
Abstract
Background:
Adolescent boys with addictive behaviours often have comorbidities. India has scarce free short-term rehabilitation facilities for them. The Ministry of Social Justice funds one centre per state. In our centre in Kerala state, a low budget allowed full-time treatment staff of two counsellors and two nurses only. A yoga therapist, a clinical psychologist, and a psychiatrist visit part-time. This study aimed to develop a comprehensive care model within such staff constraints.
Methods:
We collected screening and assessment tools from child psychiatry clinics and through a literature search. We chose activities and worksheets from adolescent-specific workbooks on therapeutic (e.g., motivational enhancement, mindfulness) and positive psychology (e.g., managing emotions or relations) techniques. The psychiatrist trained the counsellors in their application.
Results:
We utilised pre-available Malayalam (the local vernacular) versions of the Alcohol, Smoking, and Substance Involvement Screening Test and Strengths and Difficulties Questionnaire. We translated and content-validated DBD Rating Scale, Teen Addiction Severity Index, and Adolescent Smoking Consequences Questionnaire. From 11 workbooks, we chose 123 activities, considering patient needs and cultural relevance, and translated 17 worksheets. Counsellors found the CBT Toolbox for Children and Adolescents the most useful workbook. Of the 49 inpatients from the past year, 41 had dual diagnoses, the commonest being conduct-dissocial disorder. Chart review revealed that 46 patients found the activities comprehensible and acceptable. Frequent staff change was a challenge.
Conclusions:
We developed an adaptive, low-cost, feasible, and acceptable care model for addictive behaviours and common comorbidities. Its acceptability and effectiveness need to be evaluated in larger, more diverse samples.
We developed a structured, low-cost, adaptive care model for addictive behaviours and dual diagnoses in adolescent boys. It included translating and modifying appropriate assessment tools; choosing, modifying, and using activities from workbooks on therapeutic techniques and skill-building; and training the counsellors in the use of the above. The model was found feasible and acceptable.Key Messages:
Addictive behaviours in adolescents are a major public health problem in India. The National Survey on Extent and Pattern of Substance Use in India found that, among those aged 10–17, the current prevalence rates for the use of opioids, alcohol, inhalants, and cannabis were 1.8%, 1.3%, 1.17%, and 0.9%, respectively. 1 According to systematic reviews, the prevalences of alcohol consumption at least once in the past year, 2 and moderate problematic internet use 3 were 10.6%–32.9% and 21.5%, respectively. In the state of Kerala, among those seeking alcoholism treatment in a tertiary care centre, while the mean age of onset of alcohol use was 24 in those born before 1950, it declined to 17 in those born after 1985. 4 A study among adolescent school students of the state found the self-reported prevalence of ever use of tobacco and alcohol to be 7.4% and 5.6% in the current academic year. 5
Adolescents with addictive behaviours often have comorbidities: according to a systematic review, the mean prevalence of dual diagnoses in substance-using children and adolescents was 59.6%, with the most common co-morbid disorder being conduct disorder (CD). 6 However, India has scarce free short-term rehabilitation facilities for adolescents with addictive behaviours. The Ministry of Social Justice and Empowerment, through its National Action Plan for Drug Demand Reduction (NAPDDR), funds one centre for adolescent boys in each state. 7 In our centre in Kerala, due to budget constraints, the full-time treatment staff included only two counsellors (with a postgraduate degree in social work) and two nurses. A psychiatrist (semiweekly visits), a clinical psychologist (weekly visits), and a yoga therapist (thrice weekly visits) work part-time. No existing literature discusses how comprehensive care can be provided with such limited staff.
This study aimed to develop a care model for addictive behaviours and comorbidities within these staff constraints and to assess its feasibility and acceptability. The model comprises economical, effective, and culturally appropriate tools for clinical evaluation and group psychosocial interventions. This article reports the methods used to finalise and validate suitable tools for these two components and reports the model’s acceptability in a pilot sample.
Methods
Ethical Aspects
The study received approval from the Institutional Ethics Committee (IEC) of St. Thomas College of Nursing, Chethipuzha (No: STCON-STH/IEC/01/2025 dated 7th March 2025). The IEC waived the need for parental consent and patient assent because the assessment of the activities’ comprehensibility and acceptability and the qualitative observations were based on retrospective chart review.
Assessment Tools
We contacted various child psychiatry clinics in the state and searched online for the names of important screening and assessment tools and their Malayalam (the local vernacular) versions. Some scales that we found appropriate had not been translated before. With permission from the respective authors, we translated them to Malayalam, with minor modifications to make some items culturally appropriate and comprehensible. To assess the content validity of the translated versions, ratings and comments were obtained from two experts each on five domains (Clarity and readability, Conceptual and semantic equivalence, Cultural appropriateness, Consistency and formatting, and Overall usability), using a checklist we developed for the purpose. Another expert ratified the content validity of this checklist (Supplementary File 1).
Therapy Tools
Workbooks
A workbook has been found to make cognitive behavioural therapy (CBT) developmentally appropriate and engaging for young people (e.g., by helping to convert internal thoughts and feelings to a more concrete and objective state).8, 9 Due to their affordability and accessibility, we used some workbooks that feature effective therapeutic techniques for addictive behaviours and dual diagnoses. For example, motivational interviewing 10 and CBT 11 have been found beneficial in adolescent substance use. Likewise, cognitive interventions to increase self-control and problem-solving skills are effective in CD. 12
Self-confidence and psychosocial skills, when marked, improve the prognosis of substance use disorders (SUD) in adolescents. 13 Also, social skills deficits are associated with an increased risk of internet addiction in adolescents. 14 Hence, we also chose a few workbooks on skill- building and other positive psychology techniques.
Selecting the Books
The psychiatrist hand-picked adolescent- specific workbooks from online stores and publisher websites and by browsing through the ‘Related Books’ sections. Selection decisions were based on content previews, user reviews, and previous experience in using workbooks for adults with alcoholism.
Rating Their Usefulness
After using them for at least six months, the two counsellors rated each book on a scale of 1–10 on four domains (ease of use of the content, relevance of the content for your patients, engagement level of the material, and clarity of instructions and exercises) using a questionnaire we developed. The questionnaire was content validated by two experts (Supplementary File 2).
Choosing Worksheets
Worksheets, being interactive, require active participation from young people, contributing to them being perceived as engaging. Therapists have been using worksheets to explain content, make therapeutic progress, and engage young people. 8 From the workbooks, we chose appropriate activities and worksheets based on patient needs, ease of use, and cultural fit. Some worksheets were chosen from workbooks intended for adult patients, too.
Modifications
We modified many activities based on pilot sessions (e.g., when asked to describe healthier responses in example situations, the patients preferred to write verbatim what they would say rather than narrate the entire scenario) and patient feedback (e.g., in an activity to look at a situation from an outsider’s perspective, specific fellow patients were designated as the ‘outsider’ as that helped the understanding).
Conducting the Sessions
The therapy sessions were held five days a week, usually lasted about 30 minutes, and were conducted for the whole group of patients. Additional sessions were conducted for smaller groups of those with gaming disorder, attention- deficit hyperactivity disorder (ADHD), and oppositional defiant disorder (ODD) or conduct-dissocial disorder, 1–2 times a week, each lasting 20–45 minutes, depending on the nature of the activity. After the sessions, individual patients were allowed to discuss their doubts.
Treatment fidelity was not assessed because the workbooks do not dictate concrete instructions on conducting the activities. The counsellors followed a flexible approach that considered the age, social background, psychological sophistication, and diagnoses of the members of each group.
Bibliotherapy
Bibliotherapy has been effective in reducing methamphetamine use in school-going adolescents.
15
We provided the patients and parents with relevant Malayalam articles the psychiatrist authored (available at
Other Interventions
Solution-focused approach, found to reduce problematic internet use in middle school students, 16 was not covered in any workbook. The counsellors used the approach by asking the patients exception questions and, where relevant, miracle questions, 17 in an individual format.
As a component of narrative therapy, 18 we asked the patients to write a goodbye letter to the substance or online activity they have been overly engaging in. Very recently, we introduced the mentorship model. 19
We curated many Malayalam tools to remediate learning difficulties. These included lists of 2–5-letter words, sight words, and similar words; sentences of diverse lengths (Supplementary File 3); copy books that help write words and sentences of increasing lengths and complexities; magnetic boards and letters; flashcards with words; and audio stories. As the nurses had some spare time, they were assigned to train the needy patients with these tools.
To benefit patients still pursuing their studies, we provided textbooks and guides for various classes, allowed interested patients to watch free online educational videos, and arranged three books on higher education options. The nurses supervised these aspects, too.
The clinical psychologist tested the intelligence quotient (IQ) and performed structured therapies and family counselling for needy patients. A certified yoga therapist provided yoga training three days a week, one hour per session. The psychiatrist prescribed medications wherever necessary and assessed and augmented the patients’ understanding of the sessions during the rounds.
The centre was started in March 2021. Over the years, the care model has been adaptive by adding, removing, or substituting tools and activities based on their perceived usefulness and our increased understanding of patient profiles and needs.
Training
The psychiatrist trained the counsellors to use the tools and worksheets and conduct the sessions. This included explaining unfamiliar terms and the nuances of the activities, suggesting culturally appropriate modifications, clarifying doubts, and providing feedback after patient interviews. The training was an ongoing process, as we kept adding and removing tools and activities, and it took 15–45 minutes a week.
Quantitative Evaluation
A counsellor collected essential socio- demographic and clinical information (age, habitat, diagnoses) from the charts of patients admitted between 1st March 2024 and 28th February 2025. Charts of those discharged before the assessment was complete (i.e., within 7–10 days of admission) were excluded. Another counsellor cross-checked the collected information on age and habitat, while the psychiatrist cross-checked the diagnoses. Based on a review of the notes made by the psychiatrist during the rounds and the counsellors in their session notes, the psychiatrist and two counsellors rated all patients for the acceptability and comprehensibility of the activities. For acceptability, a rating of ‘excellent’ meant the patient had attended the activities enthusiastically, ‘sufficient’ meant mild reluctance or indifference, and ‘poor’ meant disinterest or resistance. Ratings of comprehensibility were based on how much the patient was able to describe the learnings during the psychiatrist’s rounds: ‘excellent’ if able to describe most of the learnings, ‘sufficient’ if able to describe at least the most important points, and ‘poor’ if able to describe none or little of the proceedings.
We also checked if we had noted adverse effects like excessive emotional reactions.
Qualitative Observations
To gauge whether the patients had absorbed the concepts and messages of the sessions, we reviewed the completed worksheets and activity notes to identify common responses to select representative activities.
Statistical Analysis
Descriptive analysis was done using Microsoft Excel.
Results
Assessment Tools
Selected Scales
We chose the available Malayalam versions of the following:
Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST): 20
It collects details about the extent and consequences of the use of various substances. We used the Malayalam version prepared by Jaisoorya et al. 21
Strengths and Difficulties Questionnaire (SDQ): 22
It provides self-reports about emotional, conduct, or peer problems, hyperactivity, and pro-sociality. We used the validated Malayalam version from Youth in Mind. 23
A checklist for learning disorders: 24
We used a Malayalam version that was being used by some centres.
We translated and validated the following:
Teen Addiction Severity Index (T-ASI): 25
It provides information on domains not covered by other tools, such as school, family, and mental health.
Adolescent Smoking Consequences Questionnaire (ASCQ): 26
The ASCQ helps assess the outcome expectancies of cigarette smoking. While translating, we modified many items to incorporate beedis and smokeless tobacco products that our patients commonly use (Supplementary File 4).
Parent/Teacher DBD (Disruptive Behaviour Disorders) Rating Scale (RS-DBD): 27
It provides DSM-IV diagnoses of ADHD, ODD, and CD (Supplementary File 5).
The Child Behaviour Checklist 28 was considered but excluded due to its cost and because most of our patients’ comorbidities were externalising disorders. The Brief Assessment of Recovery Capital 29 was considered but not used because many of the questions do not apply to adolescents and the tool is more relevant for follow-up visits.
Some Observations
Patients gave more honest information about their substance use through ASSIST than through clinical interviews. The scale was usually administered after about a week of inpatient stay; the number of types of substances used and their extent of use were, on most occasions, higher when collected using the scale than the information they provided during the intake assessment. Likewise, SDQ captured emotional issues that were otherwise not reported by the patient or family during routine history taking—subsequent interviews and observations based on the SDQ findings often confirmed the presence of emotional issues. T-ASI provided the details of factors that needed addressing in the family environment, a lot of change talk that was otherwise not elicited, and the insight that the patients perceive counselling for various domains as important. ASCQ helped identify and correct misconceptions about the use of tobacco products, suggested alternatives for the perceived benefits (e.g., many patients found the use of smoking and nicotine products to help make parties and hanging out with friends more enjoyable), and elicited change talk.
Therapy Tools
Workbooks and Worksheets Used
We chose 11 workbooks (Table 1) and 123 activities from them (the patients stay up to 90 days, and a few are readmitted; Supplementary File 6). We also chose and translated seven worksheets on addiction and 10 on gaming.
Details of the Workbooks Used.
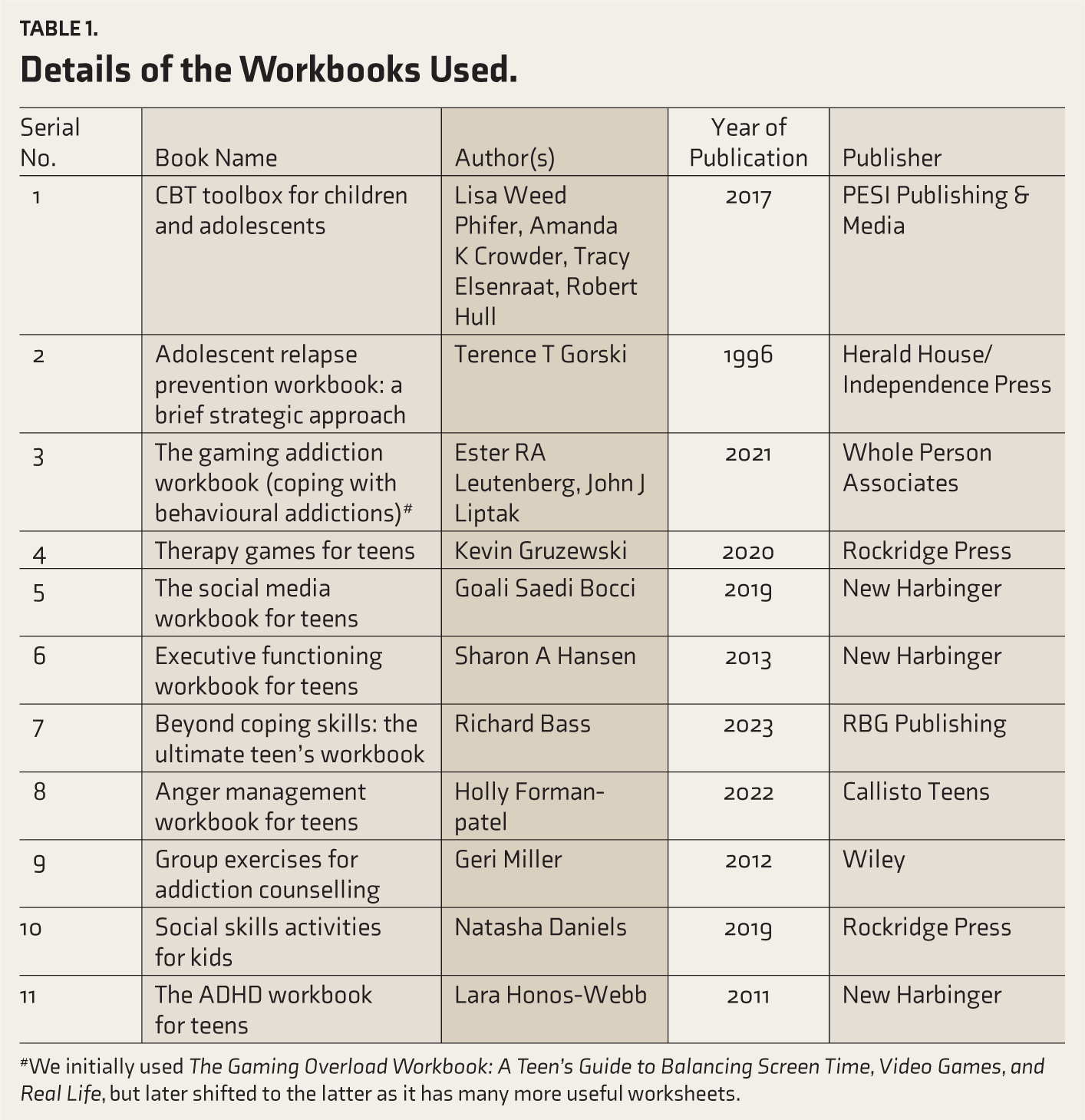
#We initially used The Gaming Overload Workbook: A Teen’s Guide to Balancing Screen Time, Video Games, and Real Life, but later shifted to the latter as it has many more useful worksheets.
Most Useful Workbooks
Of the 11 books, the counsellors gave the CBT Toolbox for Children and Adolescents the highest average score (37.5 out of a maximum of 40). 30 Group Exercises for Addiction Counselling and Anger Management Workbook for Teens got the second (33.5) and third (32) highest scores.31, 32
Evaluations of Responses to the Activities
Demographics and Diagnoses
During the study period, three patients were discharged before the assessment was complete, for various reasons, and their charts were excluded from the analysis. We reviewed the charts of the remaining 49 patients. Their age ranged from 12 to 17 (median = 15, IQR = 2). Most (n = 41) were from villages, and six were from towns.
The most common clinical diagnoses of addictive behaviours according to ICD-11 were harmful pattern of use of nicotine (n = 27), nicotine dependence (n = 15), harmful pattern of use of cannabis (n = 13), harmful pattern of use of alcohol (n = 11), and gaming disorder (n = 11). While four patients had a diagnosis of a harmful pattern of use of volatile inhalants, one each had cannabis dependence and sedative, hypnotic, or anxiolytic dependence.
Forty-one patients had dual diagnoses. The commonest were conduct-dissocial disorder (n = 22), ADHD (n = 14), and ODD (n = 11). Developmental learning disorder and disorder of intellectual development were seen in eight and five patients, respectively.
Acceptability and Comprehensibility
Based on our notes, we rated all except three patients ‘excellent’ for the comprehensibility and acceptability of the sessions. The remaining three had either intellectual development disorder or developmental learning disorder (Table 2).
No adverse effects were recorded in patients during or after the sessions.
Dual Diagnoses in the Three Patients Rated Less Than ‘Excellent’ for Comprehensibility or Acceptability of the Sessions.
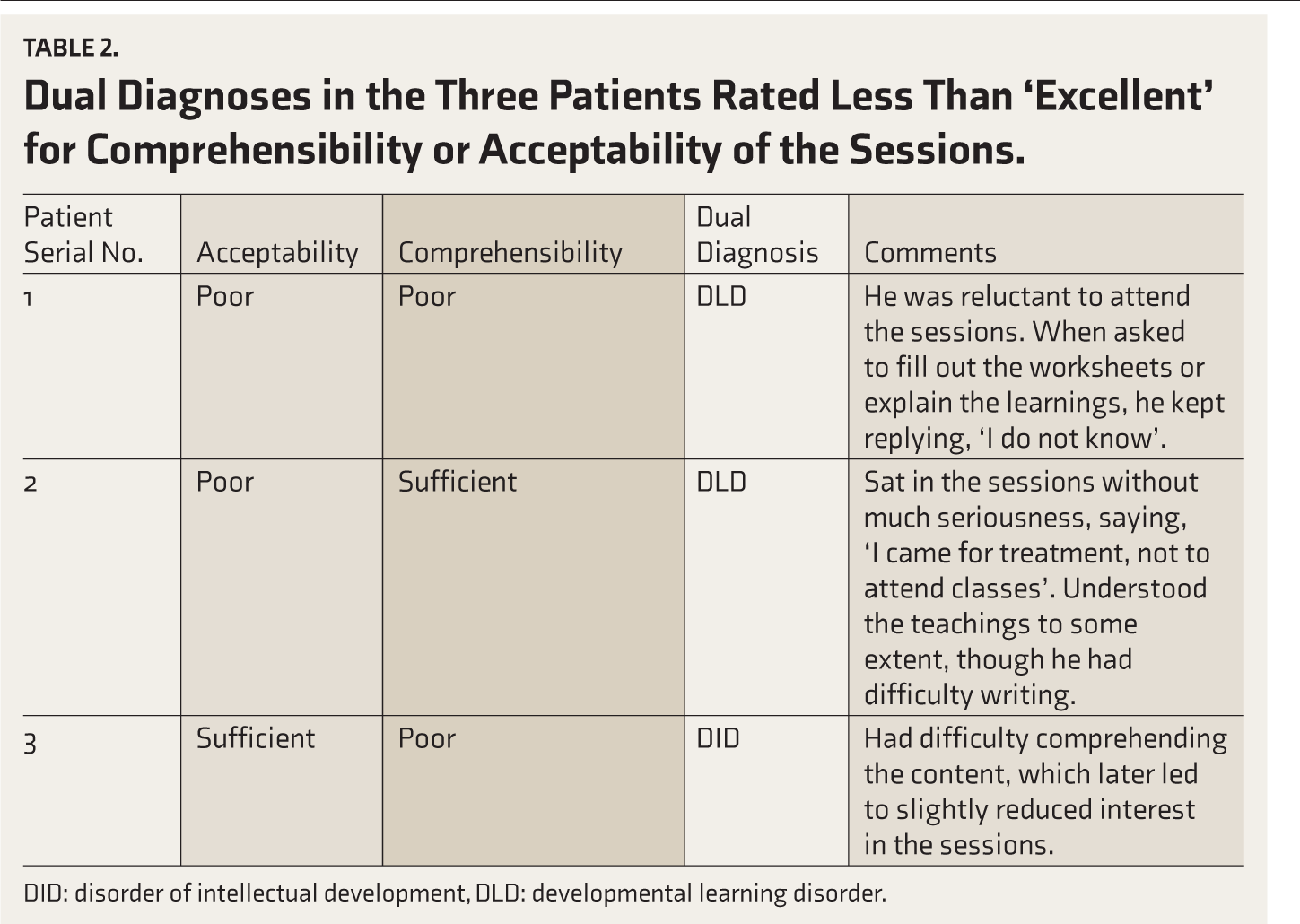
DID: disorder of intellectual development, DLD: developmental learning disorder.
Qualitative Observations
In response to exception questions, common responses from those with gaming disorder were that they managed the cravings by engaging in offline games like football or arts and crafts activities like drawing. Those with substance use utilised alternate activities such as watching movies, reading newspapers, and walking around with friends.
Though we initially asked only those in the conduct/ODD group to write a gratitude letter to an appropriate person, later, as we found the participants interested in the activity and the content of the letters insightful, we extended the activity to all patients. Most letters were addressed to their parents, especially the mother, or friends. The common reasons the patients thanked their mothers were for looking after them, buying them the things they wanted, and caring for them despite all their ‘bad’ behaviours. Some patients living in childcare institutions thanked their caretakers for empathetically listening to the problems they shared.
Common themes in the goodbye letters were (a) they started the use due to peer influences and (b) a major motive for quitting smoking was the resultant cough and dyspnoea.
Challenges Faced
Many counsellors and nurses left the centre for greener pastures after working for about a year, and the training had to be repeated for the recruits. The impact is lessened because only one of the two staff members leaves at a time; the recruits get to watch the remaining experienced staff administering the tools, conducting the sessions and clarify doubts. The challenge is also partly overcome by having the old and new staff work together for about two weeks. Better salaries and infrastructure might help retain the staff for longer periods. A few counsellors had difficulty understanding some portions of the workbooks due to deficient knowledge of English. The psychiatrist and fellow staff helped them overcome this obstacle.
Discussion
We found that using available and translated screening and assessment scales and carefully chosen and adapted activities from workbooks and worksheets-based exercises and training the counsellors in their use were feasible. The activities were comprehensible and acceptable to patients with no intellectual development disorder or developmental learning disorder.
Models such as task-sharing approaches, collaborative stepped care, and integration of care into alternative platforms have been suggested to be appropriate for Low- and Middle- Income Countries (LMICs). 33 Task shifting means shifting tasks from highly trained to less trained individuals to use available resources efficiently. 34 A systematic review found that task-sharing approaches may increase the reach and effectiveness of mental health care in low-resource settings. 35
Examples of interventions successfully used in low-resource settings for addiction treatment include the use of peer-based recovery coaching and a recovery support network, 36 providing telepsychiatry-based training on the management of tobacco addiction to a primary care doctor, 37 and the use of individuals with lived substance use experience to improve retention to methadone treatment in opioid use disorders. 38 Indian research has demonstrated the usefulness of lay counsellors (those without a professional qualification in mental health care) in managing addictions. A randomised controlled trial demonstrated that a brief intervention provided by lay counsellors improved remission and abstinence over three months among adult males with harmful drinking; the improvement was enhanced at 12 months.39–41 We also used task shifting to staff who are not mental health professionals (as per the Mental Healthcare Act 2017). Patients who benefited from our model may be used in the community and other settings as peer mentors in peer-based recovery coaching or to motivate newly recovering patients to remain in treatment. No research had addressed the kind of setting or patient group we did.
The book our counsellors found the most useful, CBT Toolbox for Children and Adolescents, was listed in a compendium of child treatment resources. 42
Limitations
The RS-DBD is based on the DSM-IV; however, no such tool based on DSM-5 criteria is available. Though both DSM-IV and DSM-5 categorise CD symptoms under the same four major domains, the ODD criteria have been significantly updated.
Due to the lack of a trained family therapist, we could not do structured interventions such as family-focused therapy 43 or family-based therapies, 11 which are among the most effective interventions for SUD in adolescents. Also, many patients were from broken families or institutions, and they stayed in our centre alone, without their parents, who mostly lived in distant locations. Our family interventions were limited to 1–2 face-to-face family counselling sessions by the clinical psychologist and 5–6 face-to-face or over-the-phone sessions by the counsellors. Also, we could provide parent management training, one of the most effective interventions for DBDs, 44 to a limited extent only, mainly through an article on behavioural therapy techniques the psychiatrist wrote in the vernacular.
The model included components of some interventions, such as mindfulness 45 and solution-focused therapy, 46 that have sufficient evidence in adult populations but are understudied in adolescents.
We confirmed only the content validity as we made only a few minor modifications to the scales we translated. We did not perform a formal adaptation or establish reliability or other validities. No formal pilot testing was conducted. However, the counsellors administered the questionnaires with context-sensitive adaptations, considering individual patient characteristics while maintaining the core intent of each item. This approach aimed to enhance patient understanding without compromising the validity of the questions’ content. Translations of the worksheets were informal and formal validation is pending.
The qualitative observations are anecdotal and not systematic. Besides, our sample is small, and most patients were from villages. This sample may not truly represent the broader adolescent population in Kerala. Another limitation is that, as most patients are from faraway places, we insist on coming to us only for the first follow-up; after that, they are referred to appropriate nearby hospitals. Hence, direct assessment of long-term outcomes will be difficult.
Implications
The model can be adapted for other low- resource settings, especially the NAPDDR- funded centres in other states and similar centres in other LMICs, with culturally appropriate modifications and translations. Besides, policymakers could use this model to scale up services under initiatives like NAPDDR. The materials we translated can be used for Malayalam-speaking patients in any setting.
Future Directions
Regular updating of the model based on future patient profiles and feedback and emerging research.
Community-based participatory research involving parents, teachers, community leaders, etc., to further refine the model.
Training community health workers on these assessment tools and interventions so that more patients can be reached.
Assessing feasibility and acceptability, after appropriate modifications, in other low-resource settings, especially those with larger and more diverse samples.
Assessing the short- and long-term effectiveness on both addictive and disruptive behaviours.
To improve generalizability, the last two can be done in multi-centre studies across urban and rural Kerala or in collaboration with other NAPDDR-funded centres in other states.
Conclusions
A structured, low-cost, adaptive care model for addictive behaviours and dual diagnoses in adolescent boys was developed and found feasible and acceptable. If effectiveness studies find it to be beneficial, the model can be used, with appropriate modifications, for low-cost adolescent addiction care in other NAPDDR-funded and low-resource settings.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
We acknowledge the following experts for content-validating the tools we translated: Drs Sandeep Grover (Post Graduate Institute of Medical Education & Research, Chandigarh), Vikas Menon (Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry), Varsha Vidyadharan (Government Medical College, Kozhikode), Rachna George (Christian Medical College, Vellore), Vidhukumar K (Government Medical College, Alappuzha), Sheena G Soman, Arun Ayyappan (Government Mental Health Centre, Thiruvananthapuram) Ganga Kailas (Consultant Psychologist in private practice, Alappuzha), Sreejayan K (Northern Health, Melbourne, Australia), Anju Mathew (Government Medical College, Thiruvananthapuram), and Immanuel Thomas (Previously at University of Kerala, Thiruvananthapuram).
We thank Fr. Jince Chorattu Chamakala and Mr TM Mathew of Changanacherry Social Service Society for their help in implementing the model.
Data Availability Statement
The data will be available from the first author on email requests.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
Inputs from ChatGPT were used in developing the online-only supplementary files 1 and 2. Both the tools were subsequently content-validated by experts. The authors assume full responsibility for their contents.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
A waiver for parental consent and patient assent was obtained from the IEC because the assessments were based on retrospective chart review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.