
Abstract
Background:
Transcranial electrical stimulation (tES) is a non-invasive neuromodulation technique increasingly recognized for its therapeutic potential in psychiatric disorders. Recent advances have enabled its administration in home settings, potentially increasing accessibility, reducing costs, and overcoming logistical barriers to in-clinic care. This scoping review systematically maps the preliminary evidence on home-based tES interventions for psychiatric disorders, while also assessing their feasibility, safety, and methodological trends.
Collection and Analysis of Data:
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR), we conducted a comprehensive literature search in PubMed and Scopus, covering publications from 2000 to 2024. Eligible studies examined the use of home-based tES (transcranial direct current stimulation [tDCS], transcranial alternating current stimulation [tACS]) for the treatment of psychiatric disorders. Extracted data included study characteristics, stimulation protocols, monitoring approaches, outcomes, and reported challenges. Forty-three studies met the inclusion criteria, comprising 19 randomized controlled trials (RCTs), 12 open-label studies, and 12 case series or case reports. These studies encompass various psychiatric conditions, with depressive disorder and mild cognitive impairment/dementia being the most frequently investigated. The majority of the studies utilized tDCS, often with remote supervision or digital support.
Conclusions:
Our review suggests high feasibility, good adherence, and minimal adverse effects, with potential symptom improvement across various disorders. However, small sample sizes, heterogeneity in protocols, and limited long-term data restrict the generalizability of results. Larger, methodologically rigorous trials are needed to establish efficacy, optimize stimulation parameters, and inform standardized guidelines for safe at-home tES use. Integration with telehealth systems and digital therapeutics may further enhance its scalability.
Keywords
Psychiatric disorders such as major depressive disorder, bipolar disorder, schizophrenia, and anxiety-related conditions contribute significantly to the global burden of disease, with many individuals experiencing chronic symptoms and functional impairment despite receiving standard treatments.1,2 Conventional therapeutic modalities, including pharmacotherapy and psychotherapy, are often limited by suboptimal adherence, treatment resistance, and accessibility barriers. In recent years, non-invasive brain stimulation (NIBS) techniques, particularly transcranial electrical stimulation (tES), have emerged as promising adjunctive or alternative strategies in managing these disorders.
The tES techniques include transcranial direct current stimulation (tDCS) and transcranial alternating current stimulation (tACS), which modulate cortical excitability by applying low-intensity electrical currents via scalp electrodes.3,4 Newer emerging tES modalities include transcranial random noise stimulation (tRNS), which acts via the application of randomly fluctuating current across a frequency range that may improve the sensitivity of neurons to weaker signals, and transcranial pulsed current stimulation (tPCS), which applies direct current in the form of pulses to modulate cortical excitability.5,6 The standard tES setup includes two electrodes placed over target scalp regions, secured with saline-soaked sponges or conductive gel. The current intensity typically ranges between 1 and 2 mA, with each session lasting 20–30 minutes. The effects may depend on both the polarity and duration of the stimulation, as well as the underlying brain state.4,7 Among these, tDCS has been the most extensively studied for psychiatric indications. When administered repeatedly over multiple sessions, tES has demonstrated the potential to alleviate symptoms in conditions such as depression, schizophrenia, and obsessive-compulsive disorder, with a favorable safety profile and minimal side effects.8–10
Recent technological advancements have enabled the development of portable, user-friendly, and remotely monitored tES devices, paving the way for home-based administration. This innovation addresses several critical challenges in psychiatric care, including limited access to specialized clinics, stigma associated with in-person treatments, and high drop-out rates. Home-based tES has the potential to increase adherence and continuity of care by empowering patients to self-administer treatment in familiar and convenient settings. Moreover, tele-supervision frameworks and safety monitoring protocols have evolved to ensure the feasibility, safety, and regulatory compliance of at-home use. 11
While the clinical utility of clinic-based tES is increasingly supported by randomized controlled trials and meta-analyses, the evidence base for home-based tES remains nascent and scattered across varying study designs and patient populations. 9 Given the growing interest in decentralized and personalized treatment models in mental health care, it is crucial to systematically map the existing literature on the use of home-administered tES in psychiatric disorders. A comprehensive synthesis will help identify the scope of clinical applications, effectiveness across diagnostic categories, common stimulation parameters, implementation practices, and prevailing knowledge gaps.
Accordingly, this scoping review aims to explore and summarize the current landscape of home-based tES interventions for treating psychiatric conditions. Specifically, we examine the study characteristics, clinical outcomes, stimulation protocols, modes of administration, safety considerations, and disorder-specific findings. By consolidating and contextualizing this emerging evidence, this review seeks to inform future clinical practice, guide research priorities, and support the development of scalable and accessible neuromodulation strategies in psychiatry. In this context, the present scoping review primarily aims to explore and summarize the current landscape of home-based tES interventions in treating psychiatric conditions. Specifically, we examine the study characteristics, clinical outcomes, stimulation protocols, modes of administration, safety considerations, and disorder-specific findings. By consolidating and contextualizing this emerging evidence, this review further seeks to inform future clinical practice, guide research priorities, and support the development of scalable and accessible neuromodulation strategies in psychiatry.
Methods
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. 12 as outlined in Figure 1 (See supplementary online material for PRISMA-ScR checklist). The review was initiated in February 2025 and ended in April 2025.

ADHD: Attention deficit hyperactivity disorder; BED: Binge eating disorder; MCI: Mild cognitive impairment; OCD: Obsessive-compulsive disorder; PTSD: Post-traumatic stress disorder.
Search Strategy
A comprehensive literature search was conducted in two electronic databases— MEDLINE (via PubMed) and Scopus—covering all publications up to 31 December 2024. The search strategy utilized a combination of free-text terms and Boolean operators to capture relevant studies. The search terms included: (“at home” OR “domiciliary” OR “home-based” OR “home administered” OR “remotely supervised” OR “home treatment”) AND (“transcranial direct current stimulation” OR “tDCS” OR “tES” OR “transcranial electrical stimulation” OR “transcranial alternating current stimulation” OR “tACS”). The search was restricted to articles published in the English language (Details in supplementary online material). References of relevant articles and reviews were also manually screened to identify additional eligible studies not captured in the initial search.
Eligibility Criteria
Studies were eligible for inclusion if they met the following criteria: (a) original research articles; (b) investigated the use of home-based tES (including tDCS or tACS) for the treatment or management of primary psychiatric disorders (as defined by DSM-5 or ICD-11); and (c) involved human participants. Studies focusing solely on neurological conditions (e.g., stroke, chronic pain, or epilepsy), animal models, or healthy individuals were excluded. Additionally, opinion papers, editorials, and review articles were excluded from this review.
Study Selection
The review was conducted using the Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia). Duplicate records were initially identified and removed automatically by Covidence, followed by manual verification by the reviewers to identify and remove any remaining duplicates. Subsequently, two independent reviewers (the first author and the second author) screened all identified titles and abstracts for relevance. Full-text articles were subsequently retrieved for studies meeting the initial eligibility criteria or where relevance could not be determined from the abstract alone. Disagreements regarding study inclusion were resolved through discussion until a consensus was reached.
Data Extraction and Synthesis
After removing duplicates, a total of 352 unique records were identified. Following title and abstract screening, 244 articles were excluded due to irrelevance (e.g., studies not involving home-based tES, studies not addressing psychiatric disorders, or review/opinion articles). The remaining 108 articles were assessed in full text. An additional 65 studies were excluded at this stage. Ultimately, 43 studies met the inclusion criteria and were included in the final synthesis (Supplementary Figure 1). 13
The extracted data were organized and synthesized descriptively, focusing on study design, population characteristics, psychiatric diagnoses, stimulation protocols, remote supervision mechanisms, outcome measures, and reported efficacy and safety outcomes.
Results
A total of 43 studies investigating home-based tES for psychiatric disorders were included in the review (Table 1).14–56 Of these, 19 were randomized controlled trials (RCTs),15,21,22,24,26,29,31,34,36,39,41,42,46,49–51,53,54,56 12 were open-label studies,20,27,32,33,35,37,38,40,43,45,47,52 and the remaining 12 were case reports or case series.14,16–19,23,25,28,30,44,48,55 Sixteen studies focused specifically on depressive disorders,22–24,27,28,30,31,33,34,37,38,43,45,46,51,56 while four examined bipolar depression,19,26,47,52 and one included participants with both unipolar and bipolar depression. 20 Additional studies addressed other psychiatric and neurodevelopmental conditions: one study targeted individuals with mild cognitive impairment (MCI) and co-morbid depression, 49 and a case series included treatment-resistant depression along with bipolar affective disorder (BPAD) and fibromyalgia. 18 Schizophrenia was the focus of four studies,14,17,44,48 two studies evaluated binge eating disorder (BED),50,53 and a single study explored the utility of tES in obsessive-compulsive disorder (OCD), 36 attention deficit/hyperactivity disorder (ADHD), 29 post-traumatic stress disorder (PTSD), 35 and Prader-Willi syndrome with intellectual disability. 16 Furthermore, 10 studies focused on MCI and various forms of dementia, such as AD, vascular dementia, and frontotemporal dementia (Figure 1).15,21,25,32,39–42,54,55
Studies on Home-based tES in Psychiatry.

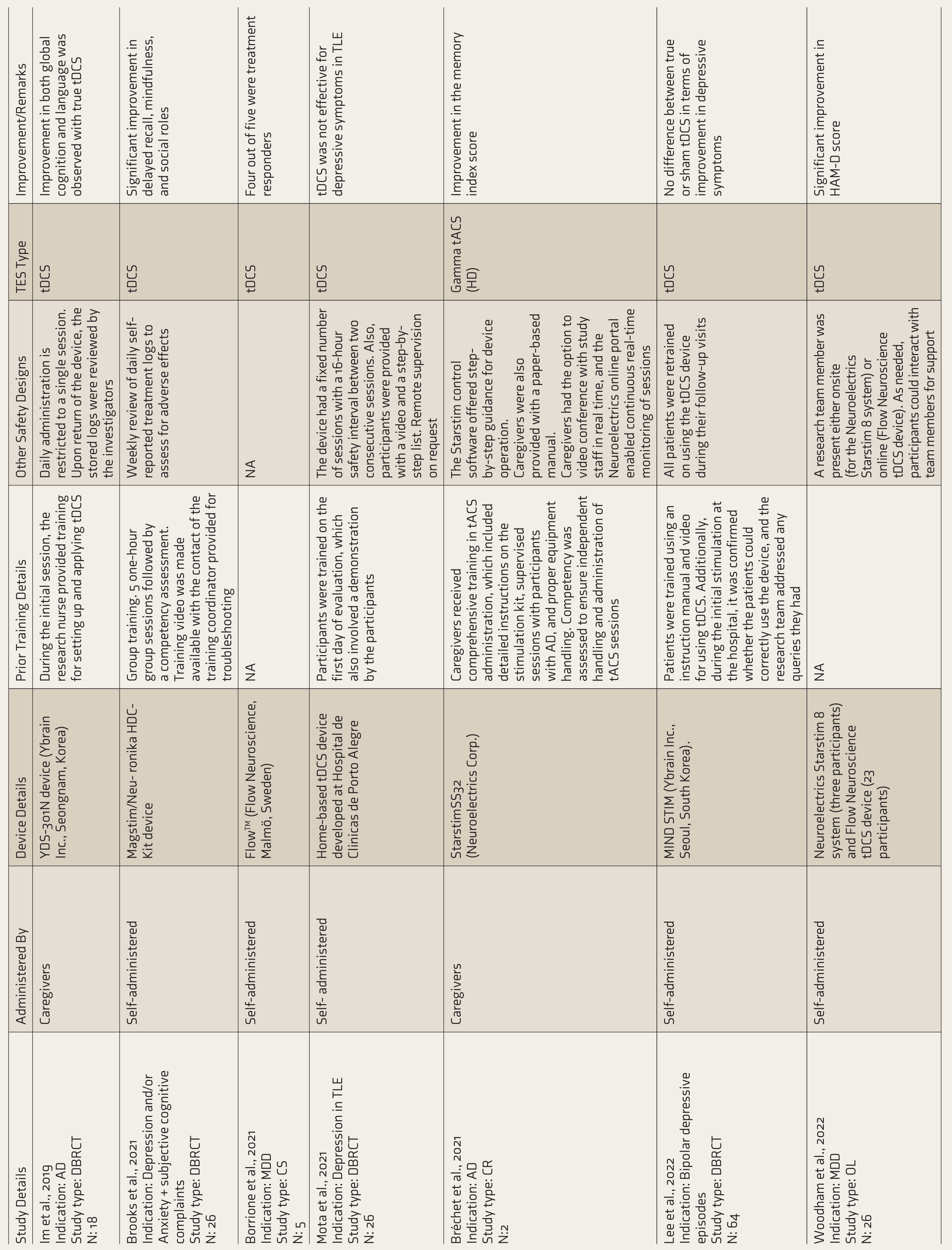



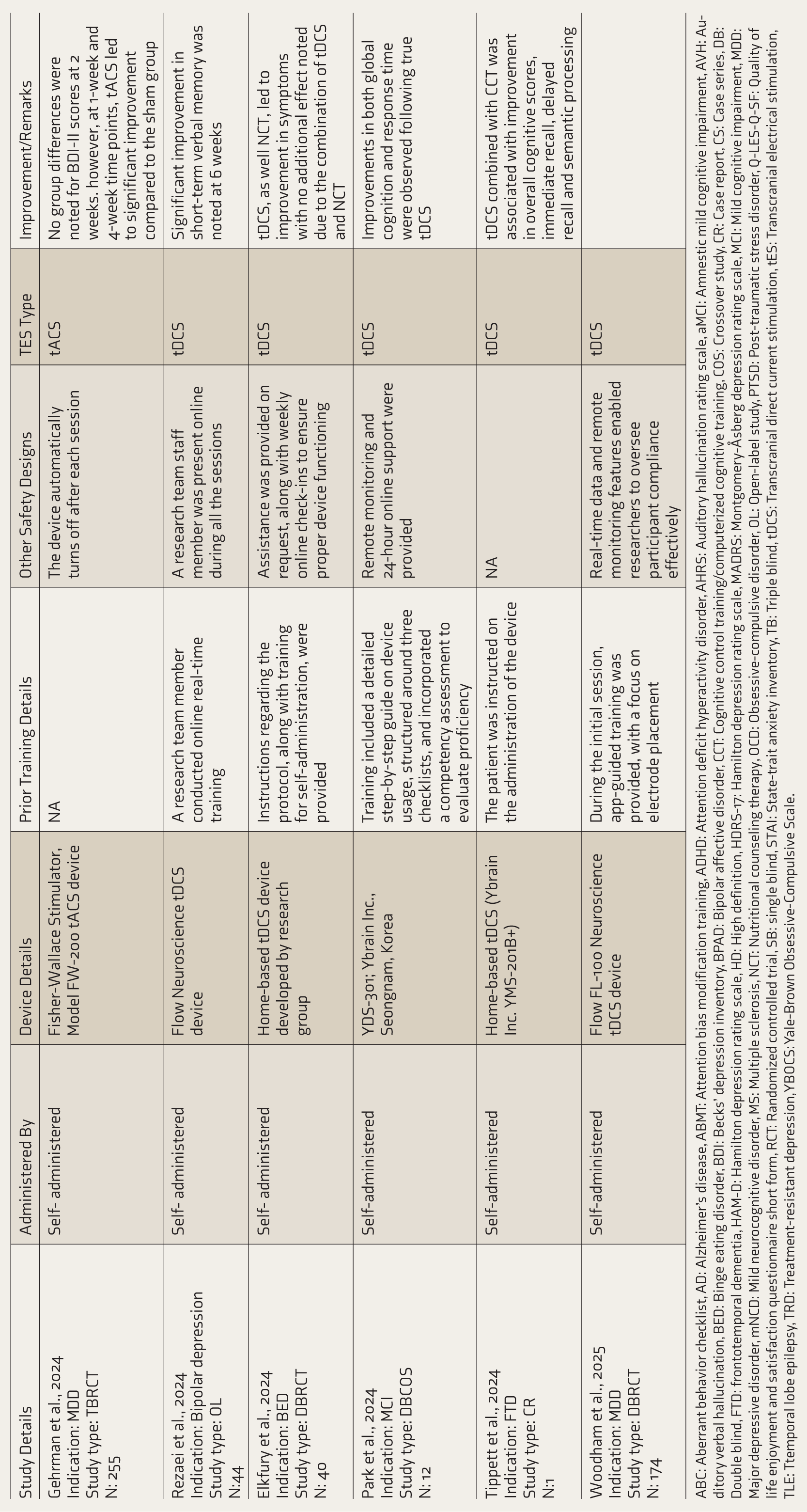
ABC: Aberrant behavior checklist, AD: Alzheimer’s disease, ABMT: Attention bias modification training, ADHD: Attention deficit hyperactivity disorder, AHRS: Auditory hallucination rating scale, aMCI: Amnestic mild cognitive impairment, AVH: Auditory verbal hallucination, BED: Binge eating disorder, BDI: Becks’ depression inventory, BPAD: Bipolar affective disorder, CCT: Cognitive control training/computerized cognitive training, COS: Crossover study, CR: Case report, CS: Case series, DB: Double blind, FTD: frontotemporal dementia, HAM-D: Hamilton depression rating scale, HD: High definition, HDRS-17: Hamilton depression rating scale, MADRS: Montgomery-Åsberg depression rating scale, MCI: Mild cognitive impairment, MDD: Major depressive disorder, mNCD: Mild neurocognitive disorder, MS: Multiple sclerosis, NCT: Nutritional counseling therapy, OCD: Obsessive-compulsive disorder, OL: Open-label study, PTSD: Post-traumatic stress disorder, Q-LES-Q-SF: Quality of life enjoyment and satisfaction questionnaire short form, RCT: Randomized controlled trial, SB: single blind, STAI: State-trait anxiety inventory, TB: Triple blind, tDCS: Transcranial direct current stimulation, tES: Transcranial electrical stimulation, TLE: Ttemporal lobe epilepsy, TRD: Treatment-resistant depression, YBOCS: Yale-Brown Obsessive-Compulsive Scale.
Regarding the stimulation modality, most studies employed tDCS, with only five using tACS.25,36,40,41,51 Stimulation intensities ranged from 1.5 to 3 mA, with session durations between 20 and 30 minutes. The montage differed depending on the disorder and targeted symptoms; however, the dorsolateral prefrontal cortex (DLPFC) was the most frequently targeted region (Table 2). Devices varied widely, encompassing certified commercial units and indigenously developed systems.
tES Protocols Across Studies.
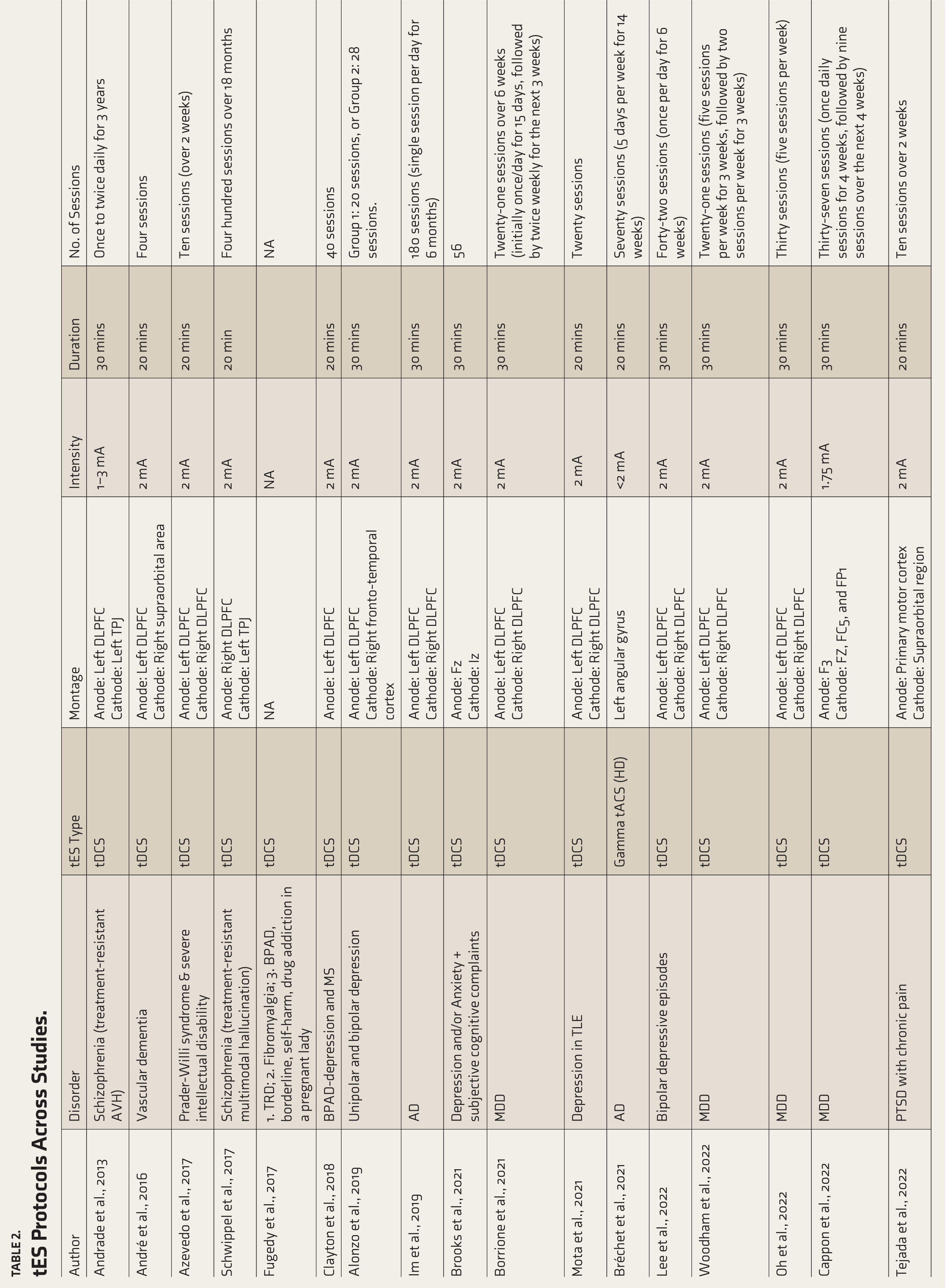
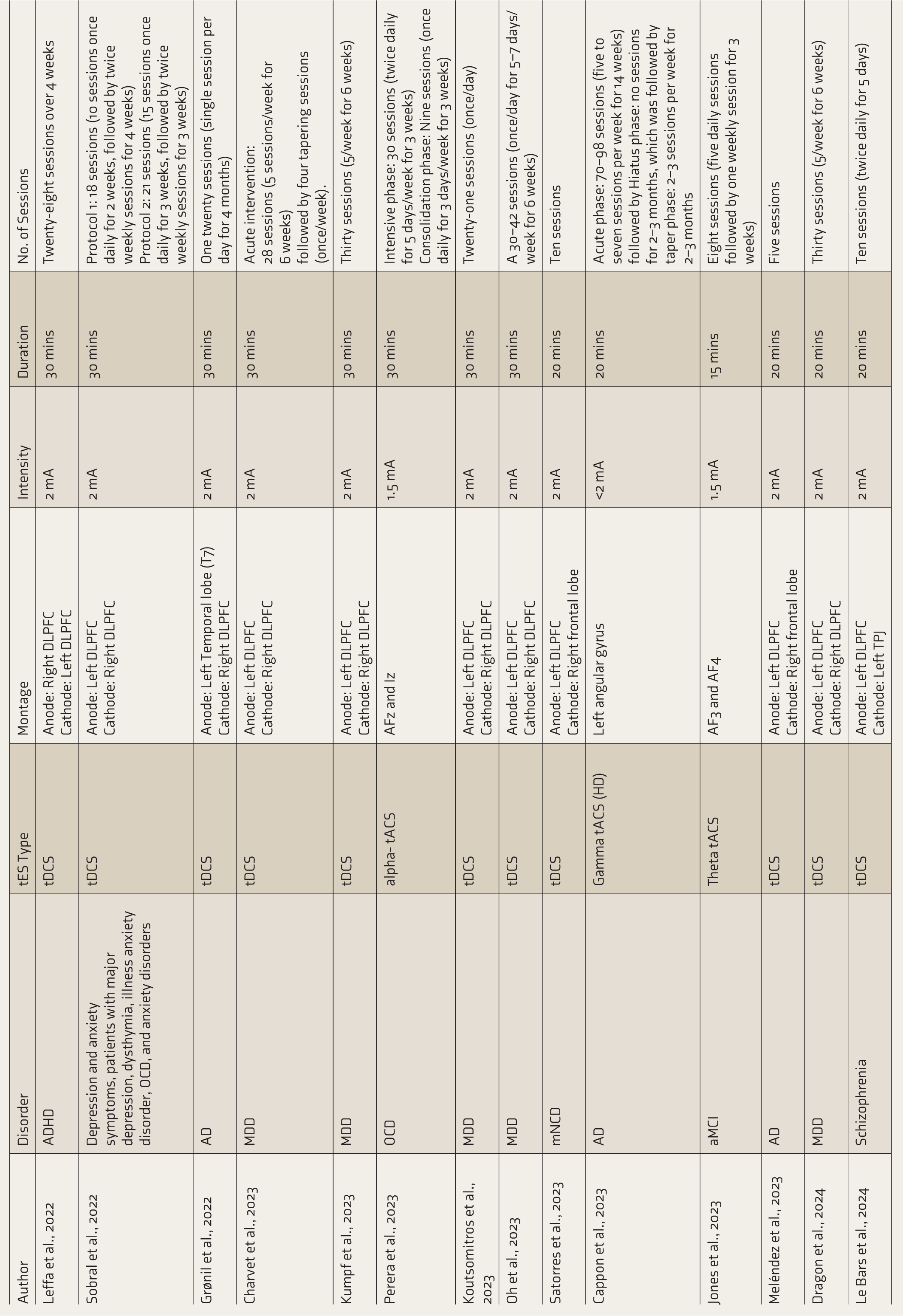

AD: Alzheimer’s disease, ADHD: Attention deficit hyperactivity disorder, aMCI: Amnestic mild cognitive impairment, AVH: Auditory verbal hallucination, BED: Binge eating disorder, BPAD: Bipolar affective disorder, FTD: Frontotemporal dementia, HD: High definition, MCI: Mild cognitive impairment, MDD: Major depressive disorder, mNCD: Mild neurocognitive disorder, MS: Multiple sclerosis, OCD: Obsessive-compulsive disorder, PTSD: Post-traumatic stress disorder, tDCS: Transcranial direct current stimulation, tES: Transcranial electrical stimulation, TLE: Temporal lobe epilepsy, TRD: Treatment-resistant depression.
Using the Oxford CEBM scale, 57 19 randomized controlled trials were classified as Level 2b evidence, while the remaining studies (open-label trials, case series, and case reports) were rated as Level 4. A substantial proportion of the studies (24 out of 43) were open-label or case series/case reports without blinding. Furthermore, 12 of the case series/case reports included only 1–8 participants.
Therapeutic Outcome in Psychiatric Disorders
Schizophrenia
In schizophrenia, four case reports described the use of home-based tDCS in individuals with treatment-resistant auditory verbal hallucinations. Improvements were noted in some cases, such as a 16% reduction in hallucinations after 10 sessions, 44 and up to 90% symptom relief with maintenance tDCS over a period of 2–3 years. 14 Another case noted sustained benefits following 20 sessions, 48 although one report found no sustained improvement despite 400 sessions. 17
Depression
For depressive disorders, a substantial number of studies reported symptom reductions following home-based tDCS, typically involving 18–72 sessions.20,22,23,27,28,30,31,33,34,37,38,43,45,51,56 Among the RCTs assessing the effect of tDCS on unipolar depression, four RCTs reported improvement in symptoms,22,31,34,56 while two RCTs failed to demonstrate significant improvement, including one involving participants with co-morbid temporal lobe epilepsy.24,46 In contrast, all the case reports, case series, and open-label studies reported significant improvement in depressive symptoms in unipolar disorder. In the only RCT using alpha tACS, no significant improvement was noted. 50
In bipolar depression, mood symptoms improved in several case reports and open-label studies,19,20,47 along with cognitive gains.19,52 However, an RCT found no difference between active and sham conditions. 26
The MCI and dementia: In patients suffering from MCI and dementia, most studies have focused on MCI and AD, except for two studies, one each on vascular dementia (VD) 15 and Frontotemporal Dementia (FTD). 55 The number of sessions ranged from four sessions 15 to 180 sessions (over 6 months). 21 Of the RCT studies administering tDCS to participants with MCI and AD,21,39,42,49,54 three reported improvement across various domains, including global cognition, immediate and delayed memory, and language. However, one of the RCTs reported improvement in cognitive symptoms. 49 Moreover, one of the open-label studies with tDCS sessions administered daily for 4 months reported no change in cognitive measures. 32 In patients with VD, 15 an RCT reported significant improvement in short-term memory and verbal working memory with tDCS. While in FTD, 55 a case report noted significant improvement in overall cognition, along with immediate and delayed recall, after tDCS administration. Among the three studies administering tACS, two were non-RCTs (an open-label study and a case report) and used gamma-frequency stimulation.25,40 Both studies reported improvements in memory deficits. Similarly, in an RCT using theta-frequency stimulation, 41 improvement in memory deficits was observed.
OCD
In OCD, one RCT found a significant reduction in both obsessions and compulsions after 39 sessions of individualized home-based tACS. 36
PTSD
In an open-label trial involving patients with PTSD and chronic pain, 10 sessions of home-based tDCS yielded significant clinical improvement. 35
ADHD
A double-blind RCT in adults with ADHD found that 28 sessions of tDCS over 4 weeks led to improvements in attention regulation. 29
BED
For BED, two RCTs demonstrated reductions in binge eating episodes after 10–23 sessions.50,53
Intellectual Disability
In a case report on Prader-Willi syndrome with intellectual disability, approximately 50% improvement was reported in food cravings and behavioral disturbances. 16
Training, Supervision, and Administration
The majority of studies (33 out of 43) highlighted the importance of prior training before initiating home-based tES. In contrast, 10 studies did not provide any information regarding training protocols.14–16,19,23,27,34,39,42,50 Training protocols varied across studies; however, they consistently included step-by-step demonstrations of device operation and the proper administration of tES by trained personnel. In addition, several studies provided detailed instruction manuals, video tutorials, and live supervision—either in-person or remote—during the initial sessions. Some also mandated that users successfully complete competency assessments before being allowed to administer tES independently.20,25,30,36,40,48,54 Only a few studies (8 out of 43) specifically report daily monitoring of sessions,27,35,36,43,47,50,52,56 while others describe it as on-demand or as-needed online supervision. The majority of studies reported self-administration of tES at home, often under remote supervision.17–20,22–24,26–29,31,33–38,41,43,45–47,49–56 However, in 11 studies, the stimulation was administered by a clinician or a caregiver, specifically in cases of schizophrenia,14,44,48 MCI and dementia,21,25,32,39,40,42 Prader-Willi syndrome, 16 and one study on major depressive disorder. 30
Tolerability and Adverse Effects
Across studies, tES was generally well tolerated, with most adverse effects (AEs) being mild and transient (Table 3). Among 43 studies, seven did not report AEs,21,35,42,44,49,53,55 while the rest reported AEs. Most of the studies used a structured questionnaire, such as the tDCS adverse event questionnaire, to assess the AEs, either administered after each session27,46–48,52,56 or at predetermined time points.29,45 Some of the studies relied on subjective self-reporting of AEs.38,43,50,51 In a few studies, although AEs were assessed, the frequency of assessment as well as the method of reporting was unclear.14,16,19,31,36,39 The most frequently observed AEs with tDCS include tingling sensations, skin redness, itching, and mild burning or heat sensations at the electrode sites. These effects are typically experienced during or immediately following stimulation and are often localized to the scalp. For instance, Alonzo et al. (2019) found that tingling (22.3%), burning (45.3%), redness (22.6%), and itching (18.5%) were among the most common AEs, while other studies, such as those by Cappon et al., 30 Rezaei et al., 52 and Ghazi-Noori et al. 47 reported similar findings with high rates of mild sensations under the electrodes. Several studies, such as those conducted by Azevedo et al., 16 Schwippel et al., 17 and Pathak et al., 48 reported no adverse events, further underscoring the general safety of the intervention. Nevertheless, some studies reported more notable reactions. For example, Mota et al. 24 observed burning sensations in 63.7% of participants in the active group, while Leffa et al. 29 reported scalp burns and dizziness, leading to participants’ withdrawal from the study. Rare yet significant events included mild electrical burns, 31 skin lesions, 34 and a single reported fall. 22 Although these events were uncommon, they highlight the importance of correct electrode application and monitoring, particularly during the ramp-up phase. In terms of psychological effects, some studies26,56 tracked mood changes and psychiatric symptoms, with no evidence of treatment-emergent mania or hypomania. One study, 26 did report suicidal ideation and an episode of aggression in both active and sham groups, indicating no clear causal relationship with tDCS.
Similarly, in tACS studies,25,36,40,41,51 no major AEs were noted. Minor AEs, such as phosphenes, tingling sensations, itching, headaches, and sleepiness, were observed. Overall, most studies found that AEs were not serious and did not interfere with treatment.
Tolerability and Adverse Effects.
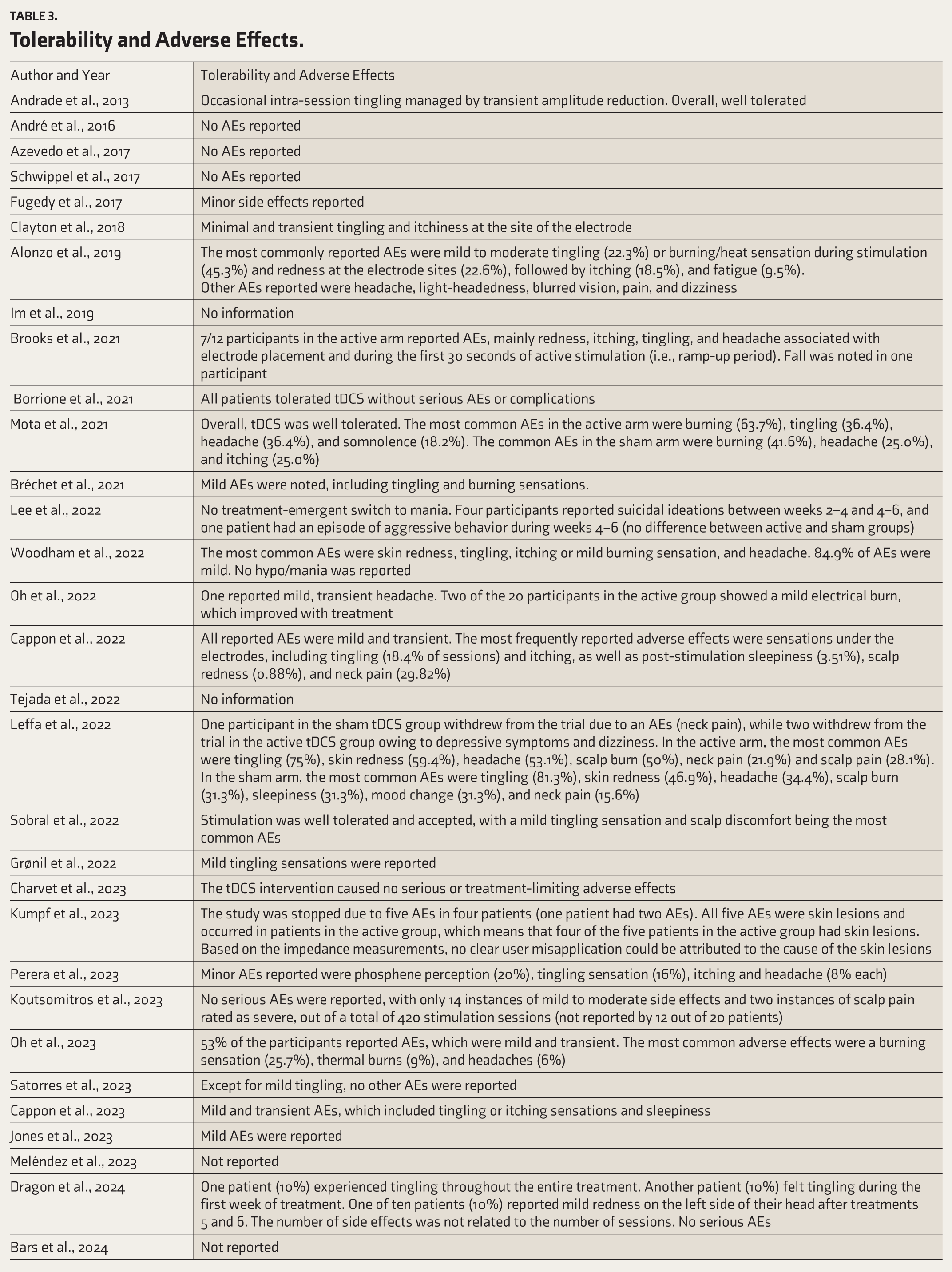

AE: Adverse effects, tDCS: Transcranial direct current stimulation, YMRS: Young Mania Rating Scale.
Discussion
Over the last decade, there has been a steady and increasingly systematic interest in the development and implementation of home-based or remotely supervised tDCS protocols, particularly for individuals with chronic or treatment-resistant neuropsychiatric disorders. The rationale behind this shift stems from several factors: the logistical limitations of in-clinic stimulation protocols, the need for prolonged and frequent sessions to optimize treatment, and the growing demand for patient-centered, accessible care, particularly among populations facing mobility, cognitive, or geographic barriers. The studies reviewed here span diverse clinical populations, including schizophrenia, major depressive disorder (MDD), bipolar depression, ADHD, OCD, MCI dementia, BED, and PTSD, and demonstrate a wide array of implementation strategies aimed at enabling safe, effective, and scalable delivery of neuromodulation in non-clinical settings. Notably, no eligible trials investigated generalized anxiety or pediatric populations, underscoring significant evidence gaps in the anxiety-spectrum and developmental conditions.
One of the central features of these studies is the emphasis on feasibility and safety, which are foundational to the acceptability of home-based tDCS. In many cases, researchers and clinicians developed detailed protocols to ensure that devices could be operated safely by patients or caregivers. This included multi-tiered training procedures, often beginning with in-person or virtual instructional sessions that provided both didactic information and hands-on demonstrations. Several studies employed practice sessions using mannequin heads or dummy devices before transitioning to live use. For example, Charvet et al.11,33 and Perera et al. 36 structured training to include both individual and caregiver education, verification of correct electrode placement, and test sessions supervised via video conferencing tools. Studies such as that by Andrade et al. 14 and Pathak et al. 48 involved long-term treatment administered by trained family members in low-resource settings, demonstrating that even without advanced telemonitoring infrastructure, safety could be maintained through careful education and adherence to conservative protocols.
The equipment used in these studies ranged from simple indigenous devices, typically seen in Indian case series and open-label studies, to sophisticated CE-certified or FDA-cleared devices such as those developed by Neuroelectrics, Soterix Medical, and Flow Neuroscience. While indigenous devices allowed for broader access and adaptability in resource-limited settings, certified systems offered pre-programmed parameters, locked protocols, and integrated compliance monitoring. Several devices required session unlock codes provided by the research team, thereby ensuring structured dosing and preventing overuse. Others incorporated cloud-based data logging, remote monitoring dashboards, or real-time video supervision to track adherence and manage technical or clinical issues as they arose. These features were particularly prominent in studies conducted in the US and Europe, where regulatory oversight and institutional infrastructure supported high-tech implementations.
Across these various systems, the stimulation parameters were relatively consistent, centering on anodal stimulation at the left dorsolateral prefrontal cortex (DLPFC) with current intensities of 1.5–2 mA for 20–30 minutes per session. Treatment schedules typically involved daily sessions (Monday through Friday) over periods of 2–8 weeks, often with optional tapering phases or maintenance sessions that extended beyond the initial intervention period. Some studies administered up to 56 sessions in conditions such as treatment-resistant depression 22 or up to 3 years in chronic schizophrenia, 14 where long-term modulation might be necessary to achieve or sustain symptom improvement.
Clinical outcomes varied by condition but were generally favorable, particularly in affective disorders. In MDD, several studies demonstrated significant symptom reduction and high rates of response and remission. For instance, in Charvet et al. 33 , which examined remotely supervised home-based tDCS for MDD, 88% of participants met response criteria, and 81% achieved remission, a striking result suggesting that home-based administration can be as effective, if not more so, than traditional in-clinic interventions. Similarly, Ruffini et al. 45 found a median reduction of 64.5% in MADRS scores across a naturalistic outpatient sample using a CE-certified home kit. Studies targeting PTSD, 35 ADHD, 29 and OCD 36 also reported moderate improvements, although results were more heterogeneous and often limited by small sample sizes or lack of control conditions.
In schizophrenia, home-based tDCS has been explored as an adjunctive treatment for persistent symptoms such as auditory hallucinations and negative symptoms. A case report 14 by Andrade et al. detailed the use of caregiver-administered tDCS over an extended period of more than 3 years. This case report, while uncontrolled, documented clinically meaningful improvements in symptom severity and social functioning, with minimal side effects. This also underscored the practical importance of caregiver involvement in populations with cognitive or functional impairments that preclude independent use of the device. Other schizophrenia-focused studies, such as those by Pathak et al., 48 employed both left DLPFC and temporoparietal junction montages, adapting stimulation targets based on symptom profiles (e.g., targeting auditory hallucinations versus cognitive symptoms). Despite promising results, the need for rigorous RCTs remains, as most data in this domain still derive from open-label or case-series designs.
The application of home-based tES, particularly tDCS and tACS, has shown promise in addressing cognitive deficits in patients with MCI and various forms of dementia. While the majority of studies have focused on MCI and AD, limited but encouraging evidence also exists for other dementia subtypes such as VD and FTD.15,55 The number of stimulation sessions varied considerably across studies. Notably, five out of ten studies administered tES over extended durations ranging from 2.5 to 6 months.21,25,32,40,55 While most reported improvements in cognitive measures, outcome variability persists, evident in one 4-month study 32 that found no significant cognitive benefits. Similarly, all three identified tACS studies—two using gamma and one using theta frequency—demonstrated memory enhancement.25,40,41 These findings, though preliminary, underscore the therapeutic potential of tES in neurodegenerative conditions. The limited efficacy of current pharmacological treatments, including sensitivity to psychotropic medications, combined with the need for long-term interventions and the generally favorable tolerability of non-invasive brain stimulation, makes home-based tES an attractive and feasible adjunctive therapy.
Importantly, safety outcomes across all studies were highly reassuring. No serious adverse events were reported in any of the trials reviewed. Minor side effects, such as transient scalp tingling, skin redness, or mild headaches, were generally self-limiting and did not necessitate treatment discontinuation. Compliance was also high in most studies, particularly those with robust supervision frameworks. Real-time or asynchronous monitoring, regular follow-up, and easy access to technical support likely contributed to these outcomes, in addition to the inherent tolerability of low-intensity tDCS itself.
Overall, the accumulated evidence supports the conclusion that home-based or remotely supervised tDCS is both feasible and safe across a range of neuropsychiatric conditions. The variability in clinical outcomes—particularly in conditions like ADHD and schizophrenia—points to a need for more standardized protocols, larger and better-controlled trials, and deeper exploration of patient-specific factors that may influence treatment response. Nevertheless, these studies collectively demonstrate that with appropriate training, monitoring, and device safeguards, home-based neuromodulation represents a viable and potentially transformative approach to long-term management of chronic mental health conditions. As technology advances and digital health platforms evolve, such interventions are poised to play a larger role in personalized, accessible psychiatric care.
Across the 43 studies included, there was a wide variation in study design and methodological rigor. Nineteen randomized controlled trials were classified as Level 2b evidence according to the Oxford CEBM scale. The remaining 24 studies were rated as Level 4, comprising 12 open-label trials and 12 case reports or case series. The open-label trials typically lacked blinding, and the case series and case reports were descriptive in nature, with no control groups. Several methodological limitations were common across studies. Sample sizes were generally small, with a median of 24 participants. Many open-label and case series studies enrolled only a few participants, with 12 case reports/series including between 1 and 8 individuals. In addition, most studies lacked sham controls, limiting the ability to account for placebo effects. The majority of studies employed short follow-up periods, often limited to immediate or short-term post-intervention assessments, providing little insight into the durability of effects. A large proportion relied on self-reported outcome measures, which are more susceptible to subjective bias and expectancy effects compared to objective measures.
At-home neuromodulation raises important ethical and regulatory considerations that extend beyond clinical efficacy.4,11,58 Informed consent must be robust, ensuring participants understand the potential risks, benefits, and their responsibilities, particularly about competence in self-administration, as well as avoiding any unintended use. Devices should be equipped with tamper-proof locks and pre-set safety parameters to prevent unauthorized adjustments. 11 Data privacy and security are critical, requiring compliance with relevant regulations such as the EU General Data Protection Regulation (GDPR) and the US Health Insurance Portability and Accountability Act (HIPAA) for secure handling of health information. 58 Regulatory oversight varies across jurisdictions, with frameworks such as the US Food and Drug Administration’s 510(k) clearance process and the European Union’s Medical Device Regulation (MDR) setting distinct approval and monitoring requirements. Clear, jurisdiction-specific guidance is essential to ensure safe, ethical, and compliant use of at-home tES devices.
To enhance safety, adherence, and protocol fidelity, practical supervision models include:
This scoping review has several strengths, including the use of a comprehensive search strategy across multiple databases. Moreover, the methodology was based on the PRISMA-ScR guideline to ensure reproducibility. A key strength of this review is its inclusion of a wide range of psychiatric disorders, providing a broad overview of the current literature on home-based tDCS and highlighting the critical gaps that can inform future research. However, this review has some limitations. The inclusion was restricted to published English-language studies. Additionally, the descriptive approach and variability among the included studies limit the ability to perform comparisons or draw definitive conclusions. Furthermore, the literature search was limited to two major databases, which, although widely used, may not have captured all relevant studies. While reference lists of included articles and related reviews were manually screened to identify additional sources, the possibility of missing pertinent literature cannot be ruled out.
Conclusions
Home-based tES represents a promising and innovative approach to expanding access to non-invasive neuromodulation therapies for psychiatric disorders. While preliminary findings are encouraging, the clinical uptake will depend on generating more robust, standardized, and long-term evidence.
Future development of home-based tES is likely to be shaped by advances in digital health technologies. Computer vision–based mobile applications can support precise electrode placement through real-time visual guidance. Adaptive AI algorithms may facilitate individualized dose finding, adjusting stimulation parameters based on treatment response and tolerability. Integration with wearable devices—such as EEG headbands or physiological sensors—could enable on-demand stimulation triggered by relevant neurophysiological or symptom changes. These innovations, coupled with secure cloud-based monitoring, hold the potential to enhance precision, scalability, and safety in at-home neuromodulation.
Call to Action
Researchers: Conduct multi-site randomized controlled trials with ≥6-month follow-up, including factorial designs (e.g., 1 mA vs. 2 mA) and cost-effectiveness implementation studies.
Clinicians: Adopt standard remote monitoring procedures and contribute to adverse event registries to improve safety surveillance.
Regulators: Develop risk-stratified device guidance, harmonizing standards across jurisdictions (e.g., US FDA 510(k) and EU MDR).
With coordinated action, home-based tES can evolve from promising innovation to a safe, scalable tool in psychiatric care.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
HP is supported by the Department of Biotechnology (DBT) - Wellcome Trust India Alliance (IA/CRC/19/1/610005). VSS acknowledges the support of the Indian Council of Medical Research (ICMR) Investigator-initiated research grant (2022-1614), NIMHANS Intramural Research grant and Life Sciences Research Board (LSRB/01/15001/LSRB-416/LS&BD/2024). GV acknowledges the support of the Department of Biotechnology (DBT) - Wellcome Trust India Alliance (IA/CRC/19/1/610005).
Data Sharing Statement
The data will be made available upon reasonable request to the corresponding author. Proposals should be submitted to
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethical Approval
As this study was a scoping review based on previously published literature, it did not involve human participants or identifiable data. Therefore, ethical approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.