
Abstract
Background:
Clinical training in traditional medical education often needs more translational value, especially for in-service MBBS doctors working in primary health centers (PHCs), who provide first-line treatment for psychiatric disorders. To address this gap, a psychiatrist-led personalized mentorship program incorporating three live consultation-driven training (CDT) methods was developed to integrate psychiatric care into PHCs.
Methods:
The authors designed and implemented a personalized mentorship program using three CDT methods tailored for in-service MBBS doctors. The CDT methods were applied through live consultations to facilitate real-time, real-life learning and integration of psychiatric care into primary health settings. Data from published articles and manuals on CDT methods were collected, focusing on their descriptions, effectiveness, principles, and advantages over traditional classroom training.
Results:
Data indicate the effectiveness of the CDT methods to translate to real-life skills (translational quotient). The personalized mentorship program showed promising results in enhancing the confidence and competence of MBBS doctors in managing psychiatric disorders in PHCs. The CDT methods were found to be superior to traditional classroom training in terms of practical applicability and real-time learning.
Conclusion:
The psychiatrist-led personalized mentorship program with CDT methods demonstrates the potential for significant improvements in the training of in-service MBBS doctors, facilitating the integration of psychiatric care into PHCs. These methods offer a practical and effective approach to bridging the gap in clinical training and can be replicated among medical students and residents across various medical and surgical specialties. Further research and longitudinal studies are recommended to validate these preliminary findings and explore the program’s broader applicability.
Keywords
Traditional medical education often lacks practical training, especially in a real-life scenario involving consecutive patients and live consultation from entry-to-exit. This is particularly true for MBBS doctors in primary health centers managing psychiatric disorders, necessitating innovative approaches. Personalized mentorship programs using live consultation-driven training methods can significantly enhance doctors’ confidence and competence in real-time psychiatric care.Key Messages:
In medical education, a gap exists between training and real-life clinical practice. Despite the best outcome of doctors in their real-time practice, medical education traditionally often relies on theory-rich training methods, such as classroom lectures, 1 simulated scenario (case conferences), or idealistic models (e.g., bedside teachings), that may not accurately reflect the complexities of actual patient consultations. As a result, various indirect or proxy clinical training methods have emerged to compensate for this deficiency. However, these methods may need to prepare trainees adequately for the realities they will face in practice. 2
Furthermore, there is a discrepancy between the idealistic approach taught in medical education—emphasizing comprehensive examinations—and the pragmatic approach often adopted by practicing physicians, which prioritizes time management, effective communication, and focused examinations tailored to each patient’s needs and cost-effectiveness. For instance, while the idealistic approach dictates that every patient undergoes a comprehensive examination regardless of necessity, the reality demands a more focused and efficient medical interview and examination, especially considering time constraints in settings like busy government hospitals in India.
Jacob et al. 3 and Gangadhar 4 highlight a long-standing gap between traditional psychiatric training and real-world clinical demands, emphasizing the need for innovative approaches that integrate practical experience. Current training methods, relying on post hoc teaching, need to capture the nuances of real-time consultations, leading to a disconnect from practical skills such as time management and effective communication. Existing methods rely heavily on simulations, which may need to fully prepare trainees for the diverse challenges of actual patient encounters. Each consultation is unique, requiring exposure to real clinical practice.
Cutrer et al. 5 illustrate how integrating wisdom and clinical reasoning in medical practice enhances outcomes, underscoring the potential for live consultation-driven training (CDT) in psychiatry to improve practical skills and decision-making simultaneously. The current training methods fail to adequately address the dynamic nature of patient consultations and fail to provide trainees with the necessary skills to navigate these challenges effectively.
To address this, the authors designed and implemented three innovative live CDT methods in psychiatry for in-service primary care doctors (PCDs) in government-run primary health centers (PHCs). These methods are on-consultation training (OCT), collaborative video consultation (CVC), and the Acharya training method. These innovative methods revolutionize psychiatry training for MBBS doctors and have the potential for broader application in medical education. This article describes their design, implementation, and effectiveness.
Methods
The authors collected data from the aforementioned three innovative training methods in their own published articles in scientific journals and manuals available in the public domain. These training sessions are conducted with the informed consent of the patients and/or their family members. The descriptions of training methods are summarized in the “Results” section. The details of implementations of these training methods are also reviewed. The data on the effectiveness of these training programs, especially of the translational quotient (an innovative outcome measure in live real-life outpatients of PHC), are also reviewed and summarized. Data were collected from published articles and did not involve any new studies with human or animal subjects performed by any of the authors. Therefore, ethics committee approval was not required.
Results
On the basis of findings from published articles, the authors briefed this result section about each training method, followed by implementation sites of these specific training methods. They then presented effectiveness data of individual versus combined training methods.
Descriptions of Training Methods
On-consultation Training
As the name suggests, training occurs through the live consultation of doctors with their real consecutive patients (without any selection bias of the patients). Here, a trainer psychiatrist and trainee doctor sit together, and the trainer psychiatrist trains trainee PCDs in live consultation of the outpatient primary care clinic with minimal disruption to regular clinical workflow. This contrasts with traditional classroom training as it exposes trainees to live, hands-on clinical scenarios. 6
The OCT can be conducted either at a trainee (in situ) or trainer (ex situ) live clinic. Suppose the trainer trains the trainee in the trainee’s real outpatient clinic. In that case, it is referred to as “in situ” because it is the best place where trainees can be trained, that is, trainee PCDs are trained in their real-world consecutive general patients, not in psychiatric patients, that too in his/her live clinic. If the trainer trains the trainee in a real outpatient clinic, it is referred to as “ex situ” because the trainer clinic is still not the best place, that is, the trainer clinics are often colored with specialty-oriented psychiatric patients, which is beyond the reality of the trainee general clinics.
Collaborative Video Consultation
As the name suggests, a trainer psychiatrist provides a video consultation on demand to the trainee doctors for their selected patients. It functions like a tele-referral or second opinion clinic of a specialist doctor. However, simultaneously, specialist trainers and trainee doctors conduct consultations in real-time with the real patients of trainees. The author initially implemented an appointment-based CVC.7-9 However, it was not a successful model in view of the inherent longer waiting period extended up to 36 hours for remote patients in India who often fail to show up for appointments, especially rural patients. Hence, the authors later transformed to instant collaborative video consultation (iCVC), where the specialist trainers would see trainee doctors’ patients immediately on their video call, which would avoid waiting time for trainee doctors and their patients. In the end, even though the specialist trainer sees their patients, the final call of the outcome of consultation lies with trainee doctors. 6
Acharya’s Training Method (the STD Training Method)
Originally called the See-, Try- and Do-it-yourself (STD) training method,6,10 the authors later renamed it “Acharya Training Method” owing to its resemblance to the ancient Indian tradition of highly skilled educators known as “Acharyas” (means experts). Acharyas are revered as a preceptor and expert instructors who impart advanced specialized skills. The authors adopted the term “Acharya” to signify proficient and seasoned psychiatrists who served as individual mentors and coaches, overseeing trainees throughout their real-life clinical responsibilities and guiding them to translate theory into practice, thus bridging the knowledge–clinical practice gap. The Acharya method aims to make trainees independent practitioners in their real-life clinics.
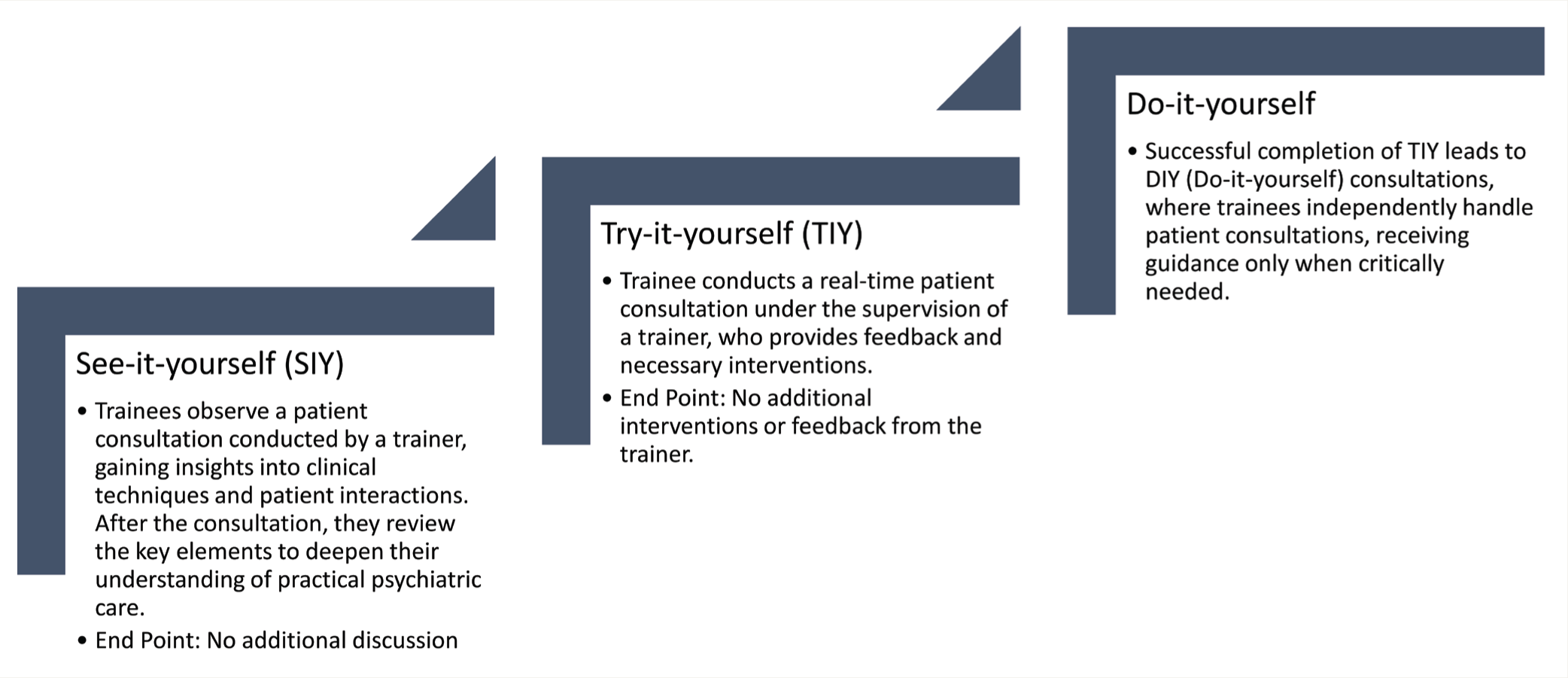
The Acharya method involves three sequential supervised training/learning steps: see-it-yourself (SIY), try-it-yourself (TIY), and do-it-yourself (DIY). By virtue of its inherent nature, the Acharya method has been conducted in the live OCT method. In SIY consultations, a trainer psychiatrist first conducts his/her live outpatient consultation. At the same time, trainee doctors observe every process of the consultation of the trainer psychiatrist from the patients’ entry-to-exit. This training method exposes the trainee doctors to the complexity of real-life clinical scenarios. After consultation with each patient, the psychiatrist and trainee doctors discuss the process involved in providing consultation, including communication skills, interview technique, screening questions, examination, diagnostic process, prescription, and counseling. Next, in sequence, after a few SIY consultations, the trainer psychiatrist encourages trainee doctors to try to do real-time consultations in front of the trainer psychiatrist (TIY consultations). The trainer psychiatrist will interfere whenever needed to achieve the desired consultation outcome. After a few TIY consultations, trainee doctors are allowed to conduct their DIY consultations in front of a trainer psychiatrist, where the trainer gives advice and corrects whenever absolutely needed. Once desired results repeatedly come in during most consultations, the trainer will come out of the trainee consultation room to make him/her an independent practitioner. 10
Please note here that, overall, the Acharya training method encourages trainees to learn the process of consultations with trainers without changing the personal style of consultations of trainee doctors. This pioneering initiative in India blends ancient teaching methods in modern clinical medicine in two variants: in-person and remote training using digital technology. Figure 1 summarizes the sequential steps of the Acharya method.
The Sequential Steps of Acharya Method.
The Implementation Details of Training Methods
On-consultation Training
Though the authors began with the in-person mode, with the rapid development of telemedicine, in-person training was converted to the telemedicine mode using the hub-and-spoke telemedicine model (popularly called tele-OCT). In-person OCT was implemented first in Gauribidanur taluk in 2014–2015, 6 now ongoing with doctors of BBMP area and Belur taluk of Karnataka, and now planned for Munisiyari taluk of Uttarakhand (NAMAN Project), as well as Tarikere and Holalkere taluks of Karnataka. Tele-OCT is implemented successfully in the states of Uttarakhand, 11 Bihar, and Karnataka.10,12 Tele-OCT is highly acceptable to PCDs and reasonable to implement in Indian rural PHCs.6,12
Instant Collaborative Video Consultation
iCVC has been implemented successfully in Bihar, Uttarakhand, Chhattisgarh, and Karnataka.11,13
Acharya Method (the STD Training Method)
Originally, the authors introduced the STD training method within the Karnataka Tele-mentoring and Monitoring (KTM) program as part of the Train the Trainer (TOT) initiative. 10 Subsequently, it was expanded to encompass all OCT sessions, serving as a direct training method for trainees. It is worth noting that the OCT module for each doctor consists of three sessions conducted at 0-, 3-, and 6-week intervals.6,12 These three sequential sessions have largely transitioned into STD methods: the first session focuses on observation (see-it-yourself), the second session encourages hands-on practice (try-it-yourself), and the third OCT session emphasizes independent application (do-it-yourself). 14
Effectiveness of Training Methods
As part of the formative assessment of the diploma in primary care psychiatry course, OCT sessions have been conducted thrice at intervals of 0, 3, and 6 weeks, and at least 25 CVCs are mandatory to qualify for the final examination. These provide the opportunity to continue learning with PCDs. 6
The authors designed a concept called “translational quotient” (TQ), an innovative outcome parameter to assess the effectiveness of these innovative training methods. The TQ of a training program can be defined as “the ability of a training program to translate learned/taught knowledge into clinical skills required for use during the busy routine clinical practice.” 6 The TQ was assessed via video streaming of live, real-time general outpatient consultations in their PHCs (in situ). In a study, the TQs were assessed in live Tele-OCT evaluative sessions by a telepsychiatrist for each PCD at 6 and 9 months after the initiation of the course. The telepsychiatrists have working experience in primary care psychiatry and need to be specifically trained for the particular PCD to become assessors of the TQ of that PCD. Evaluation criteria included elicitation of psychiatric symptoms using the screener of clinical schedules of primary care psychiatry, 15 clinical reasoning for psychiatric diagnosis, decision-making regarding psychiatric medications, components covered in brief patient counseling, time management for psychiatric evaluations at the primary care level, and overall clinical psychiatric skills. Each criterion was scored from 1 to 5, with a total score ranging from 6 to 30. The study found that the average TQ scores obtained in the first and second Tele-OCT evaluations, similar to clinical examinations but conducted during real-time consultations, were 70.33% and 76.33%, respectively, suggesting adequate TQ at 6 and 9 months into the course. 16 In another study, the effectiveness of Tele-OCT is assessed by diagnostic concordance of CVC between PCDs and telepsychiatrists, which was 83%, with a kappa agreement of 0.77 (P < .001)..11
Discussion
The central features of these CDT methods are that they are live, in situ, point of care, and personalized. A trainer psychiatrist provides training through live, real-world consultations within the regular outpatient clinic of the trainee doctor (in situ) on a one-to-one basis (personalized) while simultaneously giving live consultations to their real patients of PHCs (point of care). The uniqueness of CDT is its intensity, flexibility, and adaptability while achieving dual outcomes (training and consultations with patients happen simultaneously) with each patient encounter. Within this framework, training and consultation occur simultaneously with each patient, emphasizing the importance of time management. CDTs are especially effective for fostering critical thinking skills, addressing complex issues, and meeting the specific needs of individual trainees during real-world consultations, all under the direct supervision of trainer psychiatrists.
The following principles are incorporated into CDT methods:
6
Personalized mentorship: An exclusive trainer psychiatrist trained each trainee in a one-to-one format contrary to the group format of classroom training. Live, real-time consultations: CDT occurs in live, real-time consultations with real patients of PHCs. The entry-to-exit (E2E) consultation approach covers the complexity of each consultation. Each patient is different and poses different challenges. Pragmatic training with minimal disruption of PCDs’ clinical work. Each consultation would last for about 5–10 min, which is the maximum a PCD can spend time in their regular consultations in India. In situ (on-the-spot) in PHC itself versus ex situ at tertiary care medical college: In situ CDTs are conducted in general patients, exposing trainees to their own consultations, whereas ex situ CDT might expose trainees to specialty consultations. In situ CDT eliminates selection bias in general patients. A bottom-up approach where trainers reach out to trainees in their real-world PHC outpatients. Principles of adult learning (Andragogy).
1
Bi-directional learning: Psychiatrists will train PCDs, and PCDs will also provide inputs regarding nonpsychiatric patients to the telepsychiatrist. Practice-based learning is incorporated.
The authors acknowledge that ideally the effectiveness of each training method should be evaluated in real-world scenarios independently. However, because of the naturalistic design of the one-year Diploma in Primary Care Psychiatry course for in-service MBBS doctors, 6 the authors assessed the effectiveness of combined training methods at various time intervals. Preliminary findings indicate that both individual (Tele-OCT) and combined (Tele-OCT and CVC) approaches show effectiveness, as evidenced by innovative outcome parameters such as TQ.
The authors believe that this development heralds a new paradigm in medical education, extending its benefits to medical students and residents across various specialties. They suggest that even in surgical disciplines, the introduction of on-procedure training akin to OCT could be valuable. This innovation is seen as a catalyst for a paradigm shift in Continuing Medical Education (CME) for practitioners across specialties, particularly in surgical fields.
Future Directions
A systematic assessment of the effectiveness of individual CDTs is to be carried out. Replication studies among medical students and psychiatry residents are needed to assess the effectiveness of CDTs in tertiary care medical institutes.
Conclusions
Authors have introduced pioneering live CDT methods in medical education as personalized mentorship programs. These CDTs are tailored for the training of psychiatry among in-service PCDs working in government PHCs. Initial findings suggest that CDTs are showing promising results. This approach holds the potential for replication among medical students and residents across various specialties.
Supplemental Material
Supplementary material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
AI tools were used in the preparation of this manuscript. Specifically, OpenAI’s ChatGPT was utilized to assist in writing, structuring, and editing portions of the text. We assume full responsibility for the entire content of the manuscript, including the parts generated with the help of the AI tool.
Ethical Approval
Ethics committee approval was not required for this study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent from patients were taken.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.