
Abstract
Background:
Parenting styles shape behavioral outcomes in children with autism spectrum disorder (ASD), yet their influence in low-resource settings, such as India, remains underexplored. This study investigates how parenting styles (authoritative, authoritarian, and permissive) correlate with behavioral outcomes in children with ASD in India, and examines demographic influences
Methods:
A cross-sectional study was conducted with 82 parents of children with ASD (aged 3–17 years) at a tertiary care hospital. Parenting styles (authoritative, authoritarian, and permissive) were assessed using the Parenting Styles and Dimensions Questionnaire (PSDQ), and behavioral problems were measured with the Strengths and Difficulties Questionnaire (SDQ). Descriptive statistics, Pearson correlation, analysis of variance (ANOVA), and t-tests were applied.
Results:
Authoritative parenting predominated (mean score: 57.33 ± 9.55), linked to fewer behavioral challenges, while authoritarian (r = 0.37, p < .001) and permissive (r = 0.34, p = .002) styles were associated with increased difficulties, notably hyperactivity (6.66 ± 1.67) and peer problems (5.09 ± 1.83). Higher parental education favored authoritative practices (p = .007), whereas prolonged treatment duration worsened behaviors (p = .003).
Conclusion:
Authoritative parenting mitigates behavioral challenges in children with ASD, unlike authoritarian and permissive styles, which exacerbate difficulties. These findings underscore the need for culturally tailored interventions such as workshops addressing stigma, resource scarcity, and language barriers to promote adaptive caregiving in India. Policymakers should integrate parental education into ASD care to enhance family well-being.
Keywords
Authoritative parenting reduces behavioral challenges in children with ASD, unlike authoritarian and permissive styles, which exacerbate difficulties. Cultural norms and parental education significantly influence parenting practices in India, with higher education linked to adaptive styles. Culturally tailored interventions are essential to support ASD families in India, addressing behavioral issues and caregiving burdens.Key Messages:
Autism spectrum disorder (ASD), a neurodevelopmental condition characterized by deficits in social communication and restricted/repetitive behaviors, affects approximately 1%–2% of children globally, with rising prevalence in low- and middle-income countries (LMICs) such as India.¹ While Western studies consistently link authoritative parenting styles, marked by warmth and structured guidance, to improved behavioral outcomes in children with ASD, cultural nuances in LMICs such as India, where authoritarian practices often dominate due to societal norms and resource limitations, necessitate region-specific investigations. 2 For instance, studies from Indonesia and Malaysia reveal that authoritarian parenting remains prevalent among families of children with ASD, reflecting collectivist cultural values that prioritize obedience over open communication.3–5 This disparity underscores a critical gap in understanding how culturally ingrained parenting practices influence ASD-related behavioral challenges in settings such as India, where stigma, diagnostic delays, and limited access to evidence-based interventions exacerbate familial burdens. 5
This study is anchored in Roy’s Adaptation Model (RAM), which posits that individuals respond to environmental stimuli through adaptive or maladaptive behaviors. 6 In this framework, parenting styles act as contextual stimuli shaping behavioral outcomes in children with ASD 6 . The model identifies three types of stimuli: Focal stimuli (e.g., the child’s ASD diagnosis), contextual stimuli (e.g., parenting practices and socioeconomic factors), and residual stimuli (e.g., cultural norms and access to healthcare). 6 According to RAM, adaptive responses (e.g., authoritative parenting) foster prosocial behaviors and emotional regulation, while maladaptive responses (e.g., authoritarian or permissive styles) may exacerbate hyperactivity and peer interaction difficulties. 6 This theoretical lens provides a robust framework for evaluating parenting dynamics in resource-constrained environments. 6
Recent studies from LMICs highlight the urgency of addressing these dynamics. A 2023 Malaysian trial found that authoritarian parenting correlated with heightened emotional dysregulation in children with ASD, 7 while a 2024 Brazilian study emphasized socioeconomic barriers limiting access to parenting training programs. 8 In India, where ASD prevalence is estimated at 1 in 61 children, 9 systemic challenges such as parental illiteracy and inadequate community support further complicate caregiving. 10 Societal stigma and delayed diagnosis often intensify caregiving challenges, shaping parenting practices in unique ways. 10 These findings align with global calls for culturally tailored interventions that align parenting strategies with regional realities. 11
This study investigates the relationship between parenting styles and behavioral outcomes in children with ASD in India. It investigates three research inquiries: What are the primary parenting approaches utilized by parents of children with ASD in Bangalore, India? How do these types connect to behavioral consequences, including hyperactivity and peer issues? What demographic factors, including parental education, affect these relationships? Informed by RAM, the study anticipates that authoritative parenting will correlate with a reduction in behavioral difficulties. This research aims to contextualize worldwide findings within India’s sociocultural framework, offering practical insights for clinical treatment and policy formulation.
Understanding how different parenting styles influence behavioral outcomes can inform the development of culturally tailored interventions designed to promote adaptive parenting practices. Such interventions have the potential to alleviate caregiver stress, reduce behavioral challenges in children with ASD, and ultimately improve the quality of life for affected families.
Methods
Study Design and Participants
A descriptive cross-sectional research design was employed. Participants were selected using purposive sampling from the Child and Adolescent Psychiatry outpatient department (OPD) of a tertiary care hospital in India. Parents were purposively sampled from consecutive OPD visits to ensure diversity in socioeconomic status (e.g., income and education) and caregiving experience (e.g., duration of child’s treatment). 12 Eligible parents were identified by the child psychiatrist during routine appointments and invited to participate after confirming their child’s diagnostic and statistical manual of mental disorders (DSM)-5 ASD diagnosis. Inclusion criteria required parents (either mother or father) aged 25–50 years who had children diagnosed with ASD and were actively seeking treatment at the Child and Adolescent Psychiatry OPD. Exclusion criteria comprised parents with chronic medical (e.g., seizures, cardiac disorders, severe respiratory conditions) or psychiatric conditions that could affect parenting consistency, ensuring focus on ASD-specific caregiving dynamics. A consultant psychiatrist validated diagnoses of ASD. Children with documented comorbidities, such as developmental delay, intellectual disability, and Attention Deficit Hyperactivity Disorder (ADHD), were included. However, specific comorbidity data were not collected or analyzed separately. This decision was influenced by the study’s cross-sectional design and the emphasis on psychosocial factors, particularly parenting styles. Conducting separate analyses could have diminished statistical power due to the heterogeneity of comorbidities. Children undergoing pharmacological treatments (e.g., antipsychotics and stimulants) or therapies (e.g., occupational and speech therapy) were included in the study; however, specific information regarding medication types, dosages, or therapy details was not gathered or analyzed separately. The cross-sectional design and application of RAM emphasized psychosocial factors rather than clinical interventions. Incorporating such data could have led to unmeasured confounding, diminished statistical power due to heterogeneity, or ecological fallacy by misaligning group-level intervention data with individual-level psychosocial outcomes (Parenting Styles and Dimensions Questionnaire [PSDQ], Strengths and Difficulties Questionnaire [SDQ]).
Instruments
Parenting styles were assessed using the PSDQ-Short Version, a validated 32-item tool divided into three domains: Authoritative (15 items), authoritarian (12 items), and permissive (5 items). 13 Subdomains included warmth/support, reasoning/induction, and democratic participation for authoritative parenting; physical coercion, verbal hostility, and punitive discipline for authoritarian parenting; and indulgence for permissive parenting. 13 Internal consistency for PSDQ subscales ranged from Cronbach’s a = 0.56 to 0.78 in this study, consistent with prior validations. 13 The lower Cronbach’s a (0.56) for some PSDQ subscales reflects challenges in cross-cultural adaptation, though still acceptable for exploratory research. 14
Behavioral problems in children were evaluated using the Strengths and Difficulties Questionnaire (SDQ), 15 a 25-item tool measuring emotional symptoms, conduct problems, hyperactivity/inattention, peer relationship problems, and prosocial behavior, with a total difficulty score ranging from 0 to 40 (higher scores indicate greater problems). The SDQ has demonstrated reliability in ASD populations (Cronbach’s a = 0.65). 16 Demographic and clinical characteristics, as presented in Table 1, were collected using a semi-structured proforma designed to capture variables such as parental age, income, and the child’s duration of illness.
Data Collection Procedure
Data collection occurred from 14 October to 11 November 2023. Baseline demographic data were collected using a semi-structured proforma. The PSDQ and SDQ were administered through face-to-face interviews conducted in a private setting to ensure confidentiality and to minimize social desirability bias. 17 Interviews were conducted by a nurse trained as a research assistant to ensure consistency, with tools administered in English. Each interview lasted approximately 25–30 minutes.
Pilot Study
A pilot study was conducted from 5 to 10 October 2023, involving eight participants who met the inclusion criteria. The pilot confirmed the feasibility of the research design and tools, with no modifications required.
Sample Size Estimation
The sample size was calculated using G*Power 3.1.9.7 18 based on authoritarian parenting scores (µ = 2.21, v = 0.51) from Thanapalan et al. (2021). 19 With a 5% margin of error (E = 0.05), 95% confidence (Z = 1.96), and anticipated effect size (Cohen’s d = 0.5), a minimum of 82 participants was required to achieve 80% power. 18 The formula n = Z².v²/E² ensured methodological rigor, accounting for potential attrition in low-resource settings.
Statistical Analysis
Data were analyzed using R programming software. 20 Descriptive statistics (mean, standard deviation, and frequency distributions) were used to summarize baseline variables, parenting styles, and behavioral problem scores. Inferential statistics included Pearson’s correlation to examine relationships between parenting styles and behavioral problems, while t-tests and one-way analysis of variance (ANOVA) assessed associations with demographic variables. 20 Statistical significance was set at p < .05. This robust methodology ensures that findings are both reliable and generalizable within similar clinical contexts while addressing critical gaps in understanding parenting dynamics in ASD populations in low-resource settings such as India.
Ethical Considerations
Ethical clearance was obtained from the Institute Ethics Committee, and informed consent was obtained from parents. Subjects were allowed to withdraw from the study at any point without affecting their routine clinical care. To ensure confidentiality and anonymity, no identifying information was collected. This study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for reporting observational research.
Results
The study analyzed data from 82 parents of children with ASD to assess parenting styles and their correlation with behavioral problems in children. The findings are organized into key sections to provide a comprehensive understanding of the results.
Baseline Demographic Characteristics
The study included 82 parents of children with ASD, with a mean age of 36.96 ± 5.68 years. The majority (71.95%) were mothers, reflecting the predominant role of female caregivers in ASD caregiving. Most parents were married (98.78%), employed (53.66%), and had postgraduate education (55%), highlighting a cohort with relatively high socioeconomic and educational attainment. Household income distribution was skewed toward higher brackets, with 57.32% earning ≥₹249,044 annually. Family dynamics revealed that 52.44% had two children, while only 1.22% reported another child with ASD, underscoring the sporadic familial prevalence of the condition. Notably, 96.34% had no family history of ASD, and 98.78% received familial support, suggesting robust caregiving networks. These demographics contextualize the study’s findings within an urban Indian population characterized by educated, middle-income families actively engaged in ASD management (Table 1).
Demographic and Clinical Characteristics of Parents and Children (N = 82).
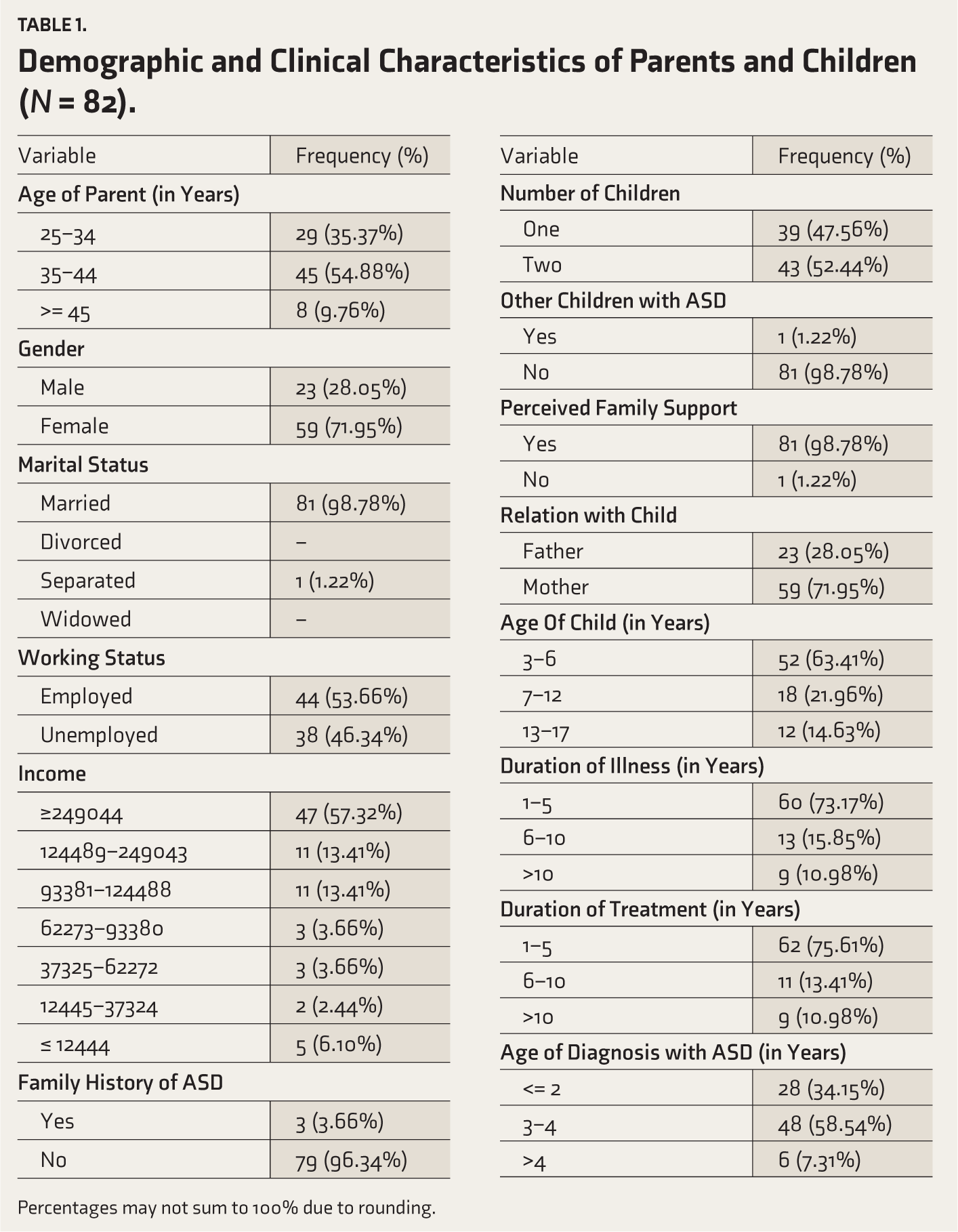
Percentages may not sum to 100% due to rounding.
Parenting Styles Among Parents of Children with ASD
The study revealed that authoritative parenting was the predominant style among parents of children with ASD, with a mean score of 57.33 ± 9.55, representing 76.4% of the maximum possible score. Subdomain analysis highlighted warmth and support (21.16 ± 2.91) as the most prominent aspect of this style. In contrast, authoritarian parenting (22.62 ± 6.83) and permissive parenting (10.99 ± 3.75) were less prevalent, accounting for 37.7% and 43.9% of their respective maximum scores. Authoritarian practices were characterized by elevated verbal hostility (8.0 ± 2.82), reflecting stricter disciplinary approaches (Table 2).
Distribution of Parenting Styles (PSDQ) and Children’s Behavioral Problems (SDQ).
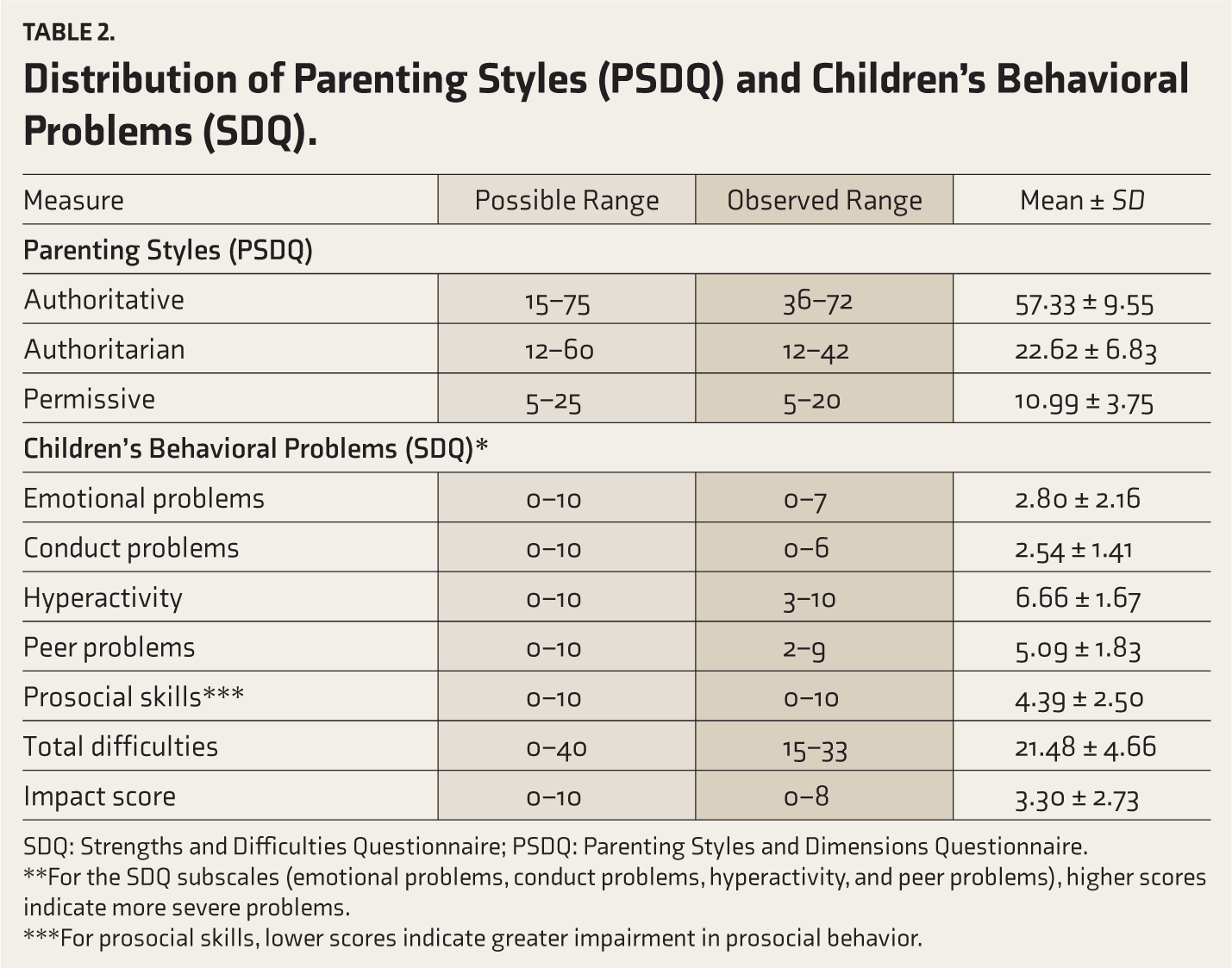
SDQ: Strengths and Difficulties Questionnaire; PSDQ: Parenting Styles and Dimensions Questionnaire.
**For the SDQ subscales (emotional problems, conduct problems, hyperactivity, and peer problems), higher scores indicate more severe problems.
***For prosocial skills, lower scores indicate greater impairment in prosocial behavior.
Behavioral Problems in Children with ASD
Children with ASD exhibited significant behavioral challenges, with a total difficulty score of 21.48 ± 4.66 on the SDQ. The most pronounced issues were hyperactivity (6.66 ± 1.67) and peer interaction difficulties (5.09 ± 1.83). Emotional problems (2.8 ± 2.16) and conduct problems (2.54 ± 1.41) were comparatively less severe. Notably, prosocial behaviors (4.39 ± 2.5) were relatively preserved, suggesting children with ASD retain some capacity for positive social interactions. The SDQ impact score (3.3 ± 2.73) underscored the substantial burden these behavioral difficulties place on family functioning (Table 2).
Correlation Between Parenting Styles and Behavioral Problems
As shown in Table 3, a statistically significant positive correlation was observed between authoritarian parenting and behavioral problems (r = 0.37, p < .001), as well as between permissive parenting and behavioral challenges (r = 0.34, p = .002). Conversely, authoritative parenting showed no significant association with behavioral issues (r = 0.21, p = .051), suggesting its potential role in mitigating maladaptive outcomes. These correlations align with RAM, where parenting styles shape adaptive or maladaptive behavioral responses to ASD. Additionally, this also aligns with global findings linking rigid or lenient parenting styles to heightened emotional dysregulation and externalizing behaviors in children with ASD.
Correlation Between Parenting Styles and Children’s Total Behavioral Difficulties (N = 82).
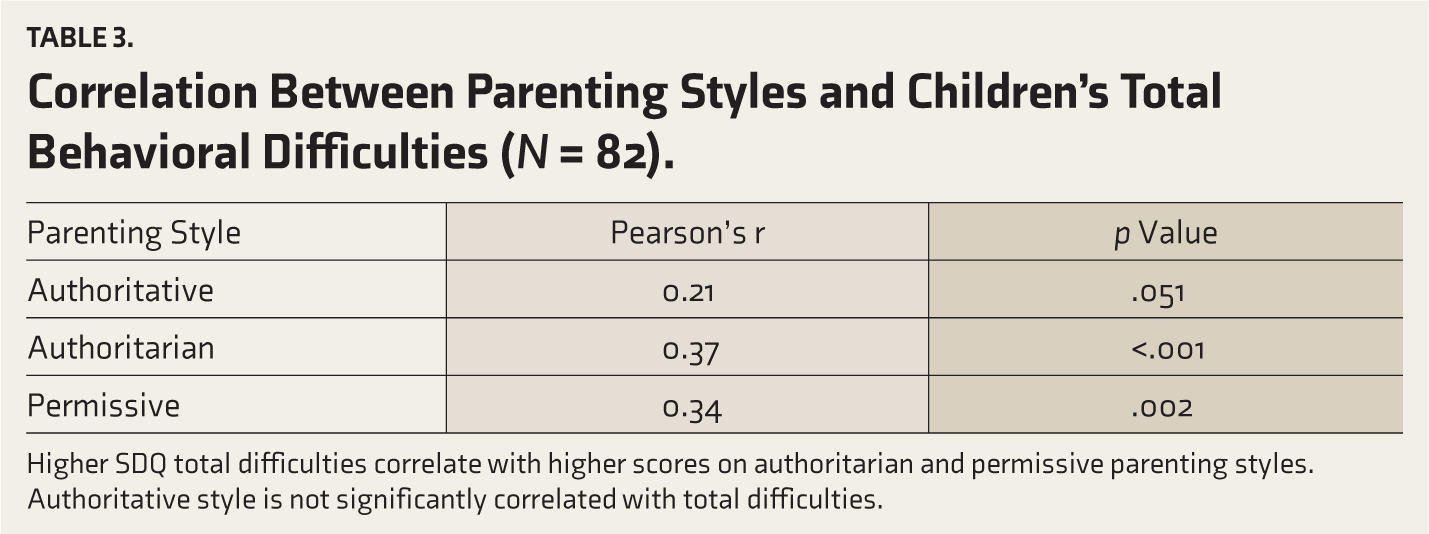
Higher SDQ total difficulties correlate with higher scores on authoritarian and permissive parenting styles. Authoritative style is not significantly correlated with total difficulties.
Association of Parenting Styles with Baseline Variables
Higher parental education levels were significantly associated with authoritative parenting (F = 3.78, p = .007), emphasizing the role of education in fostering adaptive caregiving practices. Families with more than one child were more likely to exhibit permissive parenting (F = −2.52, p = .01), potentially reflecting challenges in managing multiple caregiving responsibilities (Table 4).
Association of Parenting Styles (PSDQ) With Selected Parent Baseline Variables.
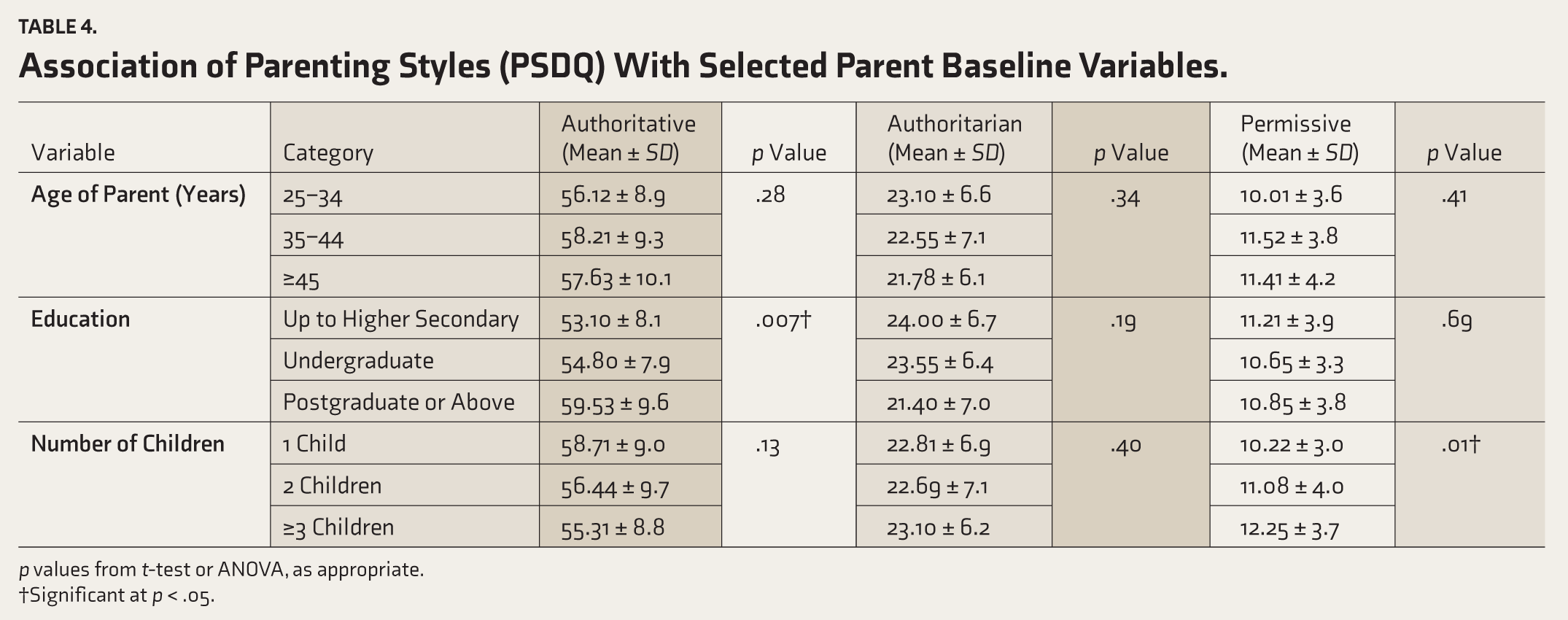
p values from t-test or ANOVA, as appropriate.
†Significant at p < .05.
Association of Behavioral Problems with Baseline Variables
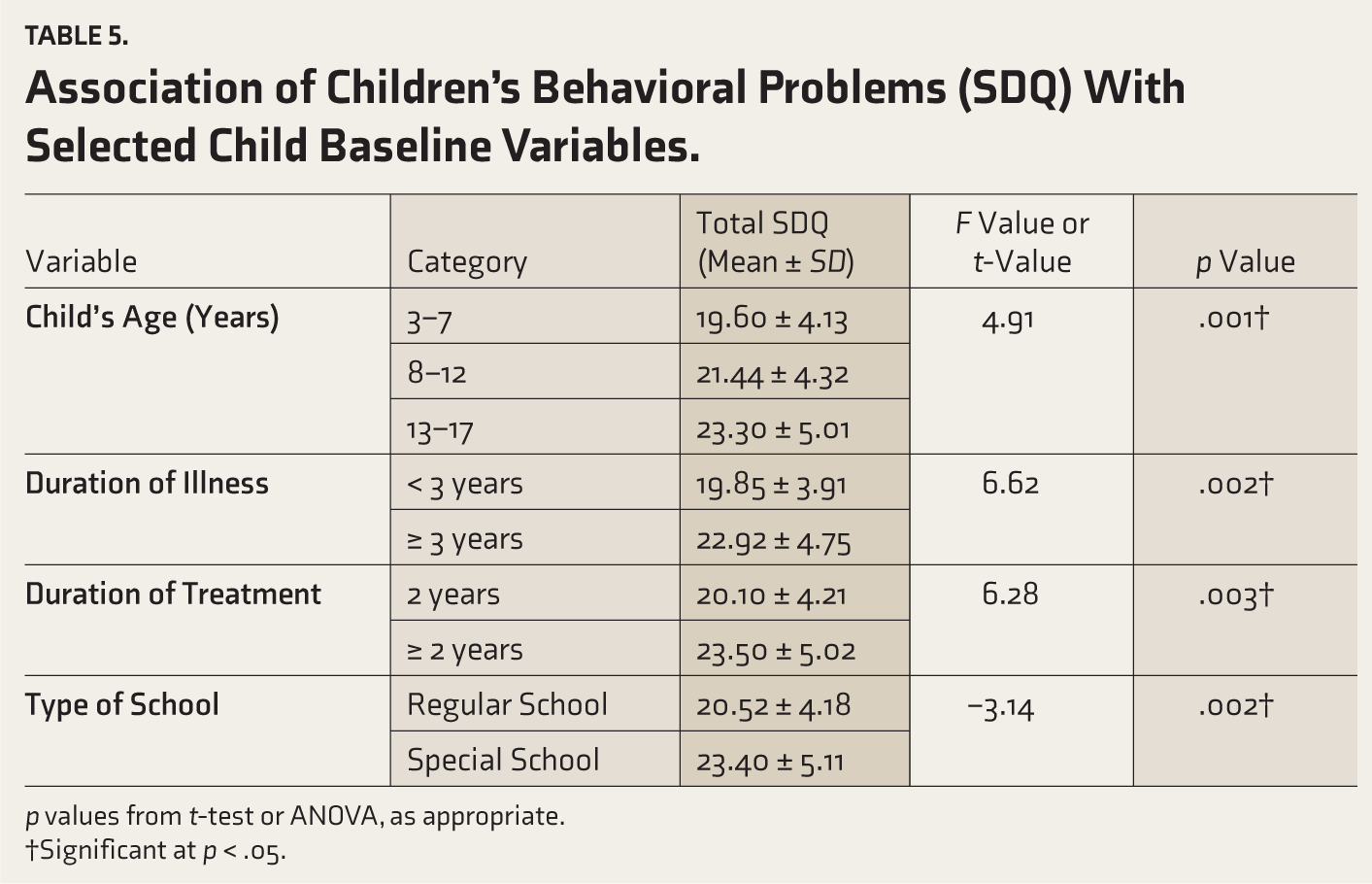
The study revealed significant associations between behavioral challenges in children with ASD and developmental or clinical factors. Older children exhibited more severe behavioral issues (F = 4.91, p = .01), while prolonged duration of illness (F = 6.62, p = .002) and extended treatment duration (F = 6.28, p = .003) were strongly correlated with heightened difficulties. Notably, children attending special schools faced greater behavioral challenges compared to those in regular educational settings (F = −3.14, p = .002), underscoring the need for inclusive strategies to support social integration (Table 5).
Association of Children’s Behavioral Problems (SDQ) With Selected Child Baseline Variables.
p values from t-test or ANOVA, as appropriate.
†Significant at p < .05.
Discussion
The findings of this study provide significant insights into the relationship between parenting styles and behavioral problems in children with ASD, particularly within the sociocultural context of India. By examining authoritative, authoritarian, and permissive parenting styles and their impact on behavioral domains such as hyperactivity, peer problems, emotional regulation, and prosocial behavior, this study contributes to a deeper understanding of caregiving dynamics in families with children with ASD.
Theoretical Implications
Within RAM, authoritative parenting serves as a contextual stimulus, promoting adaptive behavioral responses in children with ASD, such as reduced hyperactivity and improved peer interactions, by fostering emotional regulation and structured support (r = −0.29, p < .01). This aligns with RAM’s emphasis on adaptive coping mechanisms. Conversely, authoritarian parenting, associated with increased behavioral difficulties (r = 0.37, p < .001), reflects maladaptive responses to the focal stimulus of ASD, exacerbating challenges such as conduct problems due to rigid control. 6 In India’s sociocultural context, where collectivist values shape parenting (residual stimuli), authoritative styles may better balance warmth and discipline, enhancing adaptation. At the same time, authoritarian approaches may heighten stress, particularly in urban, educated families navigating ASD-related demands.
Parenting Styles in Context
The predominance of the authoritative parenting style among parents in this study (mean score: 57.33 ± 9.55) aligns with global research demonstrating its association with better developmental and behavioral outcomes. Studies conducted in Malaysia and the United States have similarly reported that authoritative parenting is the most common approach among parents of children with developmental disabilities, including ASD.4,21 For instance, a Malaysian study using the PSDQ found that authoritative parenting scored highest (mean: 3.89 ± 0.43). This parenting style, characterized by warmth, responsiveness, and structured guidance, is widely recognized for fostering adaptive behaviors and emotional regulation in children. 4
However, a subset of parents in this study exhibited authoritarian tendencies (mean score: 22.62 ± 6.83), particularly in terms of verbal hostility (mean: 8 ± 2.82). These findings are consistent with studies from Indonesia and Saudi Arabia, where cultural norms often favor controlling parenting approaches.22,23 Despite the benefits of authoritative parenting, its relatively lower prevalence compared to Western contexts may stem from cultural norms favoring hierarchical family structures and societal stigma surrounding neurodevelopmental disorders in India. Despite its benefits, the adoption of authoritative parenting in India may be hindered by limited access to training and cultural preferences for obedience-focused discipline. 24 While authoritative parenting predominated in this educated urban sample, broader Indian norms favoring authoritarianism suggest selection bias or evolving practices among informed caregivers. Indian parents often face pressure to prioritize obedience over open communication, particularly in communities where authoritarianism is culturally ingrained. 25 Subdomain analysis for authoritative parenting showed the highest scores in warmth and support (mean: 21.16 ± 2.91), while authoritarian parenting was characterized by elevated verbal hostility (mean: 8 ± 2.82). These findings indicate that most parents leaned toward a structured yet nurturing approach, although some exhibited controlling or lenient tendencies. Authoritarian practices may reflect heightened parental stress or frustration stemming from caregiving demands in resource-limited settings such as India. Similarly, permissive parenting (mean score: 10.99 ± 3.75) was observed among some parents, potentially arising from feelings of helplessness or overcompensation for their child’s difficulties. These findings underscore the influence of cultural and socioeconomic factors on parenting behaviors.
This study also highlights the role of parental education in shaping parenting styles. Higher parental education levels were significantly associated with authoritative parenting (F = 3.78, p = .007), consistent with findings from cross-cultural studies conducted in Thailand and Indonesia.26,27 Educated parents may be better equipped to implement structured yet empathetic approaches that mitigate stressors associated with caregiving for a child with ASD.
Behavioral Problems in Children with ASD
Children with ASD in this study exhibited significant behavioral challenges, particularly in the domains of hyperactivity (mean: 6.66 ± 1.67) and peer interaction difficulties (mean: 5.09 ± 1.83). These results are consistent with prior research conducted in the United Kingdom, where children with ASD scored higher on hyperactivity (mean: 7.6 ± 2.35) and peer problems (mean: 5.44 ± 1.99) compared to neurotypical peers. 28 Hyperactivity can disrupt participation in structured activities, while peer interaction difficulties highlight deficits in social communication, a hallmark feature of ASD.
Interestingly, prosocial behaviors were relatively preserved (mean score: 4.39 ± 2.5), suggesting that children with ASD retain some capacity for positive social interactions when appropriately supported. This finding aligns with studies from Brazil and China that emphasize the role of supportive parenting in fostering prosocial behaviors among children with developmental disabilities.29,30
The moderate SDQ impact score (mean: 3.3 ± 2.7) underscores the day-to-day challenges that families face. This aligns with prior studies, which highlight that even milder symptom burdens can meaningfully disrupt routines, indicating the need for tailored interventions that address both clinical symptoms and the practical demands of caregiving. 25
Correlation Between Parenting Styles and Behavioral Problems
The significant positive correlations between authoritarian (r = 0.37, p < .001) and permissive (r = 0.34, p = .002) parenting styles and increased behavioral problems are consistent with findings from Malaysia and China, which reported similar associations between controlling or lenient parenting styles and heightened emotional dysregulation or externalizing behaviors in children with ASD.31,32
Conversely, no significant correlation was observed between authoritative parenting style and behavioral problems (r = 0.21, p = .051). This result supports the existing literature, which suggests that authoritative parenting may serve as a protective factor against maladaptive outcomes by fostering emotional regulation and adaptive behaviors through a balance of warmth and structure.19,25
Association Between Behavioral Problems and Baseline Variables
The study identified significant associations between behavioral challenges in children with ASD and key baseline variables. Older children exhibited more severe behavioral issues (F = 4.91, p = .01), likely due to escalating social and academic pressures exacerbating core ASD deficits such as communication difficulties and emotional dysregulation. Prolonged illness duration (F = 6.62, p = .002) correlated with heightened behavioral difficulties, aligning with the “wear-and-tear” hypothesis, where chronic stressors such as sensory overload and social misunderstandings deplete coping mechanisms over time. Extended treatment duration (F = 6.28, p = .003) was linked to worsened behaviors, potentially reflecting parental burnout and fragmented support systems in managing complex cases.
Children in special schools displayed more pronounced behavioral challenges than those in regular schools (F = −3.14, p = .002). While specialized settings offer tailored resources, segregated environments may limit opportunities for social integration and observational learning from neurotypical peers, which is critical for adaptive skill development. This finding could also indicate selection bias, as children with severe symptoms often require specialized placements. The results underscore the need for early, sustained interventions and inclusive educational policies to address evolving challenges across developmental stages, fostering environments that mitigate behavioral difficulties and enhance quality of life for children with ASD. 33
Contribution to Existing Literature
This study makes several significant contributions to existing literature on parenting styles and behavioral outcomes in children with ASD by providing region-specific insights from India, a context often underrepresented in global research. It highlights the predominance of authoritative parenting among Indian parents despite cultural tendencies toward authoritarianism while underscoring the significant role of parental education in shaping adaptive caregiving practices. Additionally, it provides evidence linking permissive parenting to increased behavioral challenges in families managing multiple caregiving responsibilities. This finding has been less explored in prior research from India or similar resource-constrained settings. These findings emphasize how cultural nuances influence both parenting styles and their impact on child behavior while addressing critical gaps in regional research on ASD caregiving practices.
Implications for Practice
The findings emphasize the importance of promoting adaptive parenting practices through culturally tailored interventions for families of children with ASD. To bridge this gap, structured interventions integrating parenting modules into ASD care pathways could be implemented at tertiary centers. Psychoeducation should cover ASD awareness, stress management, and provide hands-on training for managing hyperactivity and peer interaction challenges, as well as practical techniques such as positive reinforcement, delivered via low-cost, multilingual workshops. Embedding these programs into routine ASD care, leveraging multidisciplinary teams (including psychiatrists, occupational therapists, and nurses), could reinforce adaptive parenting strategies during follow-ups. Policymakers should prioritize funding for community-based resources that provide accessible training on adaptive parenting strategies. Subsidizing ASD training in public health schemes could democratize access.
Establishing peer support groups could also alleviate parental stress while fostering shared learning experiences among caregivers facing similar challenges. Final, policymakers should prioritize funding for community-based resources that provide accessible training on adaptive parenting strategies, while addressing systemic barriers such as stigma and a lack of awareness about evidence-based practices. By addressing these gaps through evidence-based interventions and policy changes, stakeholders can ensure better support systems for families navigating the complexities of raising a child with ASD within resource-constrained environments such as India.
Strengths and Limitations of the Study
This study provides valuable insights into the relationship between parenting styles and behavioral problems in children with ASD within the Indian context, a region where such research is limited. By utilizing validated tools such as the PSDQ and the SDQ, the study ensures robust and reliable measurement of parenting styles and behavioral outcomes. The inclusion of a diverse urban and semi-urban population from a tertiary care hospital enhances the generalizability of findings to similar settings. Additionally, the study’s focus on associations with baseline demographic variables such as parental education and family structure offers a nuanced understanding of sociocultural influences on caregiving practices.
The cross-sectional design of the study restricts its ability to establish causality between parenting styles and behavioral problems in children with ASD. The reliance on self-reported data introduces potential biases, such as social desirability bias, which may affect the accuracy of responses. Furthermore, key factors such as parental stress, severity of the child’s ASD, mental health, and environmental influences were not assessed, limiting a comprehensive understanding of the determinants of parenting practices. The study’s single-center setting and a predominantly urban and educated sample composition may constrain the generalizability of findings to rural or less formally educated populations in India. The exclusion of children with medical conditions (e.g., seizures, cardiac disorders, and severe respiratory conditions) and the absence of specific data on developmental comorbidities, medications, and therapy details may limit the ability to account for potential confounders of behavioral outcomes, as these factors could influence SDQ scores. However, this was beyond the exploratory psychosocial focus of the study. Last, while focusing on three primary parenting styles, hybrid or situational approaches were not explored, which could provide additional insights into the real-world dynamics of caregiving.
Future Directions
The findings of this study highlight the critical need for further research to deepen our understanding of the relationship between parenting styles and behavioral problems in children with ASD. Future studies should adopt longitudinal designs to establish causality and explore how parenting styles influence behavioral outcomes over time. Expanding the scope of research to include larger, more diverse populations across rural and urban settings in India would enhance the generalizability of findings and provide a more comprehensive understanding of cultural influences on parenting practices.
Future studies could investigate whether authoritative parenting training reduces hyperactivity over a 12-month period and should also explore rural-urban differences in parenting practices. Additionally, research could also examine the role of parental stress, mental health, and social support systems in shaping parenting behaviors and their impact on children’s outcomes. Qualitative studies exploring parents’ lived experiences could provide valuable insights into the challenges of caregiving for children with ASD and the factors influencing their choice of parenting style. Intervention-based studies aimed at fostering adaptive parenting practices, such as authoritative approaches, could also be developed and evaluated for their effectiveness in improving behavioral outcomes in children with ASD.
Conclusions
This study underscores the significant role of parenting styles in shaping behavioral outcomes among children with ASD within an Indian context. The findings reveal that authoritative parenting is associated with fewer behavioral challenges, while authoritarian and permissive styles correlate with increased difficulties, particularly in domains such as hyperactivity and peer interactions. These results emphasize the need for culturally tailored interventions that promote adaptive parenting practices to mitigate behavioral problems in children with ASD. By addressing gaps in understanding through further research and implementing evidence-based strategies to support parents, stakeholders can enhance the quality of life for both children with ASD and their families. This study contributes to the growing body of literature on ASD caregiving by providing region-specific insights that can inform clinical practice, policy-making, and future research efforts.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None Used.
Ethical Considerations
The study was approved by the Institutional Ethics Committee of St. John’s Medical College (IEC Ref No. TH-185/2023).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Not applicable.
Informed Consent
The study involved parent participants completing standardized questionnaires. No identifiable patient data, images, or clinical details were collected or published. Written informed consent for participation was obtained from all respondents.
Prior Presentations
Nil.
Simultaneous Submission to Another Journal or Resource
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.