
Abstract
Background:
Binaural beats are used to reduce anxiety by presenting two sounds with steady intensities at different frequencies to each ear, resulting in a single tone midway between them, with an amplitude equal to the difference between them. We aimed to utilize this to reduce anxiety in alcohol withdrawal patients and assess its effectiveness.
Methods:
This study was done among 100 alcohol patients categorized as moderate and severe alcohol withdrawal by Clinical Institute Withdrawal Assessment of Alcohol Scale-Revised (CIWA-Ar) score. The anxiety levels for both groups were assessed using the Hamilton Anxiety Rating Scale (HAM-A). Binaural Beats were played in their ears via headphones for 10 minutes, and their anxiety levels were assessed again. The data were analyzed using an independent sample t-test and regression analysis.
Results:
Out of the 100 patients, 48 had moderate withdrawal, and 52 had severe withdrawal. Pre- and post-test HAM-A scores in moderate withdrawal showed no statistically significant difference (p = .17), whereas in severe withdrawal there was a significant reduction (p < .001). The patients with severe withdrawal had a reduction in anxiety with intervention when compared to moderate withdrawal. The rate of improvement in the severe and moderate withdrawal groups was 5.76% and 0.27%, respectively. Higher CIWA-Ar scores and pre-intervention HAM-A scores caused greater improvement in HAM-A post-intervention.
Conclusion:
Binaural beats technology could be a better add-on to conventional therapy to reduce anxiety, as evidenced by our patients’ responses.
Summary:
This is the initial research on applying binaural beats in reducing anxiety among alcohol withdrawal patients. It reveals the potential of binaural beats as a new, nonintrusive, and effective strategy in reducing alcohol withdrawal anxiety. It can be implemented in our routine setup to improve patients’ understanding of the illness, their drug compliance, and their cooperation with the initiation of therapy sessions like Motivational Enhancement Therapy and could help in minimizing the use and need for anxiolytic medications, thus making the treatment more cost-effective. Thus, it can be integrated as a part of psychiatric care, addiction treatment, and withdrawal management.
Effectiveness of binaural beats in reducing anxiety in alcohol withdrawal patients. The patients with withdrawal had a reduction in anxiety with intervention. Binaural beats technology could be an add-on to conventional therapy to reduce anxiety.Key Messages:
Alcohol use is quite common in India, both in rural and urban areas, with an estimated number of people using alcohol in India in 2005 was 62.5 million, with 17.4% of them (10.6 million) having alcohol use disorder. Of all hospital admissions in India, 20%–30% are due to alcohol-related problems. 1 The withdrawal state in alcohol use is a group of symptoms of variable severity occurring on absolute or relative withdrawal following repeated and prolonged consumption of alcohol. 2
Anxiety and alcohol use are associated in various ways: (a) anxiety can predispose to alcohol use, (b) alcohol dependence can cause anxiety symptoms, in excessive use or withdrawal, and (c) alcohol and anxiety share common etiological factors like personality disorders. 3 Also, anxiety is one of the predominant presentations of alcohol withdrawal states and has been the reason for lapsing into alcohol use.4,5 Hence, the management of anxiety plays a vital part in the management of withdrawal states and maintenance of long-term abstinence.
“Binaural beats” is a non-pharmacological way of reducing anxiety. It involves presenting two sounds with steady intensities, simultaneously administered at different frequencies to each ear. The resulting perception is of a single tone with a frequency midway between the two carrier tones and an amplitude equal to the difference between them. To achieve these results, both ears should participate in the process. This single tone is the binaural beat, which requires the two tones to be spaced between 26 Hz and 30 Hz. These beats are thought to originate subcortically in the medial nucleus of the superior olivary complex, the first nucleus in the auditory pathway to receive bilateral input. 6 The “illusory” third tone is lateralized between the left and the right ear, making the binaural beats useful for spatial sound research.
A few studies have been conducted to assess the efficiency of this technology in reducing anxiety associated with general anesthesia, 7 dental surgery, 8 urological surgeries, 9 and cataract surgeries. 10 They are also found to affect pain perception and cognition. 11 However, its efficacy in reducing anxiety in alcohol withdrawal states has not been explored in the past.
The present study was conducted to evaluate the effectiveness of binaural beats in reducing anxiety caused by alcohol withdrawal in chronic alcoholic patients and to analyze the effectiveness based on the severity of withdrawal.
Hypothesis
Binaural beats are effective in reducing anxiety levels among patients with alcohol withdrawal, with greater improvement observed in those with severe withdrawal compared to moderate withdrawal.
Aim
The study aims to assess the efficacy of binaural beats in improving the anxiety levels in patients with alcohol use disorder during the withdrawal stages.
Objectives
To identify the factors impacting the change in anxiety levels.
To assess the impact on various symptoms of anxiety.
Methods
This was a single-group pre-post interventional study designed to evaluate the immediate impact of binaural beats on anxiety levels in patients undergoing alcohol withdrawal. The study was commenced after obtaining Institutional Ethics Committee approval and conducted in the Department of Psychiatry at a tertiary care hospital from October to December 2023. All the patients who availed the outpatient and the in-patient care for mental and behavioral disorders due to use of alcohol—alcohol withdrawal state, as per International Classification of Diseases (ICD-10) 12 criteria were recruited for the study after considering the inclusion criteria: (a) those diagnosed with alcohol withdrawal syndrome; moderate and severe, (b) belonging to the age group of 18–70 years, (c) both male and female participants, and (d) those who consent to participate in the study. The exclusion criteria include: (a) those diagnosed with complicated alcohol withdrawal syndrome, (b) mild alcohol withdrawal syndrome, (c) participants with other substance use amounting to dependence pattern, (d) pre-existing anxiety disorder or other psychiatric comorbidities, (e) medical illness causing anxiety symptoms, and (f) participants with hearing deficits.
The alcohol withdrawal was assessed using the Clinical Institute Withdrawal Assessment of Alcohol Scale-Revised (CIWA-Ar). 13 Those patients with mild withdrawal were excluded, as there were minimal or no anxiety symptoms reported. Those patients with moderate and severe withdrawal were included, and the anxiety was measured with the Hamilton Anxiety Rating Scale (HAM-A). 14
Study Sample
Simple random sampling was done. The sample size was calculated using OpenEpi software, Version 3.3, 15 based on the 9.7% prevalence of alcohol use in Puducherry in a study conducted by Vijay Ramanan et al., 16 with 95% confidence interval (CI) and 5% absolute precision sample size was calculated to be 100.
Tools
Hamilton Anxiety Rating Scale (HAM-A) 14
The HAM-A is the standard scale for measuring the severity of anxiety symptoms. It contains 14 items and is clinician-rated. Each item is scored on a scale of 0 to 4, with a total score range of 0–56, where <17 indicates mild severity, 18–24 mild to moderate severity, 25–30 moderate to severe, and 31–56 severe to very severe.
Clinical Institute Withdrawal Assessment of Alcohol Scale-Revised (CIWA-Ar) 13
The CIWA-Ar is an instrument used to assess and diagnose the severity of alcohol withdrawal. It contains 10 items and is clinician-rated. The first 9 items are scored on a scale of 0 to 7. The 10th item is scored on a scale of 0 to 4, with a total score range of 0–67, where <10 indicate mild withdrawal, 10–15 indicate moderate withdrawal, and scores of 15 or more indicate severe withdrawal with impending possible delirium tremens.
Instruments
A stereo headphone and an audio device (mobile phone) to play Binaural beats. Binaural beats—theta waves were used (95 Hz on the right ear and 100 Hz on the left ear) which were of pure frequency Binaural beats without background music or relaxing sounds such as waves or raindrops, the frequencies were produced by software—Brain Waves Binaural beats, MynioTech Apps, Chapecó, Santa Catarina, Brazil, which is freely available in the playstore (
Operational Procedure
Patients were screened based on inclusion and exclusion criteria, and alcohol withdrawal state was diagnosed using ICD-10 criteria. The CIWA-Ar scale was then used to assess participants’ withdrawal levels, and they were categorized into two groups: Group 1 for moderate withdrawal and Group 2 for severe withdrawal. At baseline (t = 0), the HAM-A was used to measure anxiety levels in both groups to assess short-term change before initiating pharmacological interventions to avoid confounding. Participants were exposed to binaural beats for 10 minutes. Noise-canceling headphones were used, and the procedure was conducted in a closed, isolated room to minimize disturbance. The same room was used for all the participants. Eye closure was encouraged but was not mandatory. The participants were told to sit comfortably and move as little as possible. The intervention was conducted in the evening before any meal or beverage. To evaluate the impact of the intervention, the participants’ anxiety was then reassessed on the HAM-A (t = 10) immediately following the intervention. Those patients experiencing higher levels of anxiety and withdrawal symptoms were treated with pharmacotherapy and psychotherapies based on the clinical presentation after the intervention.
Statistical Analysis
The data were entered into Microsoft Excel and analyzed using the software IBM Statistical Package for Social Sciences (IBM SPSS), Version 24. 18 Descriptive analysis, Paired t-test, independent t-test, Pearson correlation, and Multiple linear regression were used.
Results
Descriptive Data
A total of 100 patients who presented to the Psychiatry Outpatient Department with an uncomplicated alcohol withdrawal state participated in this study. The mean age of the participants was 42.36 (SD = 11.27). The majority of participants were in the 31–40-year age group (30%), followed by the 41–50-year age group (29%). The study population consisted only of male participants. About 65% of the participants were educated (Table 1).
Frequency Distribution of the Study Population.

Measurement of the Severity of Alcohol Use
The average duration of alcohol consumption was 18.17 years (SD = 8.07), and over 77% of participants had a history of alcohol use for more than 10 years. The mean CIWA-Ar score for the population was 17.78 (+7.36). Among 100 participants, 52 participants presented with severe withdrawal, and 48 participants presented with moderate withdrawal, based on the CIWA-Ar score (Table 2).
Overall Descriptive Data of the Study Population.

CIWA-Ar = Clinical Institute Withdrawal Assessment of Alcohol Scale-Revised; HAM-A = Hamilton Anxiety Rating Scale.
Measurement of Anxiety
The mean HAM-A score before and after the intervention was 18.90 and 18.20, respectively. The mean change in HAM-A score after intervention was 0.70. The pre- and post-intervention HAM-A scores for patients with moderate withdrawal were 14.75 ± 1.86 and 14.71 ± 1.91, respectively, and the mean change in HAM-A score was 0.04 ± 0.20, which was not statistically significant (t = 1.38, p = .17). Among patients with severe withdrawal, the pre- and post-intervention scores were 22.73 ± 7.52 and 21.42 ± 6.46, respectively, and the mean change in HAM-A score was 1.31 ± 1.32, which was statistically significant (t = 7.16, p < .001). The patients with severe withdrawal had a reduction in anxiety with intervention when compared to the patients with moderate withdrawal. The rate of improvement in the severe withdrawal group was 5.76%, and that of the moderate withdrawal group was 0.27%, indicating a markedly greater anxiolytic response in the severe withdrawal group. In the moderate withdrawal group, the pre-post change in HAM-A scores showed a small effect size (Cohen’s d = 0.20; 95% CI = −0.09 to 0.49), indicating a negligible clinical effect. In contrast, the severe withdrawal group demonstrated a large effect size (Cohen’s d = 0.99; 95% CI = 0.66–1.32), reflecting a substantial and clinically meaningful reduction in anxiety following the intervention (Tables 2 and 3).
Comparison of the Change in HAM-A Between Moderate and Severe Withdrawal.
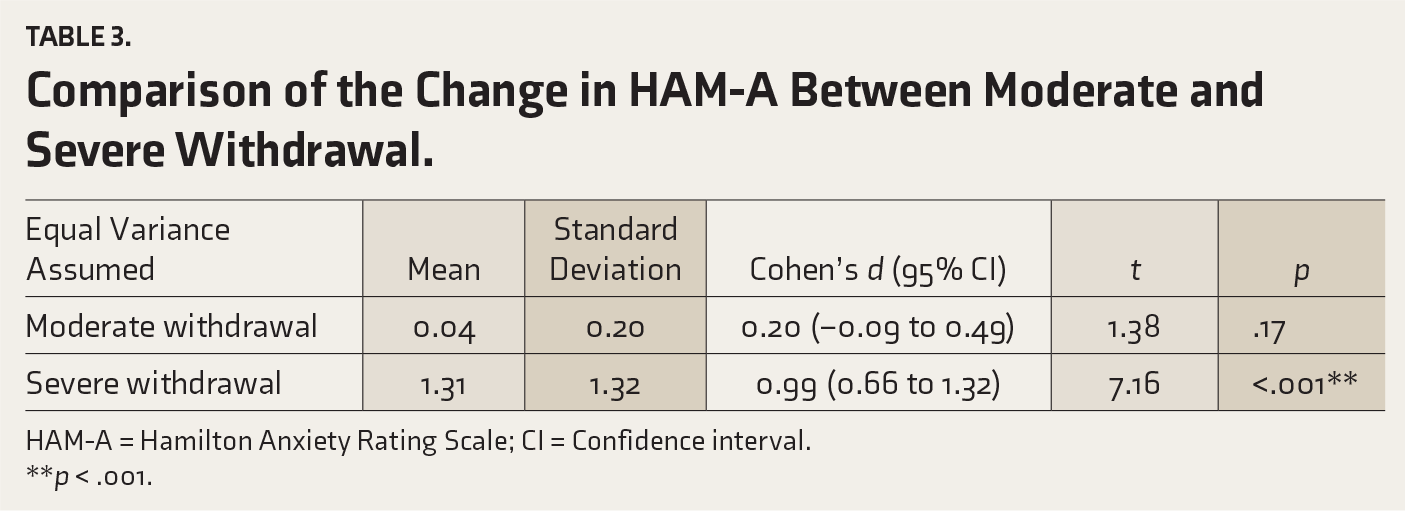
HAM-A = Hamilton Anxiety Rating Scale; CI = Confidence interval.
**p < .001.
Association of Independent Variables with Change in HAM-A After Intervention
The total HAM-A score before the intervention had a strong statistically significant association with the change in HAM-A scores after the intervention. The strongest association was with anxiety (r = 0.82, p < .001), followed by agitation (r = 0.79, p < .001) and nausea and vomiting (r = 0.71, p < .001) (Table 4).
Item-wise Association of CIWA-Ar with Change in HAM-A.
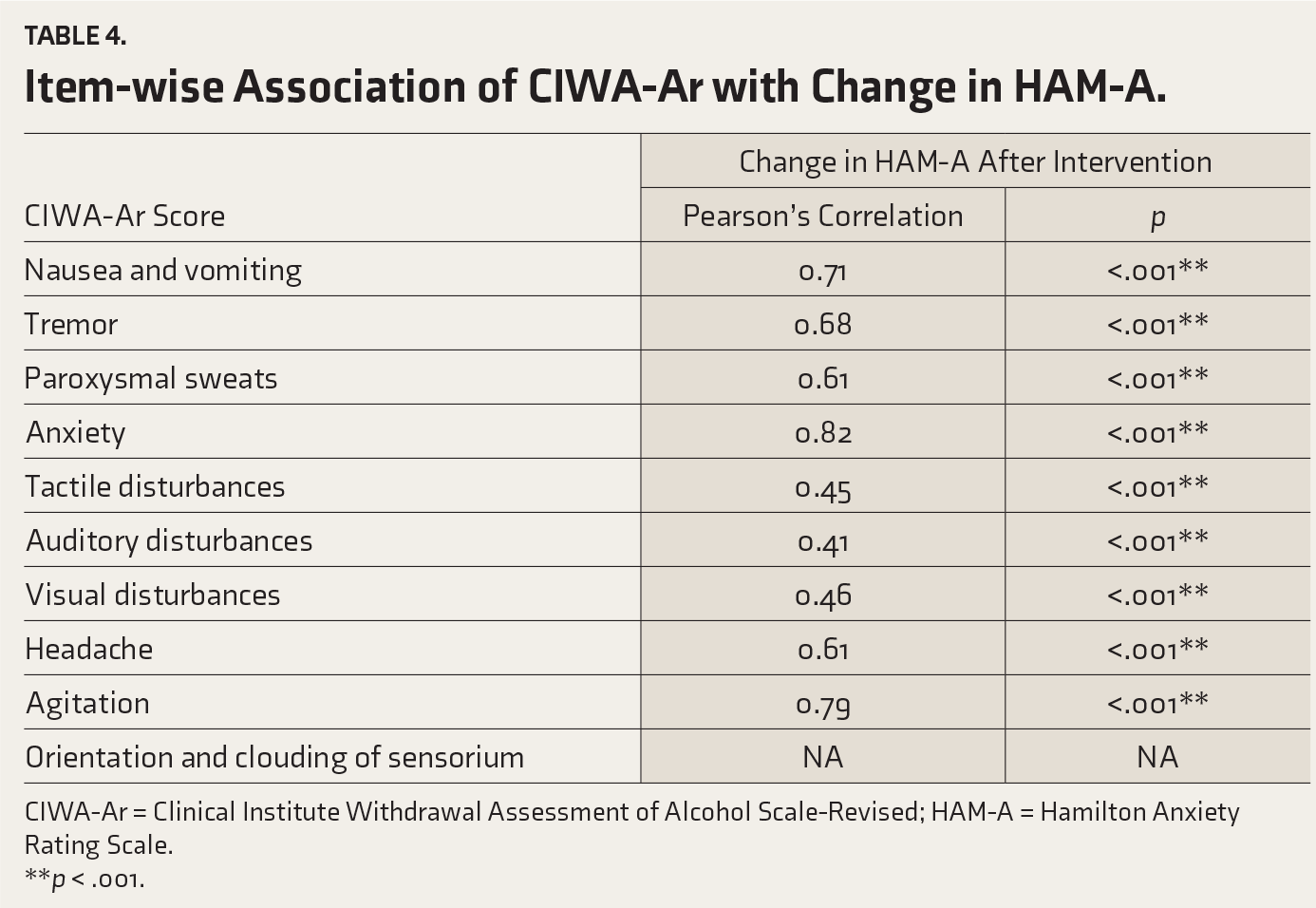
CIWA-Ar = Clinical Institute Withdrawal Assessment of Alcohol Scale-Revised; HAM-A = Hamilton Anxiety Rating Scale.
**p < .001.
The post-intervention changes in HAM-A score were strongly associated with the CIWA-Ar score. Item-wise analysis showed that individual item scores had a strong association with the change in HAM-A after the intervention, with the strongest association with anxious mood (r = 0.80, P < .001), followed by tension (r = -0.77, P < .001) and behavior at interview (r = 0.74, P < .001).
Discussion
Binaural beats are produced when two tons of slightly differing frequencies are played into each ear individually, so that the brain perceives a rhythmic beat equal to the difference in frequency. In contrast to acoustic beats, which are produced by physical interference, binaural beats are generated within the brain, likely due to neural convergence in the auditory pathways. Binaural beats are most apparent at low frequencies. The dominant explanation is that neurons retain phase information and send it to binaurally responsive brainstem neurons that produce the percept of binaural beats. 19
Binaural beats technology is marketed and popularized as a personal development and health improvement tool. Regular listening to binaural beats is claimed to have benefits such as reducing stress and anxiety, increasing focus, concentration, motivation, and confidence, and deepening meditation. It also helps with cognitive enhancement and reducing pain perception. 11
Alcohol withdrawal typically starts 1–3 days following the last use and may persist for as long as 1 week. Symptoms arise when the central nervous system, initially exposed to chronic alcohol consumption, suddenly transitions to a state of reduced alcohol consumption. Numerous mechanisms mediate alcohol withdrawal syndrome, and the brain achieves neurochemical equilibrium through various inhibitory and excitatory neurotransmitters. The primary inhibitory neurotransmitter is γ-amino-butyric acid (GABA), which exerts its action via the GABA-alpha (GABA-A) neuroreceptor. One of the principal excitatory neurotransmitters is glutamate, which exerts its action via the N-methyl-D-aspartate (NMDA) neuroreceptor. Alcohol potentiates the action of GABA on GABA-A neuroreceptors, leading to reduced overall brain excitability. Chronic alcohol exposure leads to a compensatory reduction of GABA-A neuroreceptor response to GABA, as reflected by growing tolerance to the actions of alcohol. Alcohol blocks NMDA neuroreceptors, and chronic alcohol exposure leads to upregulation of these receptors. Sudden withdrawal of alcohol exposure leads to brain hyperexcitability, since receptors that the chronic alcohol usage had blocked are now no longer blocked. Brain hyperexcitability is expressed clinically as anxiety, irritability, agitation, and tremors. Severe manifestations of alcohol withdrawal include seizures and delirium tremens. 20 The severity of anxiety tends to increase with the severity of withdrawal, making it difficult to establish rapport and deliver effective psychotherapy. As the vital element in psychiatry is communication, it creates good opportunities for methods to decrease anxiety, like binaural beats, without pharmacotherapy.
In this context, we conducted a pre- and post-single-arm experimental study in a medical college in South India among 100 alcohol withdrawal patients with anxiety who were given a single session of 10 minutes of exposure to binaural beats. The patients with severe withdrawal had a reduction in anxiety levels when compared to the patients with moderate withdrawal. Despite the confounding factors, the mean difference in the severe withdrawal group was statistically significant. There is also a significant association between the severity of withdrawal symptoms and the degree of change in HAM-A score, with a maximum effect in anxious mood, followed by tension, and behavior at interview. It is also observed that a higher CIWA-Ar score and pre-intervention HAM-A score will cause greater improvement in HAM-A post-intervention. Patients with severe withdrawal had higher baseline anxiety levels, allowing greater potential for measurable improvement. In contrast, the increased physiological and autonomic arousal associated with severe withdrawal may have enhanced responsiveness to calming interventions such as binaural beats.
A study was conducted to assess the psychological and physiological effects of binaural beats technology after a 60-day intervention in eight healthy individuals. The results showed decreases in trait anxiety, increases in quality of life, and decreases in insulin-like growth factor-1 and dopamine between pre- and post-intervention measurements. 21 This finding was in line with our study.
A study done to determine whether mildly anxious people would report decreased anxiety after listening to tapes embedded with tones that create binaural beats daily for 1 month showed that listening for approximately 30 minutes per session resulted in a reduction in the anxiety score of the patients with mild anxiety. 22 There was a major variation in the methods of binaural tone delivery in our study. However, a significant anxiety reduction was observed with minimal exposure of 10 minutes.
Another study done to explore the effectiveness of binaural beats at reducing anxiety associated with cadaveric dissection in anatomy students proved to be effective in reducing and maintaining students’ state anxiety levels in comparison to a control group. 23 Further research has been conducted on preoperative patients before undergoing general anesthesia for a day procedure by dividing them into three groups: the binaural group, the audio group with an identical soundtrack but without adding any tones, and a no-intervention group. It reported a significant decrease in preoperative anxiety in the binaural group. 7 Binaural beats were also used to try to reduce preoperative dental anxiety, and they were compared with a music group and a control group. It showed a comparable decrease in anxiety among both the binaural and music groups, whereas there was no significant improvement in the control group. 24 These studies have consistent results with our study; however, they have a comparison group, unlike our study.
Strengths
It is a low-cost, accessible, and effective tool. The minimal intervention period proved effective. No reported side effects immediately after the intervention. Various age groups were taken into the study.
Limitations
The sample size was small, consisting only of male participants. Only one binaural beat frequency was tested; the effectiveness of different frequencies remains unknown. This study evaluated only the immediate short-term effects of binaural beats on anxiety and did not examine long-term outcomes. The absence of a control group limits causal conclusions. Therefore, findings should be considered preliminary. More comprehensive research, including comparison with a control group, is necessary to assess its effectiveness, long-term impacts, influence of confounding factors, and other clinical uses. The effect size, indicated by Cohen’s d, was moderate; this might be partly due to low variability in change scores rather than the actual clinical improvement. The study did not determine the minimal clinically important difference or patient-reported relief, which restricts conclusions about clinical significance.
Implications
Post-intervention anxiety reduction in alcohol withdrawal patients can be implemented in our routine setup to improve patients’ understanding of the illness, their drug compliance, and their cooperation with the initiation of therapy sessions like Motivational Enhancement Therapy. The use of binaural beats could help minimize the need for anxiolytic medications, making the treatment more cost-effective. Thus, it can be integrated as a part of psychiatric care, addiction treatment, and withdrawal management.
Conclusion
This is the initial research on applying binaural beats in reducing anxiety among alcohol withdrawal patients. It provides preliminary evidence that a brief session of binaural beats may be associated with a modest reduction in anxiety levels among patients with severe alcohol withdrawal. Although the observed change in anxiety levels was small in absolute terms, the statistically significant reduction suggests a potential short-term anxiolytic effect, particularly in patients with higher baseline withdrawal severity and anxiety. This research opens the door to exploring binaural beats. Future studies should aim to reproduce these results with more heterogeneous, larger populations, with comparison groups over long periods, and to assess their efficacy in other psychiatric conditions.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Clinical Trial Registration
This study was registered with the Clinical Trials Registry, India (CTRI/2024/05/067976).
Data Availability Statement
Deidentified individual participant data will not be made available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethical Approval
Ethical approval for this study was obtained from the Institutional Ethics Committee, Sri Manakula Vinayagar Medical College and Hospital (Approval No.: SMVMCH-EC/ECO/IL/269/2023; Date: 6 October 2023).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent has been obtained from the patients and the caregivers for participation in the study.
Prior Presentations
No.
Reporting Guideline (Supplementary Online Material)
The study followed the Template for Intervention Description and Replication (TIDieR) checklist. The checklist is provided as supplementary material. Hoffmann T, Glasziou P, Boutron I, et al. Better reporting of interventions: Template for Intervention Description and Replication (TIDieR) checklist and guide. BMJ 2014; 348: g1687. doi: 10.1136/bmj.g1687
Simultaneous Submission to Another Journal or Resource
No.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.