
Abstract
Background:
Thought disorder is considered to be central to the core disturbances in schizophrenia and was described by Goldstein as aberrant “concept formation.” Executive dysfunction is another core deficit in schizophrenia. With a greater emphasis on psychopathology in nosological systems, the classical thought disorder receives less prominence. The present study aimed to understand the association between classical thought disorder (aberrant concept formation and concrete abstraction) and executive dysfunction.
Methods:
Thirty patients with schizophrenia and thirty healthy subjects, matched on age, gender, education, and socioeconomic status, were screened using MINI 5.0, following which they were assessed on object sorting test (OST) and selected tests for executive functions (EFs).
Results:
Individuals with schizophrenia were found to have significantly decreased performance on all domains of EFs and OST. Total peculiar scores on OST were significantly associated with mental speed, focused attention, and divided attention. Total impoverished scores on OST was significantly associated with focused attention, sustained attention, planning, set shifting, perseveration, and concept formation.
Conclusion:
Several correlations, among performance on OST and neuropsychological tests, suggest that patterns of responses on OST can point to underlying executive dysfunction. Both thought disorder and executive dysfunction mirror similar constructs. This similarity represents a conceptual bridge between the classical and contemporary descriptions of the core deficits in schizophrenia.
In patients diagnosed with schizophrenia, performance on OST is associated with performance on tests of executive functions. Deficits in attention, working memory, and perseveration predict impoverished response on OST, and deficits in divided attention predict peculiar responses on OST. The pattern of responses in OST can give an overview of executive dysfunction in patients with schizophrenia.Key Messages:
Classical thought disorder refers to aberrant concept formation and concrete abstraction. In schizophrenia, it is seen as a breakdown in the mechanisms, rules, or laws of governing the orderly and logical sequence of thinking. 6 Payne 7 and Goldstein 8 considered abnormality of concept formation as a cause of thought disorder in schizophrenia. Cameron 9 considered thinking problems in schizophrenia to be due to an inability to maintain conceptual boundaries. OST, as described by Rapaport, 10 is a measure of sorting behavior and is an expression of concept formation. It is similar to Kasanin and Hanfmann’s 11 block sorting test. Using this test, Kasanin and Hanfmann 11 reported that in schizophrenia, there is a reduction in the ability to form new concepts, which is apparent even in patients with previous high intellectual abilities and educational attainment. They concluded that in schizophrenia, there is a regression from conceptual thinking to lower levels, such as found in children.
Cognitive impairments are at the very core of the dysfunction in schizophrenia. 12 Emerging evidence from neuropsychological and neuroimaging studies in schizophrenia demonstrates executive dysfunction and frontal lobe deficits in schizophrenia.13–15 We now consider schizophrenia as a “cognitive disorder.”16,17 Hence the concept of thought disorder as described by Bleuler 1 or Cameron 9 may mirror closely the deficits seen as dysexecutive syndrome in schizophrenia.
Studies attempting to find correlations between thought disorder and executive function (EF) have reported strong associations between thought disorder in schizophrenia and tests of verbal memory, attention, abstraction, and EF.18–21 In recent years, studies have exclusively focused on Andreason’s 4 concept of FTD and have reported it to be associated with semantic and executive dysfunction.22–24 These studies suggest a potential theoretical association between the two concepts; however, there have been no studies examining associations between classical thought disorder as assessed by OST with neuropsychological test performance. Hence, the present study aimed to examine this gap by identifying those deficits in EFs that are implicated in the poor performance in OST. The main objective of this study was to assess EFs as measured by standardized neuropsychological tests and their association with thought disorder as assessed by OST in patients with schizophrenia.
Materials and Methods
Study Design
A time-bound cross-sectional research design was used. Purposive sampling was adopted for data collection.
Participants
The participants included 30 stable schizophrenia patients (26 paranoid and 4 undifferentiated), and 30, age (±1 year), gender, education, and socioeconomic status matched, healthy control subjects. The schizophrenia group (SG) was recruited from outpatient and inpatient services and rehabilitation center of the psychiatry department of a tertiary care hospital (Kasturba Medical College Hospital, Udupi, Karnataka). The inclusion criteria are as follows: (a) DSM IV-TR 25 diagnosis of paranoid or undifferentiated schizophrenia, (b) on a stable dose of antipsychotics in the last six weeks, (c) age range of 18–50 years, and (d) had no observable side effects interfering with test performance. Subjects with comorbid Axis I psychiatric disorders, history of receiving electroconvulsive therapy or cognitive rehabilitation in the last one-month, serious medical conditions, neurological disorders, acute agitation, suicidal tendencies, or catatonic features were excluded. The diagnosis of schizophrenia was made based on clinical interview and examination independently by two psychiatrists.
The participants in the healthy control group (HCG) were recruited from the same catchment area through convenient sampling. Those in whom screening revealed Axis I psychiatric disorders, serious medical conditions, neurological disorders, or presence of the family history of psychosis in first-degree relatives were excluded.
Tools
Sociodemographic and clinical information was collected on a semistructured pro forma, which also included Global Assessment of Functioning (GAF) scale from DSM-IV-TR. 2 Cross-sectional assessments were performed on SG and HCG on the following tools.
Mini-International Neuropsychiatric Interview (MINI) 5.0 26 : MINI was administered on SG to confirm the diagnosis of schizophrenia and to rule out comorbid psychiatric disorders. The MINI screen was administered on HCG to rule out the presence of psychiatric disorders.
Scale for the Assessment of Negative Symptoms (SANS) 27 and Scale for the Assessment of Positive Symptoms (SAPS) 28 : SANS and SAPS were administered to assess negative and positive symptoms respectively in SG. The rating is based on the information obtained through interviews, observations made during a standard clinical interview, and discussions with close associates such as family members.
Tests of Executive Functioning from NIMHANS Neuropsychological Battery 29 : The tests for EFs were taken from NIMHANS neuropsychological battery, which has been standardized on the Indian population. The tests of executive functioning used are as follows.
Digit Symbol Substitution Test (DSST): The DSST measures mental speed. The subject is asked to substitute each digit with a symbol, using a number-symbol key given at the top of the page, row by row, after a practice trial for the first ten squares. The raw score of the time taken in seconds to complete the test was taken for analysis.
Controlled Oral Word Association (COWA) Test: COWA test is a measure of phonemic fluency. The subject is asked to generate words beginning with the letters F, A, and S for 1 minute each. The average number of new words generated over the three trials was taken for the analysis.
Animal Names Test (ANT): ANT is a measure of category fluency, which is another form of verbal fluency. The subject is asked to generate the names of as many animals as possible in 1 minute. The total number of new words generated forms the score.
Digit Vigilance Test (DVT): The DVT measures sustained attention. The test consists of numbers 1–9 randomly ordered and placed in rows on the sheet. The subject is asked to scan the sheet and cancel the target numbers 6 and 9 by drawing “/” mark on them as fast as possible, without missing the targets or canceling the wrong numbers. The analysis was done on the raw score of time taken in seconds to complete the test.
Color Trails Test (CTT): This test measures focused attention. The subject is presented with a sheet of paper in which 25 printed circles are scattered, each enclosing one of the numbers 1–25, and is asked to join the circles in numerical order as quickly as possible. The time taken in seconds to complete Trail 1 forms the score. Both color Trail 1 and 2 were administered, but since many participants could not complete the color Trails 2 task, the data was not used in the analysis.
Triads Test: This assesses divided attention. The subjects are given a verbal triad task and tactual number identification task simultaneously. In the former, they have to name the odd word, and in the latter, they have to identify the number written on their nondominant hand. The number of errors committed on the tasks was taken for analysis.
Verbal and Visual N-Back: N-back tests are a measure of verbal and visual working memory. In the verbal 2-back test, 30 randomly ordered consonants common to multiple Indian languages are presented auditorily at the rate of 1 per second. The subject responds whenever a consonant is repeated after an intervening consonant. The visual 2-back test consists of 36 cards, each with one black dot placed randomly. Each card is individually presented to the subject. The subject is told to respond whenever the location of the dot repeats after an intervening card. The number of correct responses forms the score in each test.
Tower of London Test (TOL): TOL is a test of planning and evaluates the subject’s ability to plan and anticipate the results of their actions to achieve a predetermined goal. The test consists of two sets of boards, each with three pegs and three different colored balls. The subject is presented with goal state of the arrangement of the three balls and is told to arrange the balls in the other board in the same way by following certain rules. The raw score of the number of moves made to attain the goal state on the fifth trial was taken for the analysis. Performance on the fifth task on TOL was taken into consideration because most participants successfully performed the first four tasks. The fifth step, which involves a more complex level of planning, best discriminated between patients and controls, and hence is reported and also used in further regression analysis.
Wisconsin Card Sorting Test (WCST): WCST measures concept formation, abstract reasoning, perseveration, and set shifting, which is the ability to shift cognitive strategies in response to changing environment. WCST consists of four stimulus cards consisting of one red triangle, two green stars, three yellow crosses, and four blue circles and a deck of 128 cards that are placed in front of the subject. The subject is told to take one card at a time from the deck and match it with the stimulus cards. Feedback is provided for each response as “correct” or “wrong” response. A raw score of the number of errors, perseverative responses, and the number of conceptual responses was taken for the analysis.
Stroop Color Word Interference Test: Stroop test is a test of response inhibition and is used as a primary measure of response conflict. The subject is asked to read the stimuli column wise as fast as possible. The time taken to read all the columns is noted. Next, the subject is asked to name the color in which the word is printed, and the time taken to name all the colors is noted down. Stroop effect was calculated by subtracting the time taken to read the words from the time taken to name the colors.
Object Sorting Test (OST) 30 : Indian adaptation of OST was administered to assess thought disorder, which refers to overlapping conceptual boundaries, concrete thinking, idiosyncratic associations, and symbolic thinking. The test comprises of 30 objects and has two phases: active and passive phase. The active phase has ten trials in which the subject is provided with a stimulus object and is told to add objects to the stimulus object to make a meaningful group and explain the principle behind it. The passive phase has 16 trials in which the examiner makes sort of the objects, and the subject is asked if the group is congruent or incongruent, and if congruent, what makes it so. The responses are classified as adequate, fused, impoverished, and peculiar. A response is scored as adequate when the concept used to explain the sort is adequate, and there is an appropriate fit between the verbalized concept and the sorted objects. A response is scored fused if multiple concepts or subconcepts are fused under a single response. The impoverished type is characterized by poverty of association and this score is given when the meaning ascribed to the sort is trivial and inconsequential. Peculiar concepts involve unrealistic or farfetched use of objects, dramatic contexts, idiosyncratic thinking, personal significance, and symbolization. Each response is classified into the appropriate category and the quantitative score is assigned as per the severity of the thought disorder. In this analysis, we have considered total peculiar scores and total impoverished scores. We have not included fused scores as they are mostly seen in patients with bipolar disorder. Higher peculiar and impoverished scores indicate thought disorder. 30 The protocol of each subject was first scored by the principal investigator and cross-checked by an experienced clinical psychology consultant (second author). The discrepancies in the scoring were discussed and the scores were finalized. This was done to reduce the subjectivity in the scoring. Inter-rater reliability by raters blind to the diagnosis was 0.78 for qualitative scoring and 0.90 for quantitative analysis. 30
Procedure
The study was carried out from September 2012 to April 2013 after obtaining clearance from the Institutional Ethics Committee. Subjects who consented to participate were recruited for the study and screened using MINI 5.0. SG was also assessed on GAF, SANS, and SAPS. Following this, both groups were assessed for EFs (selected tests of NIMHANS neuropsychological battery) and thought disorder (OST). The tests were administered in two sessions of 1 hour each on the same day, with a short break in between the sessions.
Statistical Analysis
Data were analyzed using Statistical Package for Social Sciences, Version 20.0. Armonk, NY: IBM Corp. On the Kolmogorov Smirnoff test, the variables were normally distributed. Scores of the performances on the neuropsychological tests are reported as mean and standard deviation. Group differences in scores were compared on Student’s t-test. Pearson’s product moment correlation was applied to assess the association between executive functioning and thought disorder in the SG.
Results
Sociodemographic Characteristics of the Two Groups
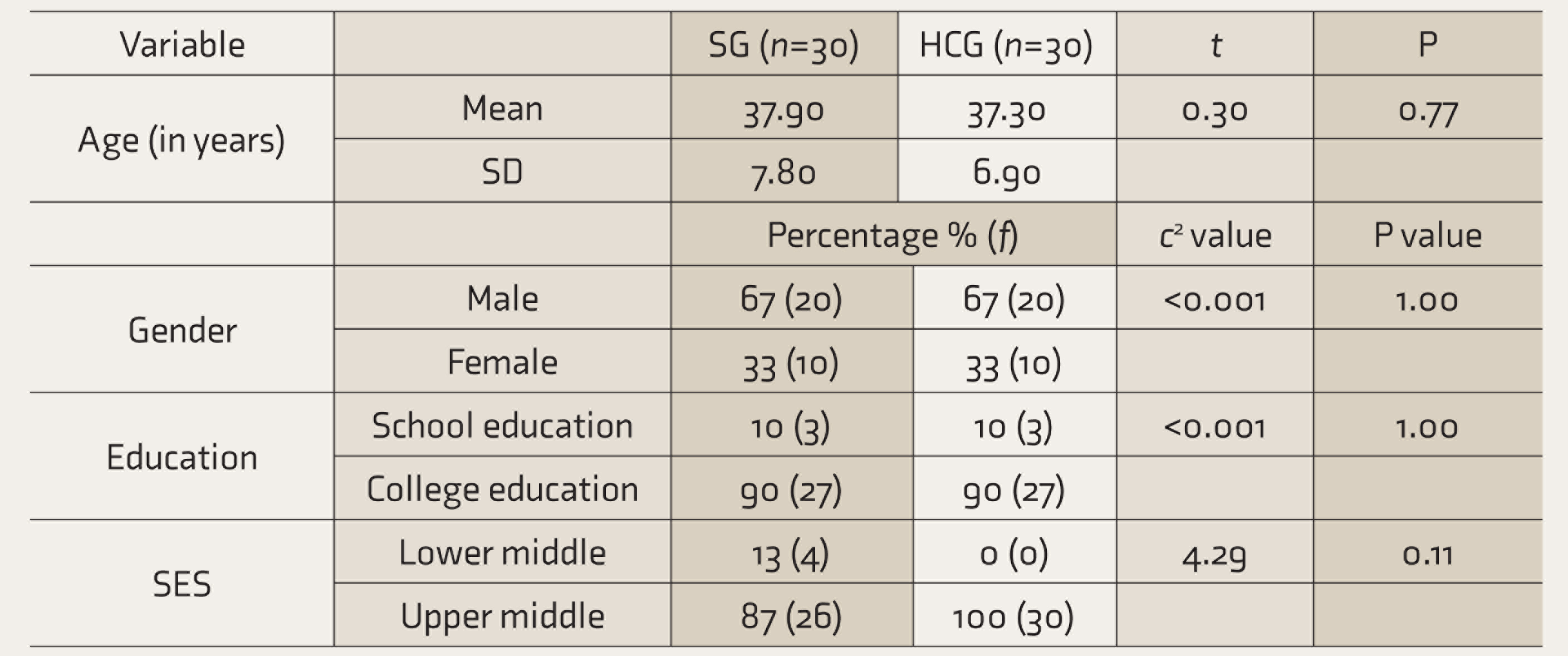
P ≤ 0.05 considered significant. SG, schizophrenia group; HCG, healthy control group; SES, socioeconomic status.
The SG had a mean ± SD duration of illness of 14.27 ± 6.04 years. The mean scores on SAPS and SANS were 23.6 ± 14.1 and 21.1 ± 12.9, respectively. The GAF measured at the time of assessment during the interview for sociodemographic pro forma was 42.33 ± 9.2, indicating moderate impairment in socio-occupational functioning.
All subjects were able to follow instructions and complete the OST tasks. The SG performed poorly on all scores of OST (both active and passive phase scores) (
Comparison of Performance on OST Between the Two Groups
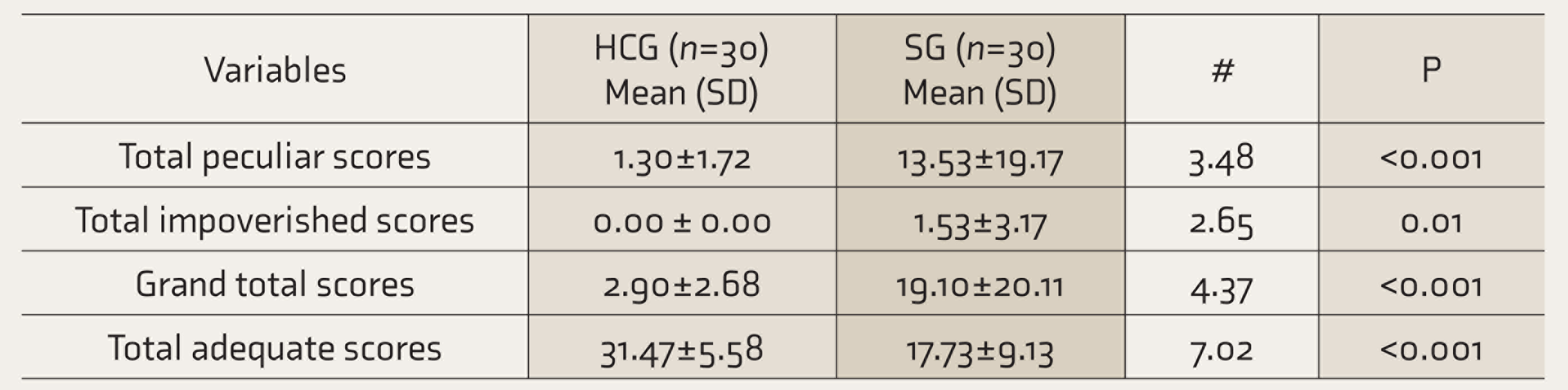
P ≤ 0.05 significant. # = t-test value. SG, schizophrenia group; HCG, healthy control group; OST: object sorting test.
Comparison of Performance on Tests of Executive Functions
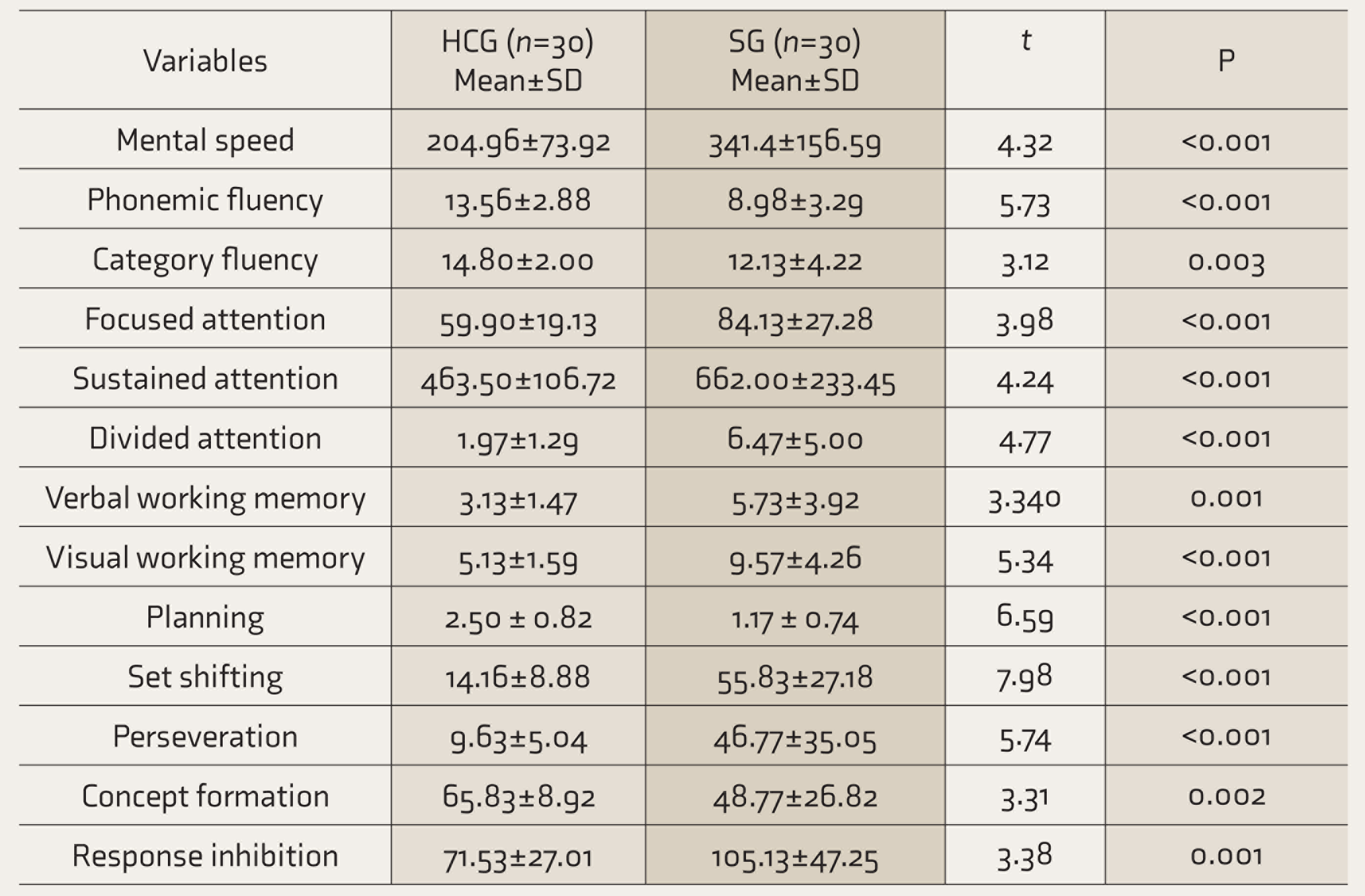
SG, schizophrenia group; HCG, healthy control group.
On Pearson’s correlation analysis (
Correlation Between Executive Functions and Thought Disorder in the SG
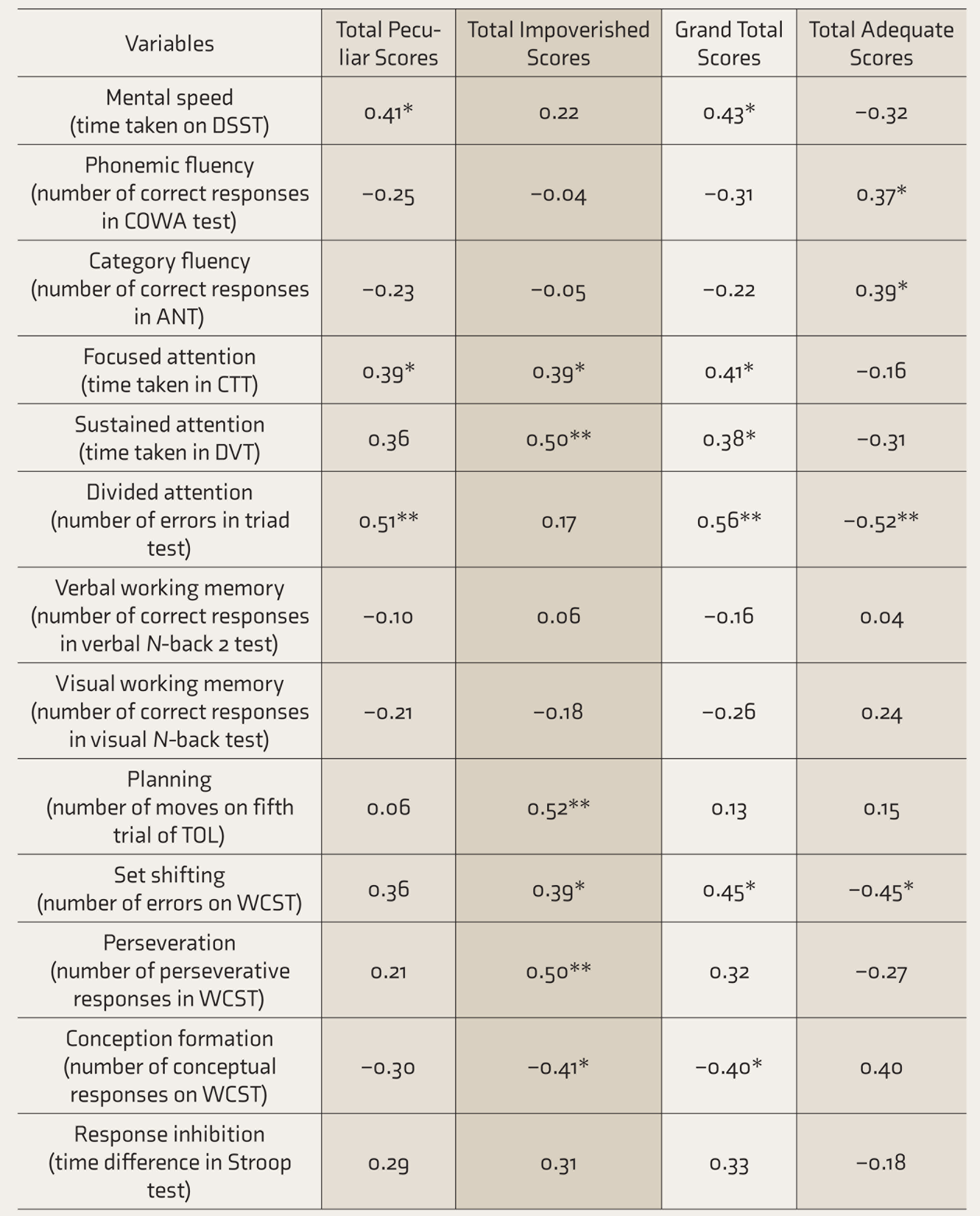
Significant Pearson’s correlation r values at *P ≤ 0.05, **P ≤ 0.01; n = 30. SG, schizophrenia group; DSST, digit symbol substitution test; COWA, controlled oral word association; ANT, animal name test; CTT, color trails test; DVT, digit vigilance test; TOL, tower of London; WCST, Wisconsin card sorting test. Time taken on all the tests was recorded in seconds.
Total impoverished scores on OST significantly correlated positively with the time taken on CTT (focused attention, P = 0.03) and DVT (sustained attention, P = 0.005), number of moves in fifth trial of TOL (planning, P = 0.004), and number of errors (P = 0.03) and number of perseverative responses on WCST (P = 0.005) and negatively with the number of conceptual responses on WCST (P = 0.02). For planning, only the fifth trial of TOL was used, as the first four tasks were easy and were successfully performed by most participants. The fifth step is complex and involves complex planning and, hence, only those final scores were considered.
Grand total scores of OST, which are the sum total of peculiar, impoverished, and fused responses, correlated positively with the time taken on DSST (mental speed, P = 0.02), CTT (focused attention, P = 0.02), and DVT (sustained attention, P = 0.04) and number of errors in triad test (divided attention, P = 0.001) and WCST (set shifting, P = 0.01) and negatively with the number of conceptual responses on WCST (P = 0.03).
Total adequate scores on OST, which is the total number of correct responses, correlated positively with the number of correct responses in COWA test (phonemic fluency, P = 0.04) and animal name test (category fluency, P = 0.03) and negatively with the number of errors in triad test (divided attention, P = 0.003) and WCST (set shifting, P = 0.01).
Stepwise linear regression analysis was carried out after controlling for age, duration of illness, and education. To test for collinearity, correlation coefficients and variation inflation factor (VIF) were examined. As the correlations between the variables did not exceed 0.8, tolerance values were less than 0.1, and VIF values were below 2, the relationships between the variables will not pose problems in the regression analysis. Regression analysis was carried out for total impoverished scores, total peculiar scores, and grand total scores separately (
Regression for Performance on OST as the Dependent Variable and Executive Functions as Predictors After Controlling for Age, Education, and Duration of Illness
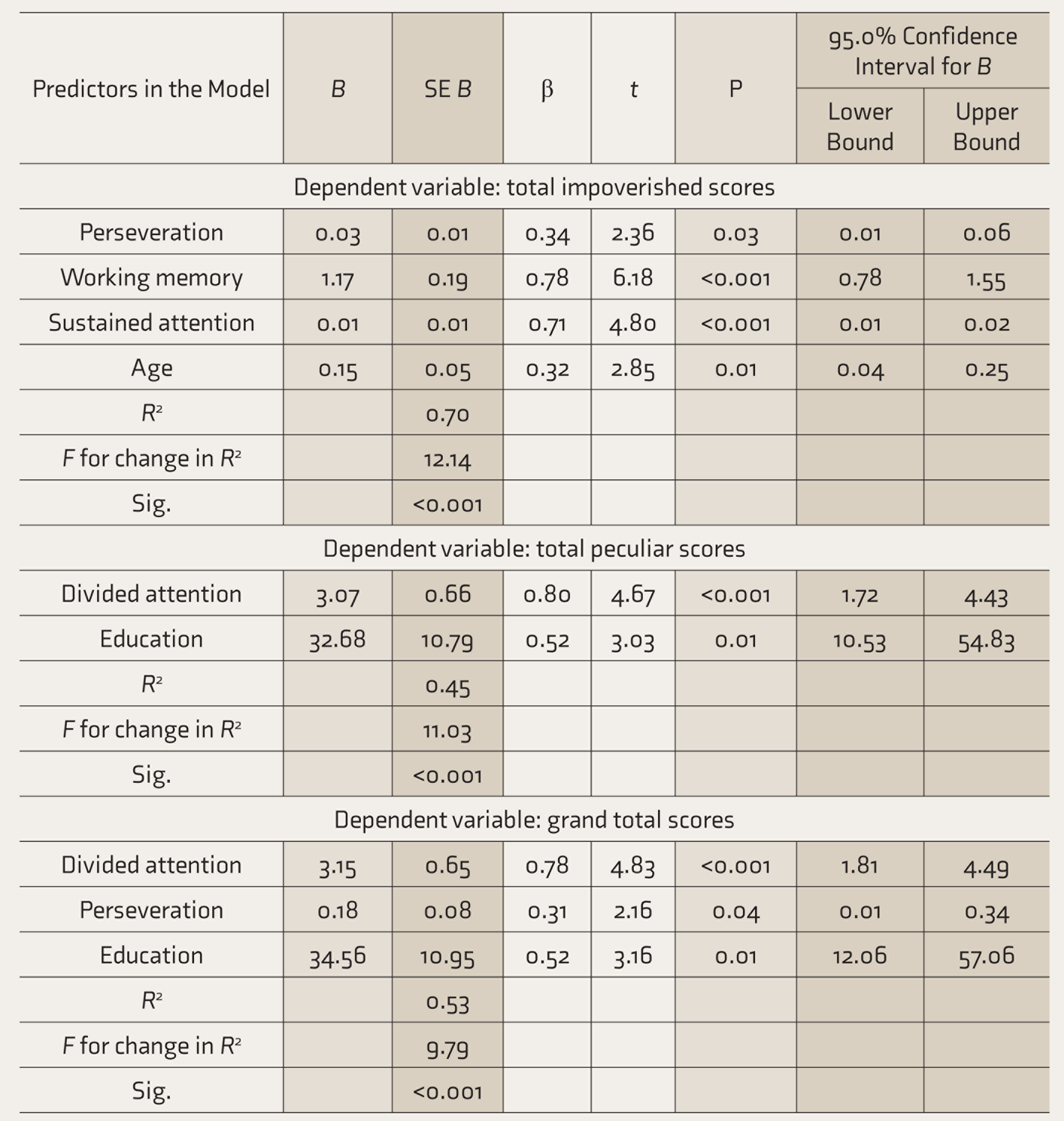
Stepwise linear regression. OST, object sorting test.
The results indicate that perseveration (b = 0.34, P = 0.03, 95% CI: 0.01 to 0.06), working memory (b = 0.78, P < 0.001, 95% CI: 0.78 to 1.55), sustained attention (b = 0.71, P < 0.001, 95% CI: 0.01 to 0.02), and age (b = 0.32, P = 0.01, 95% CI: 0.04 to 0.25) were independently associated with or predicted total impoverished scores on OST. R 2 for the model was 0.70, explaining more than half the variance of the impoverished responses. Total peculiar scores were associated with or independently predicted by divided attention (b = 0.80, P < 0.001, 95% CI: 1.72 to 4.43) and education (b = 5.2, P = 0.01, 95% CI: 10.53 to 54.83). Here, R 2 was 0.45, suggesting that 45% of the variance was explained by this model. Perseveration (b = 0.31, P = 0.04, 95% CI: 0.01 to 0.34), divided attention (b = 0.78, P < 0.001, 95% CI: 1.81 to 4.49), and education (b = 0.52, P = 0.01, 95% CI: 12.06 to 57.06) were independently associated with or predicted grand total scores on OST. R 2 for the model was 0.53, explaining more than half the variance of the grand total responses.
Discussion
Schizophrenia patients performed poorly on all domains of OST and neurocognitive functions as compared to the control group. There were significant correlations between variables of thought disorder as measured by OST and EFs, implying an association between thought disorder and EFs. Deficits in sustained attention and working memory and perseveration independently predicted impoverished responses, whereas divided attention independently predicted peculiar responses in SG. This suggests that performance on tests of neuropsychological functions may be differentially related to performance on OST. Further, grand total scores on OST (which is the sum of peculiar, impoverished, and fused responses) were predicted by deficits in divided attention and perseveration. As those patients with schizophrenia who performed poorly on tasks of attention, working memory, and perseveration also tended to exhibit thought disorder on OST, perhaps, the utility of OST can be extended beyond the assessment of thought disorder to be an indicator of deficits in EFs. Currently, OST is used as a part of diagnostic psychometry assessment, and since neuropsychological assessment is not carried out on all patients, perhaps, an inference about executive dysfunction can be drawn based on their performance on OST.
This study revisited the old construct of thought disorder as defined by Goldstein. 8 The study findings demonstrate that classical descriptions of thought disorder (deficits in concept formation and abstraction) are closely associated with cognitive deficits (executive dysfunction). This observation suggests that both thought disorder and executive dysfunction mirror similar constructs.
In the current scenario, with the emergence of the concept of “formal thought disorder,” which gives importance only to the form of thought by assessing the speech output, the original concept of thought disorder as an aberrant concept formation and concrete abstraction is being sidelined and OST has become an outdated tool. Although studies using the bizarre-idiosyncratic thinking rating system; abstract concrete rating system; and thought, language and communication scale as measures of thought disorder have found associations with attention, verbal memory, EFs, 20 the methods used for assessment of thought disorder have been largely language-dependent. 31 However, in the presence of negative thought disorder (impoverishment of content and speech), language-dependent assessments may not elicit the underlying core disturbances of aberration in concept formation and concrete thinking. 32 The tasks in the OST are not as language-dependent as other measures of thought disorder and may be better suited to assess these aspects of thought. The current study has attempted to review the original concept as well as extend the utility of the OST.
Executive dysfunction in schizophrenia includes problems with planning and is reflective of frontal lobe pathology. In the present study, we found that classical thought disorder, as measured through OST, is associated with several EF deficits, and hence, thought disorder as measured by OST may be a sign of executive dysfunction and, therefore, a reflection of frontal lobe pathology.
With the focus of contemporary classificatory systems on psychopathology, the evaluation for classical thought disorder has fallen out of favor in clinical assessments of schizophrenia. With our study observations, we would like to highlight that clinicians need to be aware of the importance of concept formation and abstraction to the clinical description of schizophrenia. The presence of this thought disorder may make the clinician aware of possible underlying cognitive dysfunction, with consequent implications for prognosis and planning rehabilitative strategies.
The strengths of the study are that we used Indian adaptation of OST suitable for use in our population, with established criteria as defined by Rapaport 10 in scoring the results. Neurocognitive tests standardized for use in the Indian population were administered. The study observations may have been influenced by the SG patients who had thought disorder as measured by OST and scored higher on all OST scores. The sample size of the thought disorder positive group in our study was small, and hence, we could not perform further subgroup analysis. However, the regression analysis suggests that the observed associations were significant. Given that there are hardly any reports in the literature studying the associations between performance on classical measures, such as OST and contemporary neuropsychological tests; these preliminary observations are encouraging. Nevertheless, these preliminary study findings need to be corroborated on a larger sample of patients with schizophrenia. Future studies may need to compare associations of performance in language-dependent tasks of formal thought disorder versus OST, with neuropsychological performance. These observations could be strengthened by evidence from neuroimaging studies examining underlying neurobiological substrates that mediate the influence of EF deficits on thought disorder.
Conclusion
This study demonstrated a significant association between thought disorder as measured by OST (concept formation and abstraction) and EFs. The study extends the utility of the OST tool beyond its current usage in psychometry; the pattern of responses in OST can point toward underlying executive dysfunction in patients with schizophrenia. Clinicians should be mindful of deviance in concept formation in schizophrenia as their presence may point to underlying cognitive deficits. Both thought disorder and executive dysfunction mirror similar constructs. This similarity represents a conceptual bridge between the classical and contemporary descriptions of the core deficits in schizophrenia.
Footnotes
Acknowledgments
We appreciate all who helped us in this research from Department of Psychiatry, Department of Clinical Psychology, and Department of Biostatistics, Manipal University, Manipal, India.
Data Sharing
Deidentified individual participant data will be made available in SPSSS format. The data will be made available upon publication to researchers who provide a methodologically sound proposal for use in achieving the goals of the approved proposal. Proposals should be submitted to sahithyabr@gmail.com
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.