
Abstract
Background:
Depression is a highly prevalent mental disorder. Maternal depression can adversely impact perinatal outcomes and child development, and can increase mental disorders for children and adolescents. Understanding the impact could lead to opportunities for early intervention and prevention.
Methods:
We selected 29 mothers attending a tertiary care setting for mental health, who had remitted following a depressive episode, and 35 control mothers. They rated their children’s behavior on the strengths and difficulties questionnaire (SDQ) and temperament measurement schedule (TMS). Using a cross-sectional design, we compared the scores on behavior and temperamental characteristics between the two groups. We also studied if the severity of depression correlated with increased behavioral difficulties and evaluated if there were any differences based on gender or age.
Results:
Our results suggest no significant difference in behavior and temperament between the two groups. There was a trend for the children of mothers who had depression to have poor emotionality, higher rhythmicity on TMS, and higher peer relatedness based on SDQ scores. There was no correlation between the severity of depression in the mother and the severity of behavior problems.
Conclusion:
The lack of significant differences between the two groups could be related to less severe forms of depression, the remission of depression in the mother, the presence of other supportive family members, or elevated problems in the control arm. Further research in this area with a longitudinal design, including mothers with ongoing symptoms and longer-term follow-up, studying the bidirectional influence, is warranted.
Depression in the mother can adversely impact children and adolescents. Effective treatment of the mother’s depression could mitigate the risk for the children. Further longitudinal research is required to understand the bidirectional influence of maternal depression and behavior problems, risks for mental disorders, and prevention opportunities.Key Messages
Depression is the leading cause of disability in the world. 1 The prevalence of depression amongst women in India varies from 11% to 13% based on studies conducted in rural Tamil Nadu 2 and Goa 3 to about 16.3% in a study from Chennai. 4 Depression in mothers can be associated with impaired cognitive development and insecure or disorganized attachment styles,5–7 in younger children. Depression is also common in mothers outside the postpartum period. 8 Researchers have demonstrated an increased risk of depression,9–11 anxiety disorders, substance abuse, 12 and low academic achievement 13 in older children, adolescents, and even reduced life span in adulthood. 12 In the STAR*D-child study, consisting of depressed mothers with children aged 7 to 17 years, nearly one-third of the children had a current psychiatric diagnosis and nearly half had a history of psychiatric diagnosis. Atypical features of depression and suicidal attempts in the mother further increased the children’s risk of depression by threefold. 14 In a longitudinal study, prenatal, postnatal, and later episodes of depression were all somewhat equally predictive of antisocial outcomes in the offspring. However, cumulative exposure with onset in the perinatal period conferred the greatest risk. 15 Effect on the children could be mediated by the mother’s negative affect, thoughts, behaviors (parenting), or contextual factors (such as poverty and domestic violence) that contributed to it. 16
Elevated behavior problems were common in the children of mothers with depression and were predictive of future psychopathology.17,10 Sameer and colleagues 18 compared the children of mothers with unipolar depression, those of mothers with bipolar disorder, and those of control mothers based on parent rating when the mothers were in remission. They found increased internalizing and externalizing behavior in the children of mothers with depression compared to control mothers. Young children are more likely to show behavioral difficulties rather than fulfill the criteria for mental disorders. Understanding the impact of maternal depression on children’s behavior could lead to the early identification and, potentially, the prevention of mental disorders for these children. 19 To our knowledge, only Sameer and colleagues 18 studied the impact of maternal depression on the behavior of school-age children in India. So we wanted to see if those findings would be replicated in our sample. We further wanted to evaluate if there would be any correlation between the severity of depression and behavioral difficulties. We were also interested in understanding if there was any difference between genders and age groups.
Methods
The study was conducted in Institute of Mental Health, Chennai, which is a tertiary care mental health setting, between December 2004 and December 2005, using a cross-sectional design. The protocol for the study was approved by the Ethics Committee of the Institute.
Cases were consecutive female patients attending the Outpatient Department, who had unipolar depression, were on remission based on Mini-International Neuropsychiatric Interview (MINI), 20 and had biological children aged 4 to 14 years. Controls were chosen from attendants of patients in a tertiary care pediatric hospital (Institute of Child Health, Chennai), who had no current psychopathology as per MINI 20 and Brief Psychiatric Rating Scale 21 and no lifetime history of an affective disorder as per schedule for affective disorders and schizophrenia-lifetime version. 22 We excluded mothers with major or chronic medical problems and those who had children with developmental disorders or husbands with significant mental health issues. A total of 29 cases and 35 controls were selected.
A sample size of 60 children in each group was estimated to have 80% power to detect a difference in the mean score of -0.0620 [the difference between the group I mean of 3.750 and group II mean of 4.370 for behavior in the temperament measurement schedule (TMS)], 18 assuming that the common standard deviation is 1.2, using a two-group t-test with a two-sided significance level of 0.05.
The cases were diagnosed as per International Classification of Diseases-10th revision (ICD-10) 23 by a senior psychiatrist. The diagnosis was confirmed after an independent interview by the chief consultant of the unit. Such cases were followed up until the patient achieved remission as per the MINI interview schedule, which KK administered under the supervision of a consultant psychiatrist. The interviewer did not see the children. In most instances, both the parents were present during the interview. Where parents reported significant behavioral and emotional disturbances, they were referred to the child guidance clinic in the children’s hospital for further evaluation and management.
Measures Used
Strengths and Difficulties Questionnaire (SDQ) 24
The SDQ is a brief 25-item scale developed to generate scores in five domains of psychological adjustment among children and adolescents, namely hyperactivity–inattention, emotional problems, prosocial behavior, conduct problems, and peer problems, based on key symptoms for Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) diagnoses. 25
Temperament Measurement Schedule (TMS) 26
The TMS, developed in India by Malhotra, 27 measures nine temperament variables as described by Thomas and Chess 28 with 45 items, five each for nine variables to be rated on a five-point scale. The scores <3 are in the negative direction, those >3 are in the positive direction, and three was average, depending on the intensity and frequency of the behavior measured by each item.
Statistics
Statistical analyses were done using Statistical Package for Social Sciences version 10. The demographic and clinical data were studied using descriptive statistics. The scores of the two groups (i.e., children of depressed mothers and children of normal mothers) on the SDQ and TMS were compared using the two-group Student’s t-test. The relationship between the severity of depression in the mother and the child’s behavioral problem was studied using the Pearson correlation. The Student’s t-test was used to study the difference between the sexes in the case group. The children were divided into three groups based on age, and the difference in their behavior was studied using one-way ANOVA.
Results
Baseline characteristics (Table 1) were comparable across both cases and controls on most factors except the ages of mothers, fathers, and children. Most of them had some school education, were Hindu and from nuclear families, and with two or three children. The sample of mothers chosen were all outpatients, except one who had inpatient admission, and two have had psychotic symptoms. Two of the mothers have had one and two suicide attempts in the past.
Baseline Characteristics
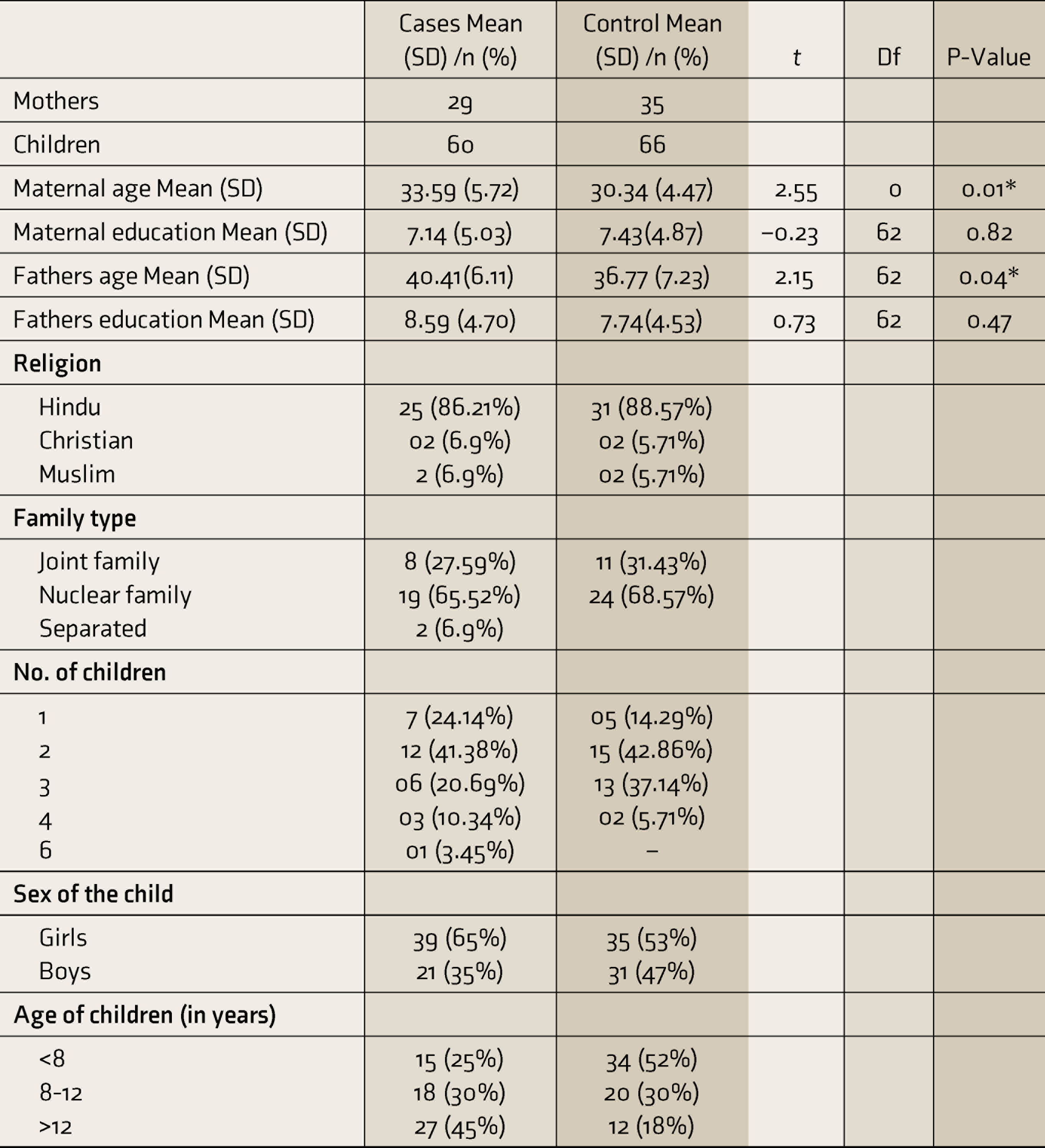
Note: Case, children born to mothers who had depression; Control, children born to normal mothers; *P < 0.05 but not significant after Bonferroni’s correction P < 0.003.
SD, standard deviation; t, student t; Df, degree of freedom.
Amongst the mothers of cases, there was a family history of suicide in three, alcoholism in two, schizophrenia in one, and cannabis-induced psychosis in one. Among the fathers of cases, three had a family history of suicide, one had a family history of alcohol dependence, and two had sisters diagnosed with depression. Amongst the parents of controls, no first-degree relative was reported to have a psychiatric problem.
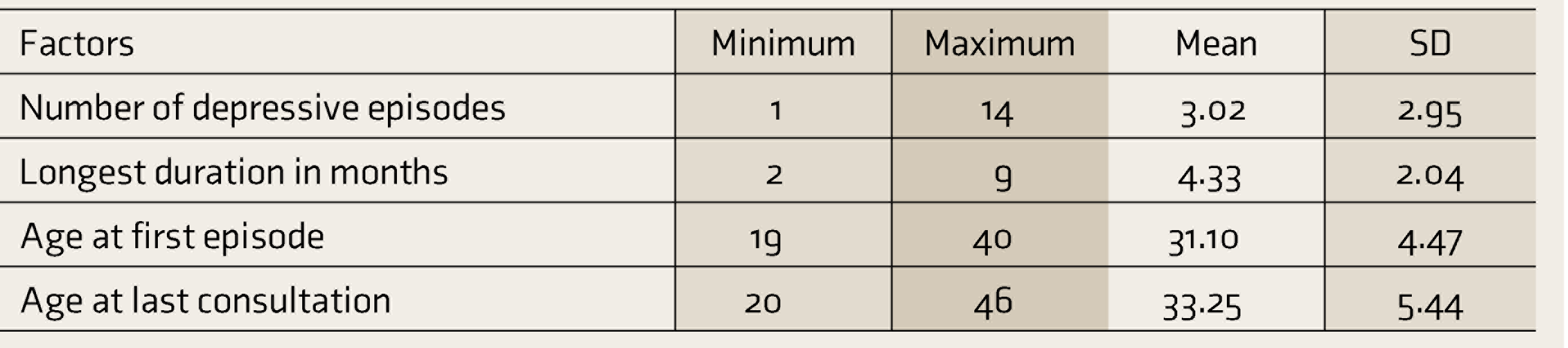
There was no significant difference in problem behaviors or prosocial scores between the two groups, based on the SDQ scores. Even though there was a trend for the children of mothers who had depression to have less peer-related problems as rated on the SDQ (Table 2), and higher scores on emotionality and rhythmicity on the TMS (Table 3), compared to the control children, it was not significant after Bonferroni’s correction. The severity of the depression was rated based on the age of onset, the number of episodes, the duration of episodes (Table 4), and suicidality. None of the severity measures predicted the difference in SDQ or TMS scores in the children. We found no differences between genders and different ages.
Comparison of the Scores on SDQ
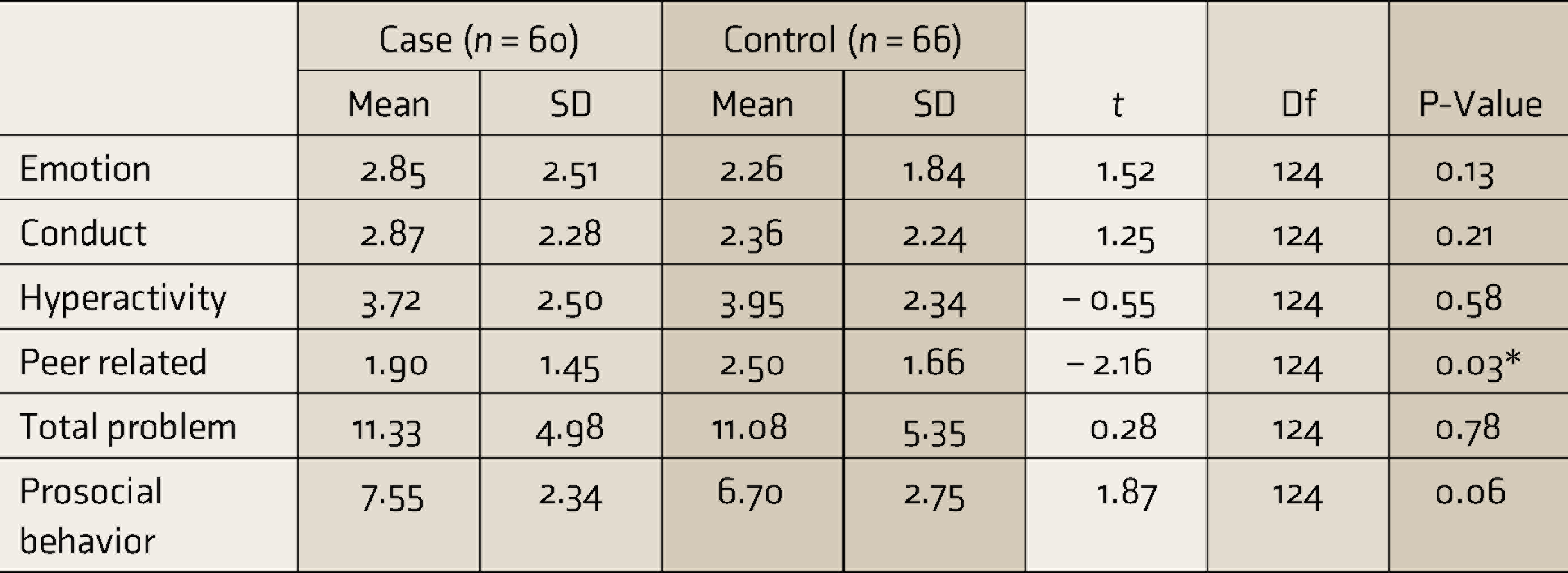
Note: Case, children born to mothers who had depression; Control, children born to normal mothers; *P < 0.05 but not significant after Bonferroni’s correction P < 0.003.
SD, standard deviation; t, student t; Df, degree of freedom; SDQ: Strengths and difficulties questionnaire.
Comparison of Scores on TMS
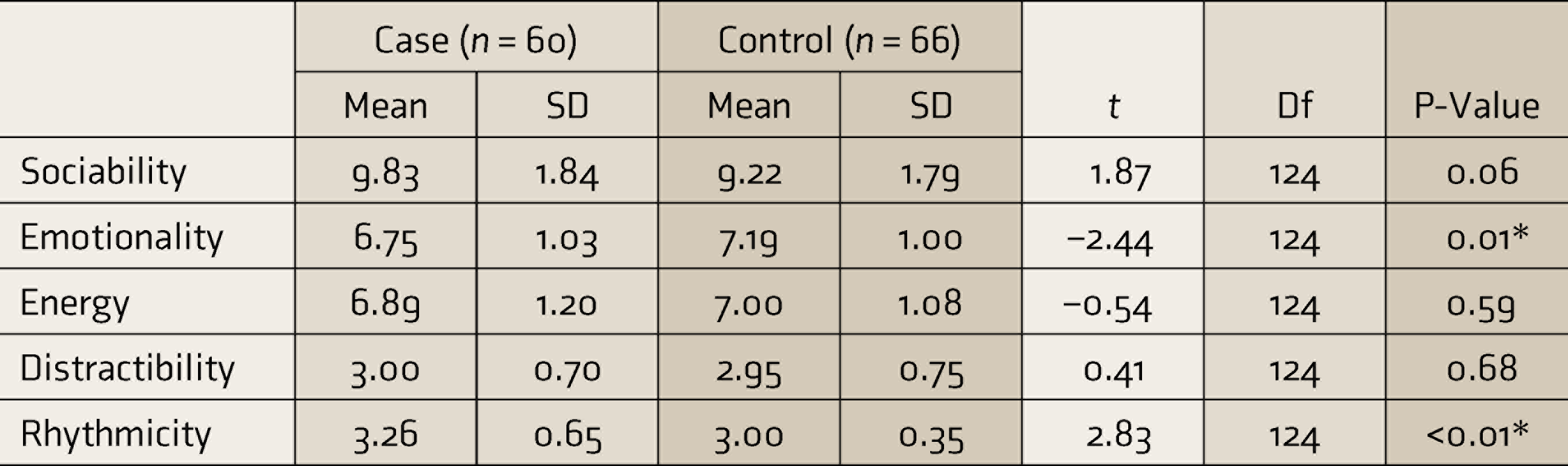
Note: Case, children born to mothers who had depression; Control, children born to normal mothers; * P < 0.05 but not significant after Bonferroni’s correction P < 0.003.
SD, standard deviation; t, student t; Df, degree of freedom; TMS: Temperament Measurement Schedule.
Severity of Depression Amongst Mothers
Discussion
This study was an attempt to understand the behavioral difficulties in the children of mothers with depression. Behavioral difficulties in this population are forerunners for future psychopathology. 29
Previous studies30–32 found that parental depression was associated with a range of adverse outcomes, including depressive disorder, behavior problems, and emotional disorders. However, in our study, the children of mothers with depression scored higher on emotional, conduct, and total problems on the SDQ, but the difference was not statistically significant. Interestingly in our sample, the cases had a trend for higher prosocial scores and lesser peer-related difficulties. This has been observed in other studies also. 33 Whether stress made these children more resilient is to be studied. Most depressive episodes in our sample occurred when the children were over 5 years of age. Studies have indicated that the younger children of depressed mothers are more affected. 34 Hence, the early development and attachment of the children may not have been affected badly by maternal depression.
Another possibility is that behavioral problems were lesser in the cases because of the less severe nature of illness in most mothers. Keller et al. 35 had shown that severe and more chronic depression in parents was associated with increased psychopathology and poor adaptive functioning in their children. The other key factor is that the mothers in our study were in remission. Weissman et al. showed that treating the mother’s depression can reduce children’s behavioral and emotional problems. 36 A meta-analysis of psychotherapeutic interventions for mothers with depression indicated that a successful treatment was associated with significant improvement in parent– child interaction and child’s mental health. 37 Other studies too had similar results,37,38 while some others reported that the successful treatment of maternal depression was not enough to prevent emotional disorders in children. 39 They have suggested adding parent–child interventions and parenting programs, such as enhanced Triple P. 40 At least one of the children of the control mothers was undergoing medical treatment at the time of assessment; these children could have a higher risk of behavioral difficulties, which could have colored the reporting and confounded the results.
Except for two separated families, all were from intact families. Other family members could have compensated for a reduction in mother’s functioning because of depression. In a longitudinal study, the father’s positive involvement was able to mitigate the impact of the mother’s depression on the child’s behavior. 41
When we combined the scores of different domains on the TMS 26 into the five-factor structure, namely sociability, emotionality, energy, distractibility, and rhythmicity, there was a trend that cases had poor scores on emotionality but higher scores on rhythmicity. The increased emotionality was something that was expected, but higher scores in rhythmicity were in contrast with the finding by Sameer et al., 18 who found lesser persistence, rhythmicity, and threshold for responsiveness compared to controls. This could be because, unlike other domain scores on TMS, rhythmicity scores on both extremes could indicate problems. For example, lower scores indicate irregularity, while the highest scores could indicate obsessiveness. Our results were dissimilar to a study by Weissman, 42 where cases had high energy, low sociability, and low adaptability compared to normal controls.
Previous studies42,43 have indicated that the severity of psychopathology in children increases with the number of episodes of illness in the parent. However, unlike the findings from Keller et al., 35 in our study, there was no relation between the severity of depression in the mothers and behavioral problems in children. In the STAR*D-child study, a history of suicide attempts in the mother and comorbid panic attacks with agoraphobia were associated with threefold and eightfold increased risk of depression in children. The majority of the mothers in this study (72%) had severe depression. 14
In our study, suicidal ideation, the number of episodes, age at the onset of illness, and illness duration did not correlate with the severity of the behavioral problems. This could be because our sample was largely from an outpatient population with milder illness and without too much variation in severity. An effective treatment could have also mitigated the effects of severity. Other studies have shown that the effective treatment and remission in the mother was associated with lesser psychopathology in the offsprings.36,44,45 But that was not the case in the study by Sameer et al., 18 who also included mothers in remission.
A previous study 33 found that boys tend to have more behavioral problems and girls more emotional difficulties. But we did not find any such difference between boys and girls. This could be because of the low levels of behavior problems overall. Also, there was no difference between age groups. Researchers had suggested that maternal psychopathology could impact the reporting of their child’s behavior problems 30 ; hence, we decided to include only mothers who were in remission. Raju et al., who studied the psychopathology of the children of parents with chronic mental disorders (over two years), had interviewed the patient’s asymptomatic spouse. 46 Sameer et al., who studied the children of mothers with affective disorders, too included those in remission only. 18
Because of practical issues with feasibility, we used a cross-sectional design. Other groups have also used cross-sectional methods on parents with unipolar depression.18,42,46,47 Like us, the Avon longitudinal study of parents and children 47 studied the behavioral and emotional problems in children using the SDQ, 24 while Sameer et al. 18 used child behavior checklist scores 48 and TMS. 27
Limitations
The cross-sectional design of the study was a significant limitation. Ideally, it would have been better to follow these children up into their early adult life to determine their risk for mental disorders. The design also limited the ability to study the potential bidirectional influence of maternal depression and childhood behavioral problems. Only maternal reports were obtained; it would have been better if information from the teacher and the other parent was also obtained, along with an interview of the children by a child and adolescent psychiatrist. Though mothers in both arms were from similar socioeconomic backgrounds, more details about their social situation, parenting, and other stressors could have helped control important confounders to improve the confidence in our findings. The hospital-based sample and mild severity limit the generalizability of the findings.
Conclusions
Contrary to expectations, the children of mothers with depression did not have increased behavioral problems compared to controls. Less severe symptoms, effective treatment, and the presence of supportive family members could have mitigated the risk. Further research with a longitudinal follow-up, focusing on mental health outcomes, is warranted to study the bidirectional influence between maternal depression and children’s behavioral problems.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.