
Abstract
Background:
Although personality disorders (PD) are known risk factors for suicide attempts, studies on personality dimension are scarce, which may provide further insights for interventions.
Methods:
The relationship between personality dimension, lethality, intent, and quality of life (QOL) was studied in suicide attempters with or without PD. We used the international personality disorder examination (IPDE) dimensional score, the scale for assessment of lethality of suicide attempt (SALSA), suicide intent scale (SIS), and WHOQOL-BREF QOL scale, to assess a sample of suicide attempters admitted to a general hospital.
Results:
PD was present in 43.2% and 57.9% of them had more than one PD. Comparison of attempters with or without PD suggested that the lethality of attempts and QOL were comparable, whereas self-reported suicide intent was significantly low in patients with PD. A higher proportion of PD patients reported relational problems as the reason for the attempt. The personality dimensional score was significantly higher for female attempters from urban backgrounds than for those with previous attempt histories. It was negatively correlated with the lethality of attempts and suicide intent.
Conclusion:
It is important to explore the personality dimension of the suicide attempters, along with PD, that may highlight additional risks and suggest the need for specific support.
Keywords
Although common, personality disorder diagnosis is often missed in suicide attempters, and many of them have more than one. Personality dimension was high in female, urban, and repeat attempters. Personality dimension was negatively correlated with suicide intent and lethality.Key Messages:
Suicide and suicidal behavior is a major public health concerns in India. 1 Suicide rates are increasing over the years in India, with a current prevalence of 12.4 per 100,000. 2 The National Mental Health Survey of India, 2015–2016, reported that 0.3% of participants had at least one suicide attempt in the past month. 1 However, this can be variable, 3 and reported 12-month to lifetime prevalence rates of suicide attempts have been 1% and 5.7%. 4 The magnitude of the issue can be highlighted by the fact that for every death by suicide in India, there are around 15 suicide attempts and over 200 persons with suicidality. 1 There are many studies about sociodemographic and clinical risk factors associated with suicide attempts in India5–7; however, there are only a few studies on personality disorder (PD), which is a known risk factor.8–10 Among PD, borderline PD with impulsive and aggressive traits is known to be at higher risk. 11 In essence, the presence of PD may make individuals more vulnerable to suicidal attempts and deaths.
Various personality characteristics have been associated with repeat attempts, for example, impulsivity and aggressiveness, and these might influence the intent and lethality of the attempts. Patients at risk of suicide have been observed to be socially introverted, depressed, and psychasthenic, with irritable, dysthymic, cyclothymic, and anxious temperament, even hysterical and schizoid. 12 In adolescents, personality traits such as impulsivity, identity diffusion, affective instability, aggressiveness, sadism, and perfectionism associated with borderline, antisocial, and narcissistic PD have been reported to be significantly associated with suicidal risk. 13
There are only a few studies from India that reported personality factors or disorders in suicide attempters.14–18 Some of these studies highlighted traits of impulsivity, aggression, and neuroticism. It appears that PD in suicide attempters has not been studied adequately in an Indian setup. It is plausible that, in many cases, PD is not diagnosed or missed. Identifying PD and associated vulnerability might open up therapeutic options, 10 and help prevent future attempts, improving the prognosis.
Although in the diagnostic systems, PD has been categorical, they are not truly dichotomous, as multiple traits overlap. There is an advantage of supplementing categorical diagnoses with dimensional information, which will reflect the intensity of personality issues. The dimension encompasses various characteristics described as facets within broader personality factors or traits that can be depicted in a continuum. Holistically, it takes into account all of the maladaptive and extreme traits and conveys the degree of personality pathology of the person. Most studies on risk factors of suicide attempt do not mention personality dimension as probably this is not specifically studied. The personality dimension, which is reflective of the intensity of personality issues, might provide additional information regarding suicidality and risk. To our knowledge, there is hardly any study on personality dimension, including from India, and our study intends to bridge the gap.
The international personality disorder examination (IPDE) dimensional score takes into account all the traits, including those that do not meet the criterion threshold required for a PD 19 and can present the personality pathology holistically. However, most previous studies have not considered the influence of the severity of personality pathology on suicide-related factors or outcomes. 8 It has been suggested that the severity of the PD might be more helpful in reflecting on the suicide risk than the specific PD diagnoses. 20 The personality dimensional score (PDS) might help to explore the relationship with other suicide attempt-related variables, for example, lethality, intent, etc. There are hardly any studies looking at these aspects.
In the above context, we intended to study the personality of the suicide attempters, including both personality diagnoses and the dimension, along with the relationship of personality with suicide intention, lethality of attempt, quality of life (QOL), and other clinical and sociodemographic factors associated with the suicide attempt.
Materials and Methods
Setting, Design, Duration
It was an observational and cross-sectional study conducted in a tertiary teaching hospital attached to a Medical College in Eastern India. Data collection was done over one year (September 2019 to August 2020).
Participants
All the consecutive patients of both genders, aged between 18 and 65 years, referred from medical, surgical, and casualty departments following suicide attempts, were included in the study. All suicide attempters were considered for participation in the study, irrespective of their physical or psychiatric disorders. The patients were not included if, following clinical evaluation, the injuries were considered to be accidental, with no suggestion of self-harm intention. Patients who died from their injuries were excluded. Acutely ill patients who could not participate in the study and those who were unwilling to participate in the interview or did not give valid informed consent were also excluded.
Recruitment
Information about the study was provided to the medical, surgical, and casualty departments emphasizing referral. The psychiatric assessments were conducted in the medical or surgical wards once patients were physically stable. Patients were seen on a one-to-one basis, and following their agreement, their history was also taken from their accompanying family caregiver. A detailed psychiatric history was taken, and a mental state examination was carried out. The assessments were carried out in at least two or more sessions, considering the length of the assessments; specifically, the IPDE interview was conducted in a separate session.
Measures
We used a predesigned questionnaire for the sociodemographic variables. The sociodemographic variables assessed were age, sex, domicile status, and family type, marital status, education, employment. We also collected information about the place, method, and reason for the suicide attempt and the history of any previous suicide attempt. We checked for any stressful life events or situations in the previous month. We specifically enquired about past psychiatric history, substance use, physical illnesses, and family history of mental illness and suicide.
The psychiatric diagnoses were based on the ICD-10 Classification of Mental and Behavioral Disorders, Diagnostic Criteria for Research, following a detailed clinical evaluation. 21
We assessed personality by IPDE. 19 The IPDE is an instrument for the clinical diagnostic assessment of PD. The IPDE comprises both a self-report screening questionnaire (59 True/False) and a separate semi-structured diagnostic interview (67 items). Following completion of the screening questionnaire, patients who have three or more positive answers in any PD category go through the interview. The scope includes the history from the informants. IPDE interview leads to either a definite, probable, or negative diagnosis for each PD. IPDE provides PDS based on the traits of each of the PD, irrespective of the presence of categorical PD diagnosis. 19 The PDS from each of the categorical PD categories was added to arrive at the person-specific total PDS, which would reflect the personality pathology of the individual holistically.
The lethality of the suicide attempts was assessed by the scale for assessment of lethality of suicide attempt (SALSA). 22 The SALSA is a clinician-rated scale with two components; the first component has four items (method of attempt, rescue possibility, physical outcome, and the level of medical intervention need), and the second component is the global impression of lethality, which is the overall view of the clinician about the lethality of a suicide attempt. All the items are scored from 1 to 5, with total scores ranging from 5 to 25, where higher scores suggest higher lethality. There is no cut-off score for the scale. 22
Suicide intent was assessed by the suicide intent scale (SIS). 23 The SIS has 20 questions, out of which 15 questions are included in scoring and have two parts. The first one (questions 1–8) covers the objective circumstances, actions, etc., related to a suicide attempt, and the second half (questions 9–15) covers self-report about the belief of the patient regarding his actions. The scores of 15–19 suggest low intent, 20–28 medium intent, and 29 or more suggest high intent. 23
We assessed the QOL using WHOQOL-BREF (Odia version).24,25 WHOQOL-BREF is a 26-item self-administered generic scale that measures four domains of QOL, which include physical health, psychological health, social relationships, and environment. Item number 1 is about overall QOL, and item 2 reflects satisfaction with health, and these are not considered within any specific domain. The items are scored from 1 to 5. Scores for each domain of the WHOQOL-BREF are arrived at by calculating the mean of all items included in each domain and multiplying by a factor of four. 25 The WHOQOL-BREF has been validated in the local language, Odia. 24
Statistical Analysis
The data was analyzed using SPSS version 28. Missing data was not included in the analysis. Chi-square tests analyzed the associations of categorical variables, Yate’s correction was done when necessary, and t-tests compared the differences in the means. We used Pearson’s correlation to assess the strength of the linear relationship between the variables with personality dimension. The threshold of statistical significance was at standard 0.05.
Results
A total of 71 suicide attempters were referred during the study. Out of them, 16 patients left the ward early against medical advice, and 11 patients did not agree to participate in the study, leading to the final sample size of 44 patients. There were 28 (63.6%) male and 16 (36.4%) female attempters in the sample with a mean age of 35.4 ± 14.04 and 25.6 ± 5.77 years, respectively (p < .05). The mean age of the sample was 31.9 ± 12.6 (range 19–65) years. The demographic details of patients with or without PD are given in Table 1. The mean age of attempters with PD diagnoses (30.5 ± 14.7 years) was not significantly lower than those without PD (32.9 ± 10.9 years).
Demographic Characteristics of Patients with and Without Personality Disorder.
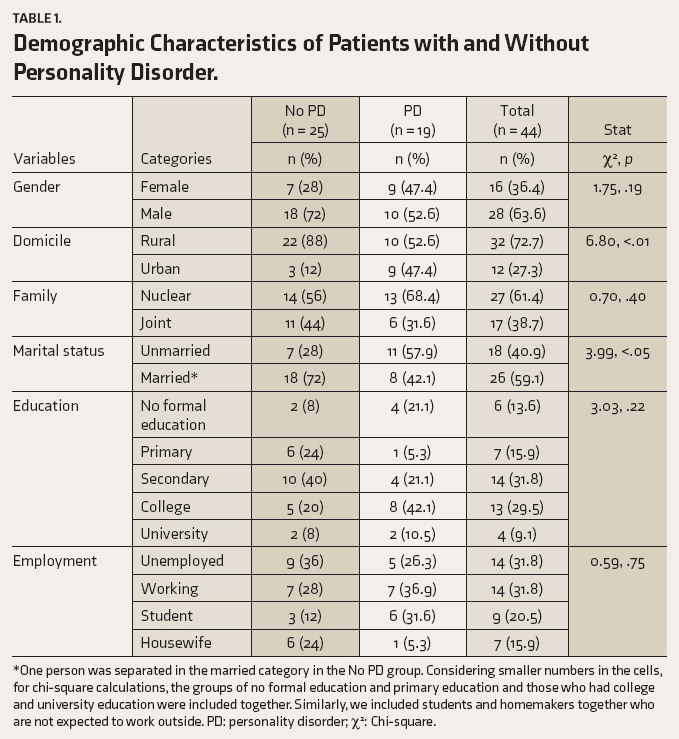
*One person was separated in the married category in the No PD group. Considering smaller numbers in the cells, for chi-square calculations, the groups of no formal education and primary education and those who had college and university education were included together. Similarly, we included students and homemakers together who are not expected to work outside. PD: personality disorder; χ 2 : Chi-square.
Clinically, 65.9% (29/44) of attempters (93.7% of female and 50% of male attempters) had psychiatric diagnoses other than PD. The overall prevalence of psychiatric illnesses in the sample, including PD, was 77.3% (34/44). We considered definite PD and probable PD diagnoses as one group for this study. There were 19 (43.2%, 95% CI: 28.4–58.9) patients with PD diagnoses; among these, 14 patients had definite PD and five probable PD. Many patients with PD had multiple PDs (11/19, 57.9%).
The proportions of patients with different PD diagnoses were paranoid (3, 6.8%), schizoid (2, 4.5%), dissocial (4, 9.1%), emotionally unstable impulsive (8, 18.2%), emotionally unstable borderline (13, 29.5%), histrionic (5, 11.4%), anankastic (3, 6.8%), dependent (1, 2.3%), unspecified (1, 2.3%), and none had anxious PD. Suicide characteristics of the two groups with or without PD are given in Table 2. There was no difference in family history of mental illness, suicide, or suicide attempt in two groups with or without PD. Proportions of attempters who reported physical illnesses were similar in both the groups with or without PD (4, 21.1% vs. 4, 16% respectively, p: .67). Similarly, proportions of attempters who had comorbid psychiatric illnesses with or without PD (14, 73.7%, vs. 15, 60.0% respectively, p: .34) were comparable.
Suicide Characteristics of Attempters with or Without Personality Disorder.
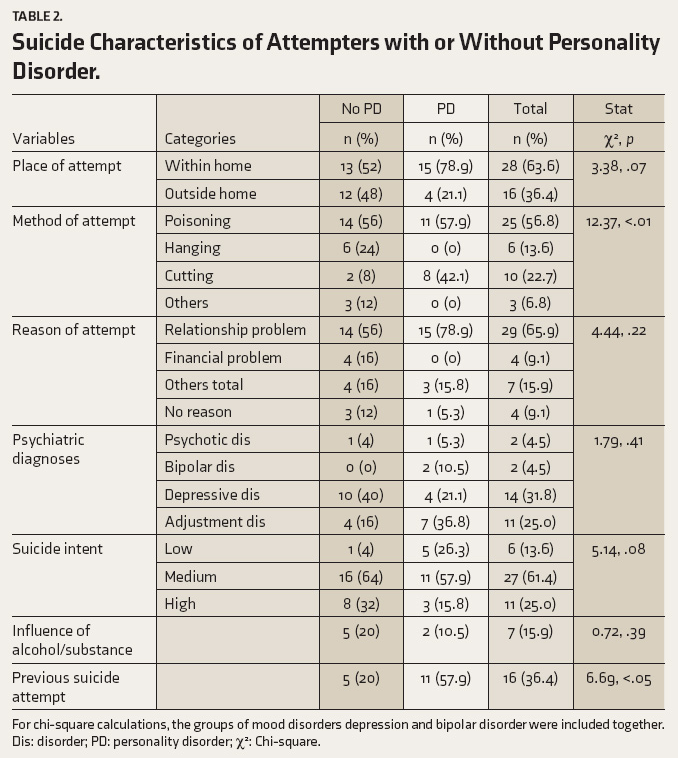
For chi-square calculations, the groups of mood disorders depression and bipolar disorder were included together. Dis: disorder; PD: personality disorder; χ 2 : Chi-square.
Suicide intent, lethality, PDS, and QOL for attempters with or without PD are given in Table 3. WHOQOL-BREF score for overall QOL (2.95 ± 0.97 vs. 2.92 ± 1.1) and health satisfaction (3.2 ± 1.2 vs. 3.3 ± 1.2) did not differ between attempters with or without PD, respectively.
Comparison of Suicide Intent, Lethality, Quality of Life, and Personality Dimension of the Attempters with or Without Personality Disorder.
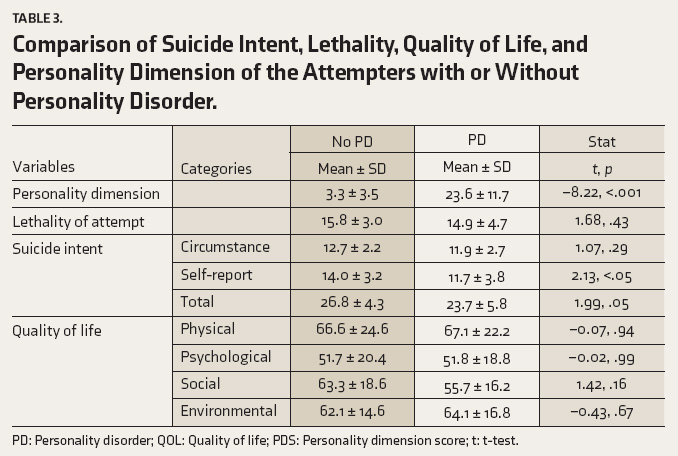
PD: Personality disorder; QOL: Quality of life; PDS: Personality dimension score; t: t-test.
PDS (range: 0–52, mean: 12.04 ± 12.95) was significantly more in female compared to male attempters (18.1 ± 16.8 vs. 8.6 ± 8.7, p < .05, respectively); urban versus rural (22.5 ± 16.0, vs. 8.1 ± 9.1, p < .001); unmarried versus married attempters (17.7 ± 14.6 vs. 8.2 ± 10.3, p < .05) and those with history of previous suicide attempt (19.2 ± 14.1 vs. 8.0 ± 10.5, p < .01). PDS of patients who attempted at home approached statistical significance compared to that outside (14.8 ± 14.1 vs. 7.2 ± 9.3, p: .59); the attempts under the influence of substance had considerably low PDS (5.7 ± 6.8 vs. 13.2 ± 13.5, p: .16) although it was statistically not significant.
Patients with previous suicide attempt history had significantly higher PDS (19.2 ± 14.1 vs. 8.0 ± 10.5, p < .01); they were significantly younger (26.9 ± 7.5 vs. 34.7 ± 14.1, p < .05), had lower lethality (SALSA score) (13.6 ± 4.1 vs. 16.6 ± 3.3, p < .05), and lower intention based on the circumstance (SIS score) (11.4 ± 2.6 vs. 13.0 ± 2.1, p < .05).
Intent, lethality, and PDS in various demographic and clinical groups were studied. The mean lethality score of the sample based on SALSA was 15.1 ± 3.8 (range 7–21). The mean intent score (SIS all items) was 25.5 ± 5.2 (range 15–37), which could be categorized as low (13.6%), medium (61.4%), and high (25.0%) intent. Male attempters had significantly higher suicidal intent based on SIS total score (26.8 ± 4.2 vs. 23.1 ± 5.98, p < .05) and self-report (13.9 ± 3.1 vs. 11.6 ± 4.1, p < .05) compared to female attempters. Attempters with physical morbidities had significantly higher suicidal intent (SIS total score: 28.8 ± 5.4 vs. 24.7 ± 4.9, p < .05).
We assessed the correlation of PDS with age, QOL (WHOQOL-BREF score), suicide intent (objective, self-report, and total score of SIS), and lethality (SALSA score) (Table 4).
Correlation Among Age, Intent, Lethality, Quality of Life, and Personality Dimension.
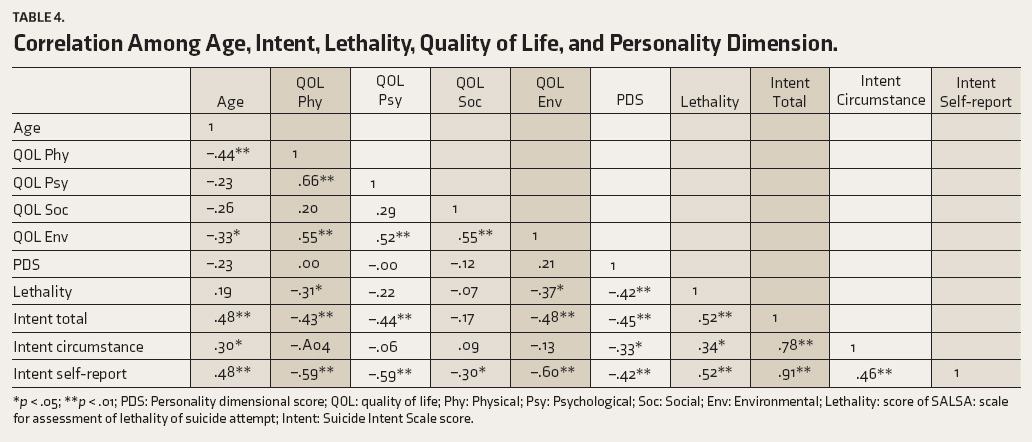
*p < .05; **p < .01; PDS: Personality dimensional score; QOL: quality of life; Phy: Physical; Psy: Psychological; Soc: Social; Env: Environmental; Lethality: score of SALSA: scale for assessment of lethality of suicide attempt; Intent: Suicide Intent Scale score.
Discussion
To our knowledge, this is the first study from India exploring PD and personality dimension, and their relationship with intent, lethality, and QOL in a group of suicide attempters admitted to a tertiary level of care. There are a few interesting findings related to PD and personality dimension. A considerable proportion of suicide attempters had PD; the most common type was emotionally unstable PD. A significantly higher number of attempters with PD had a previous history of suicide attempts. There were no differences between lethality and QOL; however, suicide intent based on self-report was significantly low in PD patients. The PDS was significantly negatively correlated with lethality (SALSA) and suicide intent reflected by the circumstance, self-report, and total score of SIS.
In this study, a considerable proportion (43.2%) of suicide attempters had PD, and more than half of them (57.9%) had more than one PD. A previous study using IPDE reported a slightly higher prevalence of 52%, 15 whereas clinical assessment-based studies in India reported lower figures of around 2%–7.6% of suicide attempters having PD.6,17,26,27 Studies on adolescents with suicidal ideas and behavior reported PD prevalence figures of 19.5%–22.8% (29.6%–42.1% in autopsy studies) 13 ; even as the personality pathology was emerging.
While there are many studies about the suicidality of patients with PD in India, it is surprising that only a few studies explored PD through detailed assessments of suicide attempters. There is a possibility that routine clinical evaluations in general hospitals set up after suicide attempts do not include detailed evaluation of PD and might miss diagnoses of PD, suggesting a need for in-depth assessments that may help in the diagnosis process. Considering such a high prevalence of PD, it appears relevant to use at least a PD screening routinely and further evaluation of screen-positive patients.
In our sample, the most common type of PD was emotionally unstable PD, which included impulsive and borderline; followed by histrionic and dissocial PD. While borderline PD has been mostly reported with suicide attempters attending emergency departments, 28 studies do report other PD such as dissocial PD. 29 Indian studies reported borderline and dependent, 30 anankastic, and histrionic PD 26 in suicide attempters. While the type of PD, especially those with impulsivity and borderline traits, would remain relevant for suicide attempts, changing diagnostic approaches for PD in ICD-11, 31 personality dimension or the severity of PD might be more useful to assess.
As expected, the PDS of the patients with a PD diagnosis was significantly higher in the studied sample. PDS was significantly higher in women, although the proportions of PD diagnoses in both genders were comparable. Women are known to have a higher risk for suicide attempts, 32 however, the ratio is probably changing. 33
The PDS was also significantly higher in attempters from urban backgrounds, which had a higher proportion of attempters diagnosed with PD. This urban-rural difference deserves further study, as India’s demography has changed rapidly with urbanization in recent years. It would be interesting to explore whether personality concerns are more evident in an urban context.
PDS was significantly negatively correlated with lethality, although lethality in general did not differ between attempters with or without PD. This suggested that the higher the severity of personality pathology, the lower the lethality of the suicide attempt; however, its clinical relevance needs to be studied further. Similarly, PDS was also significantly negatively correlated with suicide intent based on circumstance, self-report, and total SIS score. This would suggest that the higher the personality pathology, the lower the intent. This is clinically relevant as patients with higher PDS may have self-harmed for different reasons than having the intent to die.
It was observed that repeat attempters had significantly higher PDS. In addition, a significantly larger proportion of PD patients had previous attempts compared to attempters with no PD. This re-emphasizes the observations of PD being a risk factor for repeat attempts. 34 It has been reported that attempters with severe PD had more frequent attempts than those with simple PD or patients with no PD. 20 The above observations suggested that higher PDS is linked to lower lethality and lower intent but with a higher risk for repeat attempts.
Overall QOL, health satisfaction, and various domains of QOL did not differ between attempters with PD and without PD, and the PDS did not correlate with QOL. The suicide attempters probably had comparable QOL, and the presence of PD did not make any appreciable difference; nonetheless, the lack of correlation between PDS and QOL deserves further exploration.
The method of attempt in patients with or without PD had considerable variations, as none of the patients with PD attempted by hanging. At the same time, self-poisoning was comparable, and higher proportions of PD patients used cutting. In our study, there was a significant correlation between suicide intent and the lethality of the suicide attempt. A similar positive correlation has been reported between these two entities35,36; however, this relationship has been debatable, as no relationship has also been reported. 37 However, suicide intent categories were not significantly different, but the suicide intent scores based on self-report were significantly low in PD patients, and the total score approached statistical significance. There was no difference in the lethality of suicide attempts between the two groups with or without PD. It may be highlighted that the self-reported suicide intent was low in attempters with PD, but the overall lethality of the attempts was comparable between the groups. This may be clinically relevant to reflect that although the intent and lethality correlated positively, self-report of low intent may be observed where the lethality was comparable.
A higher proportion of PD patients (78.9% vs. 56.0% of non-PD) reported relational problems as the reason for the attempt. Interpersonal issues are a key problem area in patients with PD, and in general, a considerable proportion of suicide attempts and suicides are linked to relational problems.6,16,38 This should be a focus area of assessment and intervention for suicidal patients.
It would be pertinent to highlight sociodemographic and clinical variables about PD and PDS among the attempters. There were no differences in age, gender, education, and employment of suicide attempters with or without PD. However, more attempters with PD were female and of lower age. These were not statistically significant. Similarly, significantly more unmarried attempters had PD diagnosis and significantly higher PDS. Although single status in relationships has been linked to suicide attempts, 39 specifically for men 40 ; it needs further study about its association with PD or PDS alongside suicidality.
Proportions of patients with physical or psychiatric morbidities in both PD and no PD groups were comparable. The overall prevalence of psychiatric disorders in the sample was comparable to reported figures for suicidal patients in India.17,41 Depression and adjustment disorder are commonly reported diagnoses in suicide attempters. 42 In our study, depressive disorders were present in 21.1% of patients with PD and 40% of patients without PD. Although psychiatric diagnoses were common in both groups, adjustment disorder, rather than depression, was more common in PD patients. It highlights the relevance of stressful life events, including those of relational problems that may lead to adjustment disorders, which could precipitate suicide attempts.
The study has a few limitations. This is a single-center study with a relatively smaller sample size. Considering the sample, the results can be generalizable to attempters admitted to hospitals rather than to all suicide attempters. Future studies may look into the personality dimension in a larger multi-centric sample covering different levels of healthcare systems, including community samples, which might help to make the sample more representative. There was no comparison group; assessment of PD in other patients admitted for different reasons to the hospital could have helped to explore its specific association with suicide attempters. The study did not explore all the factors that may be influenced by personality, such as the number of previous attempts.
Conclusion
A considerable proportion of suicide attempters in this study had PD, most commonly the emotionally unstable type, and the findings re-emphasized PD as a risk factor in the Indian context. Besides PD, PDS emerged as a relevant factor with additional information that might be helpful in assessing suicide attempters. PDS was considerably more among female attempters and those who had previous attempt histories. PDS was significantly negatively correlated with the lethality of the attempt and suicide intent. This suggested that suicide risk assessment may routinely contain a method to rate personality issues and severity. The study findings also suggest the need for specific assessment and appropriate supportive measures relevant to personality pathology in suicide attempters.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
We thank S.C.B. Medical College and Mental Health Institute, Cuttack to facilitate the study; The Institute of Insight, United Kingdom and Quality of Life Research and Development Foundation (QoLReF), India; for the additional support in conducting the study.
Data Availability Statement
Data will be shared on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the use of Generative AIs
Nil.
Ethical Approval
Full name and institution of the review committee, and the approval number: S.C.B. Medical College, Cuttack, India. (No: 236/Dt: 26/08/2020)
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
All participants provided written informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.