
Abstract
Background:
Dissociative disorders, characterized by disruptions in consciousness, memory, and identity, pose significant challenges in understanding their neuropsychological domains—particularly within the Indian context—due to limited research. This study aims to compare the neuropsychological functions of young adults diagnosed with dissociative disorder to those of a healthy control group.
Method:
A comparative cross-sectional study was employed using a between-group design. The sample consisted of 30 individuals diagnosed with dissociative disorder and 30 healthy controls (aged 18–30), selected through purposive sampling from a government neuropsychiatric hospital in North India. Standardized assessments, including the Dissociative Experiences Scale (DES) and selected subtests from the National Institute of Mental Health and Neurosciences neuropsychological battery (Auditory Verbal Learning Test and Triads Test [AVLT]), along with the Stroop Color and Word Test (SCWT) and the Trail Making Test (TMT), were administered. Statistical analyses, including t-tests, Mann–Whitney U-tests, chi-square tests, and correlational analyses, were conducted using the Statistical Package for the Social Sciences (SPSS) Version 27.0.
Results:
Participants with dissociative disorder demonstrated significantly higher DES scores than controls, indicating more significant dissociative experiences. While some neuropsychological domains did not show significant differences, individuals with dissociative disorder exhibited poorer performance on the SCWT, TMR Parts A and B (TMT-A and TMT-B), and the recognition commission component of Rey’s AVLT. Correlation analyses revealed moderate associations between executive functioning, verbal memory, inhibitory control, and dissociative experiences.
Conclusion:
The findings highlight the association between neuropsychological factors and dissociative disorders, particularly within the Indian population. These insights may contribute to improved clinical assessments and interventions.
Keywords
Individuals with dissociative disorder exhibit significant impairments in executive functioning and inhibitory control compared to healthy controls, highlighting the neuropsychological deficits associated with the disorder. The study emphasizes the importance of neuropsychological assessments in understanding dissociative disorders, particularly in the Indian context, where such research is limited.Key Messages:
According to Bernstein and Putnam, dissociation is a “lack of normal integration of thought, feeling, and experiences into consciousness and memory.” 1 Subtypes include dissociative amnesia, dissociative fugue, dissociative trance, and dissociative motor disorders, among others. 2 According to the National Mental Health Survey conducted in 2016, the lifetime prevalence of neurotic and stress-related disorders was reported to be 3.7%. 3 Despite extensive research on psychosocial factors,4,5 the neuropsychological aspects of dissociation remain underexplored.
Janet emphasized memory deficits during symptomatic periods, highlighting gaps in understanding the neuropsychological dimensions of dissociation and related conditions.6,7 Indian studies have focused primarily on children and adolescents,8,9 revealing cognitive deficits such as impaired attention and memory. However, research exploring dissociation and neuropsychological impairment in the Indian population—particularly among young adults—is limited, which highlights the need for comprehensive studies in this context.
A relationship between dissociation and memory has been explored.10,11 High scores on the Dissociative Experiences Scale (DES) were associated with remembering fewer emotionally charged words and more neutral words, suggesting that dissociative tendencies influence the processing of emotionally relevant information. It was further observed that under divided attention, individuals with high dissociation recalled fewer trauma-related words, possibly reflecting a protective mechanism against threatening information.10,11 It was found that individuals with dissociative identity disorder (DID) showed effective cognitive inhibition in neutral contexts but impaired inhibition in negative contexts, which was linked to heightened anxiety. This was coupled with slower responses to negative stimuli, highlighting an attentional bias and its effect on executive functioning and emotional regulation in DID. 12 Similarly, women with psychogenic nonepileptic seizures demonstrated intact verbal memory but impairments in attention and working memory, likely influenced by emotional distress. 13
Indian studies have examined neurocognitive deficits in adolescents with dissociative disorders, reporting impairments in verbal working memory, sustained attention, and executive functioning.8,9 However, the cognitive impact of dissociation on young adults in India remains underexplored. Conflicting evidence—such as findings that report no significant link between dissociation and cognitive deficits14,15—underscores the need for further research. Understanding the neuropsychological dimensions of dissociation is crucial for developing effective interventions tailored to the Indian population.
Aim
The aim of this study was to compare the neuropsychological functions of young adults with dissociative disorder and healthy adults.
Objectives
The primary objective of this study was to assess neuropsychological functions—including verbal learning, immediate recall, delayed recall, recognition, selective attention, divided attention, response inhibition, and set-shifting ability—among young adults diagnosed with dissociative disorder and a healthy control group. A secondary objective is to assess and compare the dissociative experiences of individuals in both groups. Additionally, the study aims to examine differences in specific neuropsychological domains such as verbal learning, immediate recall, delayed recall, recognition, processing speed, divided attention, response inhibition, and set-shifting ability between the two groups. Finally, the study explores potential relationships between dissociative experiences and neuropsychological functions.
Null Hypotheses
It was hypothesized that there would be no statistically significant differences in neuropsychological functions—including verbal learning, immediate recall, delayed recall, recognition, processing speed, divided attention, response inhibition, and set-shifting ability—between young adults with dissociative disorder and healthy controls. It was also hypothesized that the two groups would show no statistically significant difference in dissociative experiences. Additionally, no statistically significant relationship was expected between dissociative experiences and neuropsychological functioning.
Methods
Ethical Considerations
The study was approved by the Institutional Ethics Committee. Written informed consent was obtained from all participants before their inclusion in the study.
Study Design
This was a comparative cross-sectional study with a between-group design.
Setting
The study was conducted in the outpatient department (OPD) of a government neuropsychiatric hospital that offers free services and serves individuals from both economically weaker and higher socioeconomic classes, hailing from both rural and urban backgrounds.
Sample Size
The target population for this study was defined as clients diagnosed with dissociative disorder in North India. The accessible population comprised individuals with a diagnosis of dissociative disorder (as per International Classification of Diseases, 10th Revision [ICD-10] Code F44) attending the hospital’s OPD. A sample of 30 individuals diagnosed with dissociative disorder and 30 individuals with no psychiatric illness were selected. Formal sample size estimation was not conducted, as the study was part of an MPhil dissertation and was constrained by time and institutional requirements.
Inclusion Criteria
Participants in the study group were included based on the following criteria: they had a clinical diagnosis of a dissociative disorder according to the ICD-10 criteria, as documented by the clinical team or in the case record file. Eligible participants were between 18 and 30 years of age, of any gender, and had a minimum educational qualification of completing the 10th grade. The healthy control group included individuals aged between 18 and 30 years who had completed at least the 10th grade and had no history of psychiatric illness or other comorbid medical or neurological conditions.
Exclusion Criteria
Exclusion criteria for the study group included the presence of a comorbid diagnosis of any severe mental illness or psychosis, severe organic or neurological conditions (including seizure disorders), or intellectual functioning below average or impaired as per clinical judgment. Individuals were also excluded if they had any neurodevelopmental, visual, or hearing impairments or any other physical, psychosocial, or developmental disabilities. Participants experiencing acute stress or emotional crises during the interview were excluded.
The control group shared the same exclusion criteria as the study group. Individuals were excluded if they met the criteria for any severe mental illness or psychosis, had a severe organic or neurological disorder (including seizure conditions), exhibited below-average intellectual functioning, or had any neurodevelopmental, visual, hearing, physical, or psychosocial disabilities. Participants experiencing acute stress or emotional distress at the time of data collection were also excluded.
Procedure
The study was conducted over a period of 5 months, from September 2023 to January 2024. Patients with dissociative disorder were selected from the clinical psychology department of a tertiary care hospital in North India. Participants’ handedness was assessed, and all neuropsychological tasks were performed using the dominant hand to ensure consistency, except for tasks that specifically required the use of the nondominant hand. Assessments were conducted in individual sessions, each lasting approximately one to one and a half hours.
Tools Used
DES is widely used to measure dissociative symptoms, including depersonalization and derealization. Developed in 1986 at the National Institutes of Mental Health, it aims to quantify dissociative symptoms. 1 The scale demonstrates high internal consistency (Cronbach’s α = 0.90). It consists of 28 items where participants indicate the frequency of various experiences using a 100-mm visual analog scale. A total score of 20 or above may be indicative of trauma-related or dissociative disorders.
Neuropsychological assessment was conducted using selected subtests from the National Institute of Mental Health and Neurosciences (NIMHANS) Neuropsychological Battery, developed by Shobhini Rao. This battery contains a comprehensive collection of validated cognitive tasks with norms standardized for Indian populations. 16 In this study, two key subtests were used: Rey’s Auditory Verbal Learning Test (AVLT) and the Triads Test.
The AVLT 17 was culturally adapted for different populations by the World Health Organization to suit conditions in India. The test includes two lists, A and B, with words selected from five categories for universal familiarity: body parts, animals, tools, household objects, and vehicles. Participants are asked to listen to and memorize the lists of words to recall later or recognize the items, which assesses learning, recall, storage, and memory consolidation over time. The test’s composition, instructions, and scoring method significantly influence its outcomes. The AVLT is widely used in clinical and research settings to evaluate verbal memory performance. The Triads Test, developed at NIMHANS, is a dual-task procedure that evaluates divided attention by administering a verbal triad task and a tactual number identification task simultaneously. Participants must identify the “odd word out”—the word that does not belong conceptually or categorically with the other two in verbal triads—while simultaneously recognizing a number drawn on their nondominant hand. 16 Analysis involves counting errors made during the tasks and comparing them to established age and education norms to determine performance relative to the cutoff threshold.
The Stroop Color and Word Test (SCWT), first introduced by Stroop in 1935, is a widely used neuropsychological assessment designed to measure cognitive interference and the ability to inhibit automatic responses. The Golden version, developed by Golden in 1978 and further refined by Golden and Freshwater in 2002, 18 is a commonly used test and was utilized in this study. 19 It comprises three pages: a Word Page with color words printed in black ink, a Color Page with colored Xs, and a Color-Word Page combining words and colors. Participants must read the words or name the ink color as quickly as possible within 45 s. Scores are based on the number of items completed on each sheet, with an interference score calculated to measure the disruption caused by mismatched words and ink colors. The Trail Making Test (TMT) was initially known as “Partington’s Pathways” or the “Divided Attention Test” and was developed in 1938 by Partington and Leiter. This assessment was first included in the Army Individual Test Battery in 1944. Reitan later modified it in 1955 and incorporated it into the Halstead Battery. 19 This test assesses attention, speed, and mental flexibility by requiring participants to connect 25 encircled numbers sequentially (Part A) and 25 encircled numbers and letters alternately arranged (Part B) using pencil lines. TMT comes in two forms: the Child (Intermediate) Form for ages 9–14 and the Adult Form for ages 15 and older. In TMT-A, participants connect consecutive numbers from 1 to 25, while TMT-B involves connecting numbers and letters in an alternating sequence. The time difference in completing TMT-B is a crucial measure of central executive functioning, emphasizing task-set inhibition, cognitive flexibility, and response-set maintenance.
Statistical Analysis
Statistical analysis involved descriptive analysis to outline sociodemographic characteristics (age, gender, education, socioeconomic status) using frequency distributions, means, and standard deviations. Group score comparisons were conducted using t-tests initially, with the Mann–Whitney U-test used as a nonparametric alternative when normality assumptions were violated (assessed via the Shapiro–Wilk test). Chi-square tests were used to examine associations for categorical data, and correlation analysis explored relationships between continuous variables, using Pearson correlation coefficients for approximately normal distributions and Spearman’s rank correlation for non-normal data. The Statistical Package for the Social Sciences (SPSS) Version 27.0 facilitated statistical analyses and provided output for interpretation. Cohen’s d was calculated to estimate effect sizes for significant results from parametric tests. For nonparametric comparisons using the Mann–Whitney U-test, effect sizes were calculated using the rank-biserial correlation (r).
Results
Table 1 presents the demographic characteristics of the study participants, including age, sex, education level, family type, residence, and marital status. The female-to-male ratio in this population was 14:1. Gender distribution shows a predominance of females in both groups, with 97% in the study group and 90% in the healthy control group. The mean age of participants in the study group was 22.23 years (standard deviation [SD] = 3.50), while the mean age in the control group was 22.37 years (SD = 2.31). Educational backgrounds varied, with a higher proportion of graduates in the control group (70%) compared to the study group (30%). There were no married individuals in the control group, whereas 30% of participants in the study group were married. Most participants in both groups came from urban areas (73%), with a notable minority from rural areas (27%). Family structure analysis indicated that the majority in both groups were from nuclear families, although the control group had a comparatively higher proportion (90%) than the study group (60%).
Sociodemographic Profile of the Participants.
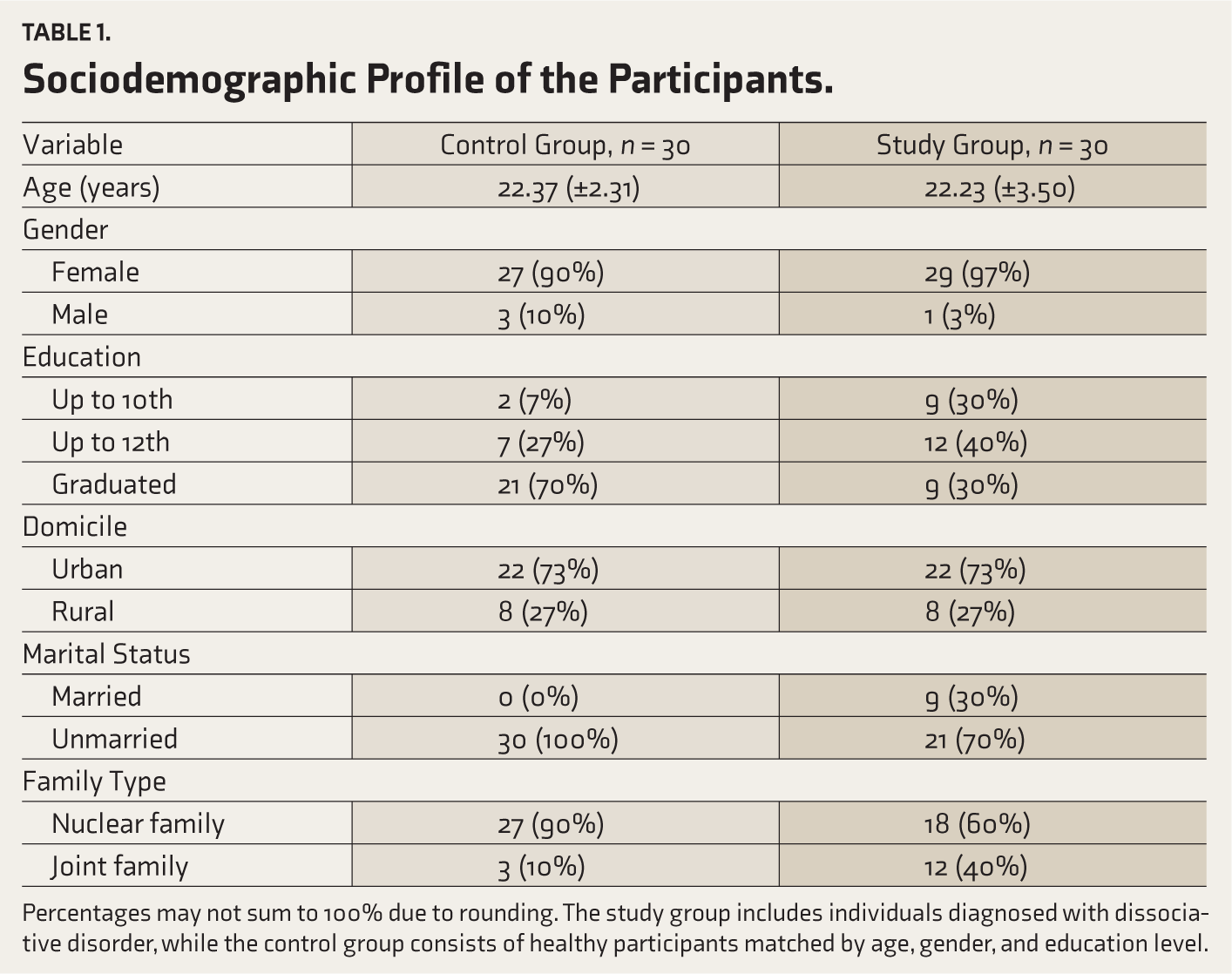
Percentages may not sum to 100% due to rounding. The study group includes individuals diagnosed with dissociative disorder, while the control group consists of healthy participants matched by age, gender, and education level.
Table 2 presents the DES scores for the control and study groups. The control group exhibited a significantly lower prevalence of high scores (above 20) on the DES compared to the study group, with only 13% of the control group scoring above 20, in contrast to 87% of the study group participants. The t-test revealed a significant difference between the two groups, with the study group having a higher mean score (M = 30.33, SD = 10.33) compared to the control group (M = 7.67, SD = 7.93), t = −9.53, p < .001. Cohen’s d was calculated as −2.46, indicating a large effect size.'
Comparison of DES Scores Between Control Group and Study Group Using t-test.
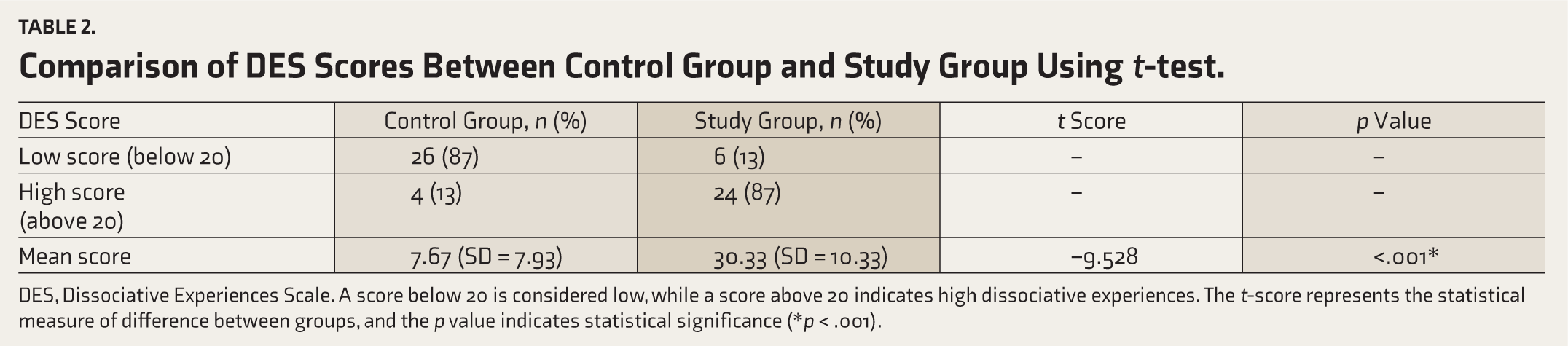
DES, Dissociative Experiences Scale. A score below 20 is considered low, while a score above 20 indicates high dissociative experiences. The t-score represents the statistical measure of difference between groups, and the p value indicates statistical significance (*p < .001).
Table 3 presents a chi-square analysis of different neuropsychological domains between the control and study groups. Based on the results of the chi-square analysis, there were no statistically significant differences between the control group and the study group in terms of AVLT Learning (χ2(2) = 1.67, p = .96), AVLT Immediate Recall (χ2(2) = 2.78, p = .10), AVLT Delayed Recall (χ2(2) = .08, p = .77), AVLT Recognition Hits (χ2(2) = 1.11, p = .29), AVLT Recognition Omission (χ2(2) = 1.46, p = .23), and Triads Test (χ2(2) = 1.20, p = .27). Notably, a significant difference was found between the control and study groups in the AVLT Recognition Commission (χ2 (2) = 8.04, p = .01).
Chi-square Analysis of Neuropsychological Domains Between Study and Control Groups.
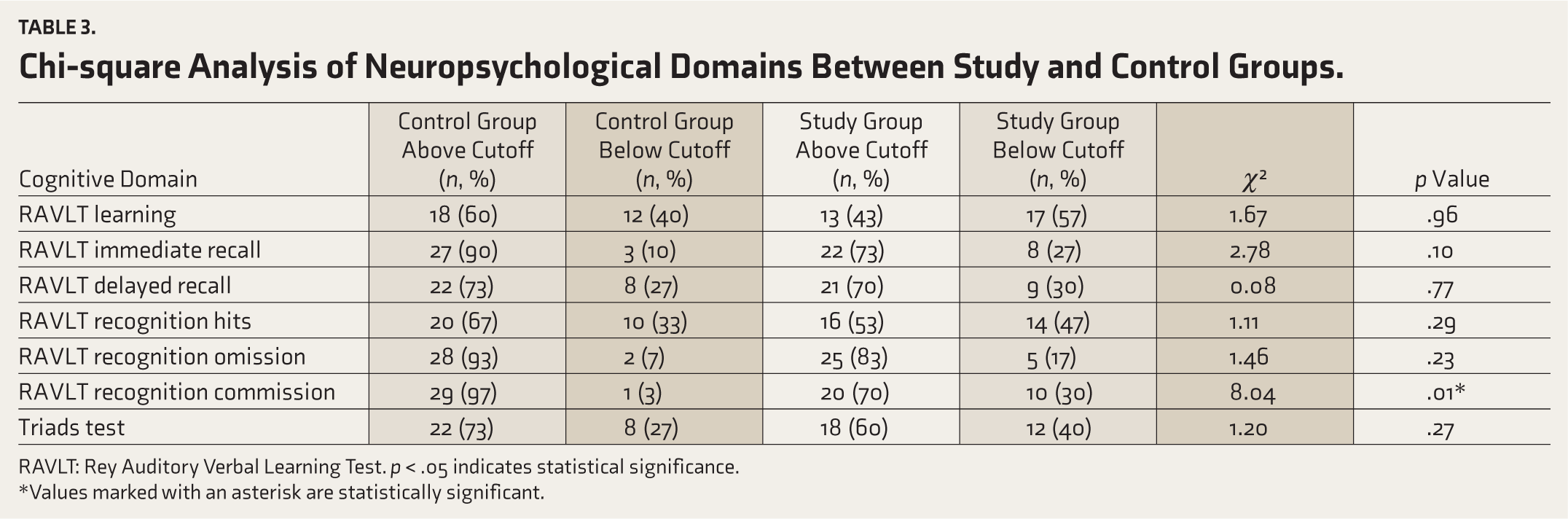
RAVLT: Rey Auditory Verbal Learning Test. p < .05 indicates statistical significance.
*Values marked with an asterisk are statistically significant.
Table 4 shows that the results revealed a significant difference between the control and study groups in their performance on the SCWT, t = 2.72, p < .001. Participants in the control group demonstrated significantly higher SCWT scores (M = 46.50, SD = 9.54) compared to those in the study group (M = 37.87, SD = 12.09), indicating poorer performance in inhibitory control and cognitive flexibility tasks among the study group. Cohen’s d for the Color Word condition was calculated as 0.701, indicating a medium effect size. However, no significant difference was found between the two groups in their performance on the Stroop interference scores, t = 1.72, p = .09. Participants in both groups exhibited comparable scores (control group: M = 50.63, SD = 8.38; study group: M = 46.70, SD = 9.29) on this measure of cognitive interference.
Comparison of SCWT Scores Between Study and Control Groups Using t-test.
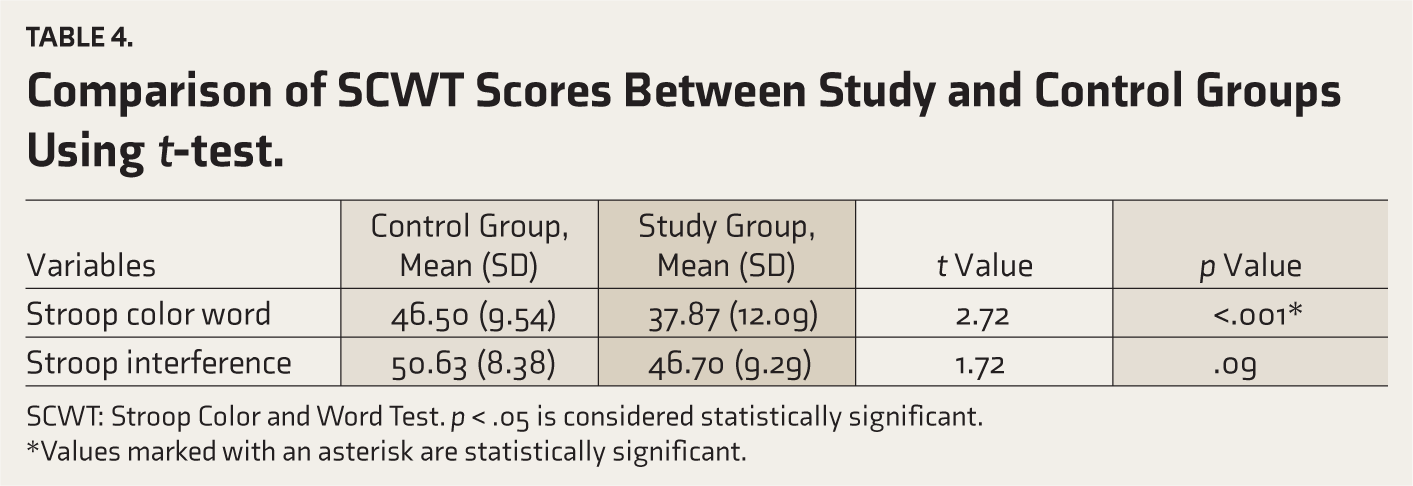
SCWT: Stroop Color and Word Test. p < .05 is considered statistically significant.
*Values marked with an asterisk are statistically significant.
Table 5 presents the results, which revealed a significant difference between the control and study groups in their performance on both TMT-A (U = 125, p < .001) and TMT-B (U = 153.5, p < .001). Participants in the control group achieved significantly lower mean ranks on both tasks than those in the study group, indicating shorter completion times and potentially better performance in visuomotor processing speed and cognitive flexibility. The effect size, calculated as rank-biserial correlation (r) = −0.62, indicates a medium effect.
Comparison of TMT Scores Between Study and Control Groups Using Mann–Whitney U-test
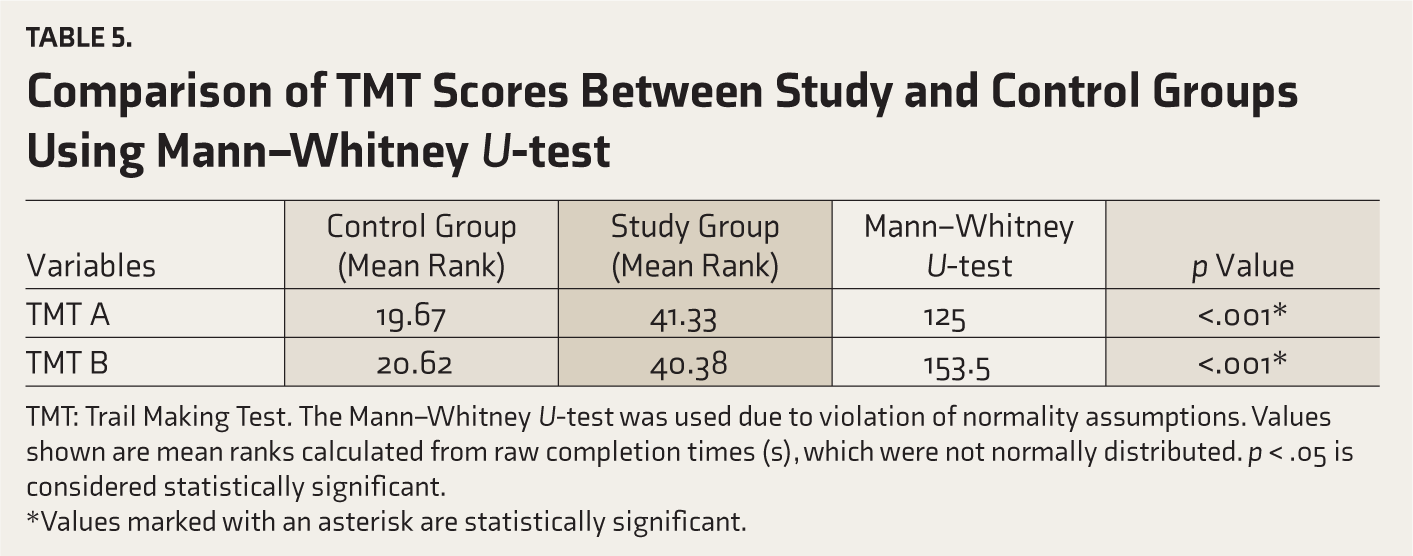
TMT: Trail Making Test. The Mann–Whitney U-test was used due to violation of normality assumptions. Values shown are mean ranks calculated from raw completion times (s), which were not normally distributed. p < .05 is considered statistically significant.
*Values marked with an asterisk are statistically significant.
Table 6 presents two types of correlation analysis, Pearson and Spearman, which comprehensively assessed the relationship between neuropsychological tasks and the DES score. Pearson correlation measures linear relationships between variables when both variables are normally distributed, while Spearman correlation is employed when the variables are not normally distributed.
As noted in Table 6, Pearson correlation was chosen for tasks such as the SCWT, where assumptions of normality were met. In contrast, due to non-normality, Spearman correlation was utilized for tasks like TMT-A, TMT-B, and various AVLT tasks. The results in Table 6 highlight the correlations between individual cognitive tasks and the DES score. Particularly significant positive Spearman correlations were observed for TMT-A and TMT-B tasks with the DES score (TMT-A: r = 0.47, p < .001; TMT-B: r = 0.36, p = .005). These findings suggest that participants exhibiting poorer performance, as indicated by longer task completion times, tended to have higher DES scores. This implies a potential link between executive functioning, as assessed by these tasks, and the level of dissociative experience measured by the DES.
Correlations Between DES Scores and Neuropsychological Test Performance Across All Participants (N = 60) Using Pearson and Spearman Correlation Methods.
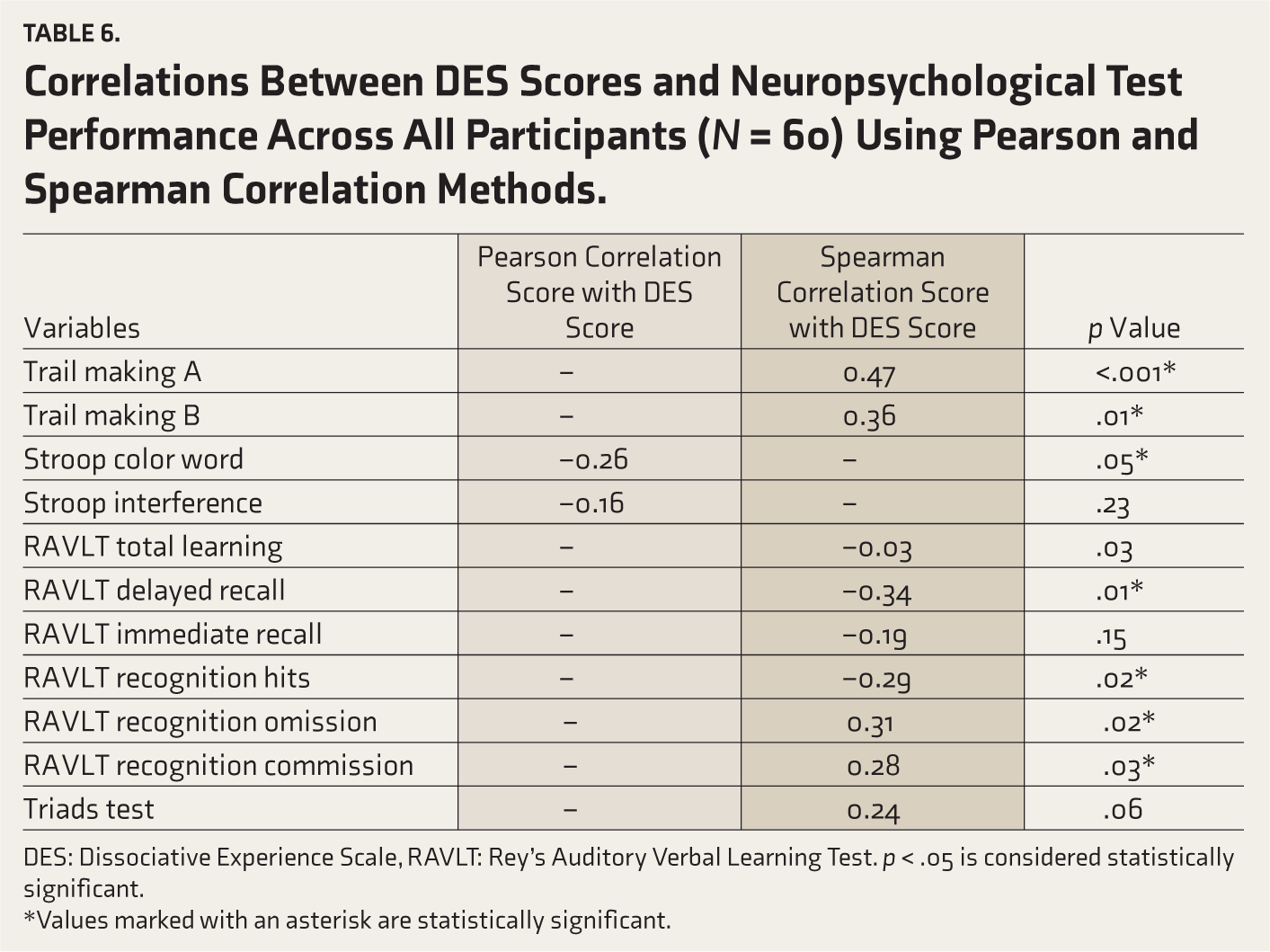
DES: Dissociative Experience Scale, RAVLT: Rey’s Auditory Verbal Learning Test. p < .05 is considered statistically significant.
*Values marked with an asterisk are statistically significant.
Additionally, the SCWT task revealed a significant negative Pearson correlation with the DES score (r = −0.26, p = .05), indicating that participants who performed better on this task tended to have lower DES scores. This implies a potential relationship between inhibitory controls as assessed by the SCWT. Moreover, several AVLT tasks displayed significant negative Spearman correlations with the DES score, including Total Learning (r = −0.29, p = .026) and Delayed Recall (r = −0.34, p = .01). These findings suggest potential associations between verbal learning and memory, as assessed by the AVLT, and dissociative experiences measured by the DES. In contrast, the correlations between DES score and tasks such as AVLT Immediate Recall, AVLT Recognition Hits, and the Triads Test were not statistically significant, indicating weaker or nonexistent associations between these cognitive domains and dissociative experience. No corrections were applied for multiple correlational analyses, so the reported correlations should be considered exploratory and based on unadjusted p values.
Discussion
This study examined neuropsychological differences between individuals diagnosed with dissociative disorders and a healthy control group. Although the groups were matched on several sociodemographic variables, a significant difference in the educational variable was observed. Consistent with the existing literature, a higher incidence of dissociation among females was observed, 20 and it was found that dissociative motor disorder was the most prevalent subtype, followed by dissociative convulsions. 21
The DES scores were significantly higher in the study group, indicating a greater frequency and intensity of dissociative experiences. This underscores the value of the DES in identifying and quantifying dissociative symptoms. Neuropsychological tests revealed significant differences between the study and control groups in specific domains, particularly executive functions. The SCWT results suggested deficits in inhibitory control and cognitive flexibility among patients with dissociative disorders, consistent with findings from other studies.10,11
The study observed significant differences in performance between the study and control groups across several neuropsychological tasks. The SCWT revealed lower mean scores in the study group, suggesting potential deficits in inhibitory control and cognitive flexibility. Lower scores on the color-word part of the Stroop Test, along with a significant difference from the control group, indicate a range of cognitive difficulties, such as processing speed, inhibitory control, attention, memory, and executive functioning. These lower scores may reflect broader deficits in executive functioning, including difficulties with planning, problem-solving, and cognitive control. This may be due to slow processing speed, which can affect the ability to accurately identify ink colors while suppressing the automatic tendency to read the word. Despite intact individual color and word scores, lower performance on the color-word component of the Stroop Test suggests interference effects. Previous literature has associated such interference with reduced cognitive flexibility and executive function challenges, potentially linked to prefrontal activity. 18
The TMT also indicated impaired processing speed and executive function in the study group. These findings align with study, 22 which linked higher dissociation levels to poorer performance on executive function tasks. The TMT results indicated impairments in both processing speed (Part A) and cognitive flexibility (Part B). Poor performance in Part A reflects difficulties in processing speed, while difficulties in Part B suggest deficits in cognitive flexibility, which involves the ability to shift between tasks or mental sets. These findings highlight that the clinical group faces challenges in both processing speed and cognitive flexibility, which may contribute to difficulties in managing complex tasks. Despite these differences, no significant differences were found in tasks assessing verbal learning, memory, and divided attention, consistent with some previous studies.9,23
In this study, individuals with dissociative disorder showed difficulties in some areas of executive functioning compared to the control group. Specifically, impairments in processing speed, set-shifting ability, and response inhibition were identified as key neuropsychological functions associated with the prefrontal cortex. The prefrontal cortex is essential for managing executive control and moderating an overactive response from the amygdala.24,25 Extended exposure to stress has the potential to negatively affect both the prefrontal and hippocampal regions, resulting in symptoms commonly seen in individuals who have experienced trauma, such as intrusive thoughts, complete memory loss, or dissociative memories. 25 While previous literature has suggested that chronic stress may impact both the prefrontal and hippocampal regions, the present study did not find significant differences between the groups in verbal learning, immediate memory, or delayed recall as measured by the AVLT. These findings suggest that hippocampal-related memory functions may not be significantly impaired in individuals with dissociative disorders in this sample. Instead, the observed deficits in tasks involving processing speed, inhibitory control, and response inhibition—such as the SCWT and TMT—are more consistent with dysfunctions in the prefrontal cortex, particularly the orbitofrontal region, which plays a key role in executive functions and emotional regulation.
Correlation analysis revealed moderate-strength positive correlations between dissociative experience scores and performance on TMT A and B, and a moderate-strength negative correlation with the SCWT. This suggests that higher levels of dissociation are associated with poorer performance in tasks requiring attention and cognitive flexibility, supporting findings from other studies. 26
Although higher proportions of participants in the study group scored below the cutoff in most neuropsychological tasks—suggesting greater difficulties in attention, processing speed, and executive functions—these differences were not statistically significant for specific tasks, such as the AVLT. While this study found group-level differences in some domains of neuropsychological functioning, such as processing speed, executive function, and attention, the cross-sectional and exploratory design of this study does not allow for conclusions about causality. These findings highlight potential neuropsychological factors that may co-occur with dissociative disorders.
Limitations
First, using a convenience sample from a tertiary care center may introduce selection bias and limit generalizability. The cross-sectional design prevents exploration of temporal relationships, so longitudinal studies would be valuable in understanding changes over time. Another significant limitation is the inability to account for medication effects, as specific medication details were not assessed. These limitations suggest areas for future research to better understand the complexities of dissociative disorder and neuropsychological functioning.
Conclusion
This study has provided valuable insights into the relationship between dissociative disorders and neuropsychological functioning. It has revealed significant differences between individuals with dissociative disorders and healthy controls through a comprehensive analysis of neuropsychological domains such as processing speed, set-shifting ability, inhibitory control, attention, memory, and executive functioning. Specifically, individuals with dissociative disorders demonstrated deficits in certain areas of neuropsychological functioning, particularly those associated with executive functions mediated by the prefrontal cortex. However, no significant relationship difference was found between the groups in verbal learning, immediate memory, and delayed memory. Additionally, the study revealed significant correlations between different neuropsychological functions and scores on the DES, suggesting a significant relationship between dissociative experiences and neuropsychological functioning. These correlations underscore the importance of considering psychological and cognitive factors in understanding dissociative disorders and designing appropriate interventions. The absence of significant differences between the study group and control group in some neuropsychological domains, despite their significant association with dissociative experiences, may be attributed to the complexity of dissociative disorders, methodological considerations, and variability in dissociative experiences among individuals. These factors underscore the need for comprehensive assessments and larger-scale research to better understand the interplay between dissociative experiences and neuropsychological functioning in individuals with dissociative disorders. This study advances our knowledge of dissociative disorders and underscores the importance of integrating neuropsychological assessments into clinical practice. By addressing both cognitive and emotional components, clinicians can develop more holistic treatment approaches tailored to the unique needs of individuals with dissociative disorders.
The findings underscore the importance of considering both cognitive and emotional aspects in assessing and treating dissociative disorders. Therapeutic interventions should aim to address neuropsychological deficits alongside emotional dysregulation, recognizing the interconnected nature of these domains. By adopting a comprehensive approach, clinicians can provide more effective support and treatment for individuals with dissociative disorders, ultimately improving their quality of life. Furthermore, the study contributes to the broader understanding of dissociative disorders and their impact on neuropsychological functioning. It highlights the need for further research to elucidate the underlying mechanisms driving neuropsychological impairments in dissociative disorders and to explore potential factors that may influence variability in neuropsychological performance across individuals.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Statement
Ethical approval was provided by Institutional Ethics Committee—IHBAS (IEC-IHBAS-2023/7/37/V-2).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.