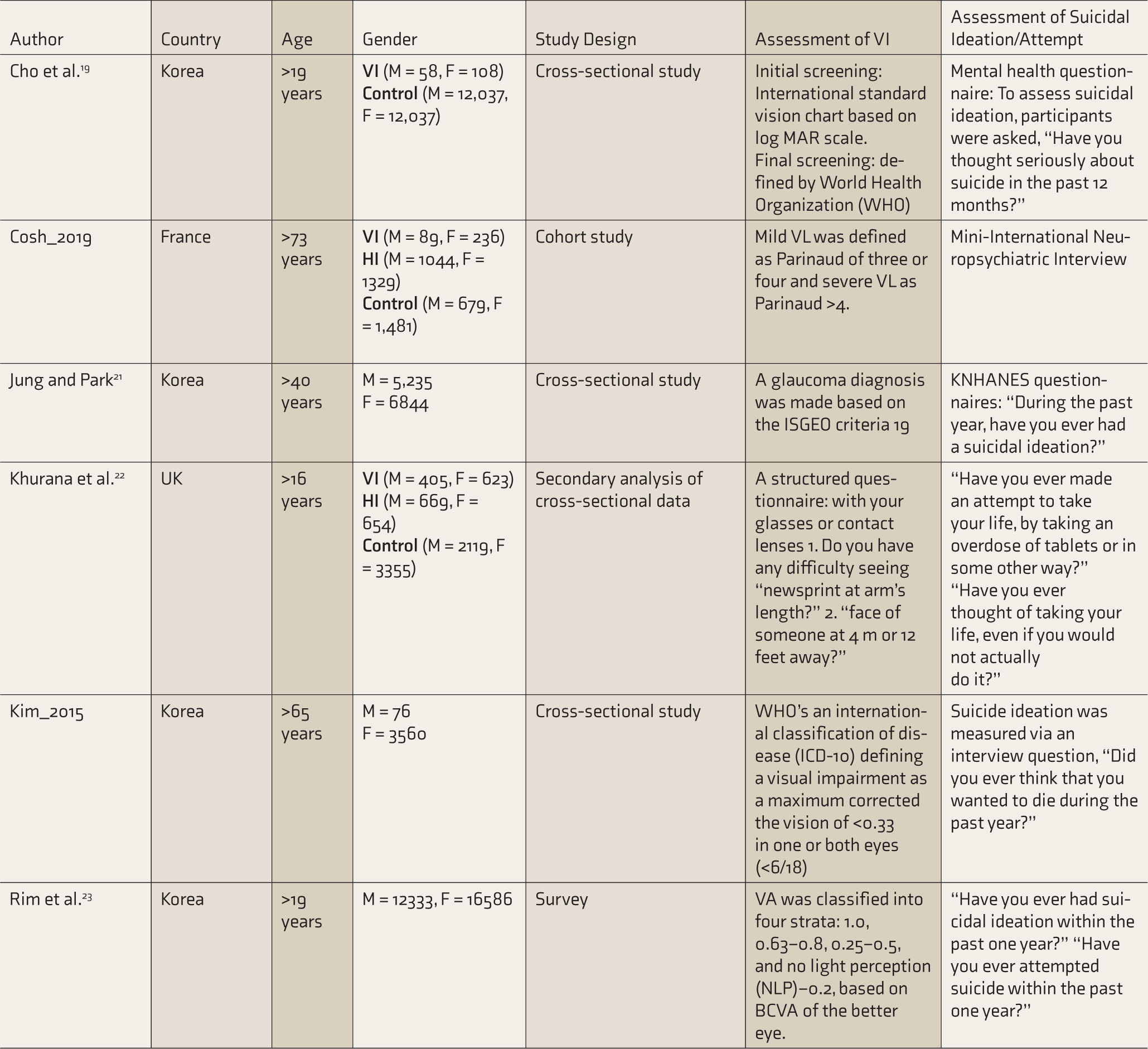
M, male; F, female; VI, visual impairment; VL, vision loss; VA, visual acuity; HI, hearing impairment; logMAR, logarithm of the minimum angle of resolution; KNHANES, Korea national health and nutrition examination survey; BCVA, best corrected visual acuity.
Exclusion Table
Forest Plot of the Association Between Suicidal Ideation and Visual Impairment
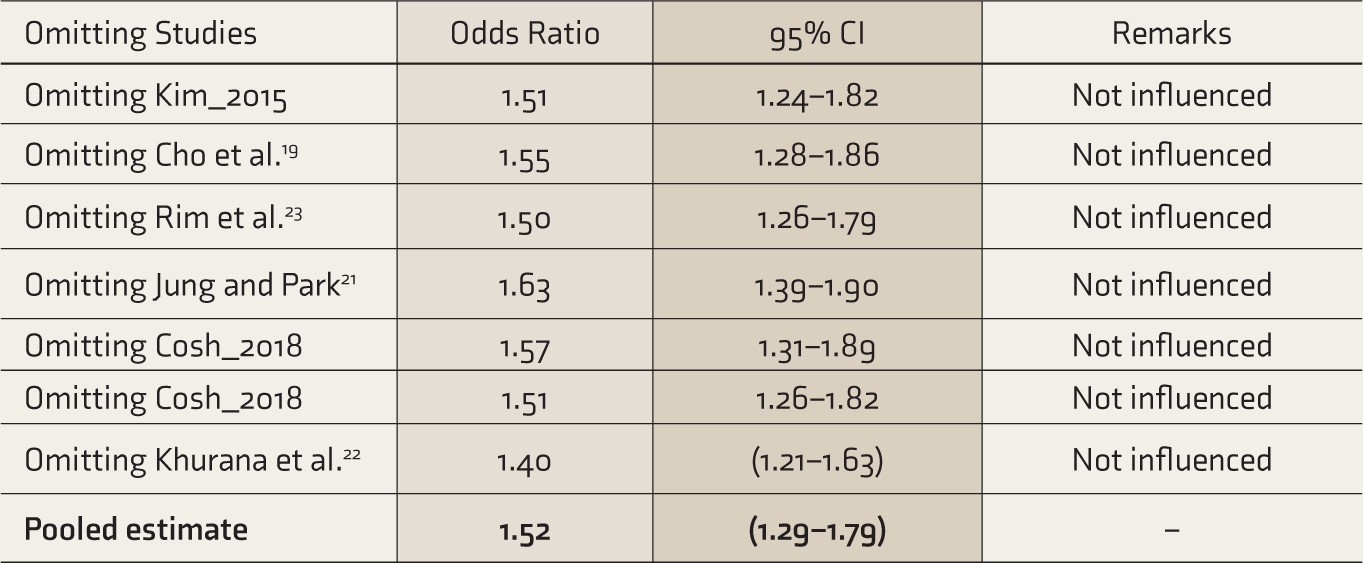
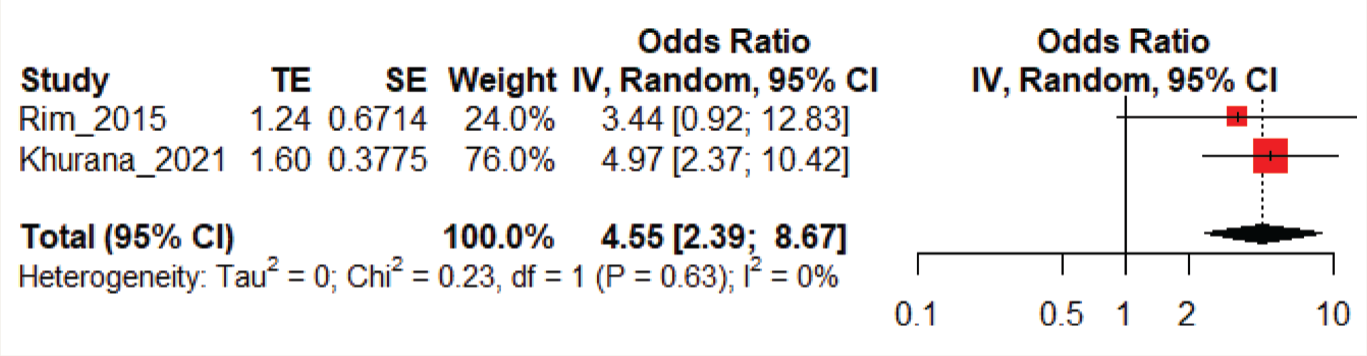
Association between suicidal attempts and VI was reported by two studies with a pooled sample size of 31,270. The pooled OR was 4.55 (2.39–8.67). No heterogeneity was found among the studies (I2 heterogeneity: 0%, P: 0.63; Figure 4). While performing sensitivity analysis, by omitting the Khurana et al. study, the pooled OR was 1.40 (1.21–1.63), and by omitting the Jung and Park study, the pooled OR was 1.63 (1.39–1.90; Table 4).
Sensitivity Analysis of the Association Between Suicidal Ideation and Visual Impairment
Forest Plot of Suicidal Ideation Between Groups with and Without Additional Sensory Impairment
Forest Plot on the Association Between Suicidal Attempt and Visual Impairment
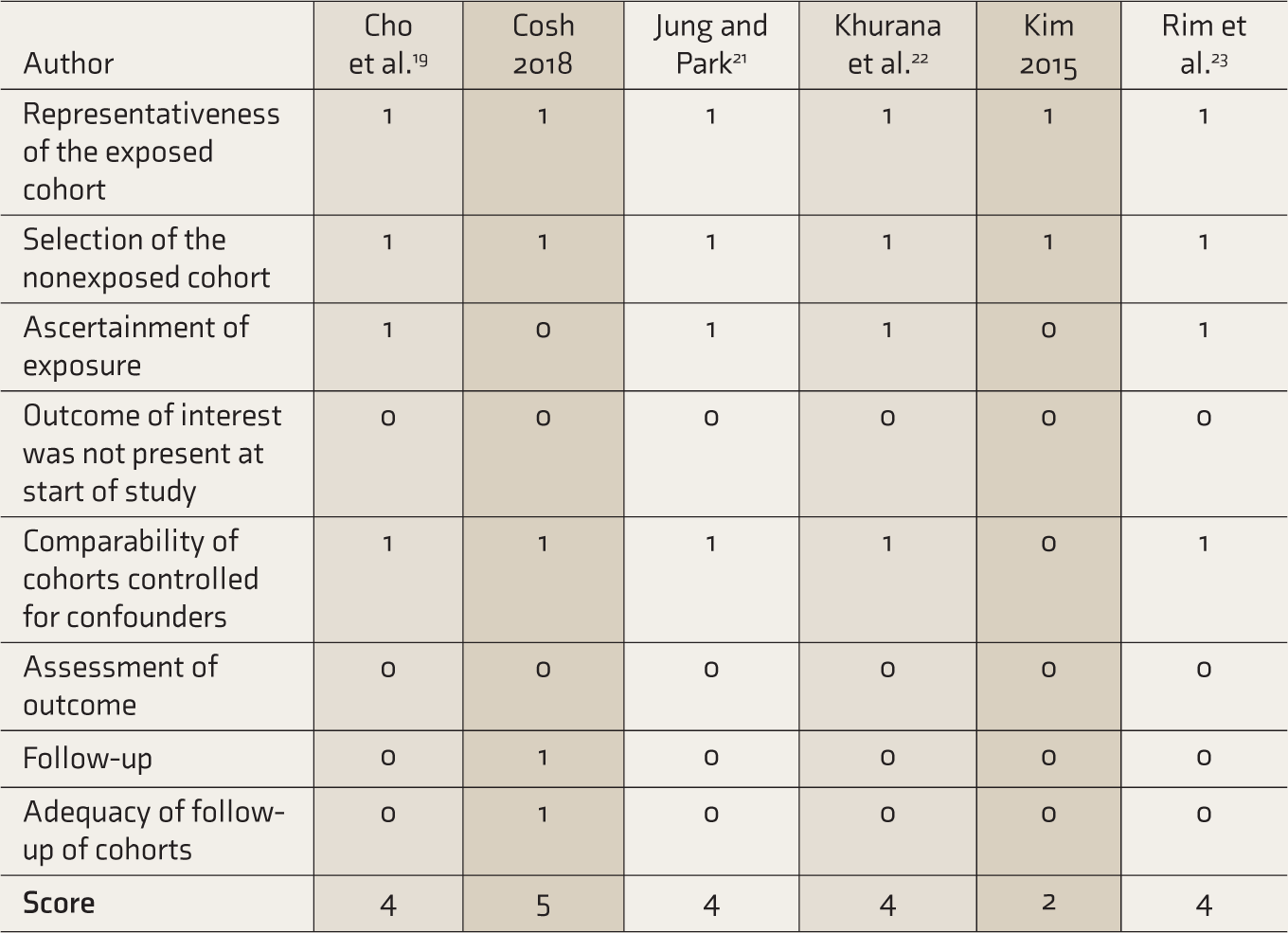
Regarding the risk of bias, overall, there was a mean NOS score of 4 out of 8. One study scored 2 out of 8 (Table 5). 12 Assessment of outcome (SI/attempts) was self-reported in all studies. In general, the outcome of interest was reported at the start of the study, and also, there was a lack of adequacy in follow-up in almost all the studies except one. 20
Risk of Bias Assessment
Discussion
To our knowledge, this is the first meta-analysis of the association between VI and suicidal behaviors (ideation/attempts). Eight studies have examined the association between VI and suicidal behaviors, with various measures of association. The current meta-analysis shows a significant association between SI and VI. The risk of suicidal attempts is four times higher in those with VI than those without any sensory impairment. Previous studies have revealed that other sensory impairments like hearing impairment also have an association with SI.20,24 Moreover, persons with additional sensory impairment have a higher risk of SI than those with only VI.
In this analysis, we excluded a few studies, given less clarity on group VI. In SI, suicide attempt, and depression, variations in terms of sociodemographic correlates such as age and socioeconomic position have been observed. 23 Previous studies have reported that VI increased the risk of falls and medication errors, impaired activities of daily living, and reduced the quality of life. 25
Increasing prevalence of VI and its significant association with mental health factors in older age have been consistently found in many previous studies.19,26,27 In specific VI like glaucoma, fear of blindness and the potential adverse effects of treatment can lead to depression and subsequent mental health issues.21,28 A study reported that the risk of suicide attempts decreased abruptly after 50 years of age, compared with young adults, whereas the older adults were more likely to have SI than young adults. 23 Many studies reported that SI increases as the age and severity of impairments increase. Because the reported OR of VI for the subset of the young population in the included studies was of negligible value, subgroup analysis based on age was not performed in the present review (Table S1). On the other hand, subjects with dual impairment (visual and hearing impairment) are more likely to have SI than those without sensory impairments. The combined indirect effects of reported VI operating jointly through poorer self-rated health and a higher number of reported nonocular conditions significantly increased the risk of death from suicide. 29 Older adults with VI or both auditory and VI were at a higher risk for SI than those without sensory impairments.12,30
Our meta-analysis has several strengths, including the rigor of the literature searches and the methodology followed, to provide reliable estimates. Moreover, information from most of the studies included in the systematic review also contributed to the meta-analysis. With high cases and participants, there was sufficient statistical power to detect moderate associations. As we performed a sensitivity analysis, it is evident that none of the studies influenced the overall estimate. We conducted subgroup analyses to elucidate whether adjustment for specific confounding factors influenced the summary estimates. A few studies have emphasized the possibility that some aspects of suicidal behavior may be higher among persons with VI than in those with hearing impairment or without any sensory impairment. 24
Our meta-analysis has some limitations too. Confounding by other risk factors may have influenced the present results. Also, the duration of VI has not been specified in many studies. Assessing publication bias would be difficult (and less relevant) in reviews with <10 studies, so it was not performed. 31 Differences in sociodemographic factors like age and socioeconomic status can act as confounders in SI and suicidal attempt. Because the primary studies did not perform subgroup analysis based on these parameters, our review could not explicitly address this aspect. Lack of explicit mention in primary studies of temporal association of VI preceding the suicidal behavior precluded us from proposing casual association between the two factors. Our findings have significant clinical and public health implications because of the high prevalence of VI. 32 If the current trends persist, it might contribute to increased death rates because of suicide. The existing psychosocial interventions for enhancing mental health in people with VI show some promise but are bounded by low adherence and lack generalizability. 33 However, a few interventions like cognitive behavioral therapy (CBT) and dialectical behavior therapy (DBT) have been found to reduce suicidal behaviors.34,35 These interventions help deal with stressful experiences and prevent the person from making another attempt.
Conclusion
This study indicated the strength of association between suicidal behavior and VI. Suicidal behaviors are a sign of extreme distress, and hence they should not be ignored. The ophthalmologist must detect these signs at an early stage and should refer to an appropriate mental health specialist to maintain good psychological condition and mental status of these patients. Regular counseling and social–emotional learning programs must be an integral part of the clinical management of visual and other sensory impairments. This is essential to prevent adverse psychological consequences, including suicidal behavior.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We acknowledge the technical support in data entry, analysis and manuscript editing by “Evidencian Research Associates.”
Declaration of Conflicting Interests
The authors have no potential conflicts of interest to declare with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.