
Abstract
Providing psychosocial interventions through telehealth is an approach to mitigate intimate partner violence (IPV). However, tele-consultation for IPV survivors need to be handled perceptively considering the risk to safety of the survivor and need for emergency support. This article provides strategies to address such issues while providing interventions to IPV survivors using telehealth in the clinical settings. Strategies for screening, assessment, planning psychosocial interventions, and termination of sessions are also summarized with supportive guidelines.
World Health Organization (WHO) remarks that worldwide, one in three women have undergone at least one form of violence by their intimate partner at some point in time. 1 Intimate partner violence (IPV) refers to all forms of violence, including physical, sexual, and emotional abuse and controlling behaviors such as isolating a person from family and friends, constantly monitoring them, and controlling their finances, education, employment, and medical care. 2
Though psychosocial interventions are available to address IPV, logistic issues have been a barrier to the availability and accessibility of such services. These challenges can be overcome by adopting telemedicine, which refers to the technology-driven delivery of healthcare services. Tele-consultation can be provided via real-time and/or asynchronous modes. Real-time interactions can be carried out via video-conferencing software, mobile applications, video-chat platforms (e.g., Skype/Facetime), audio mode such as phone call/VOIP, mobile apps, text-based methods (using chat-based applications such as specialized smartphone apps for telemedicine), websites and other relevant internet-based systems, and/or general messaging/text/chat platforms (e.g., WhatsApp, Google Hangouts, Facebook, Messenger). Examples of asynchronous means include email and fax. After the onset of the COVID-19 pandemic, technology-driven psychosocial interventions have become a familiar phenomenon and widely acceptable globally.
WHO recommends that every healthcare professional be trained to identify and address psychosocial distress associated with any form of violence against women, children, and older adults. 3 Mental health professionals (MHP) play a vital role in a multi-sectoral response to IPV, including screening, identifying those who have been subject to or are at risk of violence, appropriate referral to specialized services, and follow-up in the community. 4
In India, National Tele-Mental Health Programme was launched by the Government of India with the National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, as the nodal center to network with 23 tele-mental-health centers of excellence across the nation. 5 In addition, a series of telehealth guidelines have been prepared for MHPs,6-9 based on the framework of the Medical Council of India. 10 These are getting gradually implemented in various clinical settings. Providing technology-driven psychosocial support for IPV survivors requires specific pre-requisite skills compared to conventional face-to-face sessions. It involves risks to privacy, confidentiality, and digital and physical safety. If not handled sensitively, the violence may increase. For example, the perpetrators may monitor the survivors’ call history and browsing history. When they find out about the survivor reaching out for formal or informal help, the use of violence may increase, eventually leading to drop out of the survivor from seeking help, either by choice or force, which may prevent attaining the goal of the service provider. Therefore, this paper attempts to provide practical guidelines for assessment and essential soft skills for the MHP delivering tele-counseling to individuals experiencing IPV.
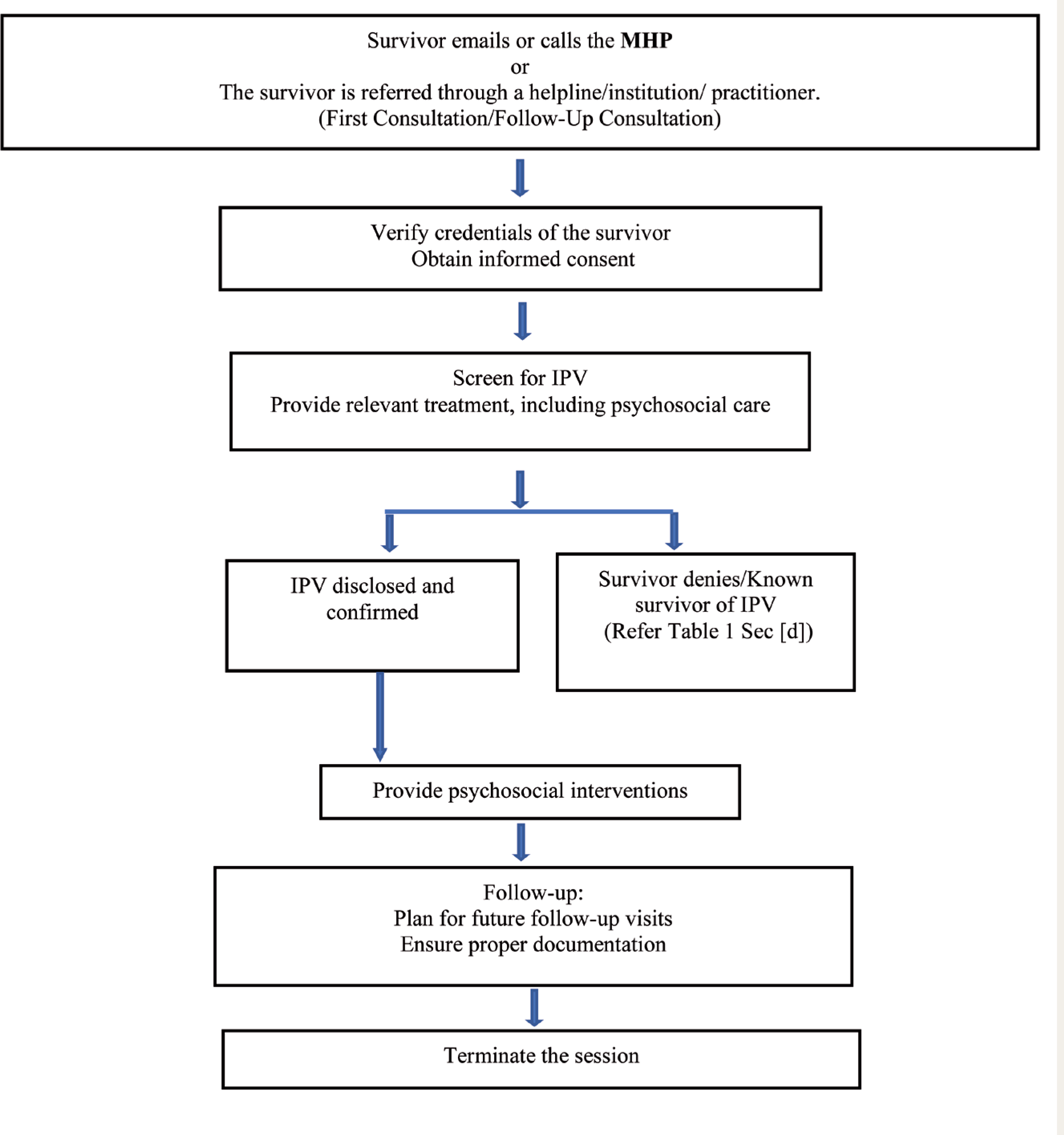
The guidelines apply to both new patients and follow-up patients transitioning from in-person consultation to teleconsultation mode. The process of recruiting individuals experiencing IPV for teleconsultation is explained in Figure 1. Strategies to be followed in recognizing and responding to IPV during teleconsultation are given in
Process of Recruiting a Survivor for Tele-Consultation
Case Identification and Assessment
The primary aim of MHP is to create a safe environment for the survivor to disclose IPV. Rarely does self-disclosure occur during a health/mental health screening. Many a time, the survivor may not be forthcoming about IPV. Some of the commonly reported causes for non-disclosure of IPV include lack of privacy, presence of an abusive partner in the vicinity, fear/threat of further violence from partner, embarrassment/shame, and fear that their story may not be believed.11-13 Therefore, the MHP should have adequate skills to pick on “red flags” associated with IPV, such as unexplained injuries, wearing long sleeves in summer to hide injuries, low self-esteem, and constantly looking up to the partner for minor decisions while the patient is reporting some other psychosocial concern.
Responding to a Disclosure of IPV
During tele-sessions, MHP may have limited control over the survivor’s environment. The abusive partner may walk in or find out about the help sought by the survivor, which could lead to an escalation in violence. To ensure the safety of the survivor, discuss cues to communicate the presence of the perpetrator near them a priori (
A few relative contradictions to teleconsultation are when a survivor: (a) is at risk of harm, (b) has thought of committing suicide, (c) expresses a homicidal idea, and (d) shows signs of cognitive impairment. The survivor should be encouraged for an in-person consultation or referred to the nearest emergency health service by providing adequate information. It is also important to assess the benefits and risks of providing tele-session.
Guidelines for Tele-Consultation—Strategies for the MHP for Identifying and Responding to Survivors of IPV
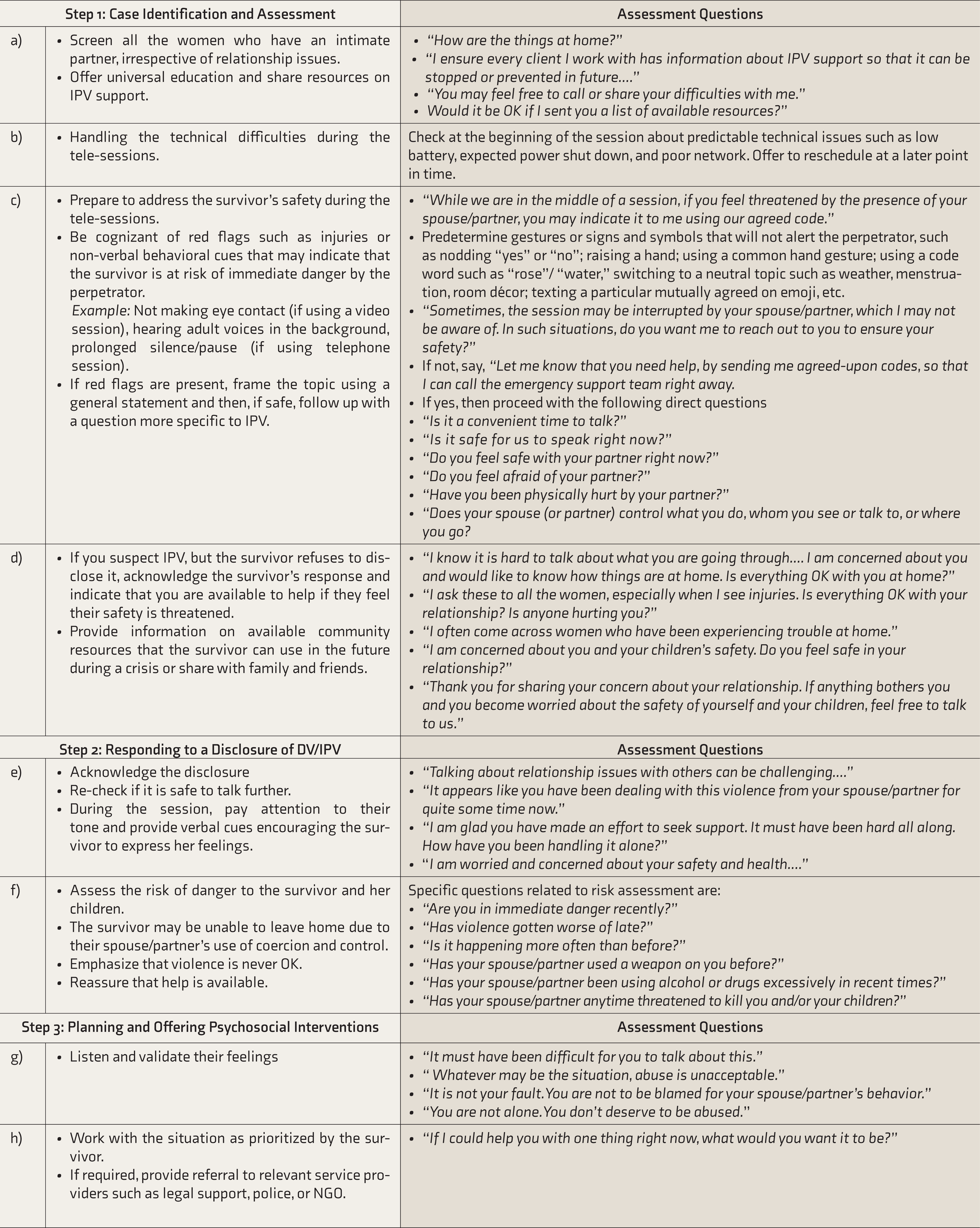
DV: domestic violence, NGO: nongovernmental organization,
IPV: intimate partner violence, MHP: mental health professional.
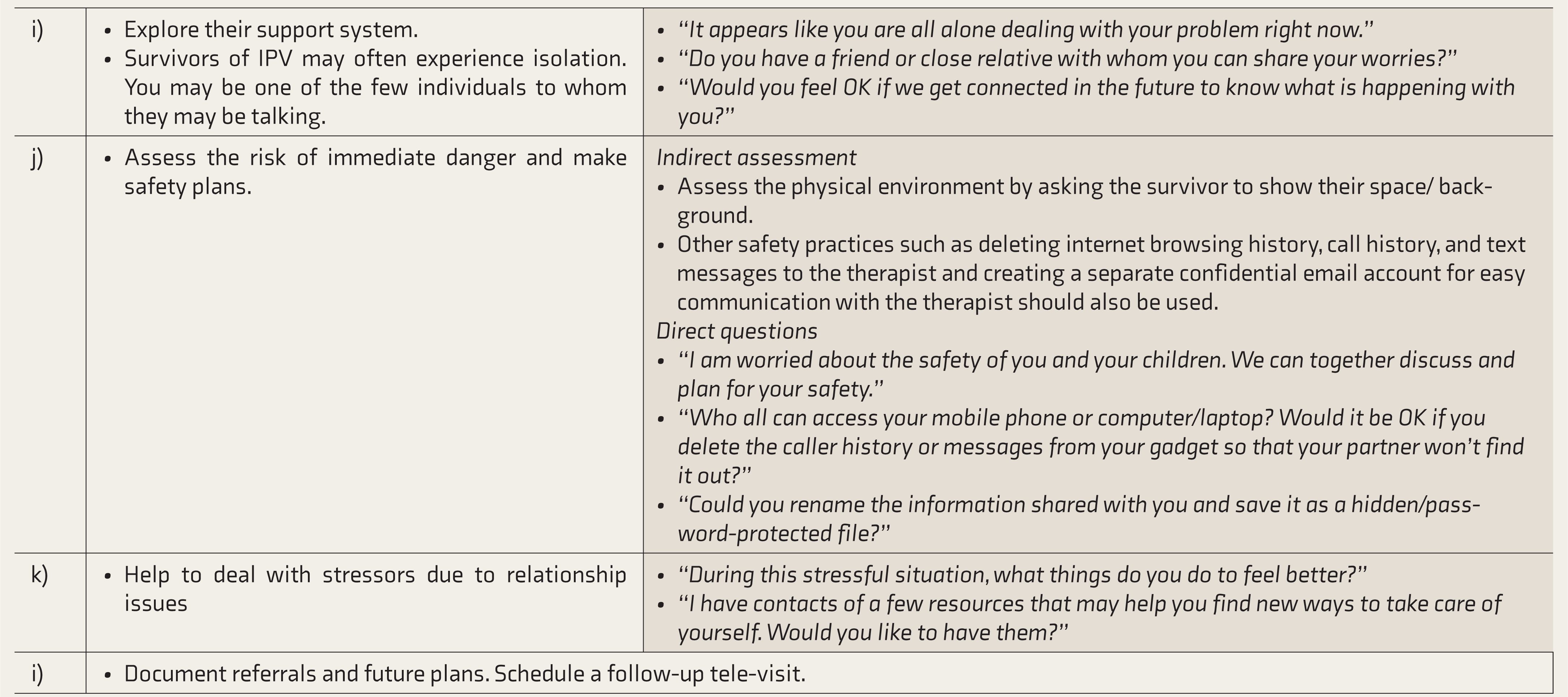
Planning and Offering Psychosocial Intervention
The initial stage of therapy should focus on building therapeutic relationship and offering immediate first-line psychological aid to alleviate the survivor’s distress. The intervention should be guided by two fundamental principles of a woman-centric approach: respect for women’s rights and the promotion of gender equality.4,14,15 Safety planning is one of the important components of the intervention to prevent further violence targeted towards self and/or their children (Table 1, subsection j).
Safety skills include recognizing cues or signs of potential danger. For example, the therapist should help the survivor identify those behaviors and traits of the perpetrator that have been associated with violence in the past, in addition to stressors such as relationship difficulties, lack of privacy, increased substance abuse, loss of employment, and financial constraints. The therapist should share a list of safety resources available in the community, such as contact of the local police station, women’s helpline numbers, local shelters, and nearby hospital facilities, taking into account what communication device the survivor is using (e.g., password-protected text messages, email to the private account of the survivor).
Teach digital safety, that is, to delete the therapist’s call history immediately after the session to prevent getting exposed if perpetrator tends to track the survivor’s actions. Also discuss strategies she has adapted in the past to prevent violence. Safely skills include planning how she might respond in different situations, including emergencies. Advice to keep a bag with all essential items (including essential documents) for easy exit in case of emergency, hide harmful items away from the perpetrator, know and recognize early signs of potential violence, know where to go in case of crisis, identify safe zone to take shelter in the house/neighborhood, rehearse to safely exit home along with the children, and train children to make emergency calls in case of crisis.
When providing online sessions, technical difficulties are common. A backup plan for services should be discussed with the client to avoid interruption with service delivery. When an element of risk to safety is involved, the therapist must wait for the client to initiate the call. If unable to reconnect with the client, the therapist can initiate a call to the local emergency women’s helpline number for further help.
Organizational Responses to IPV
After the COVID-19 pandemic started, the modality of delivery of psychosocial services has shifted from face-to-face intervention to online intervention, to some extent. The launch of the National Tele-Mental Health Programme in India has given new impetus to reach the unreached through technology, to provide quality mental health services and care to people of all ages. Healthcare institutions should have a policy and framework to implement telehealth interventions for IPV survivors. The digital divide, where most people cannot afford and access telehealth services, needs to be addressed.
Conclusion
The authors attempted to aid the MHP to identify and address IPV issues using telemedicine in clinical settings. The article highlights the need for MHP to be mindful of the safety issues and appropriate intervention strategies while delivering psychosocial care using telemedicine. As the digital divide for accessing and affording telemedicine is gradually declining, the researchers in IPV must actively develop evidence-based standard operating protocols for technology-driven emergency preparedness and IPV-focused service delivery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.