
Abstract
Background:
Dysfunctional basic cognitions have been suggested as potential vulnerability markers for alcohol dependence (AD). Although there is a growing body of research on the role of distal cognitive vulnerability factors such as early maladaptive schema in the development of AD, little is known about the role of proximal cognitive factors such as cognitive distortions, dysfunctional attitude, and negative automatic thoughts.
Methods:
This comparative cross-sectional study aimed to examine dysfunctional cognitions in individuals with AD (n = 84) in comparison with healthy individuals (n = 60). The dysfunctional cognitions were assessed on the Young Schema Questionnaire third version of Short Form, Cognitive Distortion Scale, Dysfunctional Attitude Scale-Form A, and Automatic Thought Questionnaire. Multivariate analysis of covariance was conducted to analyze the group differences in dysfunctional cognitions.
Results:
After controlling for the group difference in employment status, 12 of 18 schemas were more prevalent in individuals with AD than in healthy individuals. Individuals with AD also scored higher on seven of 10 cognitive distortions, as well as in terms of dysfunctional attitude and negative automatic thoughts.
Conclusion:
Dysfunctional cognition may play a significant role in developing AD. The findings may enhance our understanding of the nature and severity of dysfunctional cognitions in the development of AD. The information may further assist the clinicians in implementing adequate intervention strategies to manage dysfunctional cognitions in individuals with AD.
Keywords
The first study comprehensively examining dysfunctional cognition in alcohol dependence (AD) in the Indian context. Individuals with AD scored higher on dysfunctional cognitions than healthy individuals. This information may assist the clinicians in implementing adequate strategies to manage dysfunctional cognitions.Key Messages:
Alcohol is a widely used psychoactive substance with associated adverse consequences.1, 2 Despite addressing a wide range of causal factors, there is still a significant risk of relapse following treatment.3, 4 Accordingly, more information regarding vulnerability factors for alcohol dependence (AD) is of major importance to address and manage the condition.
The cognitive model stresses the importance of cognitive processes as a potential vulnerability factor in the development of substance abuse. However, the role of dysfunctional fundamental cognition has been studied to a limited extent. 5 Previous studies on the cognitive perspective have mostly focused on the significance of distal vulnerability factors (developmental antecedents) such as early maladaptive schemas (EMS) in relation to substance abuse.6, 7 However, dysfunctional cognition comprises not only the distal vulnerability factors but also the proximal vulnerability factors such as cognitive distortions, dysfunctional attitude, and negative automatic thoughts. 8 Young et al. 9 proposed an interplay among all the factors of cognition, as schemas are perpetuated via the mechanism of cognitive distortions. Through this mechanism, people ignore or suppress the emotions associated with the schema, and as a result, make no effort to recognize and change the schema. Further, these schemas are reflected by the content of dysfunctional attitude. 10 Therefore, examining the interplay among all these cognitions in connection to AD seems warranted.
To date, few studies have investigated the EMS in alcohol and other substance use disorders (SUDs). Brotchie et al. 11 compared the EMS among those who use alcohol (n = 44), opiate (n = 36), combined alcohol and opiate, and a nonclinical group. They reported a higher prevalence of 11 out of 15 schemas in the clinical groups than in the nonclinical group, particularly among those who use alcohol. Later, Roper et al. 6 examined EMS specifically among individuals with AD (n = 50) and a nonclinical population (n = 50). They reported findings consistent with Brotchie et al. 11 Shorey et al. 7 compared the schemas of young males (n = 101) in residential substance abuse treatment with a nonclinical group (n = 175) and reported that the substance abuse group scored higher than the nonclinical group on 9 of the 18 EMS. However, the role of proximal factors of cognitions in SUDs has received less attention. Najavits et al. 12 reported a higher level of cognitive distortions in a dual diagnosis group of females (post-traumatic stress disorder [PTSD] and SUD) than in a single diagnosis group (PTSD alone). Furthermore, studies had observed higher severity of dysfunctional attitudes among people with substance abuse than in a nonclinical population.13, 14
Literature suggests an impact of the cultural difference on our thinking process. 15 The cultural difference thus calls for the need to evaluate cognition in the cultural context of India. Therefore, this study attempted to comprehensively evaluate dysfunctional cognitions in individuals with AD by comparing their distal to proximal vulnerability factors with those of healthy individuals. The findings may enhance our understanding of the nature and severity of dysfunctional cognition in the development of AD and may assist the clinicians in implementing adequate strategies to manage dysfunctional cognitions in cases of AD.16, 17
Material and Methods
Ethical Consideration and Study Design
The institute ethics committee approved the study. This was a comparative cross-sectional study where a group of individuals with AD syndrome (alcohol dependence group—ADG) was compared with a healthy control group (HCG) in terms of their dysfunctional cognition.
Participants
Study participants were recruited from January 2016 to March 2018. The study involved two groups of participants. Individuals with ADS were recruited from a WHO-collaborated national drug dependence treatment center (NDDTC) in North India. They were diagnosed as per ICD-10 criteria (WHO) 18 by consultant psychiatrists and were seeking inpatient or outpatient treatment for the same. The participants had to be males between 20 and 50 years with basic reading and writing abilities. Participants were excluded if they had any major psychiatric disorder or other SUDs in the past or present (except for nicotine) as screened on Mini-International Neuropsychiatric Interview (MINI) 7.0.1. 19 The MINI screens a total of 17 most common psychiatric disorders, including depression and anxiety disorders. Participants were also excluded if they had a serious medical condition, based on their self-report, or an ongoing withdrawal state that could interfere with the assessment process.
In addition, healthy individuals were recruited from clinical (patients’ relatives or informants) or community setups. A total of 87 persons who matched on age and education criteria using the pairwise matching method were contacted for their participation in the study. The procedure followed was identifying a group of healthy individuals closest in age and education level to the ADG participants. Participants were further screened on Alcohol Use Disorders Identification Test (AUDIT) 20 and General Health Questionnaire-12 (GHQ-12). 21 They were excluded if they scored >7 on AUDIT (score <8 indicates no use to occasional use of alcohol) and >3 on GHQ-12 (a score >3 shows the possibility of mental health problems).
Assessment
Sociodemographic Datasheet
This was developed to obtain the participants’ sociodemographic details, including age, education, marital status, religion, socioeconomic status (using Kuppuswamy socioeconomic status scale), 22 and employment status.
Young Schema Questionnaire-Version 3-Short Form (YSQ-3SF) 9
YSQ-3SF is a 90-item self-report instrument that measures 18 different EMS categorized into five domains of disconnection and rejection, impaired autonomy and performance, other directedness, impaired limits, and over vigilance and inhibition. Each of these schemas is represented by five items each. Individuals complete the questionnaire using a 6-point Likert scale: 6 = describes me perfectly, 5 = mostly true of me, 4 = moderately true of me, 3 = slightly more true than untrue, 2 = mostly untrue of me, and 1 = completely untrue. The score on each schema varies from 5 to 30. Higher scores on a schema indicate a higher presence of that schema. YSQ-3SF has a strong Cronbach’s coefficient (α) of 0.84 in the Indian population. 23
Cognitive Distortions Scale (CDS) 24
CDS is a 20-item self-report, Likert-type scale to measure 10 cognitive distortions using a 7-point scale (1 = never, 7 = all the time). Each cognitive distortion is rated in two domains: interpersonal (IP) and personal achievement (PA). Hence, the score for each distortion lies in the range from 2 to 14. A higher score for a distortion indicates a more frequent presence of that distortion. The CDS has a good internal consistency (Cronbach’s α = 0.85–0.91). 24
Dysfunctional Attitude Scale-Form A (DAS-A) 25
This is a 40-item self-report instrument to assess the intensity of dysfunctional attitudes. The items are rated on a 7-point Likert scale (7 = fully agree; 1 = fully disagree). The total score ranges from 40 to 280. A higher score on DAS-A reflects a higher severity of dysfunctional attitudes. It has an internal consistency coefficient of 0.91, and an assessment of the test-retest stability had revealed a reliability coefficient of 0.71. 25
The Automatic Thought Questionnaire (ATQ) 26
The ATQ is a 30-item self-report instrument that measures the frequency of automatic negative thoughts. Each item represents a thought, and the respondents rate the frequency of this thought on a 5-point scale ranging from 1 (not at all) to 5 (all the time). The total score on ATQ is from 30 to 150; a higher score indicates a higher frequency of automatic thoughts. The ATQ exhibits a high split-half reliability coefficient (0.97) and a high coefficient alpha (0.96). 26
Procedure
The nature and purpose of the study were explained to all participants. Written informed consent was obtained. All the self-rated measures were translated into Hindi using the WHO translation-back translation guidelines, emphasizing concise conceptual translation. Two bilingual individuals first translated the tools from English to Hindi independently. After that, a bilingual expert panel (psychologists, psychiatrists, and mental health researchers) performed a review of these translations, discussed discrepancies, and prepared a revised version. Two different translators back-translated the revised version into English independently, and the expert panel again reviewed the back-translations. The final version was produced after ensuring the validity of the new English version by comparing it with the original version of the tools. At the final step, a pretesting of the Hindi version of the tools was conducted on five of the AD participants, and based on the feedback, modifications were incorporated into the final versions of the tools. A licensed clinical psychologist (G.S.) conducted a one-time assessment on all the measures of dysfunctional cognition. It took approximately 2 h to complete the assessment, and individuals were given breaks during the assessment.
Statistical Analysis
Statistical analysis was carried out using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA). Baseline sociodemographic continuous and categorical data were analyzed using the independent sample t-test and chi-square test, respectively. Normality of data was tested using Kolmogorov–Smirnov test. The general linear model one-way multivariate analysis of covariance (MANCOVA) was carried out to examine the group difference in the measures of dysfunctional cognitions after controlling for the difference in employment status because there was a significant difference between the groups in their employment status. Statistical significance was set at P < 0.05 for the Bonferroni adjusted P-values. Effect sizes were calculated using Cohen’s d. Effect sizes of 0.20 were interpreted as small, 0.50 as a medium, and 0.80 as large. 27
Results
Using purposive sampling, a total of 125 participants diagnosed with AD were assessed for their eligibility in the study, of which 22 denied participation, 14 did not meet the inclusion criteria, and five were excluded because of incomplete data on the study measures. Thus, the final sample involved 84 participants in the ADG.
In HCG, 12 of the 87 participants denied their participation in the study. Seven participants were excluded following the screening process, and eight were excluded because of incomplete data on study measures. The final sample included a total of 60 healthy participants.
As shown in Table 1, the mean (±SD) age (in years) of participants of the ADG and the HCG was 36.37 (±7.02) and 34.18 (±7.09), respectively. Most of the participants were educated between 10th to 12th standard, belonged to lower-middle socioeconomic status, were Hindu, and were married. The two groups were comparable in terms of their sociodemographic characteristics. However, they differed significantly on their employment status (P = 0.02). In addition, the clinical profile of the ADG participants revealed that their mean age of initiation of alcohol use was 19.14 (±4.77) years, and the age of onset of daily use of alcohol was 29.54 (±7.25) years. ADG predominantly (57.86%) drank Indian-made foreign liquor (IMFL), with an average amount of alcohol consumption of around 22 units per day. A total of 63% of the ADG had at least one successful abstinence attempt in the past. Of the ADG, 2.4% had a family history of psychiatric illness and 43.3% had a family history of SUD. In addition, 10.7% of them had a history of past psychiatric illness.
Group Comparison of Sociodemographic Characteristics
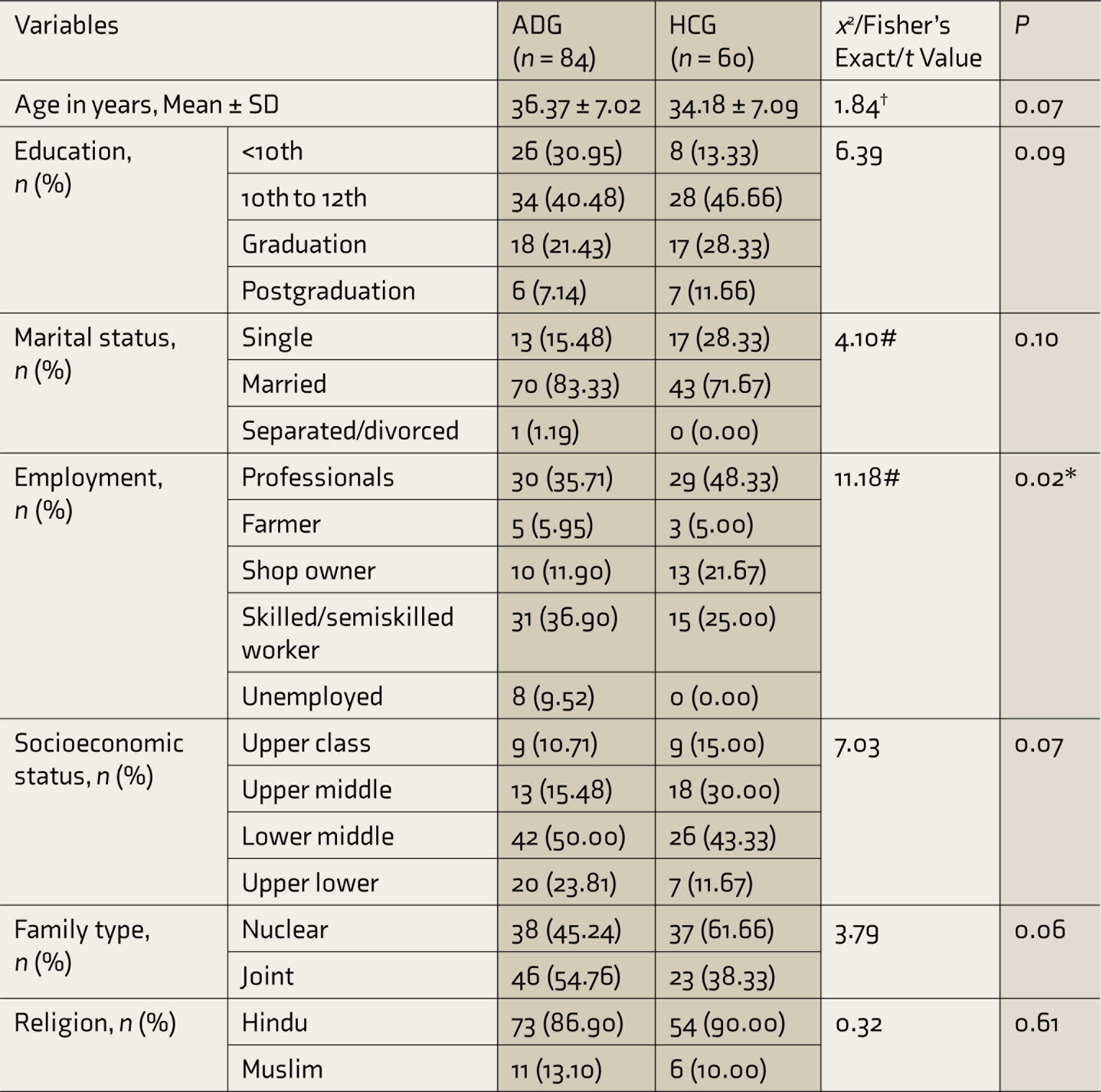
*Significant at P < 0.05, #Fisher’s exact test statistics, †t value.
SD: standard deviation; ADG: alcohol dependence group; HCG: healthy control group.
A MANCOVA showed that the group difference on the dysfunctional cognitions (combined dependent variable) was significant after controlling for the difference in employment status: F (30, 110) = 33.08, Wilks’ Lambda = 0.10, P < 0.001. The employment difference between the two groups was also significant, F (90, 330) = 1.54, Wilks’ Lambda = 0.35, P = 0.003, which indicated that employment status had a significant confounding effect on the dysfunctional cognition (dependent variables). On the measures of cognition, MANCOVA revealed the following findings:
Group Comparison on YSQ-3SF
ADG scored significantly higher on 12 of 18 EMS of emotional deprivation, abandonment, mistrust, dependence, vulnerability to harm, subjugation, self-sacrifice, approval seeking, entitlement, insufficient self-control, negativism, and punitiveness (Table 2). Effect size difference for these schemas fell into the small to large range.
Group Comparison on the Early Maladaptive Schema
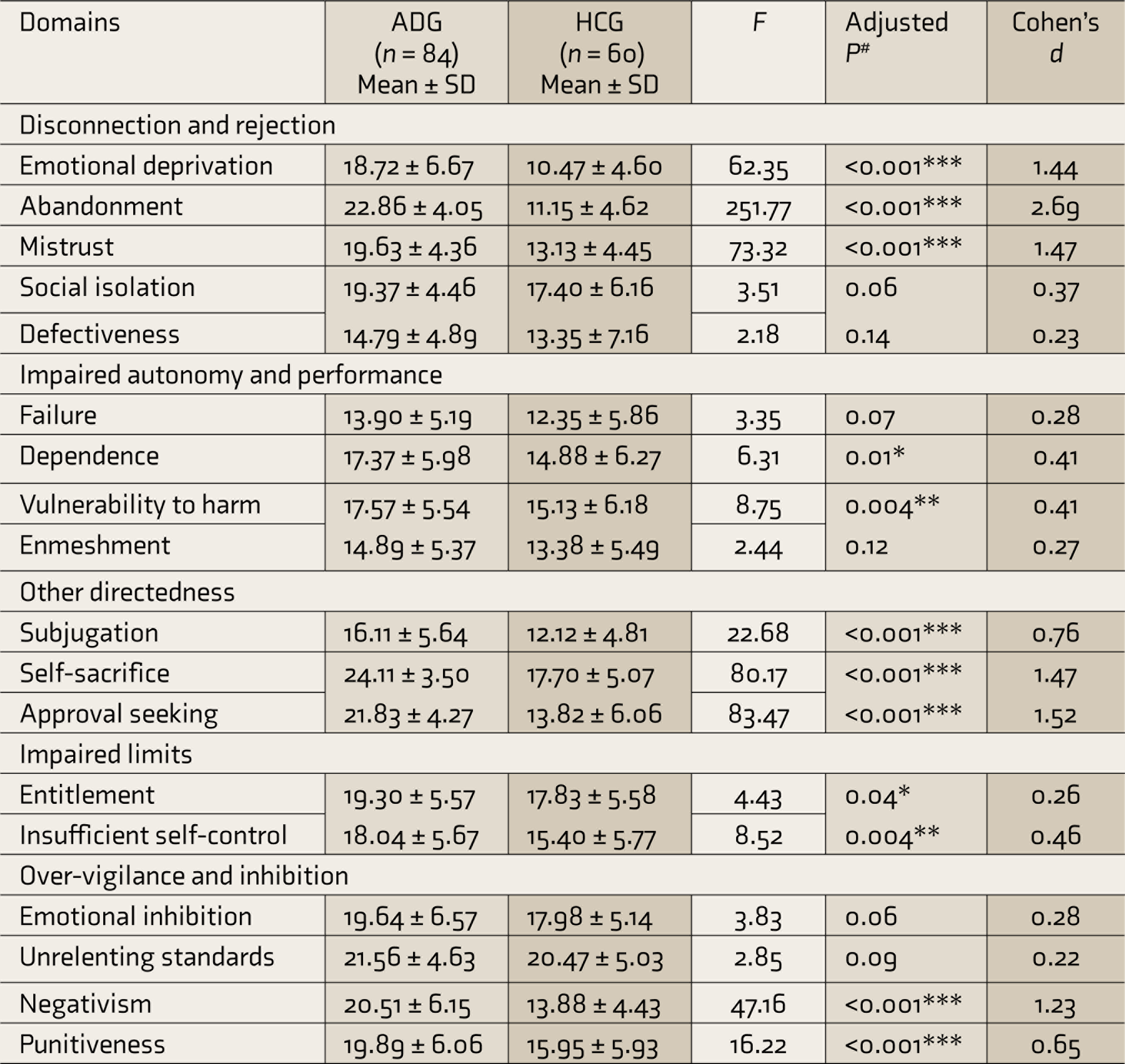
*Significant at <0.05 level, **significant at <0.01 level, ***significant at <0.001 level,
#adjusted P-value using Bonferroni correction.
SD: standard deviation; ADG: alcohol dependence group; HCG: healthy control group.
Group Comparison on CDS
ADG scored significantly higher on seven of the 10 cognitive distortions of mind reading, catastrophization, all or null thinking, labeling, mental filter, personalization, and should statement (Table 3). Effect sizes for these cognitive distortions were observed to be mostly in the large range.
Group Comparison on Cognitive Distortions
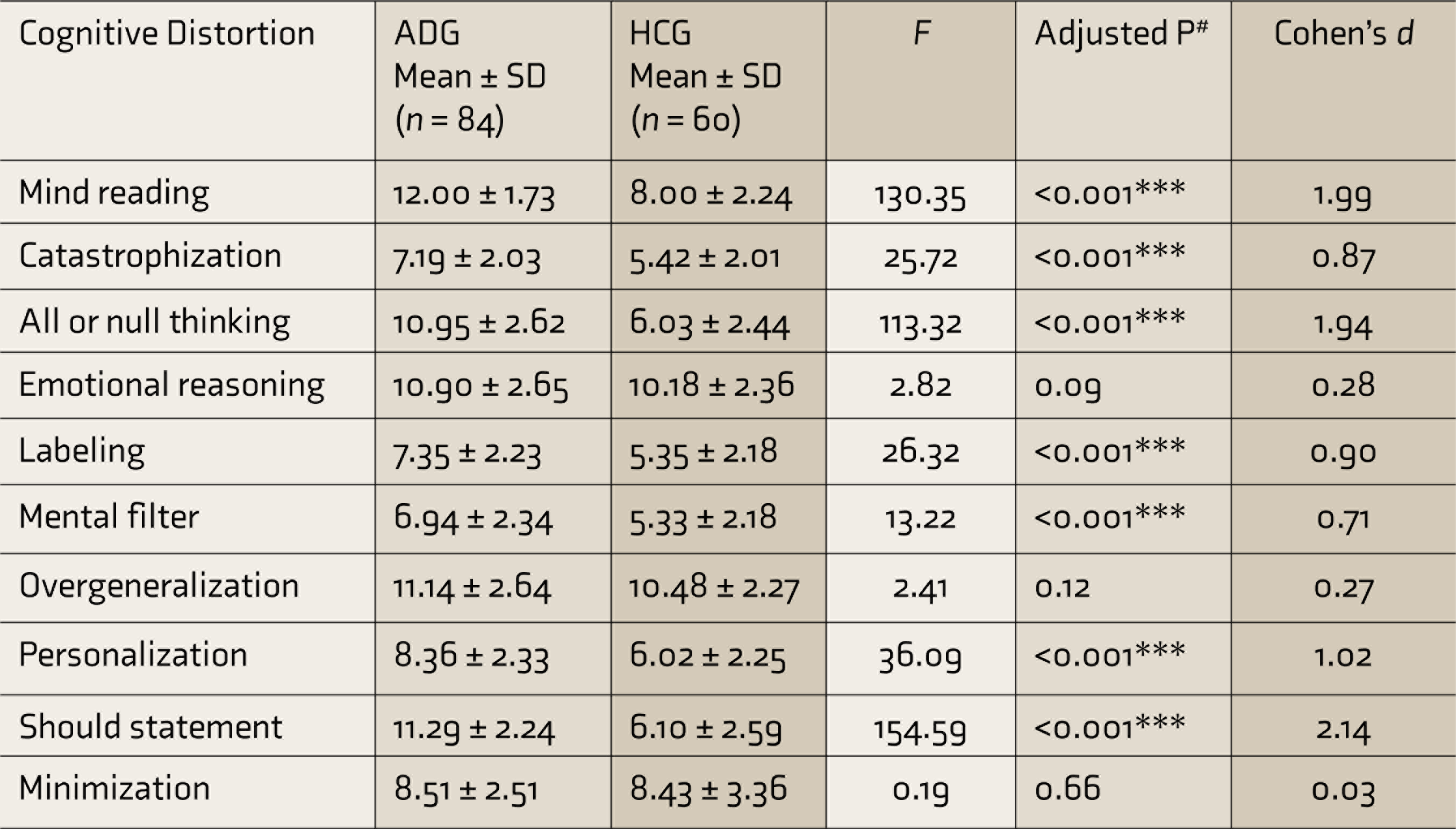
***Significant at <0.001 level, #adjusted P-value using Bonferroni correction.
SD: standard deviation; ADG: alcohol dependence group; HCG: healthy control group.
Group Comparison on DAS-A and ATQ
Analysis showed a significant difference between ADG (M = 186.86) and HCG (M = 127.83) on their total score for DAS F (1, 110) = 153.87, P < 0.001, d = 2.17, with higher severity of dysfunctional attitude among ADG. ADG (M = 78.87) and HCG (47.33) also differed significantly on the total score for ATQ F (1, 110) = 85.26, P < 0.001, d = 1.71, with a higher frequency of negative automatic thoughts in the ADG.
Discussion
To our knowledge, this is the first study to comprehensively examine dysfunctional cognitions by incorporating all the layers of cognitions among individuals with AD in comparison with healthy individuals. Moreover, no research has so far been conducted in our cultural context on dysfunctional fundamental cognition in connection to SUD. Understanding the nature of dysfunctional cognitions in the Indian context might be enlightening as culture impacts how we process information available in our surroundings. 15 After controlling for the group difference in employment status, the study revealed that ADG scored significantly higher on most of the proximal to distal factors of dysfunctional cognitions.
ADG scored significantly higher on 12 of the 18 EMS. These findings are consistent with previous research that demonstrated a higher prevalence of the majority of EMS among those with substance abuse when compared to the nonclinical population.6, 7, 11 The schemas that differed between the two groups were schema of emotional deprivation, abandonment, mistrust, dependence, vulnerability to harm, insufficient self-control, negativism, and punitiveness. In addition, surprisingly, some of the schemas relatively distinct in nature, such as entitlement, subjugation, self-sacrifice, and approval seeking, were also more prevalent in ADG. The presence of a higher level of entitlement schema could be overcompensation for their feeling of inadequacy and emotional deprivation.9, 28 Similarly, a higher level of subjugation, self-sacrifice, and approval seeking could reflect an individual’s proclivity to compensate for the other preexisting maladaptive schemas. 9
It is illuminating to highlight the three schema domains that were highly prevalent in the ADG. The schema domain of “disconnection and rejection” shows that people who endorse these schemas are likely to have had painful childhood experiences and, as adults, they could be involved in different self-destructive relationships or prefer absolute detachment from others. Literature shows that traumatic childhood experiences and difficulties in the interpersonal relationship contribute to the development of problematic substance abuse.29, 30 The “impaired limit” domain indicates an individual’s impulsive behavior, low frustration tolerance, and narcissistic tendency. 9 Research has revealed these characteristics to be common among people with problematic substance use.31–35 The domain of “other directedness” depicts an individual’s excessive concentration on the desires and feelings of others at the expense of one’s own needs for love and approval or to escape reprisal. 9 These characteristics are commonly witnessed among people with passive dependent traits and have been linked to subsequent risk of AD.32, 34
Young et al. 9 proposed that the mechanism of cognitive distortions perpetuates EMS by allowing people to exaggerate some information that supports the schema while minimizing information that contradicts it. Thus, in individuals with AD, higher severity of EMS may suggest a higher number of cognitive distortions. This study revealed that ADG scored higher on seven of 10 cognitive distortions. The list included mind-reading, catastrophization, all or null thinking, labeling, mental filter, personalization, and should statements. Ellis et al. 36 elaborated on the role of cognitive errors specific to substance abuse, which involved the use of all or null thinking, overgeneralization, and absolute thinking. Further, Najavits et al. 12 reported higher levels of cognitive distortion in the group that had both PTSD and SUD (n = 102) than one with PTSD alone (n = 27).
This study further demonstrated a higher severity of dysfunctional attitude and negative automatic thoughts in ADG. Literature shows that dysfunctional attitude is simply a reflection of the content of schemas. 10 As a result, higher severity of EMS may confirm the presence of a more severe dysfunctional attitude in individuals with AD. This finding is consistent with previous research that revealed higher severity of dysfunctional attitude among substance-dependent populations than in the nonclinical population.13, 14 It is postulated that holding negative views about the world and the future and ruminating about negative events are linked to substance abuse tendencies.37, 38
Taken together, this study found a higher prevalence of all distal to proximal dysfunctional cognitions in ADG. This suggests that all the elements of cognitions such as EMS, which is the most fundamental and rigid cognitive structure, a dysfunctional attitude, which is the reflection of schemas, cognitive distortion, which continues to perpetuate schemas through its information processing mechanism, and negative automatic thought, which is the most superficial level of cognition, are all interconnected. Their interplay may contribute to AD.
The study has several limitations. First, the study sample comprised solely males seeking treatment for AD, limiting the generalizability of the findings across gender, nontreatment-seeking population, and individuals with other SUDs. Second, no objective assessment instrument was used to screen patients’ current medical condition, which could have influenced the assessment findings. Third, the study findings do not determine whether these dysfunctional cognitions are a cause or a consequence of AD. The higher severity of the dysfunctional cognition in individuals with AD could be because of their continued use of alcohol. Hence, a longitudinal study of cognition is needed to determine the explanation for the severity of the dysfunctional cognition in individuals with AD.
In conclusion, this study emphasizes the importance of considering the possibility that dysfunctional cognition may be present in higher severity among individuals with AD than in healthy individuals. A thorough and systematic evaluation of dysfunctional cognitions could help us identify them more systematically and efficiently and aid in formulating a better management plan for people with AD. Identifying and modifying maladaptive cognitions may lead to improved substance use treatment outcomes because of their coherence with personality structure and underlying influence on alcohol use.16, 17, 39 Addressing the underlying maladaptive cognitions in AD also may contribute to a reduced likelihood of relapse, as these fundamental beliefs influence how an individual responds to different situations. As a result, a therapeutic approach that targets these cognitions may facilitate acquiring a more balanced and adaptive appraisal of events in individuals with AD, and subsequently, improve coping skills to deal with situations that could otherwise trigger alcohol use. The study further stresses the need to address both problematic alcohol consumption and dysfunctional cognitions to improve substance use treatment outcomes. 16 Future research can explain the nature of traumatic childhood experiences that lead to the development of dysfunctional cognitions. Furthermore, future studies should not be limited to examining negative cognitions in relation to AD but can also include the examination of positive cognitions.
Footnotes
Acknowledgements
The authors thank all doctoral committee members and staff of the institute for their cooperation and support.
Data Availability Statement
The data supporting the findings of this study are easily available from the corresponding author, upon reasonable request. Data will be available in the Mendeley data repository from the date of publication of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was funded by the University Grant Commission, Government of India.