
Abstract
Background:
Exposure to complex trauma in early childhood can undermine the development of mentalization capacity. Complex trauma has also been causally linked to borderline personality disorder (BPD). The inclusion of complex post-traumatic stress disorder in ICD-11 has made it imperative to have an in-depth understanding of complex trauma.
Methods:
This study used an explanatory sequential mixed method approach to assess the complex trauma and mentalizing ability in college students with BPD (N = 62) in comparison to non-BPD students (N = 60) and to explore the subjective experiences of complex trauma in students with BPD (n = 10). Participants in both groups were assessed on the Childhood Experience of Care and Abuse Questionnaire and the Reading the Mind in the Eyes Test to assess complex trauma and mentalizing ability, respectively. Qualitative data were collected through focused interviews using a phenomenological approach.
Results:
Those with BPD had significantly higher rates of six types of complex trauma as compared to those without BPD; additionally, participants who had experienced sexual abuse performed better on mentalizing tasks than those who had not. The focused interviews revealed several themes, including “perpetrator,” “impact,” “symptoms,” and “strengths,” which indicated intergenerational trauma and hope for post-traumatic growth.
Conclusion:
Although participants with BPD experienced higher complex trauma, they also had better mentalizing capacities.
Participants with borderline personality disorder (BPD) experienced more complex trauma than participants without BPD. Strikingly, participants who suffered sexual abuse had better mentalizing ability than participants who did not. Participants experienced significant post-traumatic growth; this was the highlight of the focused interview conducted to explore the subjective experience of trauma.Key Messages:
Etiological theories of borderline personality disorder (BPD) have evolved with the understanding of complex trauma. The word “trauma” was unheard of in the initial theories of BPD. 1 A review applying Hill’s criteria for causation established a causal relationship between complex trauma and the development of BPD. 2 More recently, the inclusion of complex post-traumatic stress disorder (CPTSD) in ICD-11 3 has brought complex trauma to the forefront. It is noteworthy that BPD and CPTSD, while distinct diagnoses, often co-occur at a high rate. 4 In literature, the relationship between specific trauma types and outcomes in adulthood has shown inconsistencies. Many studies have focused on a single type of traumatic experience, especially childhood sexual abuse (CSA), when trying to understand personality disorders like BPD. For instance, a cross-sectional study looked at the effect of childhood maltreatment on the development of personality disorders, but it did not explore complex trauma, considering its various subtypes. 5 Similarly, a review exploring the association between childhood trauma and personality disorders was found to be restricted to community studies of childhood sexual and physical abuse. 6
Several studies have made efforts to address these biases by exploring the subtypes of complex trauma, examining the frequency of traumatic incidents, and adopting a prospective study design. A systematic review identified that risk factors, including the domains of social, family, maltreatment, and childhood, are prospectively associated with the development of BPD. 7 In addition, a case-control study found that the frequency of traumatic experiences in childhood was significantly higher in individuals with BPD when compared to healthy controls (HC). 8 Furthermore, an exploratory case-control study from India employed a semi-structured interview to get a comprehensive understanding of complex trauma, including domains of physical, emotional, and sexual abuse and general traumatic experience. 9
Complex trauma has also been studied with regard to mentalization, and studies have consistently shown that exposure to trauma can lead to poor mentalizing ability.10,11 In the context of mentalization and BPD, the research findings have been somewhat mixed. A review found that individuals with BPD often have impaired mentalizing capacity, especially in attributing emotions, thoughts, and intentions of others. 12 On the other hand, one study using two tasks to assess mentalizing ability found no significant differences between participants with BPD and HC. The reasons can be as follows: first, the cartoon story-based task was designed primarily to assess mentalizing skills in patients with psychosis, and second, the task was the single offline emotionally neutral task, which assessed cognitive mentalization. Hence, both tasks may not have sufficiently tapped into the mentalizing ability of participants with BPD. 13 Conversely, another study reported that participants with BPD demonstrated a better capacity to discern mental states by examining the eyes as compared to those with HC. The BPD group had higher Beck’s Depression Inventory scores as compared to the HC group, which may have contributed to better performance in RMET in the BPD group. The groups were also not matched based on gender. 14
Herman 15 stated that individuals with complex trauma often express feelings as though they have become different people. Those affected severely have even stated sentiments like “I am not a person.” 15 Trauma is a personal experience that is perceived differently by each individual. The use of standardized scales may not assess a variety of experiences. This subjective understanding of complex trauma makes the study findings comprehensive. Complex trauma can be assessed better using such narrative experiences. 16 In the present study, along with quantitative measures, we have also assessed subjective experiences of trauma through focused interviews.
Given the new classification of personality disorders as mild, moderate, and severe in ICD-11, studying young adults with BPD symptoms is essential to address mild/moderate levels of BPD. A study pointed out that most of the research on BPD has been done on patients with severe symptoms who are currently undergoing treatment. Therefore, it urged future research to explore individuals with milder BPD symptoms. 17
Hence, the present study aimed to assess the complex trauma and mentalizing ability of college students with and without BPD and to explore subjective perceptions of complex trauma in young adults with BPD. The study hypothesized that those with BPD will report higher rates of complex trauma experiences and will have poorer mentalizing than those without BPD. Those with complex trauma will have worse mentalizing abilities compared with those without.
Methods
Participants in a Quantitative Study
The study participants were 122 students of different genders between 18 and 25 years, recruited from different colleges of Manipal Academy of Higher Education through purposive sampling. The sample consisted of two groups, that is, participants with BPD (N = 62) and without BPD (N = 60), based on the presence (score of 7 or above) or absence of symptoms as assessed by the Mclean Screening Instrument for BPD (MSI-BPD). 18 Participants with major psychiatric illnesses, including psychosis, mood disorders, and substance abuse disorders (except tobacco abuse), were excluded after screening them on the Modified Mini Screen (MMS). 19
Participants in the Qualitative Study
Ten participants of different genders who had experienced complex trauma, as assessed on the Childhood Experience of Care and Abuse Questionnaire (CECAQ), 20 were recruited from the BPD group. Only those participants who were verbally expressive, consented to the interview, and were undergoing psychotherapy were included.
Measures
The sociodemographic and clinical data sheet included the following information: age, gender, education, economic status, occupation, type of family, marital status, whether currently undergoing psychotherapy, and information related to substance use/abuse, including its presence/absence, form, duration, and last use.
The MMS. 19 has 22 items that assess various domains, including mood disorders, anxiety disorders, and psychotic disorders. It is based on DSM-IV, 21 Structured Clinical Interview for DSM Disorders (SCID), and the Mini International Neuropsychiatric Interview (MINI). MMS scores are calculated by adding the affirmative responses to the questions, and further categorization is based on the severity of symptoms. It has good internal consistency (Cronbach’s α 0.91) and concurrent validity with Brief Symptom Inventory.
The Mclean Screening Instrument for BPD (MSI-BPD) 18 is based on a subset of the questions that comprise the borderline module of the Diagnostic Interview for Personality Disorders from DSM-IV. It has 10 items with yes/no responses. A score of 7 or higher implies a possible diagnosis of BPD. The instrument has excellent internal consistency (α = 0.90) and showed substantial congruent validity compared to BPD diagnoses based on SCID-II (ROC AUC = 0.96).
CECAQ 20 is a self-report, retrospective measure of complex trauma in the form of lack of parental care by father and mother figures (neglect and antipathy), parental physical abuse, and sexual abuse by any adult before age 17. It has high internal consistency (Cronbach’s α 0.80 and 0.81 for two subscales) and robust test–retest reliability.
Reading the Mind in the Eyes Test (RMET) 22 assesses mentalizing abilities, which involve recognizing visual cues to emotion and/or empathy using 36 photographs of the eye region. The participants are asked to choose which of four words best describes the person’s feelings. A score of 0 or 1 is given for every wrong and right answer, respectively. It has good internal consistency (Cronbach’s α 0.72), robust test–retest reliability (0.83), and good convergent and discriminant validity. 23
Focused interviews were conducted to understand the subjective experience of complex trauma. The interview guide was prepared based on an extensive literature review. Anchor questions were developed to guide the interview process. Three experts validated the interview questions: a qualitative research expert, a clinical psychologist, and a psychiatrist, each with over eight years of experience in their respective fields. After the questionnaire was prepared, it underwent field testing with two participants. Based on their suggestions and reflections, the wording for some of the questions was changed, and the final version of the interview was administered to collect qualitative data.
Procedure
The present study used an explanatory sequential mixed method design. 24 It was carried out from March 2022 to October 2022 in a tertiary care teaching hospital in South India. Permission was sought from the respective deans of the colleges to recruit participants. Additionally, approval was obtained from the Institutional Ethics Committee, and the study was registered with the Clinical Trials Registry of India. The study was conducted in two phases. In the first quantitative phase, a Google Form containing sociodemographic and clinical information data sheets and MSI-BPD was circulated to students with the help of class representatives. The flow of the participants is shown in Figure 1. Consenting participants who met the inclusion–exclusion criteria were called to the Dept. of Clinical Psychology to administer CECA-Q and RMET.
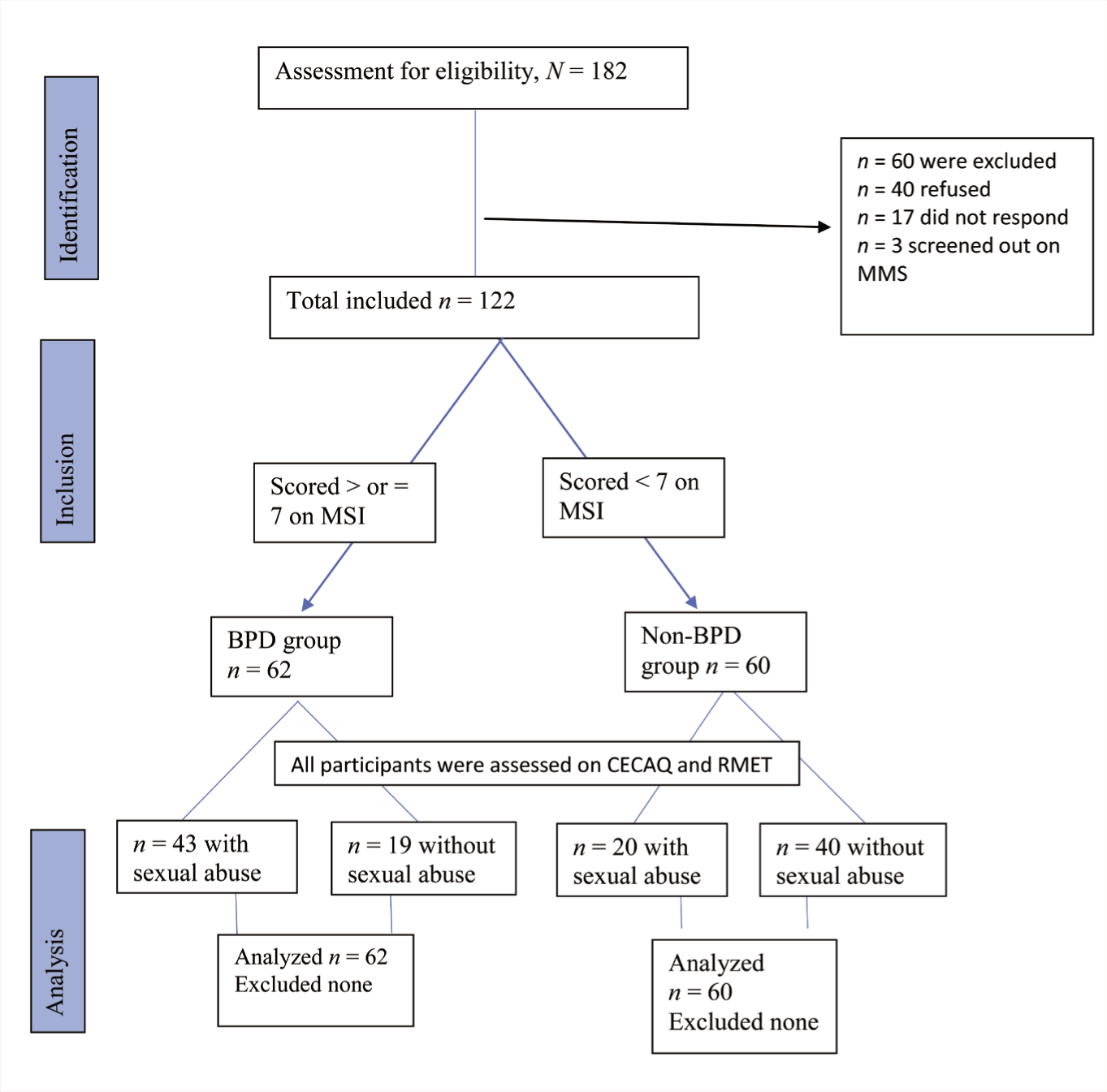
BPD: Borderline personality disorder; MSI: Mclean Screening Instrument; CECAQ: Childhood Experience of Care and Abuse Questionnaire; RMET: Reading the Mind in the Eyes Test.
In the qualitative phase, out of the 62 participants with BPD, 10 consenting participants met the inclusion criteria for the focused interviews. Face-to-face interviews were conducted in a quiet room at the participants’ convenience. Interviews were carried out by the principal investigator, who had received supervision from a subject expert and underwent practice sessions with mock interviews. The interviews were conducted in English, and the interviewer was proficient. Each interview spanned between 20 and 40 minutes without any breaks. All focused interviews were audio recorded.
Ethical Considerations
Written consent was obtained from the participants. All documentation-related ethical guidelines for quantitative and qualitative data were followed. Participants were debriefed regarding the study. After the interview, participants were taught simple deep breathing and grounding techniques. Participants with complex trauma or BPD were sensitized and urged to seek professional help.
Analysis
The quantitative data was analyzed using SPSS 22.0 for Windows (IBM Statistics). 25 Data normality in mentalization scores was examined using the Shapiro–Wilk test and histogram analysis. The chi-square and independent t-tests were conducted to examine the group differences in categorical and continuous variables, respectively. As mentalization scores in those with or without complex trauma were not normally distributed, the Mann–Whitney U test was done to see the group differences. For this, the data from both groups were combined and divided based on the absence and presence of complex trauma.
Braun and Clarke’s 26 process for thematic analysis was used for the qualitative analysis. The investigators first became familiar with the transcribed interviews, and then ideas and concepts were identified from the data and coded. An iterative process of coding, categorizing, and developing themes was then conducted. Data triangulation was carried out by two researchers, who generated themes from the data and conducted debriefing sessions with another research team member. Reliability and validity were ensured by carefully assessing outliers, checking for researcher effects, and eliciting participant feedback.
Results
Quantitative Results
Sociodemographic and Clinical Characteristics
The distribution of sociodemographic and clinical variables is shown in Table 1. The only significant difference between the two groups was in the stream of education (χ2 = 9.29, p = .026). The non-BPD group constituted more students from allied health (n = 40, 66.7%), while the BPD group had fewer students (n = 25, 40.3%). However, the BPD group had more students from medicine (n = 17, 27.4%) and humanities (n = 13, 21%) as compared to non-BPD (medicine: n = 11, 18.3%; humanities: n = 7, 11.7%). There was a significant difference in tobacco dependence and number of students undergoing psychotherapy between participants with and without BPD.
Comparison of Sociodemographic and Clinical Variables Between Participants with (N = 62) and Without (N = 60) BPD.
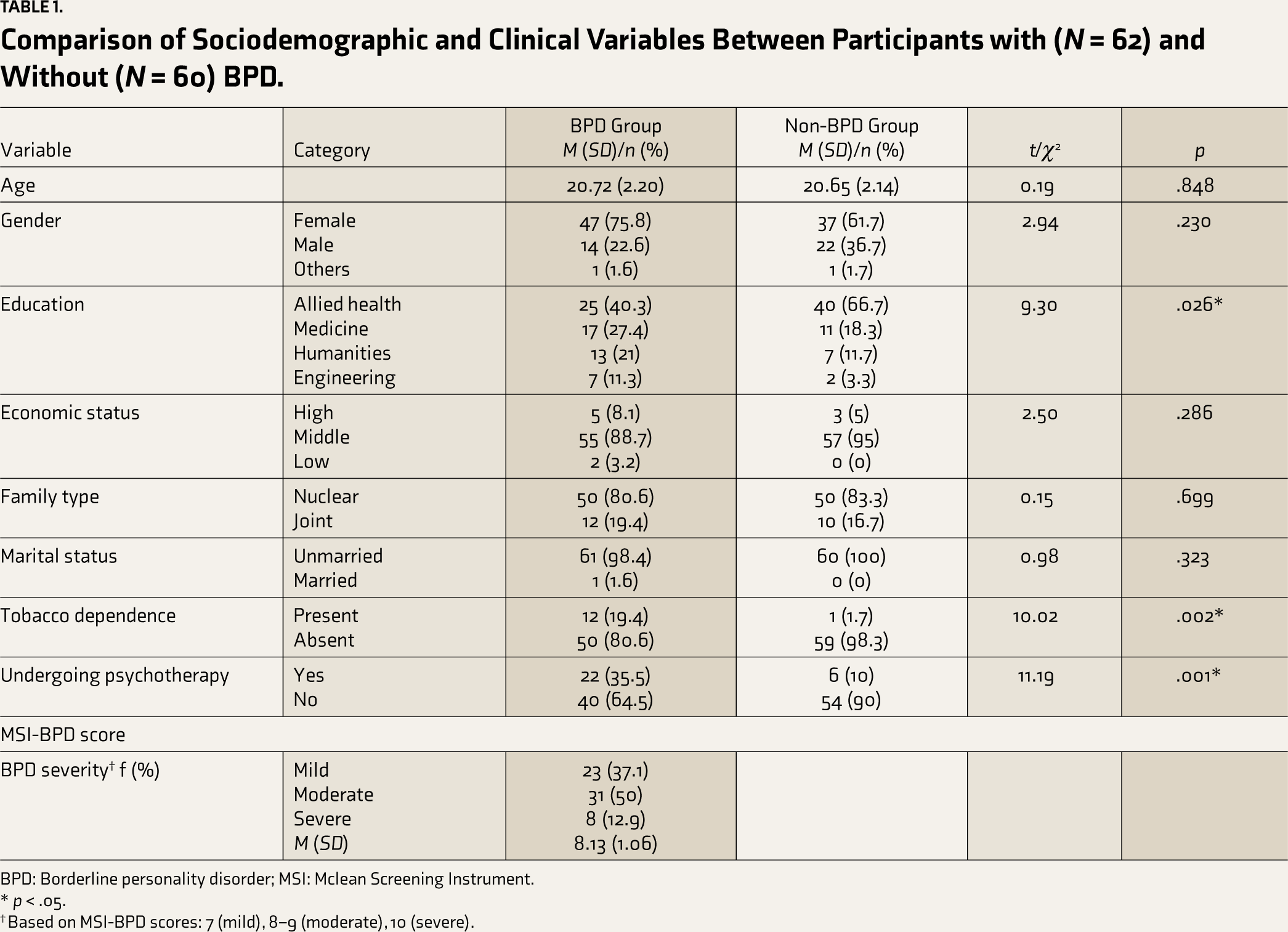
BPD: Borderline personality disorder; MSI: Mclean Screening Instrument.
* p < .05.
† Based on MSI-BPD scores: 7 (mild), 8–9 (moderate), 10 (severe).
Complex Trauma in Participants With and Without BPD
Table 2 shows that participants with BPD reported more types of complex trauma (antipathy mother, antipathy father, neglect father, physical abuse, sexual abuse screen, and sexual abuse severity) compared to participants without BPD. Concerning specific types of complex trauma, a relatively more significant number of participants with BPD (n = 43) reported sexual abuse compared to participants without BPD (n = 20).
Difference in Types of Complex Trauma Between Participants with (N = 62) and Without (N = 60) BPD.
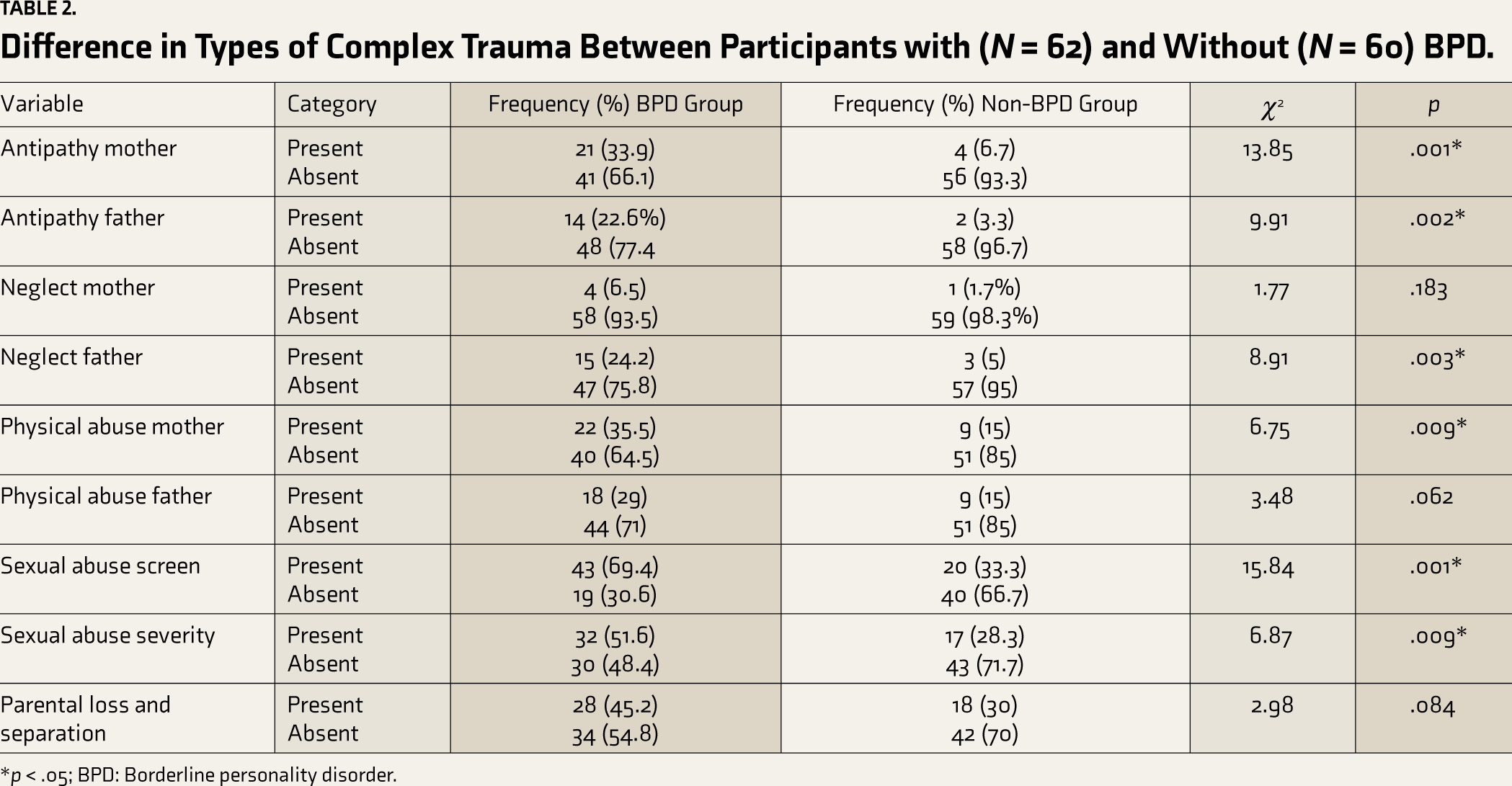
*p < .05; BPD: Borderline personality disorder.
Mentalizing Ability in Participants With and Without BPD
Mentalizing ability was not significantly different (Table 3) between participants with and without BPD.
Mentalizing Ability in Participants With and Without Complex Trauma
The Mann–Whitney U test showed that out of all types of complex trauma, mentalizing scores were significantly different (Table 3) only between participants with and without sexual abuse, that is, participants with sexual abuse had higher mentalization scores than those without.
Group Differences in Mentalization Scores Across Categories.

* p < .05; RMET: Reading the Mind in the Eyes Test; BPD: Borderline personality disorder.
Qualitative Results
All 10 participants were unmarried students (7 females and 3 males) between 18 and 25 years old (M 20.9, SD 2.5) pursuing different educational streams (e.g., allied health sciences, medical, pharmacy, etc.).
Table 4 lists the 20 sub-themes that fit under four themes and statements from participants in the respective sub-themes.
Themes and Sub-themes Derived from Qualitative Data.
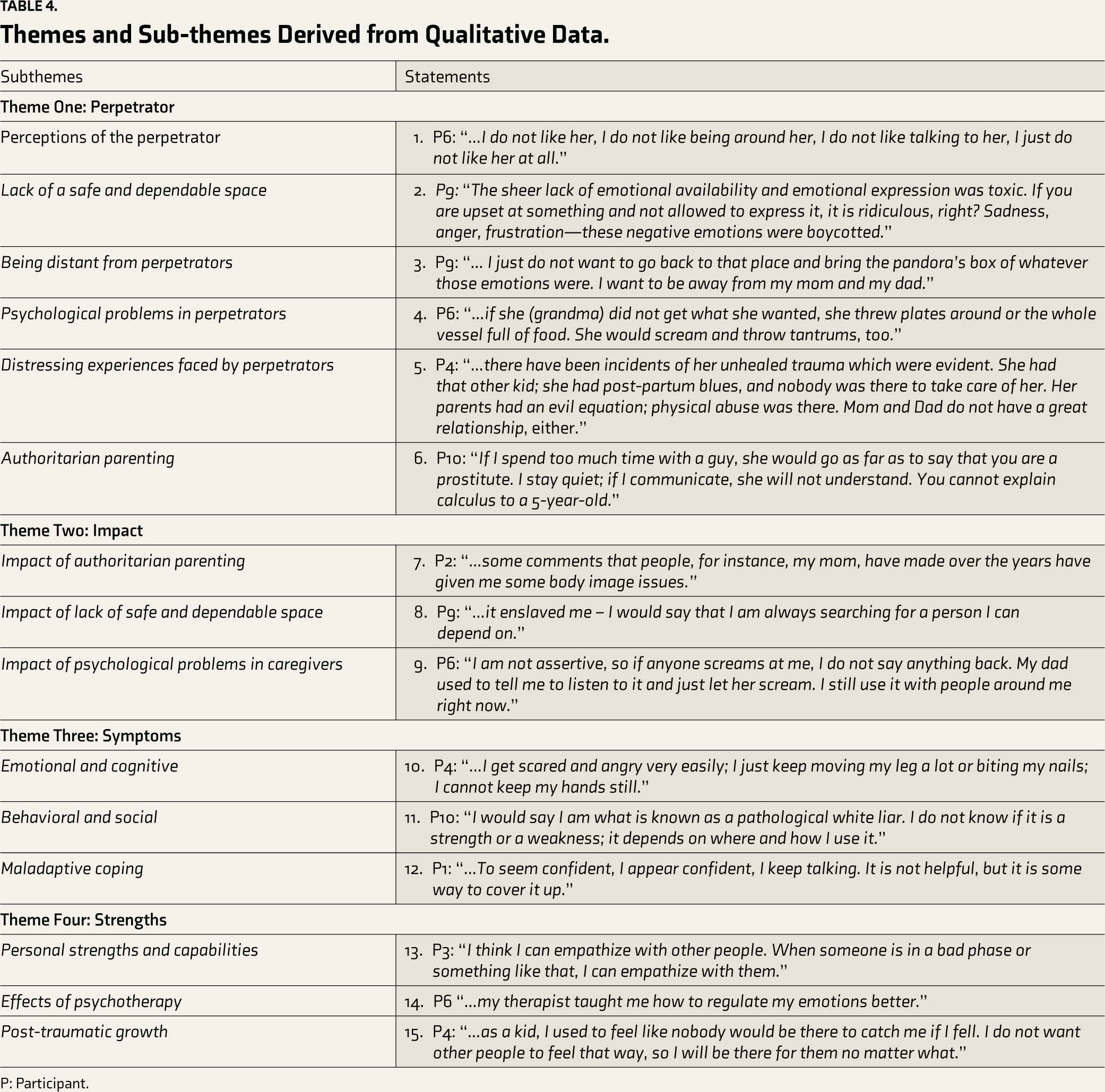
P: Participant.
Perpetrator (n = 10)
Participants were given the option to choose the perpetrator they would talk about. For most participants, the perpetrator of abuse was a parent. However, one participant’s grandmother was the abuser, and the other two reported instances of sexual abuse by people outside their families. Though participants initially started talking about one perpetrator, their experiences were intertwined with other perpetrators who were family members residing at home.
Perception of the Perpetrator (n = 8)
Many participants expressed dismay toward the perpetrators. However, opposing views were also expressed. Participant 6 (statement 1) expressed hatred for the perpetrator, as he would make many significant decisions for him, leaving little to no agency. Others have had mixed feelings toward the perpetrators.
Lack of a Safe and Dependable Space (n = 5)
Lack of a safe space in childhood was reported by many since the perpetrators, who were parents in most instances, were either not around or were emotionally unavailable (statement 2, P9).
Being Distant from Perpetrators (n = 7)
Participants reported wanting to maintain a distance from the perpetrators. Some wanted to avoid the yelling, while others were unwilling to revisit unresolved issues and the associated difficult emotions. Participant 1 was so scared of her mother yelling that she would shut herself completely (statement 3, P9).
Psychological Problems in Perpetrators (n = 6)
Participants were aware of psychological issues in perpetrators and believed that was the reason for abuse. The most evident one was their inability to regulate emotions (statement 4, P6). Along with emotional dysregulation, the need for control regarding how she dressed, studied, and even who her friends were was reported by Participant 8.
Distressing Experiences Faced by Perpetrators (n = 6)
While trying to understand why the perpetrators behaved the way they did, many participants were able to empathize with the struggles they have gone through (statement 5, P4).
Authoritarian Parenting (n = 7)
Most perpetrators were described as critical and allowed minimal autonomy (statement 6, P10).
Impact (n = 9)
Impact of Authoritarian Parenting (n = 6)
For Participant 1, being indecisive and having low confidence have been attributed to authoritarian parenting by her mother. (statement 7, P2).
Impact of Lack of Safe and Dependable Space (n = 4)
Since she could not express her emotions in childhood, Participant 2 became uncomfortable around genuine emotions. Participant 3 compulsively tries to be in others’ “good books” because of the lack of attention in childhood (statement 8, P9).
Impact of Psychological Problems in Caregivers (n = 3)
As a result of the psychological problems of caregivers, participants themselves seemed to have developed psychological issues. While talking about her mother, Participant 4 stated that she has low self-esteem because of her mother’s lack of self-worth, and she ends up becoming a parent to her mother when she visits her. Parentification was also reported in the form of trying to “fix” the family by asking them to go for therapy by Participant 9 (statement 9, P 6).
Symptoms (n = 10)
Emotional and Cognitive (n = 9)
Emotional dysregulation and autonomic arousal were quite prominent in the daily lives of many participants (statement 10, P4). Participant 6 experiences anxiety, which makes her breathless and overwhelmed quickly. Participant 3, who also reported sexual abuse, was unable to process the perpetration because she had not expected it and was shocked, angry, and disgusted when it happened. Excessive rumination, worry, and different irrational thoughts were also reported. Participant 6 stated entering a “rabbit hole” of self-blame.
Behavioral and Social (n = 7)
Non-suicidal self-injury, acting out, and lying (statement 11, P10) have been reported as behaviors participants engage in. Participant 9 reported breaking chairs and harming himself. Engaging with people in social settings and having honest, open conversations was hard for some participants. Participant 2, who was sexually abused, was also weary of unsolicited touch.
Maladaptive Coping (n = 8)
For difficult emotions, most participants used some maladaptive coping strategies, such as overcompensating by talking (statement 12, P1), overworking, blaming others, dismissing difficult emotions, etc.
Strengths (n = 10)
Personal Strengths and Capabilities (n = 9)
Participants possessed various strengths, such as being helpful, funny, good artists, good communicators, good at teamwork and project management, and empathetic (statement 13, P3).
Effects of Psychotherapy (n = 9)
Participants stated that psychotherapy helped them understand their feelings and regulate their emotions better (statement 14, P6). Few also reported being mindful of their actions and being less impulsive. Participant 5 had become weary of his actions and had more clarity due to being answerable in therapy. For participant 8, it also helped reduce her impulsive behaviors like sending passive-aggressive text messages and blaming others.
Post-traumatic Growth (n = 3)
Post-traumatic growth (PTG) was seen when participants reported growing from and because of their traumatic experiences (statement 15, P4). Finding a healthy attachment bond after the traumatic experiences was reported by participant 9.
Discussion
Quantitative findings indicated that participants with BPD scored significantly higher in six out of nine types of complex trauma than non-BPD participants. Notably, there was no significant difference in mentalization between the two groups, but participants with CSA had better mentalizing abilities than those without. It is essential to highlight here that the current understanding of personality disorders is moving toward a dimensional approach, although we have taken a categorical approach to divide the groups. Qualitative findings included several vital themes: perpetrator, impact, symptoms, and strengths. Differences were noted in complex trauma arising from paternal and maternal sources. Very few prior studies have examined specific paternal and maternal abuse, and a need to study the same was highlighted in a review. 27
“Teaching Calculus to a Five-year-old”—Emotional Abuse
Participants with BPD exhibited significantly higher complex trauma of antipathy from mother and father. Antipathy, like emotional abuse, included experiences such as being criticized, being picked on, and feeling unwanted by their mother and father figures before the age of 17. Indeed, a cross-sectional study found that childhood emotional abuse was the unique predictor of BPD as opposed to emotional neglect, physical abuse, and neglect and sexual abuse. 5
Participants also indicated this while discussing the impact of psychological problems on perpetrators. As a result of being subjected to anger and hostility by perpetrators, participants reported experiencing parentification, wherein they assumed the caregiving role for their parents instead of receiving care themselves. A cross-sectional study found that young adults who had higher levels of caregiving responsibilities with their mothers were more likely to exhibit borderline traits than those with fewer caregiving behaviors. 28 Parentification is a significant form of emotional abuse that results in dysfunctional boundaries between the victim and the perpetrator.
Another complaint reported while speaking of emotional abuse by perpetrators was a lack of assertiveness. A recent study found the presence of the internalizing cluster, including lack of assertiveness, as a personality trait in patients with BPD. 29 Though externalizing traits have traditionally been associated with BPD, examining the internalizing traits is crucial.
“If I Fall, Nobody Will Be There to Catch Me”: Physical and Emotional Neglect
Neglect by the father was another type of complex trauma found to be significantly higher in the BPD group. According to them, father figures were found to leave them unsupervised, were not interested in what they did at school or who their friends were, and did not seem concerned about their whereabouts before the age of 17. A case-control study comparing patients with BPD with other personality disorders found that 92% of patients with BPD reported being neglected by their caretakers before the age of 18. 30
When participants discussed the absence of a safe and dependable space, they described perpetrators as being physically absent or emotionally unavailable. As a result, participants stated that they were uncomfortable with genuine emotions, leading to difficulties in interpersonal relationships. Additionally, while speaking of being distant from perpetrators, participants reported being unwilling to open up to them due to unresolved emotional wounds.
However, an outlier reported feeling safe despite lacking an adequate emotional attachment to her mother. This observation aligns with contrasting literature that, despite the presence of “ghosts in the nursery” (indicating intergenerational transmission of the feelings of helplessness and fear), the benevolence of parents, including unconditional love, can be passed down through generations, leading to a positive influence on an infant’s development. 31 Moreover, Winnicott’s concept of “good enough mother” supports this finding, suggesting that mothers who have successfully provided a safe environment despite the traumatic experiences have been good enough mothers.
“You Are Not Allowed to Express Dissent!”: Physical Abuse
Physical abuse by mothers was another type of complex trauma that was significantly higher in the BPD group. Participants reported being hit repeatedly before the age of 17. A prospective study found that significantly more children with physical abuse, along with other types of abuse, met the criteria for BPD in adulthood compared to HC. 32 Physical aggression has been a significant precursor to the development of BPD. As a result of feeling physically unsafe within their attachment context, these individuals may grow up to feel unsafe and emotionally dysregulated in interpersonal relationships, which seems to be leading to symptoms of BPD.
While discussing perpetrators being authoritarian parents, they thwarted the participants’ need for autonomy by using specific disciplinary strategies such as physical punishment and verbal hostility. This resulted in them being indecisive and having excessive self-doubt, along with frequent self-critical thoughts, which are prominent features of BPD. A longitudinal study found that authoritarian parenting predicted aggression and borderline features in adolescent females, whereas authoritative parenting served as a protective factor against aggression and borderline features. 33
Overall, it is interesting to note that three-fourths of the participants who perceived emotional neglect from fathers and physical neglect from mothers were females. Considering the cultural differences in parenting, Indian parenting styles may have contributed to such findings.
“As a Child, I Was Scared of Everything”: Sexual Abuse
Lastly, like existing findings in the literature, sexual abuse was found to be significantly higher in the BPD group. Participants had a much higher number of incidents of sexual abuse before the age of 17. A cross-sectional study found that 62% of patients with BPD reported CSA. 34
Intergenerational trauma was reported as one of the reasons for emotional dysregulation in them, which constituted traumatic experiences they had themselves faced. It has become essential to break this chain of intergenerational trauma by understanding its roots and providing necessary help and support. A review that focused on preventing intergenerational trauma recommended psychotherapy and the provision of active support for parent–infant attachment. 35
Mentalizing and BPD
Mentalizing includes both cognitive and emotional aspects. 36 No significant difference was found in mentalizing between both groups. Similar to our findings, several studies that have used facial recognition tasks like RMET for studying mentalization have found that participants with BPD did not differ from other groups or even performed better than controls in a few instances.37,38 These contradictory findings can be attributed to the aspects of mentalization that were measured in the studies and the type of measurement used to assess mentalization in specific situations. The BPD group shows no deficits in the theory of mind, which is considered one aspect of mentalization rooted in the cognitive psychology tradition. In contrast, mentalization is a psychodynamic complex and multi-dimensional phenomenon in which the BPD group shows deficits. Further, two types of mentalization tasks have been used in the literature. Simple tasks measuring isolated functions that require predicting only other people’s behavior or complex batteries require participants to also understand their own emotions and experiences about others, including naturalistic conditions. The BPD group shows impaired mentalization only during the administration of complex tasks. 39
Hence, in the present study, similar performance levels in mentalization between those with and without BPD can be attributed to the task used to assess mentalization, that is, RMET. This task assesses the perceptual aspect of recognizing emotions based on a static photograph reflecting only the eye region. This makes the task simple and may not be tapping into the aspect of mentalizing ability, which is likely to be impaired in the BPD group. 40
Studies that focused on the accuracy of inferring others’ emotional states described a term called “borderline empathy,” which referred to enhanced affective mentalization in BPD. 41 A study found that participants with severe BPD had better empathic accuracy than those with milder symptomatology. The study added that the empathic advantage might not necessarily reflect better ability but may be attributable to the harder-to-infer thoughts and feelings that they possess. 42
During social interactions, though participants with BPD can make complex attributions about people’s actions by looking at pictures, they usually presume their intentions to be malevolent. The roots of this assumption of malevolence lie in the relational trauma experienced by caregivers in childhood, a shared experience among those with BPD. 43 This was further evident when participants spoke of their perception of the perpetrator, where they expressed significant dismay and dislike toward them.
Participants with BPD have a heightened sensitivity to fear. However, they accurately perceive others’ basic emotions when exposed to still pictures of faces. 44 Studies have found a positive relationship between the accuracy of perceiving others’ emotions and one’s physiological arousal. 45 Therefore, participants with BPD can accurately perceive basic emotions. However, they may be hyperreactive to certain negative emotions that trigger their fears. This may lead to their adequate performance in basic mentalizing tasks.
Mentalizing and Complex Trauma
Participants with CSA performed better at the mentalizing task than those without CSA. Individuals with complex trauma have a hyper-aroused stress system, because of which rapid automatic and biased mentalizing associated with the limbic structures takes place instead of the elaborate and controlled mentalizing associated with the prefrontal cortex. In their model for explaining how this rapid automatic processing partakes of a non-mentalizing route, Luyten et al. 46 proposed three ways to experience themselves and others: psychic equivalence, teleological, and pretend modes. In the pretend mode, one gets so consumed with ruminating about past and future events that one dissociates. 46 Looking at interpersonal cues like facial emotions in the RMET, they may dissociate and enter this pretend mode. RMET has been assumed to involve rapid processing that triggers related memories from the past associated with the lexicon of emotions seen in the pictures presented. 21 In this study, participants with complex trauma reported several distressing memories related to antipathy and physical and sexual abuse from their primary caregivers. These would have been activated rapidly while looking at pictures of similar emotions during the task.
“Pandora’s Box of Unresolved Emotions”: Symptoms
Participants elaborated on several instances of being in Luyten et al.’s 46 three modes. They reported having low self-esteem and feeling unwanted, which are examples of the psychic equivalence mode where thoughts and emotions are experienced as too accurate. They reported non-suicidal self-injury, acting out, lying, being too nice to others, talking excessively, and blaming others, which are examples of the teleological mode where they engage in actions that take precedence to provide relief from emotional pain. Finally, the pretend mode could be observed when participants reported being unable to process and make a coherent meaning of the traumatic experience. Subjective descriptions of their experiences fit with Luyten et al.’s 46 model.
“I Have Become Empathetic Because of My Experiences”: Strengths and PTG
The many strengths and considerable PTG reported by participants seemed like a silver lining in the findings related to complex trauma. The study delineated strengths and adaptive characteristics that participants reportedly developed due to traumatic experiences or psychotherapy, for example, finding healthy attachments, being empathetic, regulating emotions, etc.
There is ample literature on how a higher number of adverse childhood events (ACEs) can influence adult mental and physical health. However, only a few studies have tried to understand the positive counterpart, or positive childhood experiences (PCEs). A few studies have been based on data from nonrepresentative samples. One of them found that interpersonal PCEs have a protective effect on pregnant women and young adults exposed to ACEs. 47 In the current study, many participants experienced PCEs, which led to a feeling of safety despite the traumatic experiences they faced in childhood.
With the increased recognition of intergenerational trauma, studies have looked at what promotes these PCEs by caregivers. Despite being exposed to complex trauma themselves, many parents managed to be attuned and empathetic toward their children without any intervention. 31 It seems that the transmission of cultural resilience through shared narratives of trauma and cultural strength is what promoted them to be attuned parents despite being subjected to complex trauma. 48 These factors could have led participants to have a safe space despite lacking an emotional attachment.
Furthermore, a study found that adolescents with BPD had few protective factors, like individual competence or a positive relationship with a family member. 49 In the current study, participants were found to have protective factors, including resilience, empathy, a good sense of humor, great teamwork, and calmness in stressful situations. These resources are further enhanced as they continue psychotherapy and move toward combating their emotional dysregulation. As a result of psychotherapy, participants also reported being mindful, less impulsive, able to understand and regulate their emotions better, calm and compartmentalizing, having insight, and reducing self-blame. A meta-analysis concluded that psychotherapy was found to lead to a better quality of life in participants with BPD. 50
PTG is a crucial variable that has been studied extensively in the past decade. Participants reported growing from and because of their traumatic experiences. They added that they could be there for other people since they did not have adequate support because of their traumatic experiences. They learned to identify and develop healthy attachment bonds. They also learned to be different from their perpetrators to avoid becoming perpetrators. Few participants could appreciate their traumatic experiences since those are what led them to become who they are today. Since PTG is an ongoing process, these individuals will continue to work on themselves and heal their attachment wounds to break the cycle of intergenerational trauma, with and without psychotherapy.
Limitations
The BPD diagnosis was made using MSI-BPD, which is a screening instrument. Screening instruments are used to detect the possible presence of symptoms or to identify whether a person is at an increased risk of developing the condition. A structured interview could have been used to confirm the diagnosis. The tool used for studying mentalizing capacities needs to be ecologically valid. However, it was used due to a need for greater availability of culturally fair tools. In terms of complex trauma, data regarding the frequency and duration of the types of complex trauma, which could have given a more accurate picture, was not collected. The cross-sectional nature of the quantitative data makes it only partially reliable. The difference found in both groups in terms of education, tobacco dependence, and whether they were currently undergoing psychotherapy could have served as confounding variables. For the qualitative data, no information was collected for each participant’s type and stage of psychotherapy. This could have given a better picture of the effects of psychotherapy.
Conclusions
The study aimed to assess complex trauma and mentalization in participants with and without BPD and to explore subjective perceptions of complex trauma. The presence of complex trauma was more in the BPD group as compared to the non-BPD group. However, the two groups did not differ in mentalizing ability. These findings partially support the first hypothesis. It is of prime importance to plan prevention and early intervention for youth at risk for BPD. Mentalizing ability was better in participants with CSA as compared to those without. This finding does not support the second hypothesis. This indicates the possible strengths of the automatic, rapid mentalizing that people with complex trauma have been found to possess. The qualitative themes have given important contextual information by laying out where trauma comes from in the form of intergenerational transmission and where it goes in terms of PTG and improvement of symptoms after undergoing psychotherapy.
Footnotes
Acknowledgements
The authors wish to thank all the participants who gave their time to take part in the research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethics Approval
Ethics approval was provided by Kasturba Hospital, Institutional Ethics Committee (IEC: 782/2021) (CTRI/2022/02/040569).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.