
Abstract
Background:
Borderline Personality Disorder (BPD) features impulsivity, emotional dysregulation, and self-injurious behaviors (SIB). Cognitive deficits, such as executive dysfunction (ED) and working memory (WM) impairments, may drive these symptoms, yet their roles remain underexplored. This study examined relationships among ED, WM, impulsivity, and SIB in BPD to identify cognitive predictors of these behaviors.
Methods:
This cross-sectional study assessed 30 individuals with BPD per DSM-5 criteria. Participants completed the Barratt Impulsiveness Scale (BIS-11) for impulsivity, Deliberate Self-Harm Inventory (DSHI) for SIB, Wisconsin Card Sorting Test (WCST) for ED, and Letter-Number Sequencing (LNS) task for WM. Spearman’s correlations and regression analyses evaluated associations between cognitive deficits, impulsivity, and SIB.
Results:
Elevated impulsivity was linked to more WCST perseverative errors (ρ = 0.45, p = .02) and lower LNS scores (ρ = −0.38, p = .04). SIB correlated with ED (ρ = 0.41, p = .03) but not WM (ρ = −0.20, p > .05). High-impulsivity participants had greater WCST errors (median = 20 vs. 11, H = 8.12, p < .05) and lower LNS scores (median = 6 vs. 10, H = 7.33, p < .05) than low-impulsivity peers. Regression confirmed BIS-11 scores predicted WCST errors (β = 0.40, p < .01) and LNS performance (β = −0.35, p < .05).
Conclusions:
The ED and WM impairments were linked to impulsivity, with ED also tied to SIB. Cognitive remediation may reduce these behaviors. Lacking a control group, longitudinal research is needed.
Keywords
This study examined executive dysfunction and working memory in borderline personality disorder patients. Impulsivity was correlated with cognitive deficits; self-injurious behaviors linked to emotional factors. Cognitive interventions could reduce impulsivity in borderline personality disorder and addiction.Key Messages:
Borderline personality disorder (BPD) is a severe psychiatric condition marked by emotional dysregulation, impulsivity, unstable relationships, and recurrent self-injurious behavior (SIB). 1 While affective symptoms are well-documented, emerging evidence highlights neurocognitive deficits— particularly in executive function (EF) and working memory (WM)—as key contributors to symptom severity. 2 These impairments disrupt impulse control and coping, increasing vulnerability to self-harm. 3 Executive dysfunction (ED) in BPD involves poor cognitive flexibility and inhibitory control, often leading to impulsive acts like substance misuse or self-injury. 4 Similarly, WM deficits hinder the ability to manage task-relevant information, worsening emotional dysregulation. 5 Neuroimaging links these issues to dysregulated frontal-limbic circuits, including the dorsolateral prefrontal cortex (DLPFC), with reduced DLPFC activity tied to impaired inhibition.6, 7
Although impulsivity and SIB are recognized in BPD, 8 their neurocognitive underpinnings are underexplored, with most research predominantly emphasizing emotional dysregulation. 2 There remains a significant gap in systematically examining how specific EF and WM deficits directly drive these behaviors, particularly in contrast to, or in conjunction with, emotional factors. This study addresses this gap by systematically examining these cognitive domains, offering a novel focus on their role in BPD’s behavioral outcomes, paralleling mechanisms observed in substance use disorders. 9 Clarifying these links is vital for enhancing diagnostic precision and tailoring interventions like cognitive remediation. 10 We hypothesized that EF and WM impairments correlate with greater impulsivity and SIB. The aim was to explore these relationships in BPD patients. The specific objectives were: (a) to assess correlations between EF and WM with impulsivity and SIB, and (b) to identify whether EF and WM impairments predict the severity of impulsivity and SIB in individuals with BPD. These findings could guide clinical assessments and neurobiologically informed treatments. 11
Methods
The Institutional Ethics Committee approved this cross-sectional study. Written informed consent was obtained from all participants. The study examined relationships between ED, WM deficits, impulsivity, and SIB in individuals with BPD. 12 Data were collected from June to December 2023 at a tertiary care hospital’s psychiatry unit.
Participants and Recruitment
Thirty participants meeting DSM-5 criteria for BPD were recruited from outpatient and inpatient settings. 13 While efforts were made to reduce selection bias by approaching consecutive patients, the specific gender distribution (60% male, 40% female) and the mix of outpatient and inpatient participants should be considered when interpreting generalizability. The sample size was determined via a priori power analysis using G*Power software (version 3.1). 14 Assuming a medium effect size (ρ = 0.5) for Spearman’s correlations between cognitive deficits and impulsivity, a power of 0.80, and an alpha of 0.05 (two-tailed), a minimum of 29 participants was required. Of 38 individuals screened, 33 were eligible; 5 were excluded (three for severe substance use disorders, two for neurological conditions), and three declined due to time constraints, yielding 30 participants (78.9% participation rate). 15 The recruitment flow is summarized as follows: Screened: n = 38; Eligible: n = 33 (excluded: n = 5; 3 substance use, 2 neurological); Consented: n = 30 (declined: n = 3; time constraints); Analyzed: n = 30. Inclusion criteria included ages 18–45 years, confirmed BPD diagnosis, at least one SIB episode, basic literacy, and consent willingness. Exclusion criteria comprised major neurocognitive or neurological disorders, severe substance use disorders (except nicotine/caffeine), and sedative use impairing cognition. 16 To minimize selection bias, consecutive patients meeting DSM-5 criteria were approached, reducing cherry-picking. 13
Measures
Participants completed validated instruments to assess BPD symptoms, impulsivity, SIB, and cognitive function, administered in a controlled clinical setting. 17 While robust exclusion criteria were applied to minimize confounding factors, potential influences of untreated or subclinical comorbidities (e.g., depression, anxiety) or the impact of ongoing psychotropic medication status on cognitive performance were not explicitly controlled for as separate variables in the analysis. This should be considered in the interpretation of results and is a point for future research. The Borderline Symptom List (BSL-23) is a 23-item self-report scale measuring BPD symptom severity, including emotional instability and behavioral dysregulation, with high reliability (Cronbach’s α = 0.94) and validity in psychiatric populations. 18 The Barratt Impulsiveness Scale (BIS-11) is a 30-item questionnaire assessing motor, attentional, and non-planning impulsivity, widely used in BPD research, with strong internal consistency (Cronbach’s α = 0.83). 19 The Deliberate Self-Harm Inventory (DSHI) is a 17-item measure capturing SIB frequency, type, and severity, demonstrating good reliability (Cronbach’s α = 0.89) and sensitivity to self-harm behaviors. 20 Neurocognitive assessments included the Wisconsin Card Sorting Test (WCST), a standardized task evaluating ED through perseverative errors and categories completed, validated for assessing cognitive flexibility in BPD (test-retest reliability ≈ 0.80). 21 The Letter-Number Sequencing (LNS) task, from the Wechsler Adult Intelligence Scale (WAIS-IV), measures WM by requiring participants to reorder mixed sequences, with high reliability (Cronbach’s α ≈ 0.85) in clinical settings. 22 All tools were administered per standardized protocols, with no missing data for primary variables (WCST perseverative errors, LNS scores, BIS-11 totals, DSHI totals).
Procedure
Assessments lasted approximately 60 minutes per participant in a distraction-free environment to mitigate performance bias, though assessors were not blinded to BPD diagnosis due to the clinical context. 17 This study received no specific funding from public, commercial, or not-for-profit sectors, and was conducted as part of routine clinical research activities at the hospital.
Data adhered to STROBE guidelines, uploaded as supplementary online material. 23
Statistical Analysis
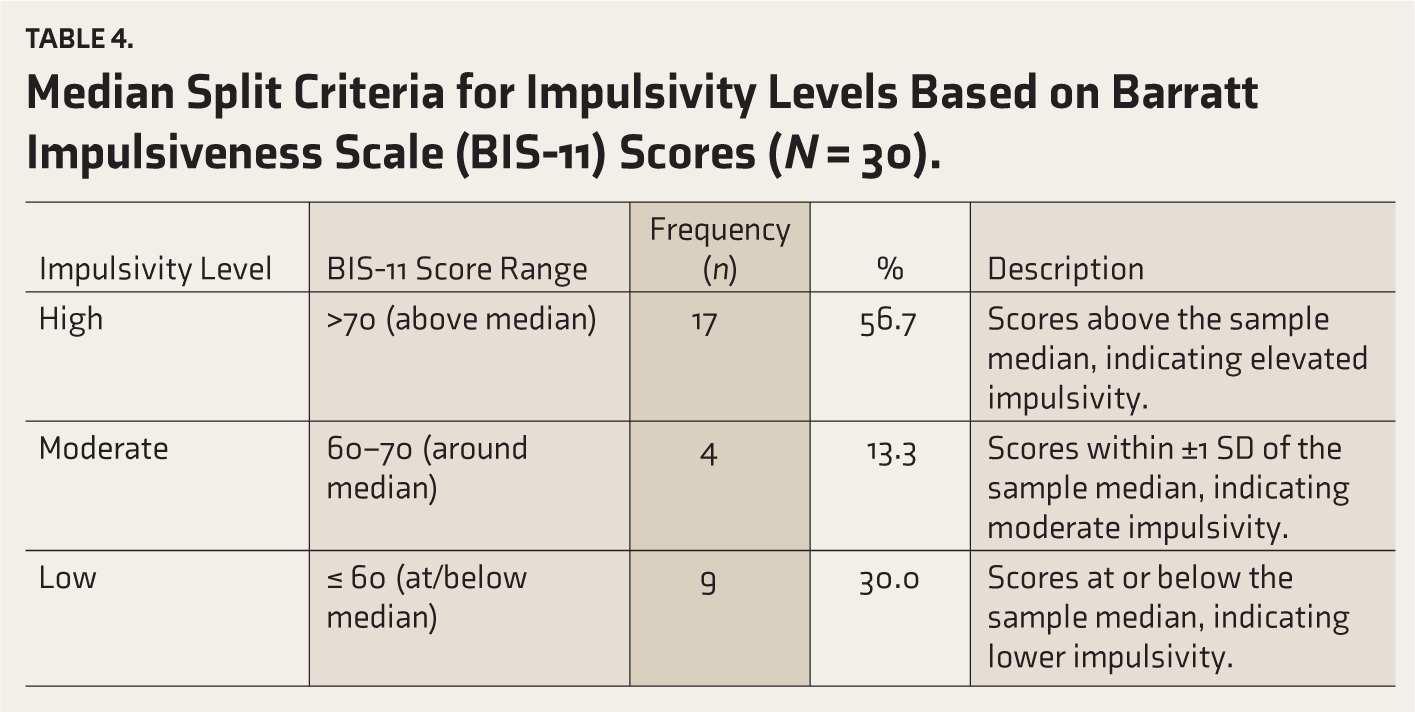
Descriptive statistics summarized demographics and clinical variables. Independent t-tests compared neurocognitive performance by recent SIB status, and ANOVA assessed impulsivity across ED levels. Spearman’s correlations explored relationships between WCST errors, LNS scores, BIS-11, and DSHI scores. Impulsivity levels were categorized using a median split of BIS-11 total scores (median = 65) into high (>70), moderate (60–70), and low (≤60) groups to explore distinct cognitive profiles, complementing continuous regression analyses (see Table 4, Supplementary Material).
Multiple linear regression identified SIB predictors. Analyses used SPSS Statistics 30.0.0 (IBM Corp, 2023) 2 4 with significance at p < .05.
Results
Socio-demographic characteristics of the 30 participants are presented in Table 1. For descriptive purposes, participants were categorized by age, with the largest group aged 26–35 years (n = 11), followed by ≤25 years (n = 10) and ≥36 years (n = 9). Males comprised 60% (n = 18) and females 40% (n = 12). Education levels were distributed with 26.7% each having undergraduate (n = 8), postgraduate (n = 8), or high school (n = 8) qualifications, and 20% holding graduate degrees (n = 6). Over half of the participants were married (56.7%, n = 17).
Sociodemographic Characteristics of Participants with Borderline Personality Disorder (N = 30).
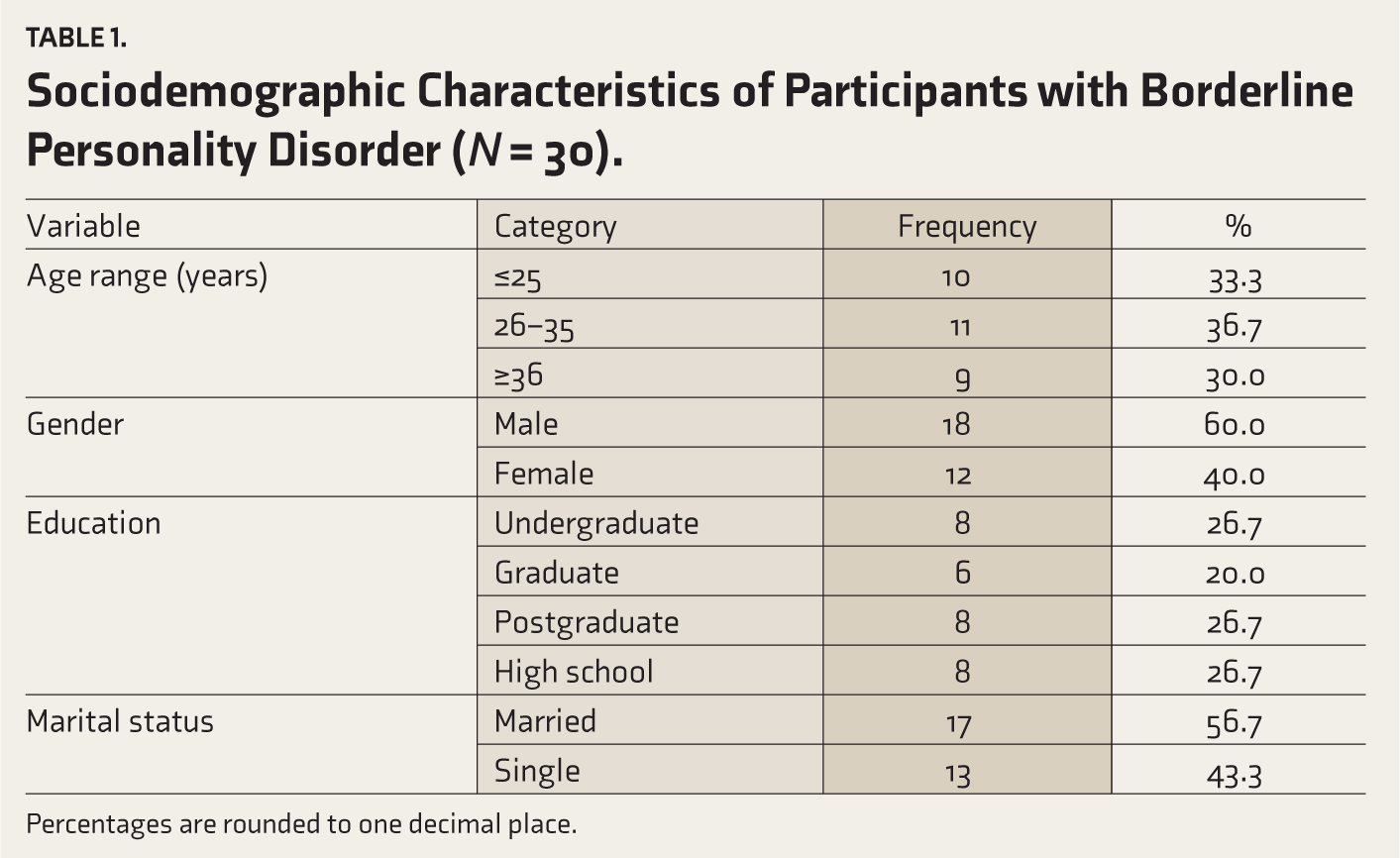
Percentages are rounded to one decimal place.
Spearman’s correlation analysis (Table 2) showed a significant positive association between WCST perseverative errors and BIS-11 total scores (ρ = 0.45, p = .02). This indicates that greater ED, as measured by more perseverative errors, was significantly associated with higher impulsivity. LNS scores negatively correlated with BIS-11 totals (ρ = −0.38, p = .04), suggesting that poorer WM performance was associated with increased impulsivity. No significant correlations were found between WCST perseverative errors (ρ = 0.25, p = .14) or LNS scores (ρ = −0.20, p = .29) and DSHI total scores.
Spearman’s Correlation Analysis of Cognitive Measures, Impulsivity, and Self-injurious Behavior in Borderline Personality Disorder (N = 30).
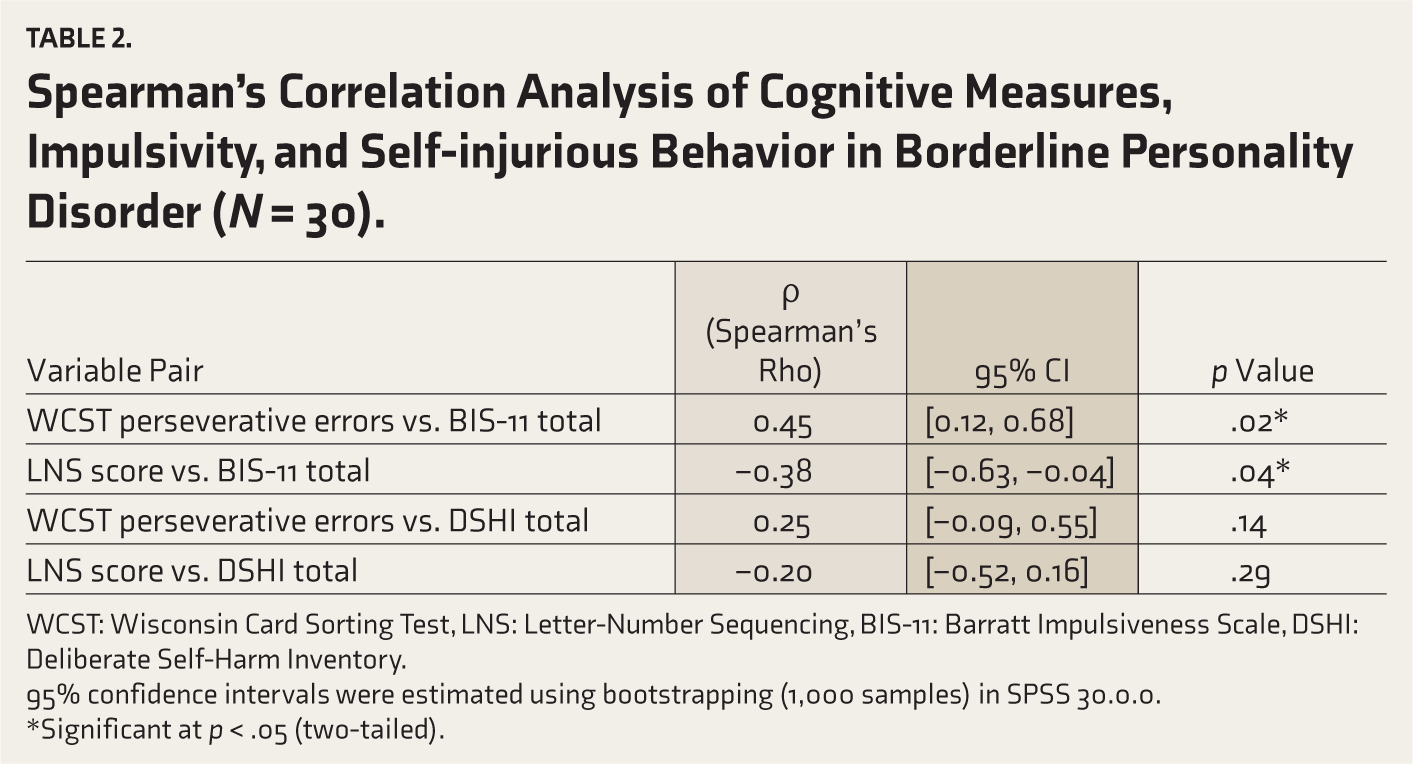
WCST: Wisconsin Card Sorting Test, LNS: Letter-Number Sequencing, BIS-11: Barratt Impulsiveness Scale, DSHI: Deliberate Self-Harm Inventory.
95% confidence intervals were estimated using bootstrapping (1,000 samples) in SPSS 30.0.0.
*Significant at p < .05 (two-tailed).
Further analysis using Kruskal–Wallis tests (Table 3) revealed significant differences in cognitive performance when impulsivity levels grouped participants. The Kruskal–Wallis H test is a non-parametric method used to compare two or more independent samples of equal or different sample sizes. Participants identified as ‘high-impulsivity’ (n = 17, defined by BIS-11 scores above the median) exhibited significantly more WCST perseverative errors (median = 20) compared to ‘low-impulsivity’ peers (n = 9, defined by BIS-11 scores at or below the median) (H = 8.12, p = .02). This suggests that individuals with higher levels of self-reported impulsivity demonstrate a clinically meaningful reduction in cognitive flexibility and problem-solving abilities. Impulsivity levels were defined by a median split of BIS-11 total scores (median = 65), with high (n = 17, >70), moderate (n = 4, 60–70), and low (n = 9, ≤60) groups, as detailed in Table 4 (Supplementary Material).
Group Comparisons of Cognitive Performance Across Impulsivity Levels in Borderline Personality Disorder (Kruskal–Wallis Test).

WCST: Wisconsin Card Sorting Test, LNS: Letter-Number Sequencing, H: Kruskal–Walli’s test statistic. Impulsivity levels were defined by a median split of Barratt Impulsiveness Scale (BIS-11) total scores (median = 65): High (>70, n = 17), Moderate (60–70, n = 4), Low (≤60, n = 9). Categorization complemented regression analyses by identifying distinct cognitive profiles associated with varying impulsivity levels. The Kruskal–Wallis H test compared medians across groups; Dunn’s post-hoc tests identified specific group differences.
*Significant at p < .05.
Median Split Criteria for Impulsivity Levels Based on Barratt Impulsiveness Scale (BIS-11) Scores (N = 30).
High-impulsivity participants also completed fewer WCST categories (median = 2) compared to low-impulsivity peers (median = 5) (H = 6.75, p = .03). Similarly, LNS scores were significantly lower in the high-impulsivity group (median = 6) than in the low-impulsivity group (median = 10) (H = 7.33, p = .03), with post-hoc Dunn’s tests confirming these significant differences (p < .05). Dunn’s post-hoc test is used after a significant Kruskal–Wallis result to identify which specific group pairs differ significantly. These findings indicate that higher impulsivity is associated with poorer WM capacity, which can manifest as difficulties in daily tasks requiring mental manipulation and attention. Demographic comparisons (Table 5) showed no significant differences across impulsivity levels for gender (χ2 = 1.23, p = .27), age (H = 2.45, p = .29), education (χ2 = 5.67, p = .13), or occupation (χ2 = 4.89, p = .18).
Demographic Comparisons Across Impulsivity Levels in Borderline Personality Disorder.
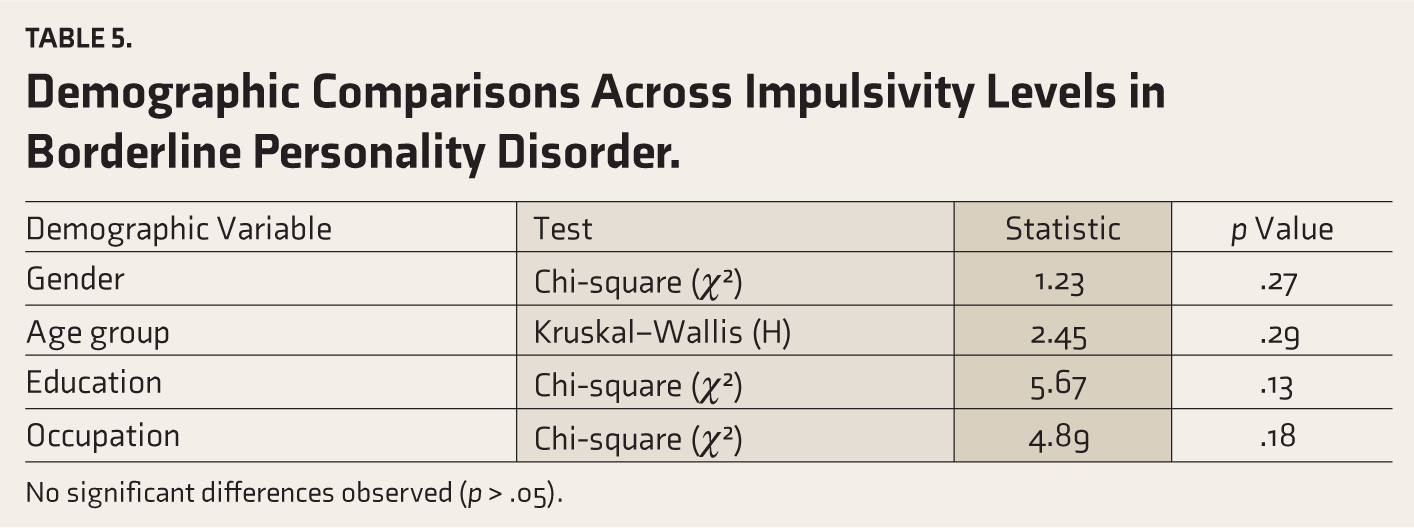
No significant differences observed (p > .05).
Multiple linear regression analyses were conducted to examine whether ED and WM predict impulsivity and SIB (Table 6).
Multiple Linear Regression Analysis Predicting Cognitive Performance in Borderline Personality Disorder (N = 30).
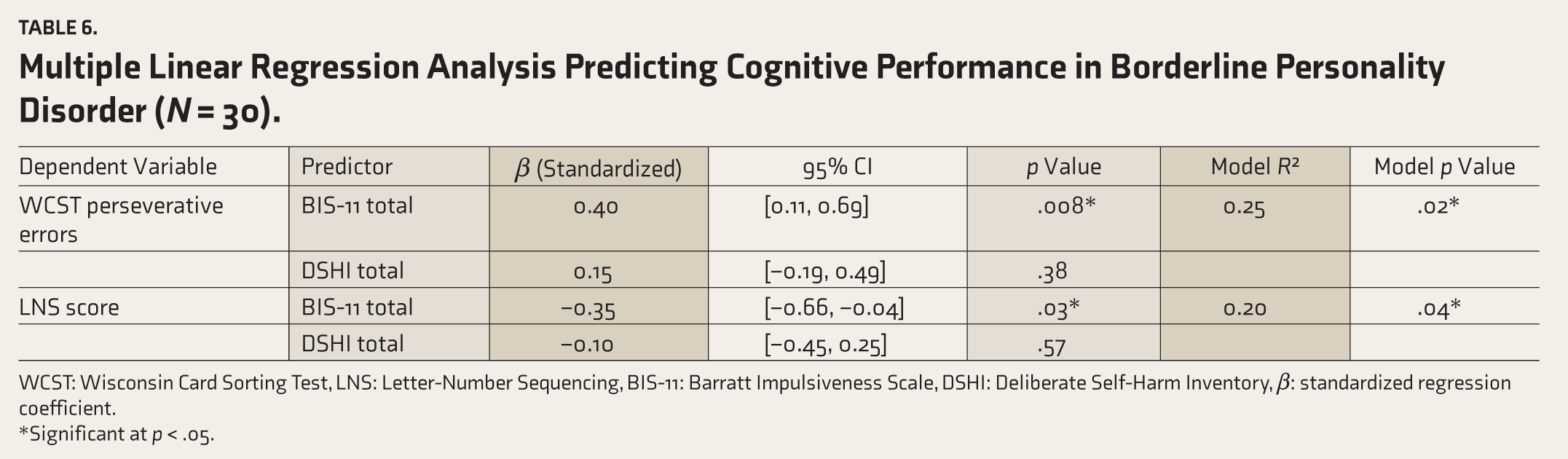
WCST: Wisconsin Card Sorting Test, LNS: Letter-Number Sequencing, BIS-11: Barratt Impulsiveness Scale, DSHI: Deliberate Self-Harm Inventory, β: standardized regression coefficient.
*Significant at p < .05.
In the first model, predicting BIS-11 total scores (impulsivity), the WCST perseverative errors (β = 0.40, p = .008) significantly predicted higher impulsivity, accounting for 25% of the variance (R2 = 0.25). The LNS scores (β = –0.35, p = .03) significantly predicted higher impulsivity, indicating that lower WM performance was associated with increased impulsivity.
In the second model, predicting DSHI total scores SIB, neither WCST perseverative errors nor LNS scores were significant predictors of DSHI total scores (p > .05).
Discussion
The BPD is a complex condition characterized by emotional instability, impulsivity, and SIB. 1 While affective dysregulation is a hallmark, this study underscores the pivotal role of ED and WM impairments in driving impulsivity and maladaptive behaviors, traits paralleling those in substance use disorders and behavioral addictions. 9 By integrating neurocognitive assessments—WCST and LNS—with validated measures like the BIS-11 and DSHI, our results affirm ED and WM deficits as central to BPD’s cognitive profile. 2 These findings are contextualized below within existing literature, followed by clinical implications and future research directions.
ED, Impulsivity, and Neurobiological Mechanisms
The significant correlation between BIS-11 impulsivity and WCST perseverative errors (ρ = 0.45, p = .02) highlights cognitive inflexibility’s role in impulsive decision-making, a mechanism also implicated in addiction, where prefrontal deficits drive compulsive behaviors. 6 This finding is consistent with previous research demonstrating impaired response inhibition and cognitive flexibility in BPD populations. Our study builds upon this by showing a direct predictive relationship where greater ED is associated with higher impulsivity. This aligns with neuroimaging evidence of dorsolateral prefrontal cortex (DLPFC) dysfunction in BPD, where reduced DLPFC activation during inhibitory tasks correlates with perseverative errors. 7 Similarly, DLPFC hypoactivity has been linked to impaired error monitoring, potentially explaining repetitive maladaptive behaviors in our high-impulsivity subgroup. 2
WM and Impulsivity
The negative correlation between LNS scores and BIS-11 totals (ρ = −0.38, p = .04) supports the frontoparietal network hypothesis, where WM relies on DLPFC and posterior parietal coordination. 8 Disruptions here, observed in emotionally charged tasks, 3 may impair task-relevant information retention under stress, precipitating impulsivity akin to patterns in addiction. 9 Our finding that poorer WM significantly predicts higher impulsivity further corroborates studies showing WM deficits in BPD and extends this by demonstrating its predictive utility for a core behavioral symptom. 7
SIB: Cognitive Versus ED
Although SIB correlated with emotional instability via BSL-23 scores, 15 its lack of a strong association with WM (ρ = −0.20, p = .29) or significant ED linkage (ρ = 0.41, p = .03) in the regression model challenges models positing cognitive deficits as primary SIB drivers. 10 Instead, our data support a dual-process theory, where limbic hyperactivity and prefrontal hypoactivity interplay, with emotional triggers dominating, 23 a dynamic also relevant to addiction relapse. 24 This suggests that while cognitive deficits contribute to the broader impulsivity seen in BPD, the more direct and immediate triggers for SIB may be rooted in emotional dysregulation, with cognitive factors potentially playing a more indirect or moderating role. Future research should explore the complex interplay between these cognitive and emotional pathways, perhaps through mediation or moderation analyses, to better understand their combined influence on SIB.
Clinical Implications
Identifying ED and WM as significant predictors of impulsivity suggests that cognitive remediation therapy (CRT)—using adaptive WCST or n-back tasks—could serve as a valuable adjunct to existing treatments like dialectical behavior therapy (DBT). In addiction contexts, CRT has shown promise in reducing relapse by strengthening cognitive control, indicating potential cross-applicability for BPD’s impulsive and SIB. Practically, CRT could be integrated into DBT by incorporating specific cognitive exercises into individual therapy sessions or group skills training. For instance, after teaching emotion regulation skills, a therapist might use WCST-based exercises to help patients improve cognitive flexibility in applying these skills under emotional distress. Combining DBT’s emotion regulation focus with CRT may thus address both cognitive and affective deficits more comprehensively. 25
Strengths and Limitations
This study’s strength lies in its multimodal approach, merging neurocognitive and behavioral measures to explore cognition-impulsivity links in BPD. The a priori power analysis ensures an adequate sample size and complete data collection, enhancing the reliability of our findings. However, several limitations should be considered. First, the cross-sectional design precludes inferences about causality, meaning we cannot determine if ED and WM deficits precede or result from impulsivity and SIB. Second, the relatively small sample size (N = 30) limits the generalizability of these findings to broader BPD populations. Third, the absence of an age and gender-matched control group is a significant limitation, preventing direct comparisons of cognitive functions between individuals with BPD and healthy controls. Therefore, our findings should be interpreted with caution regarding the absolute severity of cognitive impairments in BPD. Fourth, while the study focused on cognitive deficits, the neurocognitive assessments did not directly incorporate emotional factors. Future research could benefit from more integrated emotional-cognitive assessments to offer a fuller picture of BPD’s neurocognitive profile, given the centrality of emotional dysregulation in BPD. Additionally, while standardized administration protocols were followed, assessors were not blinded to the BPD diagnosis due to the clinical context, which may have introduced minor assessment bias. However, efforts were made to mitigate this.
Future Directions
To establish causality, future research should prioritize longitudinal studies to determine if ED and WM deficits precede or are a consequence of chronic impulsivity and SIB in BPD. Specifically, these studies could track cognitive development and behavioral outcomes over time, potentially using growth curve modeling to identify predictive relationships. Functional neuroimaging studies (e.g., fMRI) could further map the neural correlates of these cognitive deficits and their dynamic interplay with emotional circuits during impulsive or self-injurious urges. 7 Furthermore, randomized controlled trials are critically needed to robustly test the efficacy of cognitive remediation therapy in reducing impulsivity and SIB in BPD, potentially informing addiction treatment strategies as well. Such trials could compare CRT as a standalone intervention, as an adjunct to DBT, or against other active control conditions to determine optimal treatment approaches. 24
Conclusions
This study provides empirical evidence linking impulsivity, ED, and WM impairments in BPD. Our findings suggest that targeting cognitive flexibility and WM through remediation could significantly mitigate impulsive and SIB in this population, with broader implications for addiction-related interventions. These results underscore the importance of a neurocognitive perspective in understanding BPD and suggest a shift towards more integrated treatment approaches. By highlighting the specific cognitive deficits contributing to impulsivity, this study can directly influence future clinical approaches to BPD, encouraging the incorporation of cognitive assessments and remediation strategies into routine psychiatric care. Furthermore, these findings could inform policy and practice in psychiatric settings by advocating for resources and training dedicated to cognitive interventions, ultimately leading to more comprehensive and effective care for individuals with BPD.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
The authors acknowledge the use of Grok, an AI tool developed by xAI, for assistance in drafting and revising manuscript sections. All content was reviewed and edited by the authors, who take full responsibility for its accuracy.
Data Sharing Statement
Deidentified individual participant data will not be made available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No generative AI tools were used to collect or analyze data, produce images or graphs, or to write this article. Assistance from an AI tool developed by xAI was used for drafting and revising sections. The authors assume full responsibility for its entire content.
Ethical Approval
GMKMC&H/114/IEC/2023-34.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Permissions
All assessment tools used in this study, including the Wisconsin Card Sorting Test (WCST), Letter-Number Sequencing (LNS) task from the WAIS-IV, Barratt Impulsiveness Scale (BIS-11), Deliberate Self-Harm Inventory (DSHI), and Borderline Symptom List (BSL-23), were either purchased or used under appropriate licenses by the research team. The Mini-International Neuropsychiatric Interview (MINI) was not utilized in this study.
Prior Presentations
None.
Simultaneous Submission
This manuscript is not under consideration elsewhere.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.