
Abstract
Background:
Alcohol dependence occurs in about 9% of men in India. It is a major contributor to premature death and disability. Several clinical factors may play a role in the short-term outcomes of alcohol dependence.
Methods:
A total of N = 122 male patients with alcohol dependence as per ICD-10 DCR criteria were recruited in this study. They were assessed on socio-demographic and clinical parameters such as severity of alcohol dependence (SADQ), motivation to quit alcohol (SOCRATES), and global cognition (MoCA) and frontal cognition (FAB). The patients were then followed up at 1- and 3-month time points using the timeline follow-back method of enquiry into their last 30 days of drinking.
Results:
The mean age of the patients was about 40.6 (SD = 7.6) years. The duration of alcohol use was 18.56 years (SD = 7.22), and the average use was 14.14 units (SD = 8.62) per day. They had moderately severe dependence with SADQ scores of 25.13 (SD = 12.01). Two-thirds (n = 82) (67.2%) had low MoCA scores, and nearly one-fourth (n = 27) (22.1%) scored low on FAB. About 30% of patients relapsed at 1 month, and 50% relapsed by the end of 3 months. Earlier age at dependence (p = .012) was associated with relapse at 1 month. At 3 months, patients who were married (p = .040), had previous abstinence attempts (p = .003), and had higher MoCA scores (>26) (p = .042) were more likely to remain abstinent.
Conclusions:
About 30% of patients with alcohol dependence relapse within 1 month, whereas 50% relapse by the end of 3 months. Early age at onset of dependence predicted relapse at 1 month, and married status, past abstinent attempts, and intact global cognition predicted abstinence at 3 months.
Patients with alcohol dependence completing acute withdrawal management have a 30% rate of relapse at 1 month and 50% relapse at 3 months. Early age at onset of dependence predicted a greater risk of relapse at 1 month. Married men with past abstinence attempts and preserved global cognition were more likely to remain abstinent at 3 months. Clinical, cognitive, and social factors influence the short-term outcomes in patients with alcohol dependence.Key Messages:
Alcohol is widely recognized as one of the most commonly abused substances worldwide. Its consumption leads to short-term and long-lasting alterations in many neurochemical systems in the brain, resulting in harmful consequences when high usage is sustained over an extended period. 1 In the Indian setting, the lifetime risk of alcohol use disorders (AUDs) is 4.5%. The overall 12-month prevalence of AUDs among the Indian population was 2.6% in 2010, while the occurrence rate of alcohol dependence was 2.1% during the same year. 2 As per the findings of The National Mental Health Survey of India 2015–2016, 9% of adult males in India were diagnosed with AUDs. 2 Among people aged 20–39 years, around 13.5% of all deaths can be attributed to alcohol, as reported by the World Health Organization (WHO). 3 Thus, alcohol is a major contributor to premature deaths and disability. Previous studies have identified factors such as age, educational status, marital status, and employment status to be predictors of abstinence versus relapse. 4 Prolonged and excessive alcohol consumption leads to cognitive impairments that are associated with several brain abnormalities over time. This can disrupt the individual’s executive thinking processes, episodic memory, and visuospatial abilities. 5 The occurrence of cognitive impairments in alcohol-dependent patients ranges from 50% to 80%. These cognitive deficits also predict the long-term outcome and well-being of patients. 6 Prior research has shown a correlation between impaired frontal executive and global cognitive abilities and a lack of willingness to cease alcohol consumption. A study on 56 adult males with alcohol dependence found that 81% had overall cognitive impairment and 16% had frontal executive dysfunction. Older age was associated with lower FAB scores, whereas higher education was associated with higher MoCA and FAB scores. 5 In another study, the degree of alcohol dependence, as evaluated in previous studies by clinical assessment, along with the existence of cognitive impairments, was indicative of unfavorable outcomes, particularly during long-term follow-ups. 7
Therefore, we aimed to study the short-term outcomes of patients seeking treatment at an addiction clinic at a tertiary care teaching hospital in southern India. We also aimed to study the association of clinical factors, cognitive functions, and motivational levels with the short-term outcomes at 1- and 3-months.
Methods
Design and Settings
A prospective observational study was conducted in the Department of Psychiatry of Jawaharlal Institute of Postgarduate Medical Education and Research (JIPMER), Puducherry. This follow-up study was done over a period of approximately two years (from July 2021 to June 2023), including 3 months of follow-up after recruitment into the study. The study was conducted after obtaining approval from the Institute Ethics Committee for Observational Studies through approval number JIP/IEC-OS/2021/245 dated 4th August 2021. All the participants were recruited into the study after written informed consent was obtained, following an explanation of the study in their language (English/local language). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Guidelines were adhered to ensure optimal reporting of the study findings.
Patient Population
We recruited 122 patients diagnosed with Alcohol dependence Syndrome, as per the criteria outlined in the International Classification of Diseases, 10th edition, Diagnostic Criteria for Research (ICD-10 DCR). The patients were recruited from the Psychiatry Department of our hospital, both in-patient and out-patient, based on the following inclusion and exclusion criteria. Male patients who are 18–50 years old and diagnosed with alcohol dependence syndrome as per the ICD-10 DCR and who are familiar with reading and writing in both Tamil and English have been included in the study. The patients had completed acute phase management of their withdrawal symptoms, and benzodiazepines were stopped at the time of assessment.
The exclusion criteria were as follows: patients who were dependent on other psychoactive substances (apart from alcohol and nicotine), those with severe and unstable conditions such as decompensated chronic liver disease, acute kidney injury, chronic kidney disease, congestive heart failure, or those with neurological conditions such as stroke or dementia, which could make it challenging to evaluate the patient. Additionally, any evidence of cognitive impairment documented through clinical assessment or a documented IQ test report also served as an exclusion criterion.
Sample Size Estimation
Assuming that about 50% of patients without cognitive dysfunction will relapse and that about 80% of patients with cognitive dysfunction will relapse at the end of 3 months, using the Power and Sample Size (PS) calculator for two proportions with 80% power and at 5% level of significance, we required a sample size of 120. With a dropout rate expected to be 10% we required a sample size of 132.
Assessments Done
Socio-demographic and clinical variables were collected through a comprehensive clinical assessment using a semi-structured proforma. The interview was conducted in a single sitting for outpatients and prior to discharge for inpatients.
The following psychometric tools were applied for the assessment of the clinical profile of the patients:
Severity of Alcohol Dependence Questionnaire (SADQ) 8 : The questionnaire consists of 20 items, divided into five subscales. Each item is scored on a four-point scale, ranging from “Almost never” to “Nearly always.” A score of more than 30 out of 60 indicates severe Alcohol Dependence. The test takes about 5 minutes to administer.
Montreal Cognitive Assessment test (MoCA) 9 : The MoCA for Global cognitive functions is studied under eight sub-categories. The testing process lasted around 10 minutes, and it has a maximum achievable score of 30. A score below 26 denoted an impairment.
Frontal Assessment Battery (FAB) 10 : The FAB is a six-item test designed to assess various functions of the Frontal lobe. The administration of the test typically requires approximately 5 minutes, and the highest achievable score is 18. A score lower than 12 suggests impaired frontal lobe functions.
Stages of Change Readiness and Treatment Eagerness Scale (SOCRATES) 11 : The SOCRATES has 19 items designed to assess the level of readiness for change in patients who have a dependency on a substance or behavior. The administration process takes approximately 5 minutes. The assessment provides three sub-scores: Recognition, Ambivalence, and Taking steps. These sub-scores aid in identifying the different stages of motivation. The patients were instructed to schedule a follow-up appointment at the psychiatry outpatient department (OPD) every 2–4 weeks, as determined by the treatment team.
Follow-up
Follow-up assessments were done at 1- and 3-months. This assessment involved obtaining data on the user’s current alcohol consumption within the past 30 days, including any instances of relapse. The average amount consumed each day was determined using the Timeline Follow Back Method. The follow-up was done telephonically for patients who had dropped out of follow-up. Enquiry was made from the patient and a caregiver—either spouse (for married patients) or parents or siblings (for single or divorced patients) as far as possible. However, reporting bias could not be eliminated. Participants who reported no alcohol use since the initial baseline assessment were considered abstinent. Those who had any alcohol use after the initial assessment were considered relapsed. During the period of follow-up, patients continued to receive treatment-as-usual, which included 50 minutes of group therapy sessions, 50 minutes of yoga and pranayama sessions, followed by medical follow-up. The patients were prescribed one of the following medications for relapse prevention as per the decision of the treating clinician: baclofen (30–60 mg/d), acamprosate (1332–1998 mg/d), naltrexone (50 mg/d), or disulfiram (250 mg/d). The frequency of follow-up was once in 2 to 4 weeks, as per the treating clinician’s discretion.
Statistical Analysis
All the categorical variables in the study, such as socio-economic status, nature of employment, type of alcohol, and relapse status, were summarized as frequency and percentage. All the continuous variables in the study, such as quantity of alcohol and frequency of consumption, were summarized as mean with standard deviation or median with interquartile range, depending on the variable’s distribution. The normality of the continuous variables was assessed using the Kolmogorov–Smirnov test. The association between the categorical variables and the relapse status was evaluated using either the | 2 test or Fisher’s exact test. The comparison of continuous variables between patients with and without relapse was tested using either an independent sample t-test or a Mann–Whitney U test, depending on the distribution. The analyses were conducted at a significance level of 5%, and a p value lower than .05 was considered statistically significant. Since all patients were followed up over the phone, there were no drop-outs or missing data.
Results
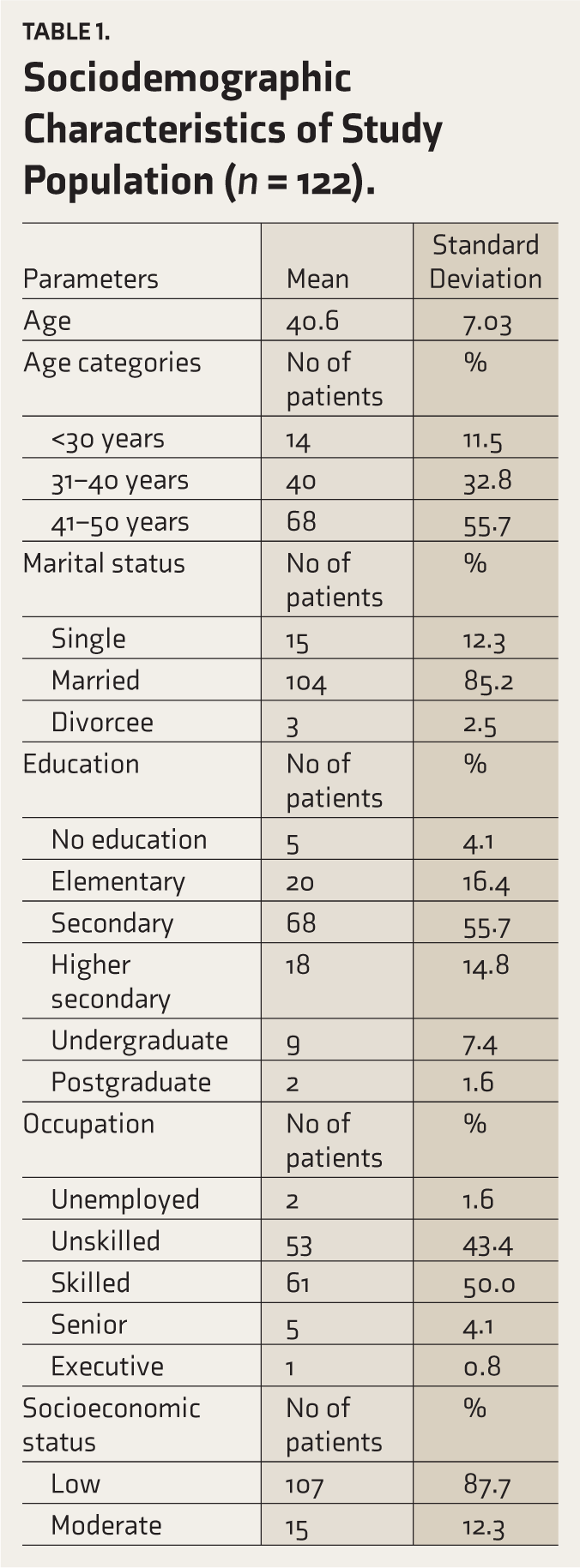
A total of 122 patients were recruited for the study. The mean age of the patients was 40.6 years (SD = 7.03). A majority of the patients were married (85.2%), had secondary school education (55.77%), were unskilled primarily (43.4%) or skilled (50%) workers, and mostly belonged to a lower socio-economic state (87.7%). The socio-demographic profile of the participants is detailed in Table 1.
Sociodemographic Characteristics of Study Population (n = 122).
As regards the clinical characteristics of the participants (Table 2), the mean age at the development of dependence was 30.67 years (SD = 8.68). The patients had, on average, been using alcohol for 18.56 years (SD = 7.22) and consuming about 14.14 units (SD = 8.62) per day. At the time of assessment, they had completed a course of detoxification and had consumed alcohol on about 10 days in the last 30 days.
Clinical Characteristics of Study Population (n = 122).
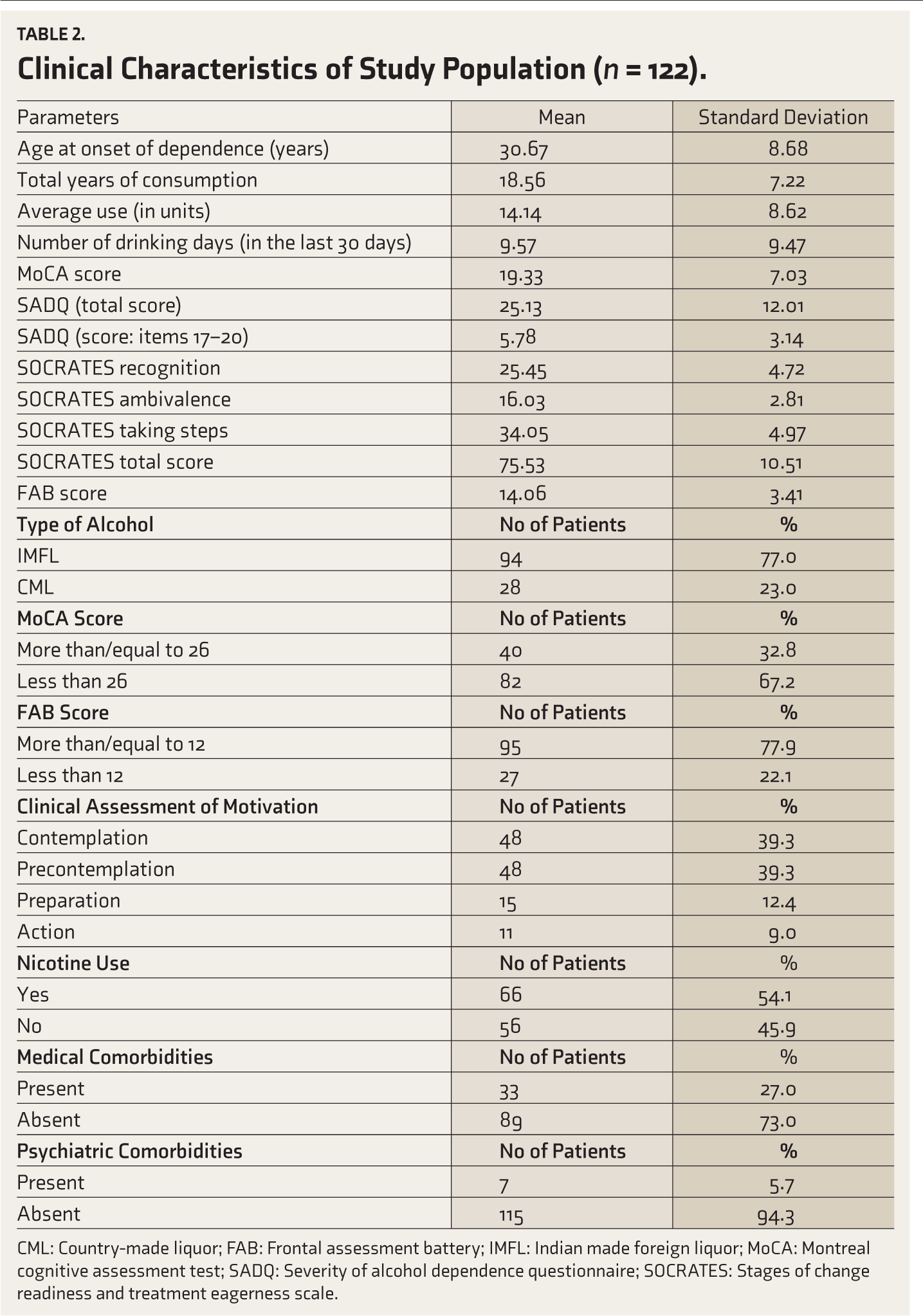
CML: Country-made liquor; FAB: Frontal assessment battery; IMFL: Indian made foreign liquor; MoCA: Montreal cognitive assessment test; SADQ: Severity of alcohol dependence questionnaire; SOCRATES: Stages of change readiness and treatment eagerness scale. Most of the patients had moderate to severe dependence, with a mean SADQ of 25.13 (SD = 12.01). At baseline, 67.2% (n = 82) had a MOCA score below the cut-off of 26, indicating global cognitive impairment. With respect to frontal cognitive impairment, n = 27 (22.1%) had an FAB score of less than 12, indicating frontal executive dysfunction. Most patients were in precontemplation or contemplation.
Short-term Mortality
At the end of 1 month, one patient had expired, and the other could not be contacted over the telephone. One more patient had expired at the end of 3 months; hence, 1/122 (0.81%) patients were lost to follow-up, and 2/122 (1.62%) had expired within 3 months.
One-month Outcomes
At 1 month, 32% (n = 39) of patients relapsed. Those who relapsed were more likely to have a lower age at onset of dependence, less than 30 years (27.95 years), whereas the abstinent group of participants had an age at onset of dependence that was more than 30 years (32.19 years) (Table 3). This difference was found to be statistically significant, with a p value of .012. Low MoCA scores (below the cut-off of 26) were seen more often among patients who relapsed at 1 month than those who remained abstinent (80% vs. 60%; p = .05). However, FAB scores did not predict 1-month outcomes (Table 4).
Comparison of Socio-demographic Characteristics Between Abstinent and Relapsed Groups at One- and Three-month.

CML: Country-made liquor; IMFL: Indian made foreign liquor; MoCA: Montreal cognitive assessment test; FAB: Frontal assessment battery.
Three-month Outcomes
At 3 months, 49.2% (n = 60) had relapsed, and the study found that married participants had a higher likelihood of abstaining from alcohol at the conclusion of the 3-month follow-up compared to other participants (53.9% vs. 46.1%; p = .040) (Table 3). The MoCA scores were more likely to be below the cut-off of 26 among patients who relapsed than those who remained abstinent at 3 months (76% vs. 68%; p = .042). However, FAB scores did not predict 3-month outcomes (Table 4).
Comparison of Clinical Characteristics Between the Abstinent and Relapsed Groups at One- and Three-month.
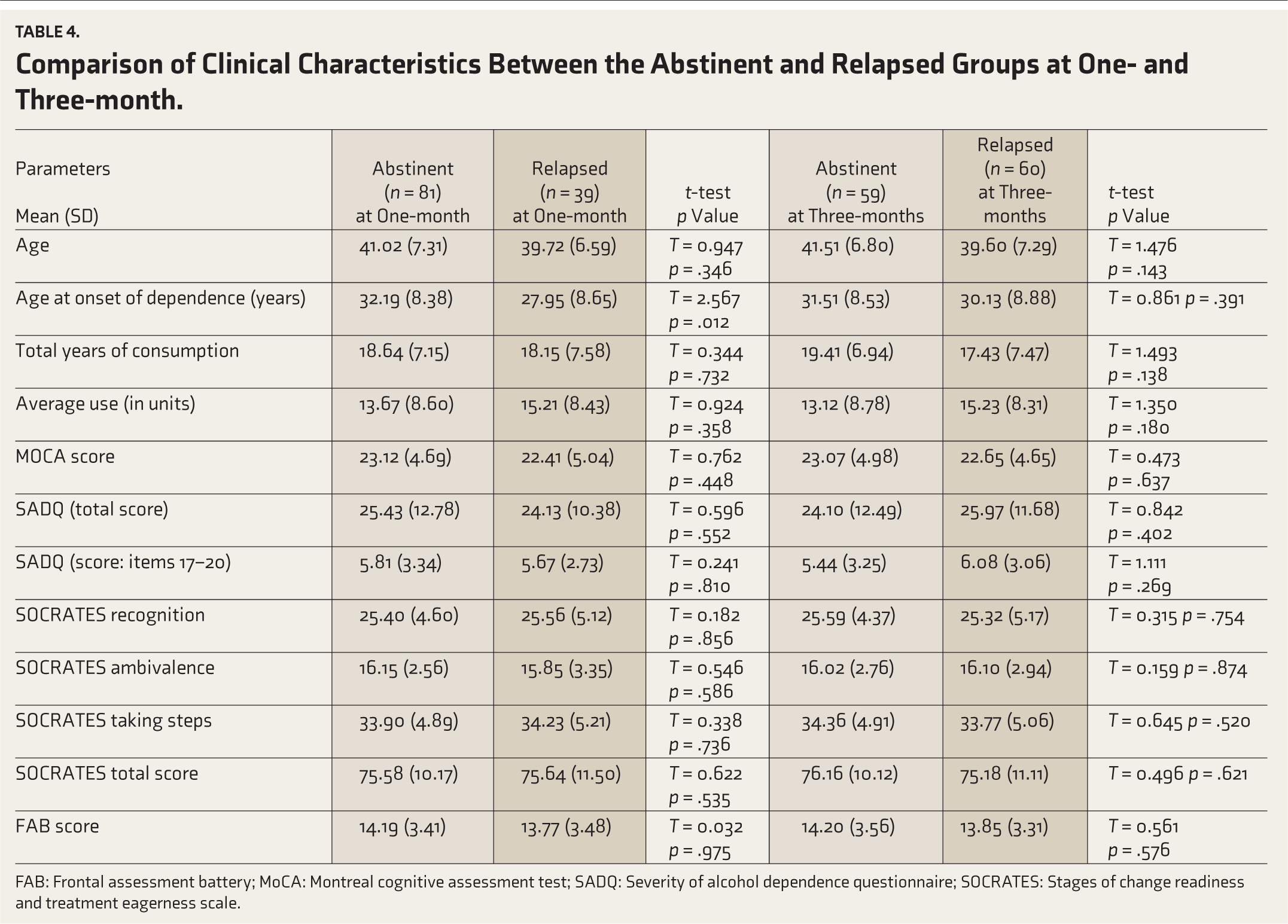
FAB: Frontal assessment battery; MoCA: Montreal cognitive assessment test; SADQ: Severity of alcohol dependence questionnaire; SOCRATES: Stages of change readiness and treatment eagerness scale.
In addition, those participants who had remained abstinent at 3 months were more likely to have had previous significant abstinence attempts (lasting at least 4 weeks) (91.5% vs. 70%; p = .003).
Discussion
Alcohol dependence has a chronic relapsing course, with some studies suggesting a 9-year abstinence rate of over 50% and a re-employment rate of 60% in participants. 12 However, few naturalistic follow-up studies have examined short-term outcomes after treatment for AUD. A systematic review of Indian studies found relapse rates ranging from 3.4% to 90%, with significant heterogeneity among studies. The median time period of follow-up in these studies ranged from 1 to 36 months. 13
Outcomes at the End of One Month
Younger age at the onset of dependence was associated with a greater likelihood of relapse at 1 month. This may be related to a more severe course of illness in those with an earlier age at onset.
However, the study found no significant association between marital status and short-term outcomes at the end of 1 month. Previous studies have found socio-demographic factors like higher education levels and higher socio-economic status to be key predictors of treatment outcomes.14,15
Outcome at the End of Three Months
The study found that marital status was a significant predictor of relapse in alcohol dependence treatment, compared to other socio-demographic factors like age, alcohol use, occupation, education levels, or socio-economic status. This finding is consistent with previous studies that found social support to be positively associated with abstinence.16–18 Therefore, it indicates that single patients with alcohol dependence are more likely to relapse and should be provided greater social support for the initial 3- to 6-month period, with family members also involved in the treatment process. The present study found that the global cognitive impairment, as indicated by MoCA scores below 26, was associated with relapse at 3 months (p = .042) but not at 1 month (p = .052). This finding supports previous research, which found that poor cognitive performance is associated with poor outcomes in alcohol dependence. Poorer cognitive functioning was also linked with problem drinking at 6-month follow-ups and a higher risk of lapse over 12-month follow-ups.19–21
Cognitive impairments in substance use disorders ranged from 30% to 80%, indicating the impact of AUD on neuropsychological well-being. 22 Neurocognitive risk factors for poorer outcomes can be identified early in alcohol dependence treatment. 5 Cognitive impairments, such as frontal executive dysfunction and global cognitive impairments, are common among patients with alcohol dependence. Motivation to quit alcohol requires patients to recognize their alcohol use as a problem, similar to anosognosia in certain neurological disorders or lack of insight in psychosis. In a previous cross-sectional study, frontal cognitive impairment predicted poorer motivation to quit alcohol, but global cognitive impairment did not predict motivational state. 5 However, in our study, we found that global cognitive impairment as determined by low MoCA scores predicted relapse at 3 months. We did not find an association between frontal lobe dysfunction and risk of relapse at 1- and 3-months. In our study, patients with previous significant abstinence were more likely to remain abstinent at the 3-month follow-up. Other factors like patient age, alcohol type, occupation, education levels, or socio-economic status did not predict abstinence.
Strengths
The present study enrolled 122 patients who were followed up during in-person visits or through telephonic follow-up, which reduced the dropout rates. This active follow-up through telephonic contact was an advantage, as clinicians usually do not know the outcomes of patients who drop out. This also helped us to identify two deaths within a span of 3 months. The cause of death could not be ascertained clearly. Therefore, this follow-up study is more generalizable to real-world practice as patients who dropped out of follow-up were also contacted and their outcomes have been assessed through telephone.
Limitations
The study has limitations due to the lack of data on in-person follow-up visits and self-reported outcomes of patients, which may not be reliable. It could have been improved by including objective measures like gamma-glutamyl transferase (GGT) levels. The medication prescribed and the dose were not analyzed for their influence on outcomes.
Conclusions
The study found that younger age at onset of dependence was associated with relapse at 1-month but not at 3-months. Being married and having previous abstinence attempts were associated with abstinence at 3 months but not at 1 month. None of the other socio-demographic attributes, clinical measures, and motivation levels were associated with relapse at either the 1- or 3-month time point.
Two patients had expired (one within 1 month, and another one before the 3-month follow-up time point), which points to a significant (~1.6%) mortality rate within 3 months of seeking treatment.
Global cognitive impairment, but not frontal cognitive dysfunction, was significantly associated with relapse at 3 months. Therefore, assessment of cognitive functions must be considered in every patient with alcohol dependence, as it may have prognostic value and also guide the nature and intensity of psychological and pharmacotherapeutic interventions.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
This study was approved by the Institutional Ethics Committee for Observational Studies of the Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry 605006, through approval number JIP/IEC -OS/ 2021/245 dated August 4, 2021.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
All participants included in this study provided written informed consent prior to being included in to the study.
Prior Presentations
The study findings have not been presented at any conferences.
Simultaneous Submission to Another Journal or Resource
The manuscript or any other manuscript from the study is not presently under consideration for publication in any other journal or resource.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.