
Abstract
Purpose of the Review:
Pharmacological and psychological therapies are the main approaches for managing anorexia nervosa (AN). Recent advances in etiology and functional pathways in the brain have opened the gateway for assessing brain-focused treatment. Noninvasive techniques such as repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS) have been researched for potential benefits. This systematic review and meta-analysis explored the effects of rTMS and tDCS on AN with respect to eating behavior, body mass index (BMI), and comorbid symptoms.
Collection and Analysis of Data:
Electronic database searches were conducted based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines using the following keywords: eating disorders, anorexia nervosa, neurostimulation, repetitive transcranial magnetic stimulation, rTMS, and transcranial direct current stimulation, tDCS. The study included articles published in English until December 2024. The data extracted from the studies included author details, year of publication, type of study design, type of stimulation, stimulation methods, sessions, outcomes, and comorbid symptoms. A total of 20 studies were included in the review; 16 used rTMS, and four used tDCS. Five studies were included in the meta-analysis. The dorsolateral prefrontal cortex (DlPFC) was the main target area for neurostimulation. One study targeted the bilateral dorsomedial prefrontal cortex, right inferior parietal lobe, and insula. The meta-analysis revealed increased BMI following rTMS (standardized mean difference [SMD] = 0.174, 95% confidence interval [CI]: −0.201 to 0.548, p = .363). The Eating Disorder Examination Questionnaire score decreased (SMD = 0.231, 95% CI: −0.204 to 0.671, p = .304), and there was a significant reduction in comorbid depression (SMD = −0.501, 95% CI: −0.941 to −0.053, p = .030) and anxiety (SMD = −0.461, 95% CI: −0.892 to −0.025, p = .040). Studies involving tDCS showed potential improvement in BMI, core symptoms of AN, and its associated symptoms.
Conclusion:
Noninvasive neurostimulation has shown improvement in the symptoms of AN and BMI, although meta-analyses have not yet demonstrated robust effects. In contrast, more substantial evidence supports its efficacy in alleviating mood symptoms. Further research is needed to understand the underlying mechanisms, optimize targets, and refine stimulation parameters, which are crucial for developing effective brain-targeted interventions.
Keywords
The term “feeding and eating disorders” refers to abnormal eating or feeding patterns. 1 The clinical description of anorexia nervosa (AN) and bulimia nervosa (BN) dates back to the 16th century in the Western nations,2,3 whereas in India, it was in the late 20th century. 4 The majority of literature on eating disorders (EDs) comes from Western nations. This void in the literature could be attributed to the cultural impact on food preference, body image concerns, nutrition, and variation in clinical presentation. This has been termed a “nonfat phobic” variant of AN. 4 Over the past 10 years, the publications on EDs and subclinical EDs have increased. 5 Studies from various countries revealed the overall lifetime prevalence of any ED was 1.01%, and those of AN, BN, and binge eating disorder were 0.21%, 0.81%, and 2.22%, respectively. 6 The frequency of disordered eating/probable ED in India ranged from 1.25% to 45.4%. 4
AN is a severe ED where patients’ deliberate weight loss is induced and maintained. This illness is linked to specific psychopathology, where a persistent, intrusive thought of excessive fear of gaining weight occurs. 7 Both mental and physical comorbidities are typical in EDs; the most prevalent psychiatric comorbidities are mood and anxiety disorders. 8 Standard management is predominantly non-pharmacological therapies, such as enhanced cognitive behavior therapy, cognitive remediation therapy, AN exposure and response prevention, acceptance and commitment therapy, and dialectical behavioral therapy. Nutritional therapy is also included in management, and pharmacological agents have been researched and documented. 9
Advances in neuroscience have shifted our understanding of EDs from primarily social and psychological factors to biological and evidence-based models. 10 An imbalance between reward-related and cognitive control/inhibitory-related brain pathways is at the heart of several neural-based models of EDs. 11 Both structural and functional alterations in the frontal cortex and insula, which are linked to reward and anxiety processing, may influence the development of EDs. 12 This opens an array of possible uses for neurostimulation in EDs. More recent neurostimulation treatments include noninvasive techniques like repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS). 13 High-frequency rTMS enhances neural activity, while low- frequency rTMS suppresses it by inducing long-term potentiation and long-term depression in neural systems. In tDCS, a low-intensity current is applied via electrodes to modulate synaptic plasticity by enhancing or diminishing synaptic transmission. 14 Neurostimulation methods may target specific brain networks or areas to reduce symptoms. They have different mechanisms of action than pharmacotherapy, which gives them scope to treat people who do not respond to drugs. Additionally, they have fewer adverse effects than pharmacotherapy. Neurostimulation as a management option in AN is the least explored area in the world. The main objective of this review is to provide comprehensive data from the literature on the efficacy of rTMS and tDCS in terms of body mass index (BMI), severity of core symptoms, and comorbid symptoms.
Methods
Protocol Registration
A systematic review was carried out and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards. 15 The study was registered in the global systematic review database PROSPERO (CRD42024514659).
Eligibility Criteria
The review included articles published in the English language, including randomized controlled trials (RCTs), clinical trials, clinical studies, case series, and case reports. The study investigated the effect, outcome, and adverse effects of noninvasive neurostimulation techniques (rTMS and tDCS) on AN. Exclusion criteria were studies on subclinical EDs and other EDs. Studies that did not report eating- related outcomes as a result of noninvasive neurostimulation, animal studies, and studies investigating other forms of neurostimulation techniques on AN, such as invasive techniques such as deep brain stimulation and vagal nerve stimulation, were excluded from this literature review. The study also excluded review articles, book chapters, unpublished data, short communications, letters to the editor, and abstracts.
Literature Search, Screening, and Selection Process
A comprehensive literature search was undertaken in electronic databases such as Medline through PubMed, Embase, Scopus, Cochrane Library, Web of Science, and Google Scholar using the keywords and MeSH terms, that is, “Eating disorders,” “Anorexia nervosa,” “Neurostimulation,” “Repetitive Transcranial Magnetic Stimulation,” “rTMS,” “Transcranial Direct Current Stimulation,” “tDCS,” and “Body Mass Index,” through appropriate Boolean operators (AND, OR). An internet search was also done for relevant papers and articles. Citation tracking was performed to identify more relevant articles. All the articles published before December 2024 were included. The initial search yielded 1,420 articles (Supplementary Tables 1 and 2).
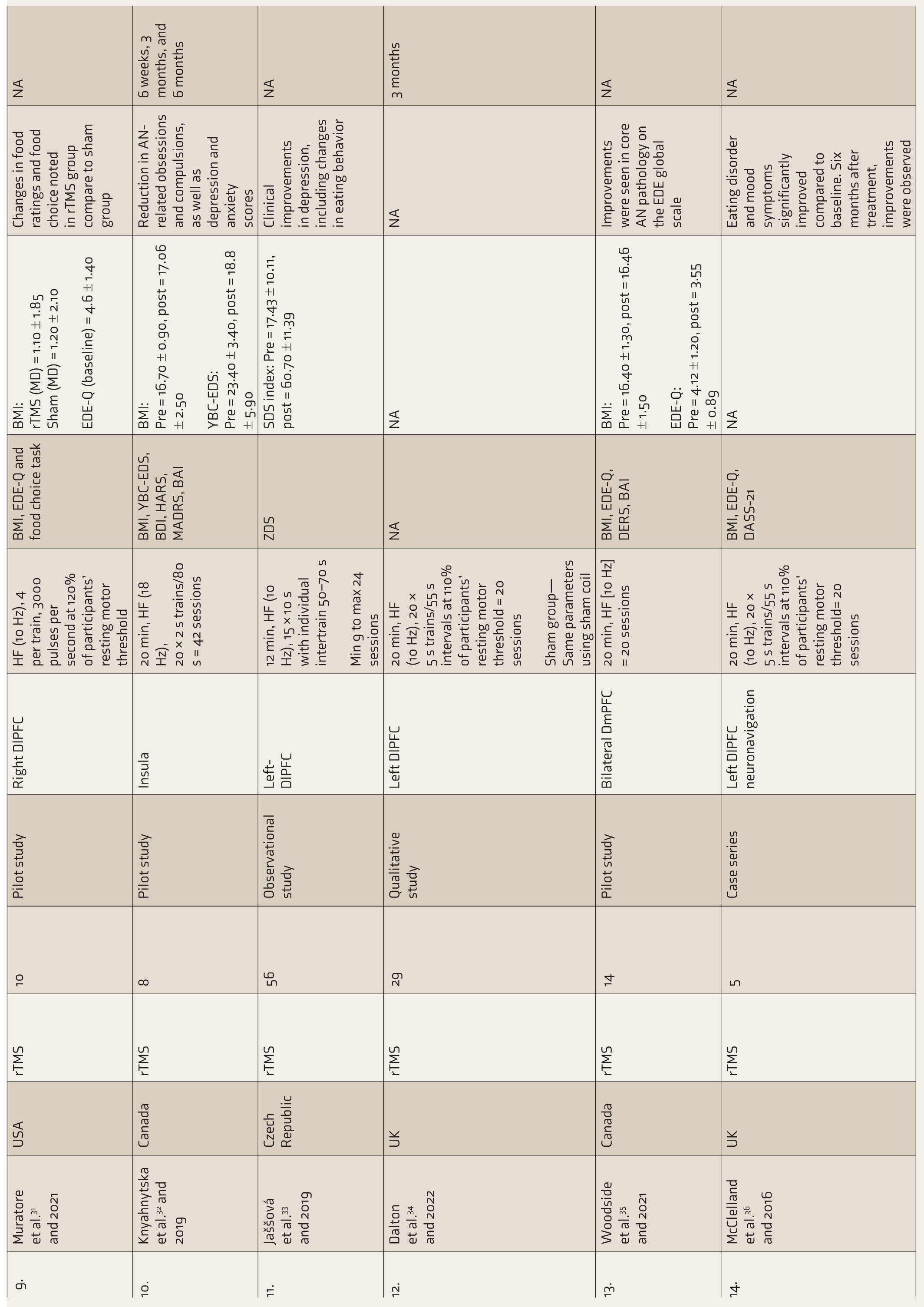
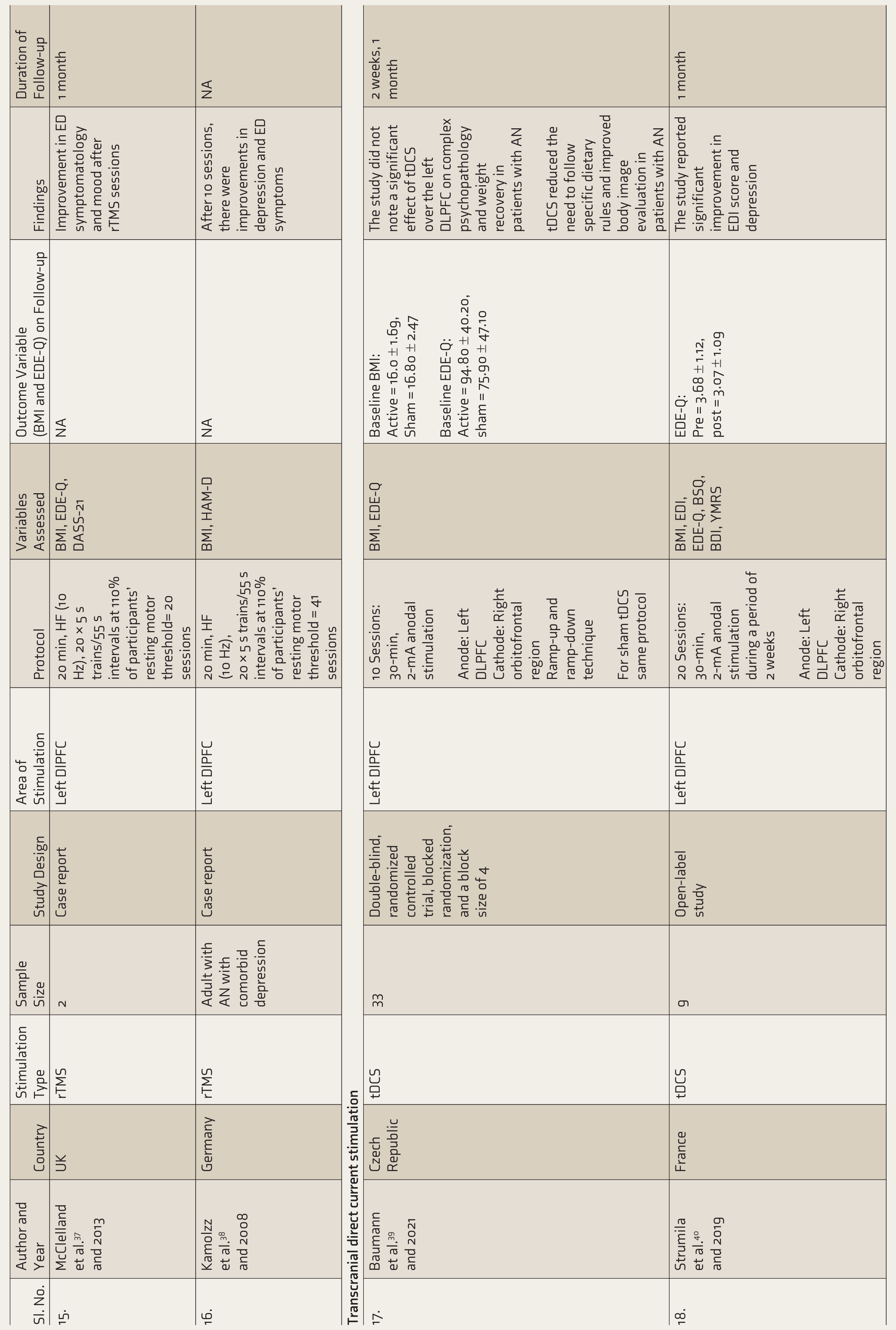
Research Assessing the Effect of Noninvasive Brain Stimulation on Anorexia Nervosa.
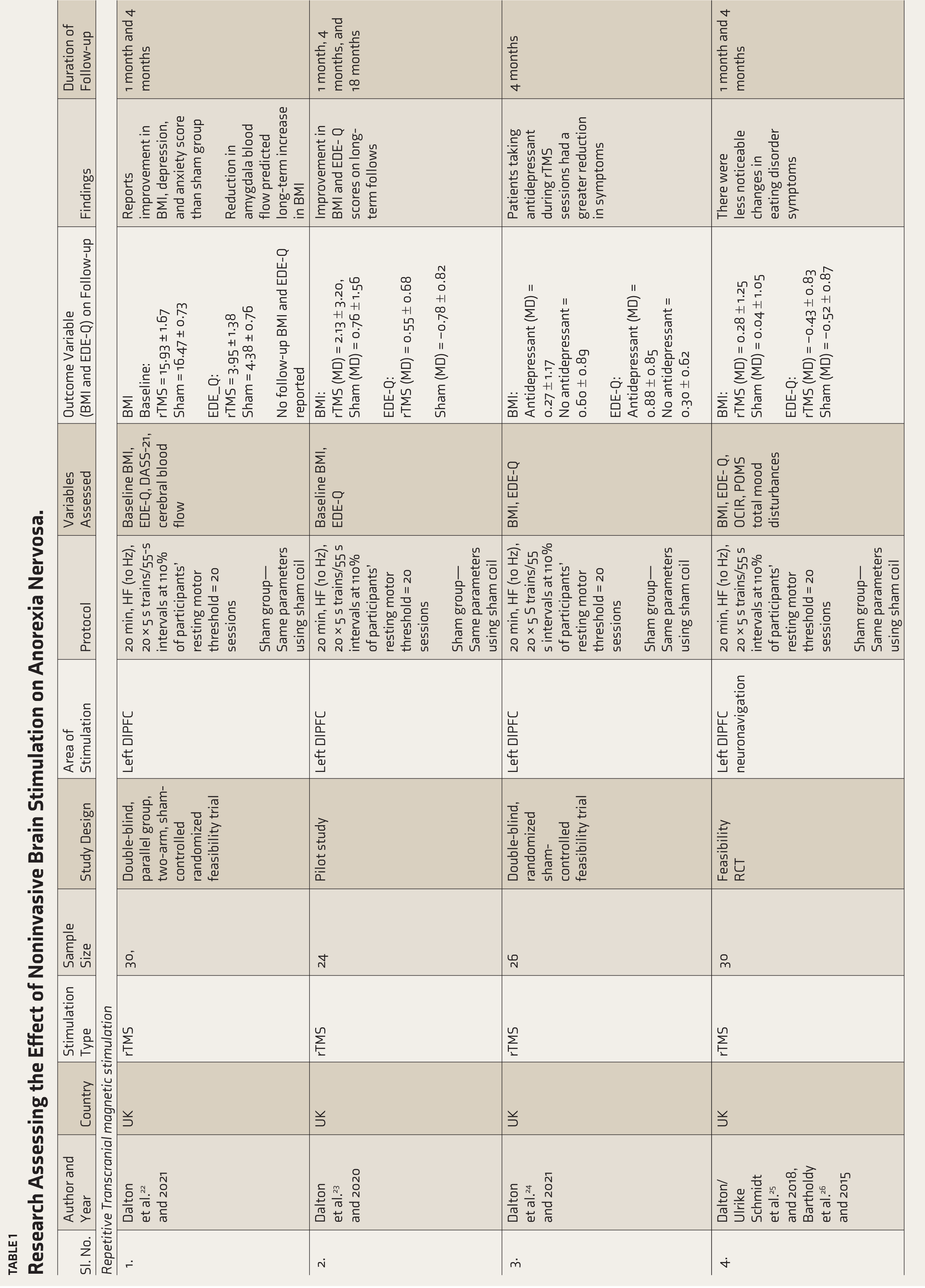

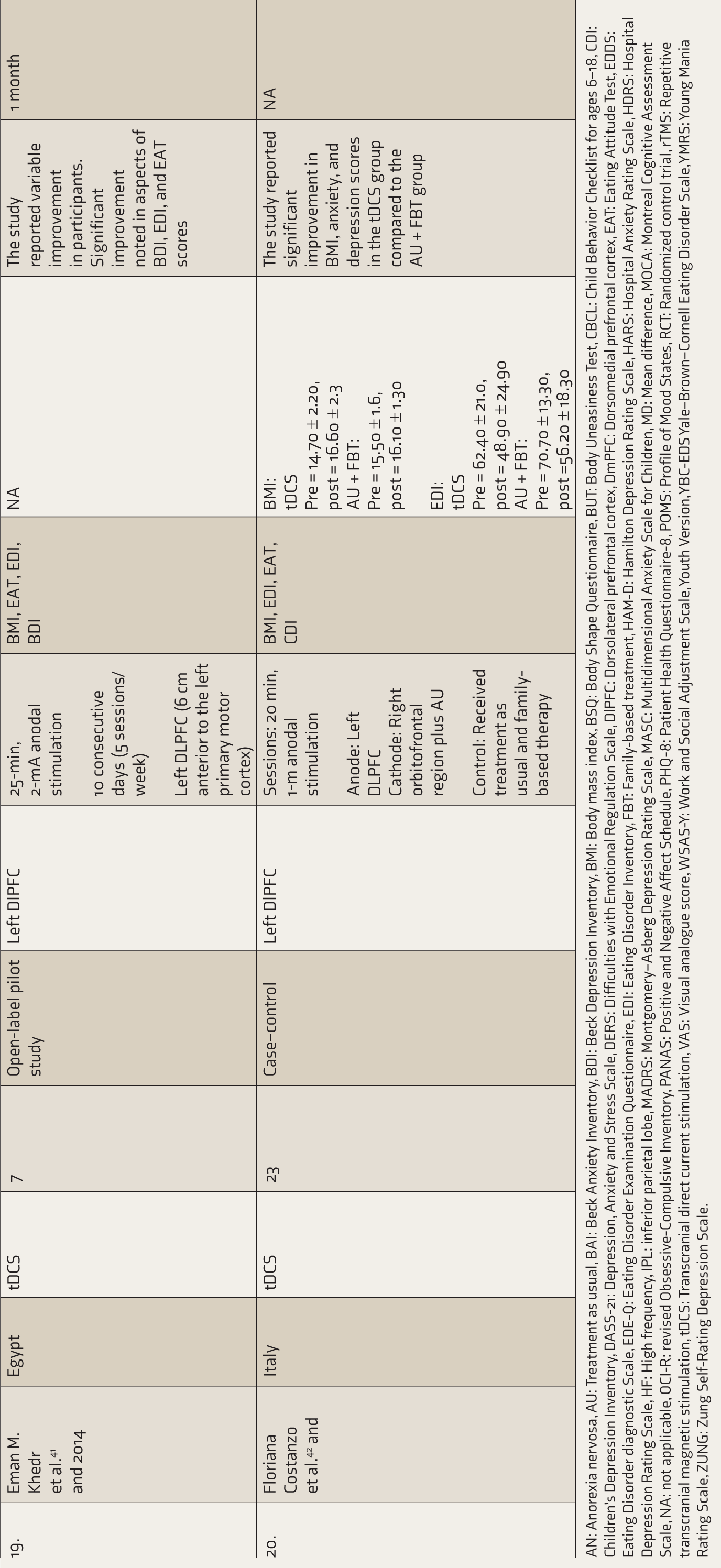
AN: Anorexia nervosa, AU: Treatment as usual, BAI: Beck Anxiety Inventory, BDI: Beck Depression Inventory, BMI: Body mass index, BSQ: Body Shape Questionnaire, BUT: Body Uneasiness Test, CBCL: Child Behavior Checklist for ages 6–18, CDI: Children’s Depression Inventory, DASS-21: Depression, Anxiety and Stress Scale, DERS: Difficulties with Emotional Regulation Scale, DlPFC: Dorsolateral prefrontal cortex, DmPFC: Dorsomedial prefrontal cortex, EAT: Eating Attitude Test, EDDS: Eating Disorder diagnostic Scale, EDE-Q: Eating Disorder Examination Questionnaire, EDI: Eating Disorder Inventory, FBT: Family-based treatment, HAM-D: Hamilton Depression Rating Scale, HARS: Hospital Anxiety Rating Scale, HDRS: Hospital Depression Rating Scale, HF: High frequency, IPL: inferior parietal lobe, MADRS: Montgomery–Asberg Depression Rating Scale, MASC: Multidimensional Anxiety Scale for Children, MD: Mean difference, MOCA: Montreal Cognitive Assessment Scale, NA: not applicable, OCI-R: revised Obsessive-Compulsive Inventory, PANAS: Positive and Negative Affect Schedule, PHQ-8: Patient Health Questionnaire-8, POMS: Profile of Mood States, RCT: Randomized control trial, rTMS: Repetitive transcranial magnetic stimulation, tDCS: Transcranial direct current stimulation, VAS: Visual analogue score, WSAS-Y: Work and Social Adjustment Scale, Youth Version, YBC-EDS Yale–Brown–Cornell Eating Disorder Scale, YMRS: Young Mania Rating Scale, ZUNG: Zung Self-Rating Depression Scale.
All the retrieved articles were uploaded to Rayyan software. 16 Title and abstract screening was conducted by two independent authors (first and second). The articles were assessed for relevance and duplication. After title and abstract screening, the full texts of the articles were accessed and screened according to the pre-specified eligibility criteria. The papers that did not meet the inclusion criteria were excluded. The title-abstract screening and full-text screening were done in a blinded manner. Any discrepancies arising during screening and data extraction were discussed with the third author. The reasons for exclusion were documented in the PRISMA chart (Figure 1) Any study type (e.g., pilot study, case–control, case series, case report) was used for qualitative analysis. RCTs and pilot studies that provided adequate data were used for meta-analysis.
PRISMA Flow Diagram of the Study Selection Process.

Data Extraction
Two reviewers (first and second) extracted the data from the selected articles, systematically entered into an Excel sheet, and evaluated it. Study characteristics were extracted, including author names, year and country, number of participants, study design, neurostimulation technique and protocol, target brain area, and relevant findings.
The primary outcome measure was the change in symptoms of AN, assessed by the body mass index (BMI) and Eating Disorder Examination Questionnaire (EDE-Q). The change in scores from baseline and to post-intervention was noted. The secondary outcome measure was the change in comorbid symptoms of depression and anxiety, assessed by the Depression Anxiety Stress Scale (DASS-21). These were also noted for analysis.
Assessment of Methodological Quality
The methodological quality of each study was assessed by two reviewers (first and second). A revised Cochrane risk-of-bias-2 (ROB-2) tool was used to assess the quality of RCTs. The Cochrane Handbook for Systematic Reviews of Interventions 17 classified domains as “low risk,” “high risk,” or “unclear risk.” Risk Of Bias In Non-randomised Studies - of Interventions (ROBINS-I) tools were used to assess the risk of bias in various domains in non-randomized studies of interventions. 18 The risk of bias was independently assessed by two reviewers (first and second), and discrepancies between them were resolved by discussion or by consulting a third reviewer.
Statistical Analysis
The meta-analysis was conducted based on the Cochrane Handbook guidelines. 19 Data extracted from eligible studies were analyzed using RevMan (Version 5.4) 20 and Jamovi. 21 Statistical heterogeneity was assessed using Cochran’s Q-test and the I² statistic, with an I² > 30% indicating substantial heterogeneity. To ensure robustness, both fixed- and random-effects models were applied; results were consistent across both. Sensitivity analysis was performed using the leave-one-out method. Publication bias was assessed using rank correlation, Egger’s regression, the fail-safe N-test, and the trim-and-fill method. Standardized mean differences (SMDs) were calculated based on pre-and posttreatment scores within the rTMS and sham groups.
Results
The screening process for the systematic review is shown in the PRISMA flow diagram (Figure 1). The initial search of the electronic databases resulted in 1,420 articles. Following de-duplication, approximately 870 articles were removed. Five hundred and fifty abstracts were screened, and 514 studies were excluded (irrelevant population = 214, intervention = 183, outcome = 117). Thirty-six articles were subjected to full-text screening, among which 17 studies were excluded (wrong intervention = 3, wrong outcome measure = 4, wrong patient population = 5, study proposal = 2, review = 2, editorial = 1). Citation tracking yielded one study, and finally, 20 studies were included in the systematic review. Among the 20 studies, rTMS was evaluated in 16 and tDCS in 4 (Table 1). We included five studies for meta-analysis,22,25,26,28,30 as many studies provided results qualitatively without any detailed statistical data or numerical values, making them ineligible for inclusion in a meta-analysis. The studies published by Dalton et al.22–24 were derived from a single trial (transcranial magnetic stimulation in severe and enduring anorexia nervosa study); to avoid data duplication, these studies were excluded from the meta-analysis.
Baseline Characteristics
The meta-analysis consisted of five rTMS studies, of which two studies had BMI data, and three studies had EDE-Q, anxiety, and depression outcome values. Studies involving tDCS were fewer and did not have common characteristics, so they were not included in the meta-analysis. The studies included in meta-analysis comprised of 111 participants with a mean age of 30.79 ± 9.10 years and a mean duration of illness of 13.31 ± 7.09 years. The baseline BMI was 15.98 ± 1.02, and the EDE-Q was 4.29 ± 3.71. The most common site for rTMS was the left dorsolateral prefrontal cortex (DlPFC); in one study, it was the dorsomedial prefrontal cortex (DmPFC), in another, the inferior parietal lobe, and in one study, the insula. The mean stimulation time was 24 ± 10.94. For tDCS, the stimulation site was the left DlPFC.
Efficacy of rTMS in AN
A total of 16 studies evaluated rTMS in AN, out of which six were RCTs, five were pilot studies, one was a qualitative study, one was observational studies, and three were case reports/series. The first trial of rTMS for AN was documented in 2008 by Kamolz et al. 38 in a case report where the patient showed improvement in symptoms. Following this, many protocols, pilot studies, and RCTs were published.
Dalton et al.22–27,34 have published five RCTs and one qualitative study on the effect of rTMS in AN. In the target area in the left DlPFC, findings showed improvement in EDE-Q, improved weight, and food choices, and assessed the cerebral blood flow to the amygdala in one of the RCTs followed up to 18 months of post-sessions, which also showed significant, sustained improvement. McClelland and co-workers 27 published one RCT, one case series, and one case report, which showed potential improvement in EDE-Q, Eating Disorder Diagnostic Scale, Visual Analogue Scale (VAS), and BMI. Van den Eynde et al. 30 Muratore et al. 31 and Knyahnytska et al. 32 conducted pilot studies targeting the left DlPFC, right DlPFC, and insula, respectively, involving small populations that showed improvement in BMI, EDE-Q, VAS, food choice, and Eating Disorder Inventory (EDI) scores. Blake Woodside conducted a pilot study targeting bilateral DmPFC, which showed improved EDE-Q and BMI. Chastan et al. 29 published an RCT targeting the right inferior parietal lobe (IPL) that assessed BMI, Body Shape Questionnaire (BSQ), Eating Attitude Test (EAT), and EDI, which showed no significant differences in body shape perception. Jaššová et al. 33 conducted an observational study that reported changes in eating behavior.
Meta-analysis of Treatment Outcomes
BMI
The forest plot showed that there was no significant increase in BMI among patients in the rTMS than sham group (SMD = 0.174, Z = 0.91, 95% confidence interval [CI]: −0.201 to 0.548, p = .363, I² = 0.00%; five studies) (Figure 2). There was no significant amount of heterogeneity in the actual outcomes (Q = 0.148, p = .997, τ² = 0.00, df = 4). The studentized residuals revealed that none of the studies had a value larger than ±2.5758; hence, there was no indication of outliers in the context of this model. According to Cook’s distances, none of the studies could be considered overly influential. Sensitivity analysis was performed using the leave-one-out method by excluding a high-risk bias study (Bethan Dalton-2020), which showed (SMD = 0.181, Z = 0.83, 95% CI: −0.252 to 0.608, p = .407; four studies) no significant difference in the effect size (Supplementary Figure 1). No funnel plot asymmetry was observed (rank correlation p = .4833; regression test p = .7833). Fail-safe N analysis showed that zero null-effect studies would nullify the findings (p = .201), indicating a lack of robustness. Trim-and-fill analysis suggested minimal publication bias (Supplementary Table 3).
EDE-Q
In addition, three studies that provided adequate follow-up data for analysis were assessed for the change in EDE-Q after rTMS and sham sessions. The forest plot showed that the EDE-Q of patients decreased after rTMS than sham (SMD = 0.231, Z =1.04, 95% CI: −0.204 to 0.671, p = .304, I² = 0.00%; three studies) (Figure 3). There was no significant heterogeneity in the actual outcomes (Q = 0.221, p = .907, τ² = 0.000, df = 2).
The studentized residuals revealed that none of the studies had a value larger than ±2.3940; hence, there was no indication of outliers in the context of this model. According to Cook’s distances, none of the studies could be considered overly influential. Sensitivity analysis was performed using the leave-one-out method by excluding a high-risk bias study (Bethan Dalton-2020), which showed (SMD = 0.184, Z = 0.69, 95% CI: −0.337 to 0.706, p = .490; two studies) no significant difference in the effect size (Supplementary Figure 2). No funnel plot asymmetry was detected (rank correlation p = .3333; regression test p = .7503). Fail-safe N analysis indicated that zero null-effect studies would be needed to nullify the findings (p = .206), suggesting the results are not robust. Trim-and-fill analysis showed minimal publication bias (Supplementary Table 3).

CI: Confidence interval, rTMS: Repetitive transcranial magnetic stimulation.
Efficacy of tDCS in AN
A total of four studies on tDCS in AN were reviewed, of which one was an RCT, two were open-label studies, and one was a case–control study. Khedr et al. 41 conducted an open-label pilot study on seven patients. Variable improvement was noted in the EDI and EAT scores. In a case–control study conducted by Costanzo et al. 42 there was a significant improvement in BMI in the tDCS group (MD = 1.90) compared to the treatment as usual plus family-based treatment group (MD = 0.60). However, no significant difference was observed in the EDI, EAT, and Body Uneasiness Test scores. In the open-label study conducted by Strumila et al. 40 the EDI total scores pre- and post-sessions were 95.11 ± 38.41 and 79.38 ± 35.35, EDE-Q were 3.68 ± 1.12 and 3.07 ± 1.09, respectively, showing significant improvement in EDI (inefficiency, perfectionism, distrust, interoceptive awareness, maturity fears, and ascetism), EDE-Q, and BSQ scores on post-treatment. Baumann et al. 39 conducted a study on 33 individuals. They showed no significant effect of tDCS on complex psychopathology (EDE-Q and Zung Self-Rating Depression Scale self-rated depression scale) and weight recovery (BMI) in patients with AN.
Comorbidity in Anorexia
According to studies by Dalton et al.22–27 McClelland et al.28,36 Van den Eynde et al. 30 Chastan et al. 29 Jaššová et al. 33 and Kamolz et al. 38 comorbid depression and anxiety were found to be high in AN patients. Other comorbid psychiatric diagnoses reported in AN also include obsessive-compulsive disorder, somatoform, substance-related disorders, and posttraumatic stress disorders (PTSDs). 35
Meta-analysis of Comorbid Symptom Outcomes
Depression
A total of three studies assessed the change in depression scores using the DASS-21 in follow-up sessions after rTMS and sham were included. Other studies could not be included in the analysis because they did not use comparable instruments or provide comprehensive statistical data or numerical values. The forest plot showed that the depression scores of patients had a significant decrease after rTMS compared to the sham group (SMD = −0.501, Z = 2.19, 95% CI: −0.941 to −0.053, p = .030, I² = 0 %; three studies) (Figure 4). There was no significant heterogeneity in the true outcomes (Q = 1.794, p = .413, τ² = 0.0047, df = 2). The studentized residuals revealed that none of the studies had a value larger than ±2.3940; hence, there was no indication of outliers in the context of this model. According to Cook’s distances, none of the studies could be considered overly influential. Sensitivity analysis was performed using the leave-one-out method by excluding a high-risk bias study (Bethan Dalton-D), which showed (SMD = 0.391, Z = 1.29, 95% CI: −1.010 to 0.213, p = .201; two studies) no significant difference in the effect size (Supplementary Figure 3). No funnel plot asymmetry was observed (rank correlation p = .3333; regression test p = .1777). Fail-safe N analysis indicated that three null-effect studies would be needed to nullify the findings (p = .011), indicating robust results. Trim-and-fill analysis showed minimal publication bias (Supplementary Table 3).

CI: Confidence interval, rTMS: Repetitive transcranial magnetic stimulation.

CI: Confidence interval, rTMS: Repetitive transcranial magnetic stimulation.
Anxiety Scores
The forest plot showed that the anxiety scores of patients had a significant decrease after rTMS compared to the sham group (SMD = −0.461, Z = 2.03, 95% CI: −0.892 to −0.024, p = .040, I² = 0 %; three studies) (Figure 5). There was no significant heterogeneity in the actual outcomes (Q = 0.064, p = .978, τ² = 0, df = 2). The studentized residuals revealed that none of the studies had a value larger than ±2.3940; hence, there was no indication of outliers in the context of this model. According to Cook’s distances, none of the studies could be considered overly influential. Sensitivity analysis was performed using the leave-one-out method by excluding a high-risk bias study (Bethan Dalton-2020), which showed (SMD = 0.471, Z = 1.73, 95% CI: −1.000 to 0.060, p = .082; two studies) no significant difference in the effect size (Supplementary Figure 4). No funnel plot asymmetry was detected (rank correlation p = 1.0000; regression test p = .9562). Fail-safe N analysis indicated that three null-effect studies would be needed to nullify the results (p = .013), suggesting robustness. Trim-and-fill analysis showed minimal publication bias (Supplementary Table 3).

CI: Confidence interval, rTMS: Repetitive transcranial magnetic stimulation.

ROB: Risk of Bias, rTMS: Repetitive transcranial magnetic stimulation, tDCS: Transcranial direct current stimulation.
Safety and Tolerability
The individuals who received rTMS generally tolerated it well but reported minor adverse effects such as slight buzzing in the head, intense and painful tapping, and dizziness. Blood pressure and pulse measurements showed no variation during or after the sessions.22–38 Individuals receiving tDCS reported adverse events such as tingling, burning sensation, headache, pinching, pressure in the head, burning in the eyes, twitching of the eye, itching, and local redness.39–42
Quality Assessment
The risk of bias and quality was assessed using the ROB-2 tool for RCTs and the ROBINS-I tool for non-randomized studies (non-RCTs). Among RCTs, bias due to missing outcome data was identified in six studies,22,25,26,28,29,39 primarily due to loss to follow-up and inadequate handling of missing data, such as the absence of appropriate imputation methods or unexplained missingness possibly related to the outcomes. In non-RCTs, one study 40 exhibited bias in intervention classification due to unclear assignment. Four studies31,32,35,42 had moderate risk across multiple domains, mainly due to unaddressed confounding, unblinded or subjective outcome measurement, incomplete outcome data, and potential selective reporting. Five studies30,33,34,40,41 were rated as having serious bias due to significant confounding, selection bias, substantial missing data, and likely selective reporting of favorable outcomes (Figure 6A and 6B).
Discussion
Early literature was largely comprised of case reports and series. However, over time, researchers experimented with the use of rTMS and tDCS through pilot studies involving single sessions without control groups, followed by open-label studies. In recent years, a few RCTs involving small groups and multi-session protocols have been conducted and published.
Stimulation Target
An ED may be predisposed by structural and functional changes in the insula and frontal cortex, including the orbitofrontal and cingulate regions, which are involved in reward and anxiety processing. Adaptive changes in these circuits in response to malnutrition or recurrent purging and binge eating may also encourage illness behavior, impede recovery, and lead to relapse. 43 The executive control, basal ganglia, and default mode networks all show poorer inter-network connectivity, whereas the executive control and basal ganglia networks showed weaker intra-network connectivity in those with higher ED symptoms. 44 Neurostimulation (rTMS and tDCS) induces significant positive changes in resting state functional connectivity and modulates the functional cortical physiology.45,46 Literature also suggests that a person with EDs have abnormal and altered frontal and cingulate connections. 47 It is likely that neurostimulation modulates brain activity in the frontocingulate circuit, leading to improvement in symptoms. 48
Most studies targeted the left DlPFC for neurostimulation in both rTMS and tDCS. Individuals with AN showed reduced DlPFC activation during cognitive reappraisal 48 and cognitive control. 49 The DlPFC has connections to limbic areas like the insula and amygdala. The development of AN and restricted food intake are linked to dysregulation in this frontolimbic circuit, which is associated with habit and reward. High-frequency (i.e., excitatory) rTMS modulation and tDCS (anode) in this region encourage a more flexible attitude toward food choice, that is, a decrease in self-controlled decisions. It is possible that high-frequency rTMS and tDCS to the DlPFC enhanced the cognitive control required to overcome unhelpful restricted eating habits.50,51 These techniques can also modulate this circuit through top-down control, leading to improvements in symptoms of AN.
Reward-based models and abnormalities in reward processing are possible mechanisms implicated in the pathogenesis of AN.52,53 Altered activity of the anterior cingulate cortex and striatum could explain patients’ pathological engagement in behaviors they consider rewarding (e.g., self-starvation) that are otherwise aversive or punishing to those without the ED. 54 Specifically, high-frequency rTMS may suppress neural activity in more distant regions (such as the orbitofrontal and anterior cingulate cortex) involved in controlling reward-based behaviors while promoting activity in the directly underlying cortex (DlPFC).55,56
The DmPFC plays a significant role in cognitive and impulse control. 57 Changes in DmPFC-striatal-thalamic connectivity are associated with improvements in Major Depressive disorder (MDD), Bulimia nervosa (BN) and Obsessive compulsive disorder (OCD) symptoms.58,59 DmPFC-rTMS has been shown to enhance the capacity for impulse control, improving AN symptom. 60 In a study conducted by Woodside et al. 35 participants diagnosed with AN and comorbid depression received 20–30 sessions of rTMS on the DmPFC. Post-intervention, there was a significant reduction in the EDE-Q scores, depression, anxiety, and an improvement in weight.
Functional magnetic resonance imaging (fMRI) studies have shown that when emaciated and malnourished AN individuals are shown pictures of food, they display abnormal activity in the insula. 32 The insula has also been identified as a potentially important region in AN pathophysiology due to its role in gustatory modulation, feeding behavior, processing of interoceptive stimuli, and self-awareness. 61 In a study conducted by Knyahnytska et al. 32 TMS directed to the insula in eight patients with severe enduring AN reduced obsessive and compulsive behaviors associated with AN, as well as anxiety and depression, without any adverse events.
In body shape perception-related fMRI studies, patients with AN showed reduced activation in the inferior parietal lobule, an area related to the attention network, after viewing images of their bodies. 62 In a study conducted by Chastan et al. 29 patients with AN, randomly allocated to the rTMS and sham groups, received high-frequency rTMS over the IPL for 2 weeks. The findings showed no significant difference in body shape perception or other related parameters.
Stimulation Protocol
Studies involving rTMS mainly used 20–60 min high-frequency (10 Hz) rTMS sessions consisting of 20 five-second trains with 55-s intervals at 90%–110% of participants’ resting motor threshold. Knyahnytska et al. 32 used deep TMS with an H-coil to target the insula; the study involved 42 sessions of rTMS, each lasting 20 min/day, 5 days/week. Studies involving tDCS have used the 10–20 electroencephalogram system for electrode placement, with the anode over F3 (left DlPFC) and the cathode over Fp2 or F4. Strumila et al. 40 had placed an anode 6 cm anterior to the left primary motor cortex (M1) along a parasagittal line, and the cathode on the contralateral arm (extracephalic). Due to the limited number of studies, stimulation protocols, stimulation, and parameters, it was not feasible to compare the efficacy of different protocols with each other.
Effectiveness
Studies involving rTMS over the DlPFC in individuals with AN reported a pooled effect size that is small and nonsignificant for the reduction of core symptoms of anorexia (SMD = 0.175, p = .424) and BMI (SMD = 0.231, p = .304). This lack of statistical significance may be attributed to the limited number of studies and small sample sizes, which reduced the overall statistical power of the meta-analysis. The reduction in symptomatology may result from restoring altered “top-down” cognitive control related to emotional and other self-regulation processes. Only a limited number of studies have assessed the long-term effects of neurostimulation on AN. Dalton et al. 22 followed individuals for up to 18 months post-randomization and showed sustained weight gain. McClelland and co-workers 27 showed improvement in ED symptoms and general psychopathology following rTMS, which often persisted for up to 12 months. Studies utilizing tDCS also demonstrated improvements in BMI, EAT, and EDI scores, as well as a decrease in the primary symptoms of anorexia (feelings of fullness and fatness). However, there is no information available in the literature on the long-term effects on the psychopathology of AN.
Comorbidities
Addressing depressive symptoms is considered a crucial approach in the treatment of severe and enduring AN. Given the low responsiveness to antidepressant medication in individuals with AN, the antidepressant effects of neurostimulation present a viable option for patients with severe and enduring AN. 24 Patients with AN often use dietary restrictions to modulate or regulate their mood. 63 Hence, it is expected that neurostimulation-related improvements in mood would reduce the need to restrict food intake and make self-controlled choices in AN.64,65 Our meta-analysis studies reported that rTMS significantly decreased depression (SMD = 0.501, p = .030) and anxiety symptoms (SMD = 0.461, p = .025). In a study conducted by Dalton et al. 24 patients who received concomitant antidepressants and underwent rTMS showed significant improvements in ED symptoms than those who did not receive antidepressants—suggesting that antidepressant use may enhance the effect of rTMS. However, the underlying mechanism remains unclear.
Safety
The occurrence of serious side effects had not been reported in our literature review. The reported side effects in rTMS are slight buzzing sensations, pain, and headache. Those who received tDCS had local redness, itching, headaches, tingling, or burning sensations.22–38 In one study targeting the IPL for rTMS, two patients who underwent rTMS experienced suicidal attempts and did not show improvement in mood and anxiety. 29 These findings suggest that IPL-rTMS may not effectively improve psychiatric comorbidities. However, there is a paucity of research addressing the safety and acceptability of noninvasive brain stimulation (NIBS), specifically in the context of EDs.
Feasibility
The feasibility of NIBS in India depends on various factors, including awareness, clinical infrastructure, cost-effectiveness, and ethical considerations. Despite the global evidence supporting NIBS, particularly rTMS and tDCS, as adjunct therapies for conditions such as AN and BN, its application in India is still in its nascent stages. There is a lack of research evaluating its safety, efficacy, and acceptability, specifically in Indian populations. The high cost of the equipment and the need for trained professionals pose additional barriers to its widespread adoption.
Ethical Considerations
The use of NIBS raises significant ethical and clinical concerns, particularly in cognitive and emotional impairments. Individuals with AN often experience distorted body image and impaired decision-making, which can compromise their ability to provide fully informed consent for NIBS. 66
The rationale for considering NIBS in this population should be based on the chronicity of the disorder and its refractoriness to conventional treatments. 67 In cases of treatment-resistant AN, neuromodulation can be viewed as a promising option to address the illness. However, it is essential to ensure that the potential benefits of such interventions outweigh the risks, particularly given the limited understanding of their long-term efficacy and safety in this context. 66
Future Direction
As initial preliminary research suggests, there is a potential benefit in the reduction of psychopathology in AN; however, the possible outcomes and its neurobiological mechanism are still yet to emerge. Future research on neurostimulation treatments for AN should focus on optimizing patient selection by identifying neurocognitive and neural predictors of treatment efficacy and refining treatment protocols, including the optimal parameters of stimulation (target areas, frequency, intensity, and duration). This would help to individualize protocols and deliver personalized treatment. Longitudinal studies are needed to evaluate whether improvements following NIBS are maintained over time and whether they require maintenance treatment of AN patients. The existing literature remains very limited and is in its early stages.
Limitations
This systematic review and meta-a nalysis have several limitations: small population sizes, methodological heterogeneity, and study design (i.e., observational, pilot, case series/report alongside RCTs); diverse stimulation areas, protocols, and parameters; and absence of long-term follow-up. The presence of comorbidities such as depression, anxiety, and PTSD in patients with AN was noted in some studies. However, there is a lack of studies comparing the efficacy of neurostimulation in patients with or without comorbidities. There is no study evaluating the effectiveness of neurostimulation in AN patients based on geographical distribution, as many pilot studies were represented, which had a serious risk of bias.
Conclusion
The research on AN in India remains in its early stages, likely due to cultural variations in the perception of the illness, societal stigma, and limited awareness, all of which present significant challenges in diagnosis. Furthermore, there is a scarcity of research on newer management techniques for AN in the Indian context. While individual Western studies have reported reductions in core symptoms and improvements in BMI following treatment, our meta-analysis has not consistently supported these findings. This study has shown more robust reductions in mood symptoms such as anxiety and depression. Most studies have targeted the DlPFC, highlighting the need for further investigation into the stimulation areas and optimal stimulation parameters. This underscores the necessity for large-scale clinical trials to evaluate the efficacy of NIBS for AN across diverse populations. Such research could pave the way for more effective and newer treatment options for this disabling condition.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
We thank the faculty and supporting staff of the Departments of Psychiatry and Community Medicine who assisted during the review process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.