
Abstract
Background:
Opioids can adversely affect sexual function by impacting the endocrine system, particularly the pituitary gland and sex hormones. While synthetic opioids have been well studied, little data exists on natural opium’s impact on sexual functioning, especially in India, where it is considered an aphrodisiac. This study aims to evaluate sexual dysfunction and related factors among men who are dependent on natural opium.
Methods:
In this cross-sectional study, we recruited 107 participants with a dependency on natural opium. The assessment included the Arizona sexual experience scale (ASEX), the International Index of Erectile Function (IIEF), the severity of opiate dependence questionnaire (SODQ), and the sex knowledge and attitude questionnaire (SKAQ-II). Additionally, assays were conducted for serum total testosterone, follicle-stimulating hormone (FSH), luteinizing hormone (LH), and prolactin.
Results:
The rate of sexual dysfunction was 47% for ASEX and 91% for IIEF. Low serum testosterone and LH levels were found in 22% and 16% of cases, respectively. Hyperprolactinemia and low FSH levels were observed in 11% and 3% of cases, respectively. Older patients had a significantly higher prevalence of sexual dysfunction and displayed more severe opioid dependence. Hormonal assessment revealed significantly low testosterone levels among those with sexual dysfunction on ASEX. Logistic regression analysis indicated that only the severity of opioid dependence was a significant predictor of sexual dysfunction.
Conclusions:
This research indicates that natural opium users frequently experience sexual dysfunction, which correlates with the intensity of opioid dependence. Consequently, clinicians must assess and address this issue to consistently improve treatment outcomes.
Sexual dysfunction frequently occurs in users of natural opium and impacts all aspects of sexual function for those dependent on it, much like synthetic opioids do. Sexual dysfunction correlates with the intensity of opioid dependence. This study tackles a widespread myth that using natural opium boosts sexual performance. Regular evaluations of sexual function and its treatment may be crucial for preventing relapse, boosting treatment adherence, and improving overall results.Key Messages:
In India, natural opium, which is commonly known as Amal/Afeem and Doda, continues to be culturally accepted despite stringent regulations, as it is thought to improve physical, mental, and sexual performance.1,2 In Rajasthan, the rate of natural opium use varies between 6.4% and 8.9%. 3 Individuals often use opium as an aphrodisiac to alleviate anxiety tied to sexual performance, enhance sexual abilities, prolong ejaculation, and alleviate sexual issues independently. 4
Long-term opioid use can cause ongoing sexual functioning issues, revealing a complex link between opioid use and sexual dysfunction. 5 Sexual dysfunction prevalence rates range from 33% to 92% among opioid-dependent patients.6–9 Opioid use affects sexual functioning, including erectile dysfunction, orgasmic dysfunction, and reduced sexual pleasure.4,5,10
Opioids negatively affect the endocrine system, leading to decreased levels of luteinizing hormone (LH), follicle-stimulating hormone (FSH), and testosterone, as well as increased prolactin levels, which results in an elevated risk of sexual dysfunction.11–14 A systematic review found hypogonadism in 63% of opioid users, along with a high prevalence of hyperprolactinemia. 12
A person’s sexual practices are shaped by their knowledge, attitudes, and influences. 15 Patients may rely on inaccurate information from articles, peers, or roadside materials, leading to superficial knowledge filled with myths and misconceptions, 16 which may contribute to sexual dysfunction.
The effectiveness and influence of natural opium on opioid receptors and hormones can vary from synthetic opioids, 17 along with differences in knowledge, attitudes, and practices. A study in India indicated that sexual dysfunction among mixed opioid users ranged from 53.3% to 81.7%, with natural opioid users experiencing a rate of 65%. 18 The specific type of opioid used significantly affects both the extent and severity of sexual dysfunction. 19
Although sexual dysfunction is common, patients often keep it to themselves, and clinicians may fail to evaluate it. This lack of awareness and inadequate assessment of sexual health in opioid-dependent patients can lead to poor treatment adherence, abandonment of treatment, relapse, and unsatisfactory outcomes. 4
The existing research on sexual dysfunction in opioid users predominantly centers on synthetic opioids, with limited studies addressing the effects of both synthetic and natural opioids. Knowledge concerning the impact of natural opium on sexual health and hormonal levels is sparse. Thus, this study was primarily aimed at assessing the prevalence and characteristics of sexual dysfunction among male patients dependent on natural opium. Additionally, it sought to analyze how this dysfunction relates to demographic factors, clinical history, sexual knowledge, and hormonal profiles (total testosterone, LH, FSH, and prolactin) as a secondary objective.
Methods
This cross-sectional study was conducted at a tertiary care hospital in northwestern India, receiving approval from the Institutional Ethics Committee between January 1, 2021 and June 30, 2022. The sample size was determined using the formula for a prevalence study. The lowest possible prevalence rate (40%) among opioid users based on the Arizona sexual experience scale (ASEX) was taken as reference, 20 assuming the low prevalence of sexual dysfunction among the natural opium users, as the data regarding prevalence among natural opium users was not available.
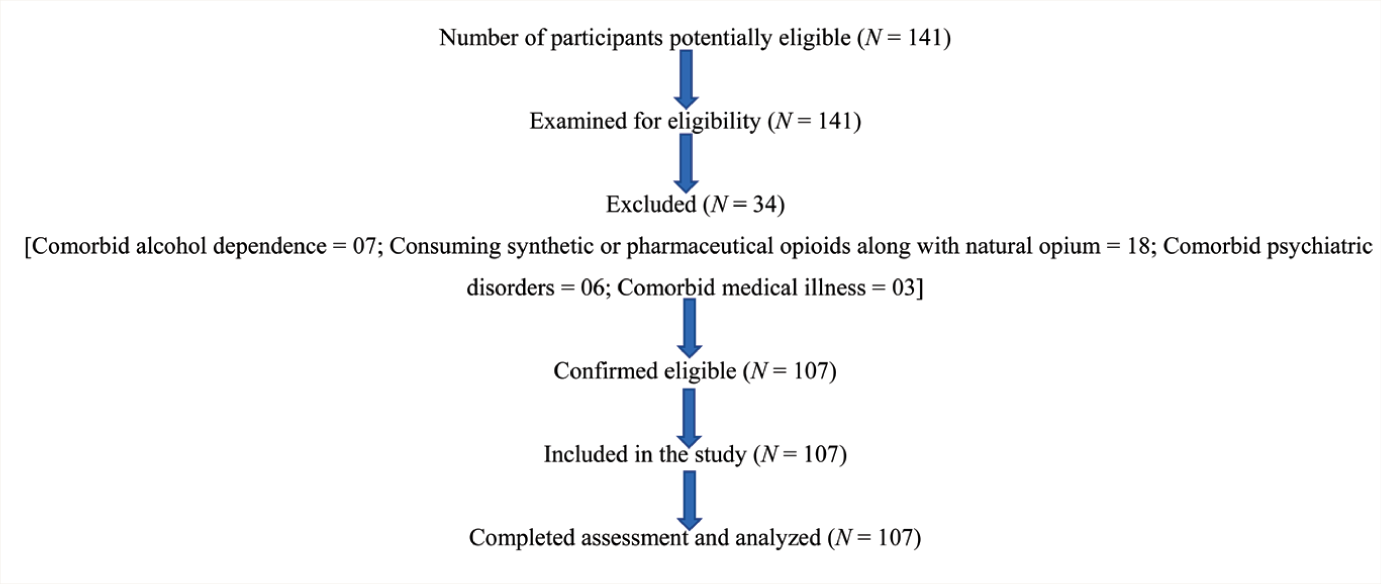
Assuming a 5% precision, an estimated prevalence of 40% for sexual dysfunction, and a typical patient population of 150 patients dependent on natural opium seeking treatment from our outpatient clinic in the past 18 months, the required sample size was calculated to be 107. The patients were recruited by the first author from the OPD, considering ease of recruitment with regular clinical work (convenience sampling). During the study period, 141 participants were examined for eligibility, and finally, 107 were assessed and analyzed (Figure 1).
Study Participants Flow Diagram.
Eligibility Criteria
All male patients aged 20–50 years with current opium use, who are first-time visitors to the outpatient department, diagnosed with opioid dependence according to ICD-11 criteria, not on any treatment, scored less than five on the clinical opiate withdrawal scale (COWS), and are either married or in a relationship (sexually active) for at least six months, were included in the study. Patients who were dependent on any substances aside from tobacco, synthetic or pharmaceutical opioids, those undergoing androgen replacement therapy, or who had any comorbid psychiatric, chronic medical, endocrinological, or neurological disorders, as well as those with a history of head injuries, trauma, or pelvic surgeries, were excluded based on self-report and clinical evaluation.
Data Collection
Participants who met the selection criteria were recruited into the study after obtaining written informed consent. After collecting socio-demographic and clinical profiles, patients were assessed using the severity of opiate dependence questionnaire (SODQ), the Fagerström Test for Nicotine Dependence (FTND), the ASEX, the International Index of Erectile Function (IIEF), and the sex knowledge and attitude questionnaire (SKAQ-II). Using morning samples, hormones such as total testosterone, FSH, LH, and prolactin were measured via chemiluminescent immunoassay (CLIA).
Measures
The socio-demographic profile sheet gathered information on age, gender, marital status or stable sexual relationships, religion, locality, family type, education, occupation, family income, and socioeconomic status of the patient. The clinical profile included the age of onset of opium use, reasons for starting, duration of use, length of the dependent pattern of use, form and amount of opium used, high-risk behaviors (high-risk sexual behaviors and injection drug use), previous attempts at abstinence, last date of consumption, and withdrawal scores before the assessment of sexual dysfunction. The severity of tobacco dependence was measured with the FTND scale. 21
The COWS, 22 a clinician‐administered instrument, was used to rate opioid withdrawal, while the SODQ 23 assessed the severity of opioid dependence. SODQ is a nine-item self-report questionnaire divided into five sections, consisting of 21 questions rated on a four-point Likert scale from 0 to 3, with a total score range of 0–63.
The ASEX is a five-item self-administered inventory that evaluates five dimensions of sexual functioning in both genders according to DSM-IV criteria. These dimensions include sexual drive, arousal, penile erection/vaginal lubrication, ability to reach orgasm, and satisfaction from orgasm. Scores are rated on a six-point Likert scale. Clinical sexual dysfunction is defined as a total scale score greater than 19 (criteria A), a score greater than five for any individual domain (criteria B), or a score of four or higher in any three domains (criteria C). 24
The IIEF is a 15-item self-administered tool with well-established cross-cultural validity that assesses the following domains of sexual function: Erectile Function, Orgasmic Function, Sexual Desire, Intercourse Satisfaction, and overall satisfaction. It positively correlates with clinical interviews about sexual function and is regarded as the gold standard for evaluating erectile function. Sexual dysfunction is indicated when the total score falls below 25 for erectile function, below 13 for intercourse satisfaction, and below nine for orgasmic function, sexual desire, and overall satisfaction. 25
The SKAQ-II is a 55-item tool that includes a 35-item knowledge section (with dichotomous responses of yes/no, yielding a maximum attainable score of 35) and a 20-item attitude section (utilizing a 3-point Likert scale, with a maximum achievable score of 60). Higher scores reflect better sexual knowledge and a more liberal attitude toward sex. It has demonstrated test-retest reliability and discriminant validity. 26
Hormonal Assessment
LH, FSH, and prolactin levels were measured using the Diasorin Liaison XL, which utilizes a sandwich CLIA. In this process, magnetic nanoparticles coated with a monoclonal antibody capture the hormones from the samples. An isoluminol-antibody conjugate reacts with these bound hormones, and the resulting chemiluminescence signal is quantified in relative light units (RLU), indicating hormone concentration.
The testosterone levels were assessed using the ADVIA Centaur testosterone assay, a competitive immunoassay that utilizes chemiluminescence. This process involves mixing the sample with a releasing agent, adding reagents, and then incubating it. The system measures RLUs, which correlate inversely with testosterone levels.
Data Analysis
Data were entered and analyzed using the Statistical Package for the Social Sciences (SPSS Statistics, version 21.0.0). Frequencies and percentages were calculated for categorical variables, while means and standard deviations were determined for continuous variables. Data normality was assessed using the Shapiro–Wilk test. Relationships between categorical variables were analyzed using the Chi-square test or Fisher’s exact test (for cells with fewer than five frequencies in more than 20% of cases).
The secondary objective of this study was to conduct an exploratory analysis to identify the factors associated with sexual dysfunction, so the sample was divided into two groups based on the ASEX score: those with sexual dysfunction and those without. Such categorization is clinically more helpful and is validated in the standard scoring of the ASEX. Comparisons between groups regarding socio-demographic and clinical parameters, as well as the association between opium use, sexual dysfunction, and hormonal levels, were examined using the Mann-Whitney U test for non-normal data.
Furthermore, a bivariate correlation analysis was employed using Spearman’s coefficient to examine the associations between continuous variables. Binary logistic regression analysis was used to identify predictors of sexual dysfunction, with a p value of <.05 considered significant. There was no missing data in this study.
We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline 27 to draft this manuscript, and the STROBE reporting checklist 28 when editing, which is included in the supplementary online material.
Results
The sample had a mean age of 35.34 years and a mean education level of 10.86 years. Among participants, 62.6% consumed Amal/Afeem, while 37.38% consumed Doda (Table 1 and Supplementary Table 1).
Socio-demographic, Clinical, and Hormonal Profile of Study Participants (N = 107).
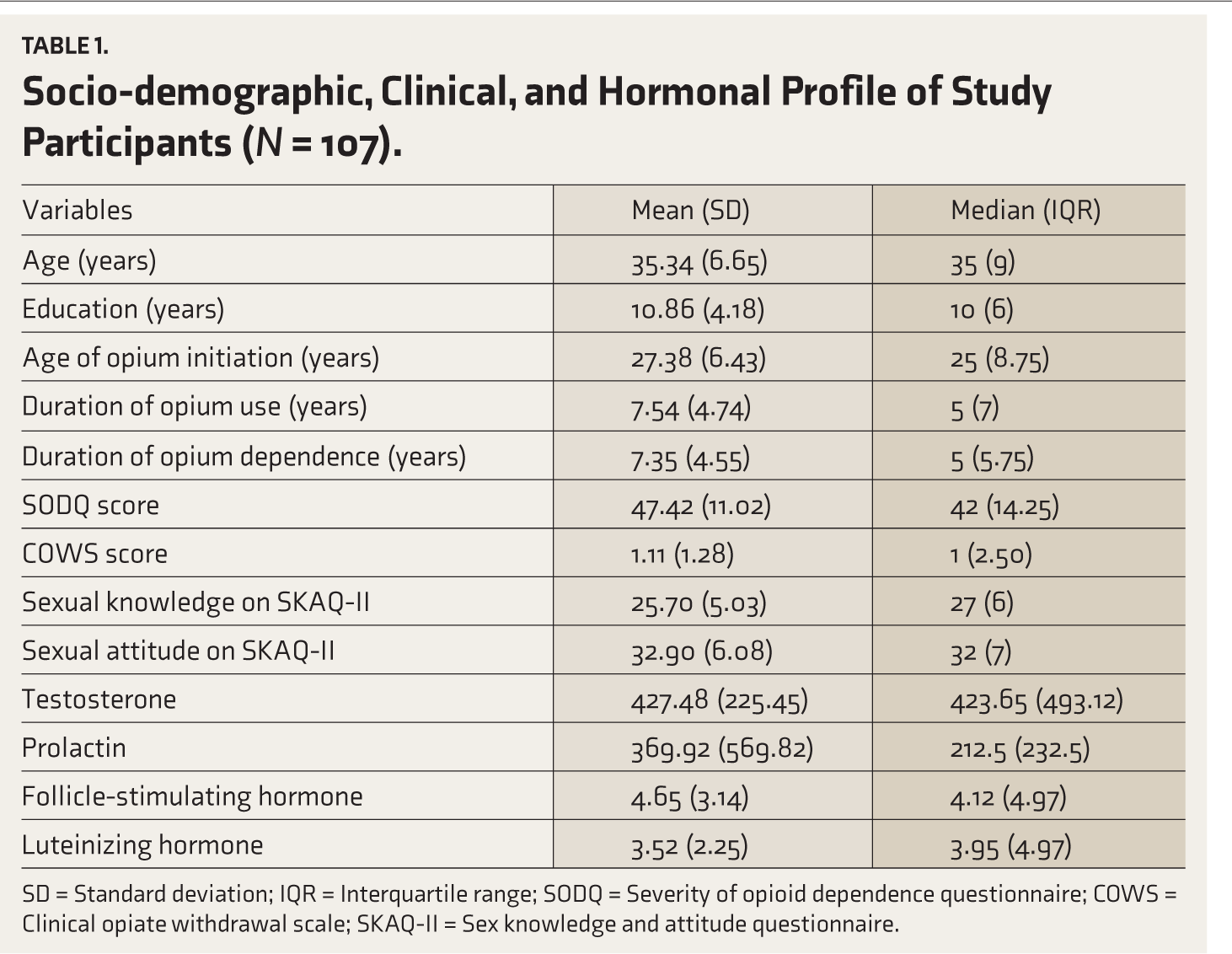
SD = Standard deviation; IQR = Interquartile range; SODQ = Severity of opioid dependence questionnaire; COWS = Clinical opiate withdrawal scale; SKAQ-II = Sex knowledge and attitude questionnaire.
The prevalence of sexual dysfunction, according to ASEX, was 46.7%. The most commonly affected ASEX domain was desire/drive, followed by the ability to achieve orgasm and erection. In contrast, the prevalence of sexual dysfunction according to the IIEF was 90.7%. The most commonly affected domains were orgasmic function and erectile function (Table 2).
Prevalence and Pattern of Sexual Dysfunction on ASEX and IIEF (N = 107).
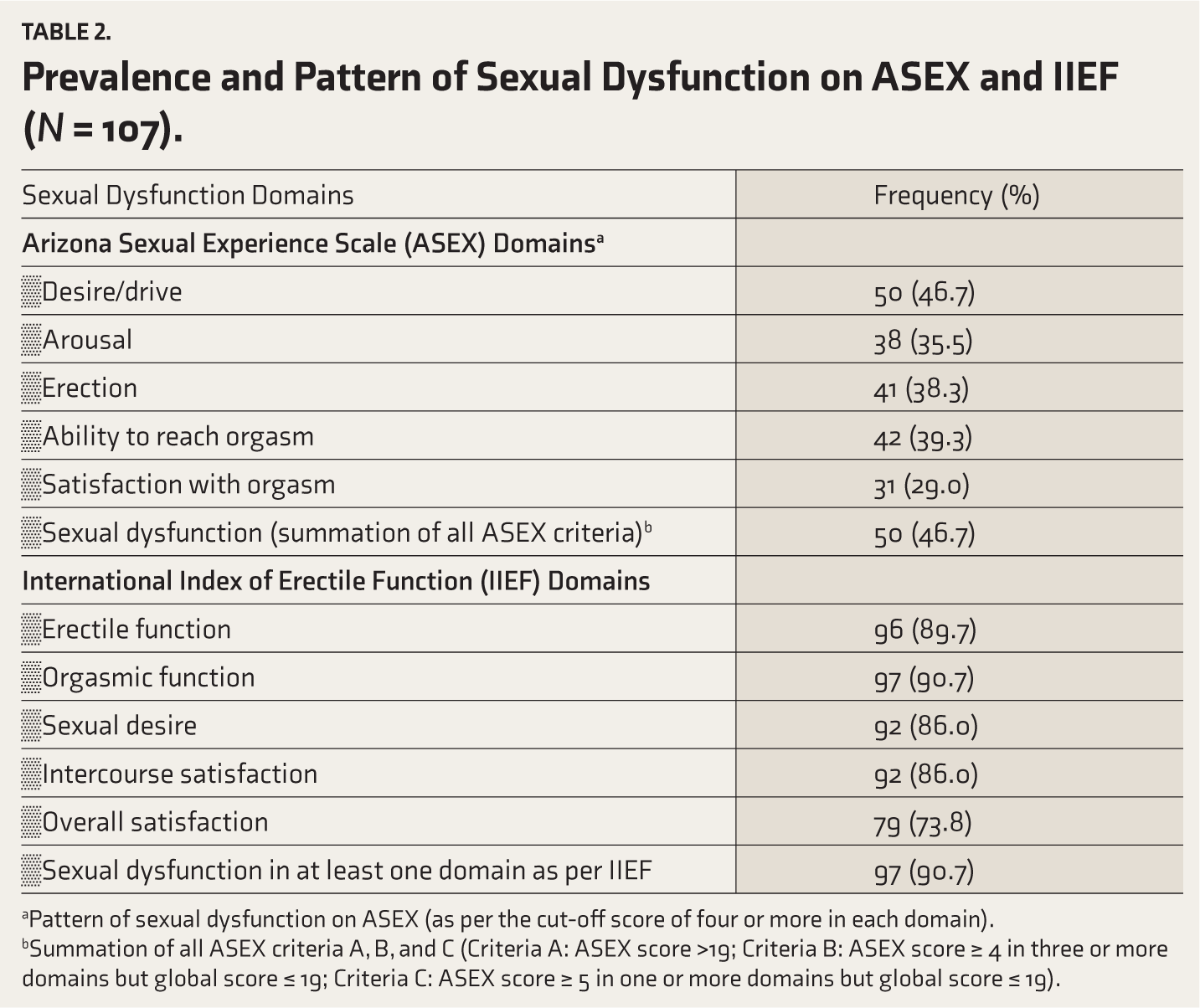
aPattern of sexual dysfunction on ASEX (as per the cut-off score of four or more in each domain).
bSummation of all ASEX criteria A, B, and C (Criteria A: ASEX score >19; Criteria B: ASEX score ≥ 4 in three or more domains but global score ≤ 19; Criteria C: ASEX score ≥ 5 in one or more domains but global score ≤ 19).
Regarding the hormonal profile, 22.4% of patients exhibited low testosterone levels, 15.9% had low LH levels, and 2.8% had low FSH levels, while hyperprolactinemia was observed in 11.2% of patients. A few patients had high LH (3.7%), FSH (3.7%), and testosterone (2.8%) (Supplementary Table 2).
In the hormonal profile, testosterone levels were significantly lower in the sexual dysfunction group based on ASEX. Sexual dysfunction was notably more prevalent among older patients (U = 1758.50, p = .037) and was associated with greater severity of opioid dependence (U = 2352.50, p < .001). However, no significant differences were noted between the sexual dysfunction and non-sexual dysfunction groups regarding education, marital status, family type, locality, duration of opioid dependence, sexual knowledge, attitude, type of natural opium, and tobacco use pattern. Nearly 75% of patients exhibited nicotine dependence in both the sexual dysfunction and non-sexual dysfunction groups based on ASEX (Table 3 and Supplementary Table 1).
Comparison of Socio-demographic, Clinical, and Hormonal Profiles of Study Participants in the Sexual Dysfunction and Non-sexual Dysfunction Groups Based on ASEX (N = 107).
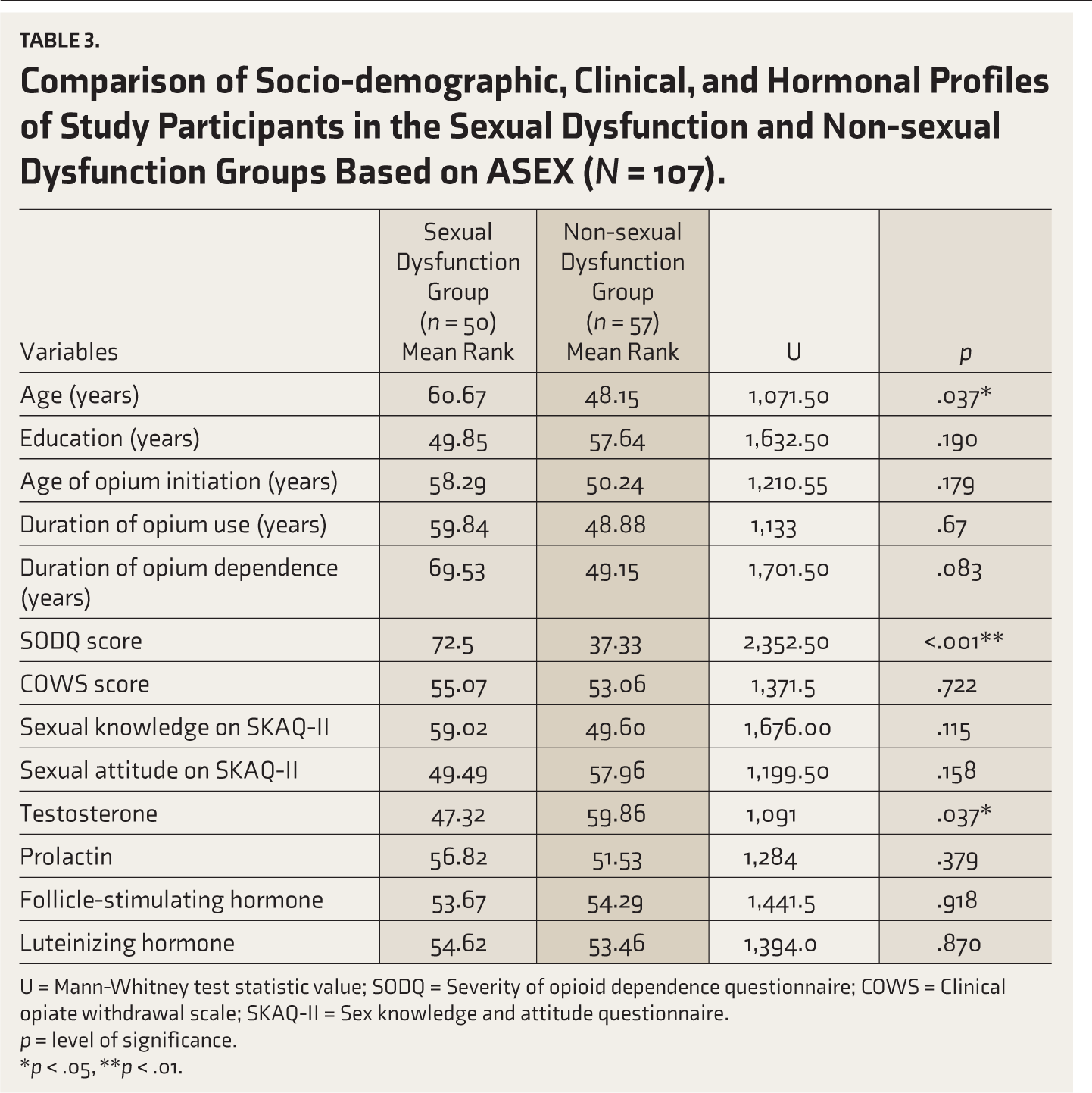
U = Mann-Whitney test statistic value; SODQ = Severity of opioid dependence questionnaire; COWS = Clinical opiate withdrawal scale; SKAQ-II = Sex knowledge and attitude questionnaire.
p = level of significance.
*p < .05, **p < .01.
The patients with sexual dysfunction scored significantly higher in all domains of ASEX (p < .001) (Table 4).
Comparison of Sexual Dysfunction Subdomains Between the Sexual Dysfunction and Non-sexual Dysfunction Groups Based on ASEX (N = 107).
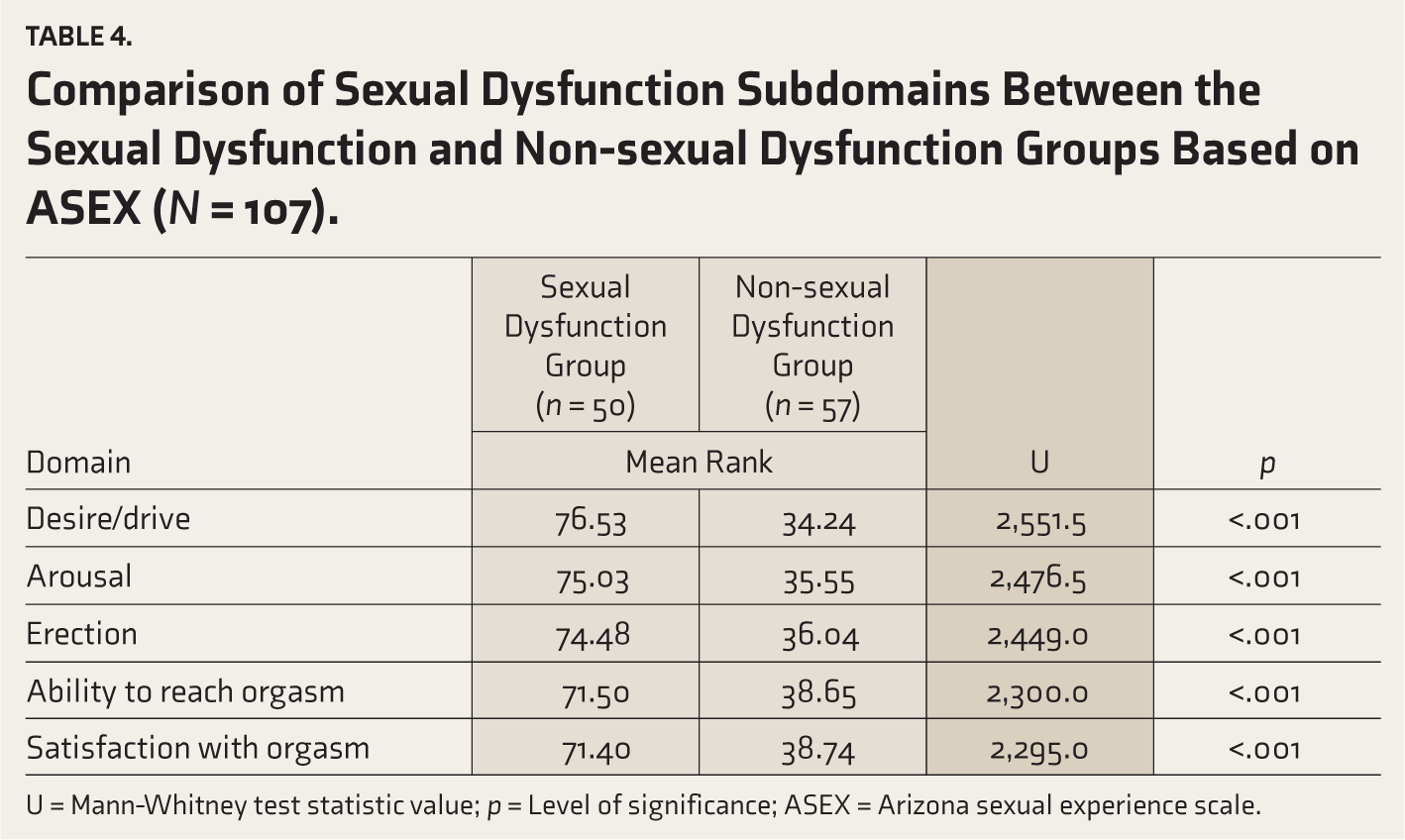
U = Mann-Whitney test statistic value; p = Level of significance; ASEX = Arizona sexual experience scale.
Furthermore, according to Spearman’s correlation, the patient’s age showed a significant positive correlation with dysfunction across all ASEX domains. The duration of opioid dependence was also significantly positively correlated with the ASEX domains of arousal, ability to reach orgasm, and the total ASEX score. The total SODQ score demonstrated a significant positive correlation with dysfunction in all ASEX domains and the total ASEX score, suggesting that higher levels of sexual dysfunction are observed in patients with elevated SODQ scores. Sexual knowledge showed a significant positive correlation with all ASEX domains, while sexual attitude was significantly negatively correlated with all ASEX domains except the ability to reach orgasm. Serum testosterone had a significant negative correlation specifically with the ability to reach orgasm domain of ASEX (Table 5).
Spearman’s Correlation of Clinical Variables (N = 107).
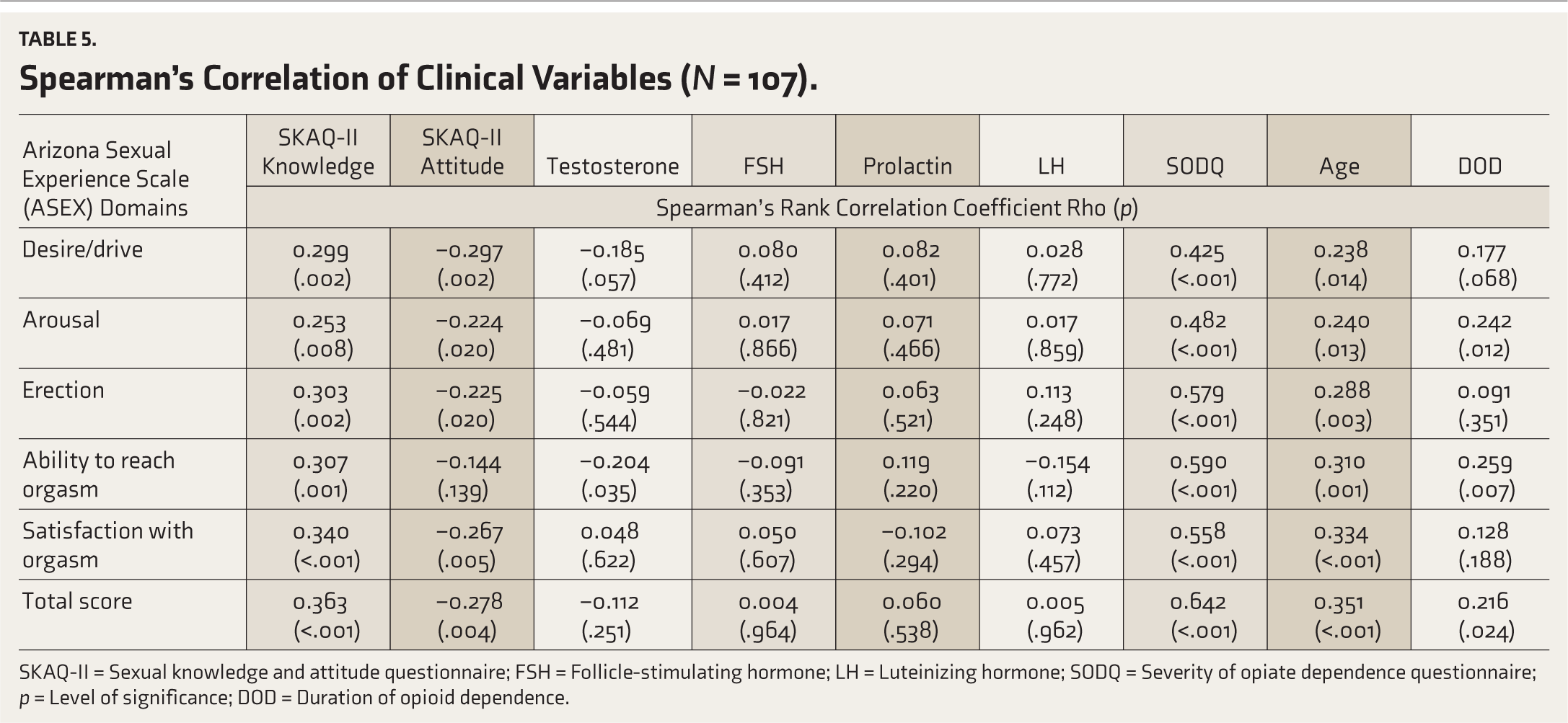
SKAQ-II = Sexual knowledge and attitude questionnaire; FSH = Follicle-stimulating hormone; LH = Luteinizing hormone; SODQ = Severity of opiate dependence questionnaire; p = Level of significance; DOD = Duration of opioid dependence.
A binary logistic regression was conducted to identify variables significantly linked to sexual dysfunction. The variables were selected based on their clinical relevance and potential association with sexual dysfunction. Key factors, such as age, clinical indicators like the duration of opioid dependence, sexual knowledge and attitude, the severity of opioid dependence as determined by SODQ scores, and serum testosterone levels, were chosen for their known impact on sexual health and opioid dependence. The model accurately classified 78.5% of patients. The specificity (true negative rate) and sensitivity (true positive rate) for this model were 89% and 86%, respectively. The model explained 39.1% of the variance in the dependent variable (Nagelkerke R² = 0.391). The findings revealed that only a higher SODQ score (OR: 1.131; 95% CI: 1.070–1.196) was a significant predictor of sexual dysfunction (Table 6).
Predictors of Sexual Dysfunction by Using Binary Logistic Regression (N = 107).
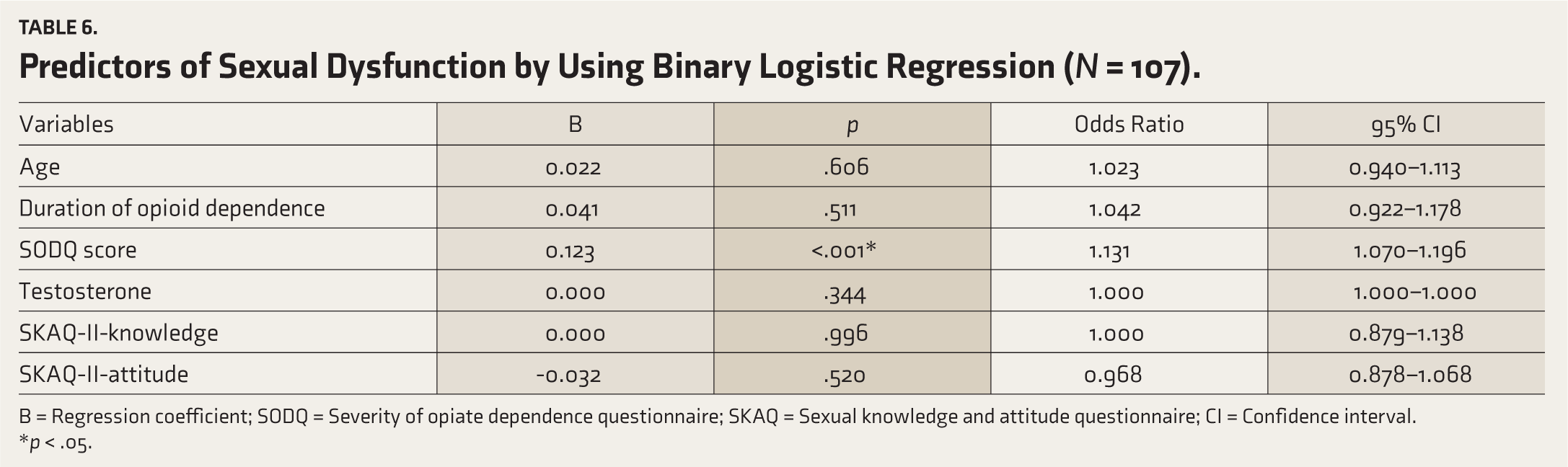
B = Regression coefficient; SODQ = Severity of opiate dependence questionnaire; SKAQ = Sexual knowledge and attitude questionnaire; CI = Confidence interval.
*p < .05.
Discussion
This study assessed sexual dysfunction, its patterns, and its association with hormonal profiles, demographics, and clinical factors among male patients dependent on natural opium. The study found that sexual dysfunction among natural opium users was approximately 47% (by ASEX) and 91% (by IIEF), significantly higher compared to the 21.15% sexual dysfunction (by ASEX) found in the healthy Indian population. 29 This aligns with the range of 48% to 92% sexual dysfunction reported by Indian studies among patients with opioid dependence after 6 days of abstinence 8 and among mixed (natural and synthetic) opioid user populations 18 assessed using ASEX and IIEF scales. However, it exceeds the prevalence reported (47%–60% by IIEF) by an Indian study of predominantly heroin users. 30 Among opioid users receiving treatment, methadone users had a pooled sexual dysfunction prevalence of 52%. 9 Another study reported that about 83% of men on buprenorphine and 90% on naltrexone reported experiencing at least one symptom of sexual dysfunction. 31
The variations in the prevalence of sexual dysfunction could be due to differences not only in socio-cultural settings, types of opioids, doses, durations, and severity of use, but also in patients’ comfort levels with therapists and the tools used to assess sexual dysfunction. Higher prevalence rates may also be influenced by confounding by indication, as natural opium in our cultural setting is commonly used to enhance sexual functioning. Our study did not assess sexual function before starting opium, and the reasons for initiation were not examined.
The ASEX and IIEF scales were used for a wider comparison, as most studies have employed both of these scales. Discrepancies in the estimate of prevalence and pattern of sexual dysfunction between the scales can stem from several factors, including the areas each scale evaluates. ASEX covers a broader range of sexual dysfunctions, while the IIEF provides a superficial assessment of sexual functioning other than erection. 32 Additionally, this study evaluated sexual dysfunction during the active phase of opium use, and when subjects were not in the withdrawal phase, contrasting with earlier studies that assessed sexual dysfunction during the treatment phase. Consequently, the results reflect the true effect of opium use rather than the influence of medications or withdrawal, which may affect the prevalence and patterns of sexual dysfunction; for instance, premature ejaculation is most common during the abstinence and withdrawal phases. 31
On the ASEX, the most frequently affected domain was desire/drive, followed by orgasm, erection, and arousal, with orgasm satisfaction being the least affected domain. These findings suggest that natural opium has a negative generalized effect on all sexual domains rather than on a specific domain. An Indian study also found hypoactive sexual desire and intercourse dissatisfaction to be the most common issues, followed by erectile and orgasmic dysfunction among patients on buprenorphine. 20 A meta-analysis also identified hypoactive sexual desire as the most prevalent dysfunction in trials involving buprenorphine and methadone substitution. 9 Few other studies have found that orgasmic dysfunction was a prevalent issue among heroin users and opioid-dependent patients.8,30,33 Opium is frequently used to increase ejaculation time, but in the long run, opioids have been associated with delayed ejaculation and even anorgasmia. 10 Delayed orgasm occurs with opioids as they interfere with the neurochemical signals involved in sexual arousal and climax. 34
In earlier studies, even though the patients used different types of opioids, such as synthetic and natural, the relationship between sexual dysfunction and the type of opioid used was not assessed, primarily due to the small numbers. Hence, findings of a head-to-head comparison are not available. Overall, the pattern of sexual dysfunction associated with natural opium appears to be similar to that of other opioids.
This study found that older age was significantly associated with sexual dysfunction. However, age has not emerged as a significant predictor in logistic regression. This reflects that the association of age was possibly reflecting the prolonged opioid dependence and the greater severity of opioid dependence, rather than the age-related physiological changes. Similarly, older age was significantly associated with sexual dysfunction (Erectile dysfunction) in opioid-dependent individuals (mostly illicit or synthetic opioids) across various studies.5,35–37 However, a few Indian studies show contrasting results, indicating that age—despite having a mean age similar to our research—was not linked to sexual dysfunction among patients with opioid dependence. This variation may stem from differences in sample size, the cross-sectional design of the current study compared to the case-control approach, a longer duration of opioid dependence in our sample, and demographic factors, as well as the type of opioids used (natural opium in our study versus mixed opioids in earlier research).8,18
The tobacco use patterns that may influence sexual functioning were similar, with nearly 75% of patients exhibiting nicotine dependence in both groups of sexual dysfunction and non-sexual dysfunction based on ASEX.
In this study, sexual knowledge and attitudes were not associated with sexual dysfunction. The possible reasons might include the complex nature of sexual dysfunction in this group, influenced by multiple factors like hormonal imbalances, the severity of opioid dependence, and age. Biological factors may be more critical determinants in this population. However, this is an essential factor contributing to sexual dysfunction and engagement in high-risk sexual behavior, as reported in previous studies. 38
In this study, only one patient exhibited high-risk sexual behavior, which contrasts with previous research among opioid users, where about 40% of the sample reported having engaged in sex with a commercial sex worker or a casual partner. In natural opium users, complications and high-risk behaviors are significantly less.39,40 Natural opium users differ from users of other opioids in that they prefer to consume it orally rather than in injectable form. Their purpose of use is to help with hard physical work, and because it is culturally accepted, they are less involved in trafficking and high-risk behavior.
The suppressive effects of opioids on the hypothalamic-pituitary-gonadal axis, low testosterone, and the alpha-adrenergic blocking activity of opioids are potential biological causes of opioid-associated sexual dysfunction, in addition to their CNS depressant and sedative effects. 41 In addition, due to its lower potency, natural opium’s impact on opioid receptors and hormones can differ from that of synthetic opioids. 17 In this study, a considerable number of patients had low testosterone levels, with some also exhibiting low LH and FSH and elevated prolactin levels.
These findings align with similar studies reporting low testosterone in opioid users compared to non-users.13,14,37,41,42 Among hormones, only serum testosterone levels were significantly low in the sexual dysfunction group, negatively correlating with most ASEX domains. This suggests that reduced testosterone levels due to opium use may be a key factor in opioid-induced sexual dysfunction, notably decreased libido.
Similarly, Hallinan et al. found that lower total testosterone was associated with lower IIEF and EF domains in Men Receiving Methadone and Buprenorphine Maintenance Treatment. 5 Cepeda et al. also reported that participants on opioids had higher odds (odds ratio = 1.40) of experiencing low testosterone levels than those unexposed. 13 Hashim et al. reported lower LH and free testosterone levels in patients using heroin and tramadol, with heroin-dependent patients having significantly lower levels than those using tramadol; however, contrary to our findings, they found no significant association with sexual function domains. 42 Among patients with illicit opioid use, low total testosterone was detected in 17% of those reporting ED, but total testosterone was not significantly associated with ED. 35 A study conducted by Brown et al. found that 8.7% of the sample had testosterone levels below the cut-off level of 1.3 and also did not find correlations between testosterone or prolactin levels and sexual dysfunction in patients on methadone maintenance. 37
In this study, some patients showed elevated levels of LH, FSH, and testosterone. This could be a result of the body’s compensatory response to opioids affecting the hypothalamic-pituitary-gonadal axis, prompting increased hormone production. This condition, called hypergonadotropic hypogonadism, occurs when the testes do not produce enough testosterone despite high levels of LH and FSH from the pituitary gland (and hypothalamus). 43
Unlike the findings of Quaglio et al., 44 the present study found no association between sexual dysfunction and the duration of opioid dependence, which is consistent with other Indian studies.8,18 In contrast, sexual dysfunction was associated with greater severity of opioid dependence in the current study, with only the severity of opioid dependence identified as a significant predictor of sexual dysfunction. This finding aligns with results from Aggarwal et al., who also reported a higher rate of sexual dysfunction correlating with increased severity of dependence. 18 This association may be explained by the notion that patients with greater severity could have consumed larger amounts of opioids, leading to more gonadotropin suppression and continued use despite the harm.
Though the study provides insight into the frequency, patterns, correlates, and predictors of sexual dysfunction among a pure sample of natural opium users, it has several limitations. For example, the sample was derived from a single tertiary care center, and the absence of a control group limits the generalizability of the findings. The ASEX and the IIEF are intended for screening purposes, and the present study has not established a diagnosis through further evaluation, so it may have overestimated the prevalence. Being a cross-sectional study, it could not establish changes in sexual functioning over time or causal associations. Another limitation is the possibility of recall bias, lack of information from patients’ sexual partners, and the influence of couples’ personalities on sexual functioning was not assessed. Additionally, the dose-effect association was not evaluated, as measuring the exact dosage of natural opium was challenging due to its availability in various forms and strengths. The Majority of patients had consumed their morning dose of opium on the day of assessment. However, the possibility of a recent reduction in the opium dose over the last few months cannot be entirely excluded. This study also did not examine the impact of adulterants on sexual functioning that may be present in natural opium. Regression analysis was used to control for potential confounding factors and adjust for selection bias.
Overall, the effects of natural opium on sexual function, as highlighted in this study, are comparable to those of other categories of opioids, such as synthetic or semisynthetic opioids (Heroin, Buprenorphine, Methadone, etc.), even though these different categories of opioids are more potent. Although we could not find any studies on natural opium users, this research, despite its limitations, aimed to fill the literature gap by assessing sexual dysfunction among natural opium users and particularly by establishing an association between sexual dysfunction, the severity of dependence, and testosterone levels.
Conclusions
This study addresses a prevalent misconception that opium use boosts sexual performance, revealing instead that sexual dysfunction significantly impacts all areas of sexuality for those dependent on natural opium. As a result, regular assessments and immediate interventions are crucial for halting relapse and enhancing treatment adherence and outcomes. Future investigations should prioritize community-based research to explore beliefs surrounding natural opium’s influence on sexual health, along with longitudinal studies to assess its long-term effects and the impact of treating sexual dysfunction on patients’ overall well-being.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Consent to Participate
Written informed consent was obtained from all participants for their involvement in the study.
Consent for Publication
Written informed consent was obtained from all participants in the study for publication.
Data Availability
The deidentified participant datasets generated and/or analyzed during the current study are not publicly available but can be obtained from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Ethical approval was obtained from the Institutional Ethics Committee (IEC) of the All India Institute of Medical Sciences, Jodhpur, vide certificate number: AIIMS/IEC/2021/3387, dated March 12, 2021.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Institute provided the necessary funding for hormonal assessment; no external grants or funding were used in this study.
Prior Presentations
None.
Simultaneous Submission to Another Journal or Resource
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.