
Abstract
Background:
Mental health integration into primary healthcare is pivotal in addressing mental, neurological, and substance use disorders in India. Community Health Officers (CHOs) and Mid-Level Health Providers (MLHPs) play a critical role in providing mental health services at the grassroots levels. Despite existing training modules, gaps persist in implementing sustained, practical training programs. This study evaluated the effectiveness of in-person mental health training combined with tele-mentoring for CHOs and MLHPs in Telangana and Tripura.
Methods:
A mixed-method cross-sectional approach was employed. In-person training was delivered to 66 participants in Telangana and 396 in Tripura, covering theoretical modules, interactive sessions, and role plays. Pre- and post-assessments evaluated Knowledge (K), Attitude (A), and Practices (P). Instant Collaborative Video Consultations (CVCs) supported participants for three months post-training. Quantitative data were analyzed using paired t-tests, while thematic analysis was applied to qualitative data from focus group discussions and feedback.
Results:
Statistically significant improvements in KAP scores were observed in both states (p < .01). The CVC model facilitated real-time support, with 91.84% of patients being first-time mental health service users. Substance use disorders (31.25%) and common mental disorders (27%) were the most identified conditions. Participants appreciated the interactive training design and recommended ongoing support.
Conclusions:
The integration of in-person training with tele-mentoring effectively enhanced CHOs’ and MLHPs’ capacity to deliver mental health services. Scaling this model nationally, supported by continuous mentoring, could significantly improve community mental health outcomes.
Keywords
In-person training combined with tele-mentoring improves CHOs’ and MLHPs’ skills in delivering mental health services. Instant, live, Collaborative Video Consultations (CVCs) provide ongoing support for mental health service users. Scaling this integrated model nationwide can strengthen mental health care in primary health settings.Key Messages
India faces significant mental health challenges with limited services available. Strengthening primary health care (PHC) with better screening and professional training is essential to address these needs. The National Health Policy 2017, along with the Ayushman Bharat Program (ABP) launched in 2018, emphasized the importance of Ayushman Arogya Mandhir (AAM), previously known as Health and Wellness Centers (HWCs), in delivering comprehensive primary healthcare (cPHC) services. One enhanced service package under HWCs includes screening and basic management of Mental, Neurological, and substance use disorders, highlighting the government’s commitment to holistic PHC strengthening. 1
Community Health Officers (CHO) and Mid-Level Health Providers (MLHP) in AAMs play a crucial role in this framework by shifting service delivery from a doctor-centric model to a team-based approach. 2 The institutionalization of the CHO and MLHP roles, with legal recognition and defined prescription rights under the National Medical Commission Act of 2019, marks a significant step in enhancing mental health services at the grassroots level. 1 The integration of mental health services into the PHC setup offers multiple advantages, such as reducing stigma, improving access to care, and facilitating better identification of psychiatric disorders among patients with other physical illnesses. 3 This integration can reduce dependency on tertiary care and improve follow-up for mental health patients. 4
Several mental health training programs have been implemented for primary care doctors and other healthcare providers, employing various modes such as onsite, online, and hybrid methods. For instance, the Chhattisgarh Community Mental Healthcare Tele-Mentoring Program (CHaMP) uses a combination of onsite training, eLearning, and Collaborative Video Consultation (CVC) to train Primary Care Doctors (PCDs) and Rural Medical Assistants (RMAs). 5 Similarly, the “Diploma in Primary Care Psychiatry” (DPCP) and other task-shifting initiatives have demonstrated the efficacy of digitally driven training programs in improving mental healthcare delivery at the primary level.6–8 Concerning CHOs, although the MNS (Mental, Neurological, and Substance Use) module exists, they have not been fully translated into an implementable training program. Another noteworthy initiative is the TORENT (Tele-mentoring for Rural Health Organizers of Chhattisgarh) program, which aims to train Regional Health Officers (RHOs) digitally, and the training sessions cover both basic and advanced mental health concepts over 12 sessions each. 9
These training programs have shown promise in enhancing the mental health literacy of healthcare workers, improving their ability to identify, manage, and refer patients with mental health disorders. Moreover, specialized training initiatives, such as utilizing digital technology for ongoing engagement, highlight the potential of innovative approaches in mental health care. 10 However, most often they lack continuous support and follow-up, which are critical for sustaining the skills and knowledge acquired. 11 Despite the promising potential of CHOs and MLHPs to improve the recognition and management of mental disorders, comprehensive training is absent, and sustained handholding compromises the long-term effectiveness of such initiatives. 12
This study will contribute to the growing body of evidence on the importance of continuous professional development for CHOs and MLHPs in the context of mental healthcare, particularly in the resource-constrained and culturally diverse states of Telangana and Tripura. To address the unique challenges posed by these settings, including stigma, a pressing need exists for in-person mental health training programs and continuous tele-mentoring through CVC to equip CHOs and MLHPs with the necessary skills and knowledge to provide effective services. In this context, this study aims to explore the impact of hybrid training (in-person mental health training combined with handholding through CVC) for CHOs and MLHPs in India.
The primary objective is to evaluate the changes in Knowledge (K), Attitude (A), and Practices (P) of CHOs and MLHPs, as well as the overall impact on community mental health outcomes. Secondary objectives included the effectiveness of this CVC-integrated in-person training model in improving mental health service delivery at AAMs (HWCs).
Methods
Ethical Considerations
The study was approved by the Institutional Ethics Committee (IEC) (Approval No. NIMHANS/43rd IEC (BEH.SC.DIV) 2023, dated December 8, 2023) and registered with the Clinical Trial Registry of India (Registration No. CTRI/2024/02/062906). Verbal informed consent was sought from all participants, including the CHOs, MLHPs, and patients. This study employed a mixed-methods cross-sectional design to evaluate the impact of in-person mental health training combined with CVC on CHOs and MLHPs in India, specifically in the states of Telangana and Tripura. We used the STROBE cross-sectional checklist when writing our report, and it is uploaded as “STROBE Complete Checklist.” 13
Setting
The in-person training sessions were held in Hyderabad for Telangana and Agartala for Tripura, as requested by the respective states. CVCs were taken on a virtual video conferencing platform. In the CVC module, video consultations were conducted by a Mental Health Professional (MHP), such as a Psychiatrist, Clinical Psychologist, Psychiatric Social Worker, or Nursing Officer. The MHP was available during working hours and for emergencies to provide advice and support. CHOs discussed selected patients after using the Mental Health Screening and Counseling Tool [MERIT] to determine treatment plans, referrals, or resolve screening issues. After each CVC, the MHP recorded clinical data in a proforma, including the key learning points.
Participants
The In-person training in Telangana for CHOs and MLHPs took place in two batches, spanning over two days with 15 hours of training per batch in January and March 2024. The training was carried out for 66 trainees from the State of Telangana, representing all the districts nominated by the state. The In-person training in Tripura for CHOs and MLHPs took place in two batches, spanning over two days with 15 hours of training per batch in July and August 2024. The training was carried out for 396 trainees from Tripura in 2 batches, representing all the districts nominated by the state. Participants included all CHOs and MLHPs nominated by state health authorities. Those who missed training sessions were excluded (Figure 1).
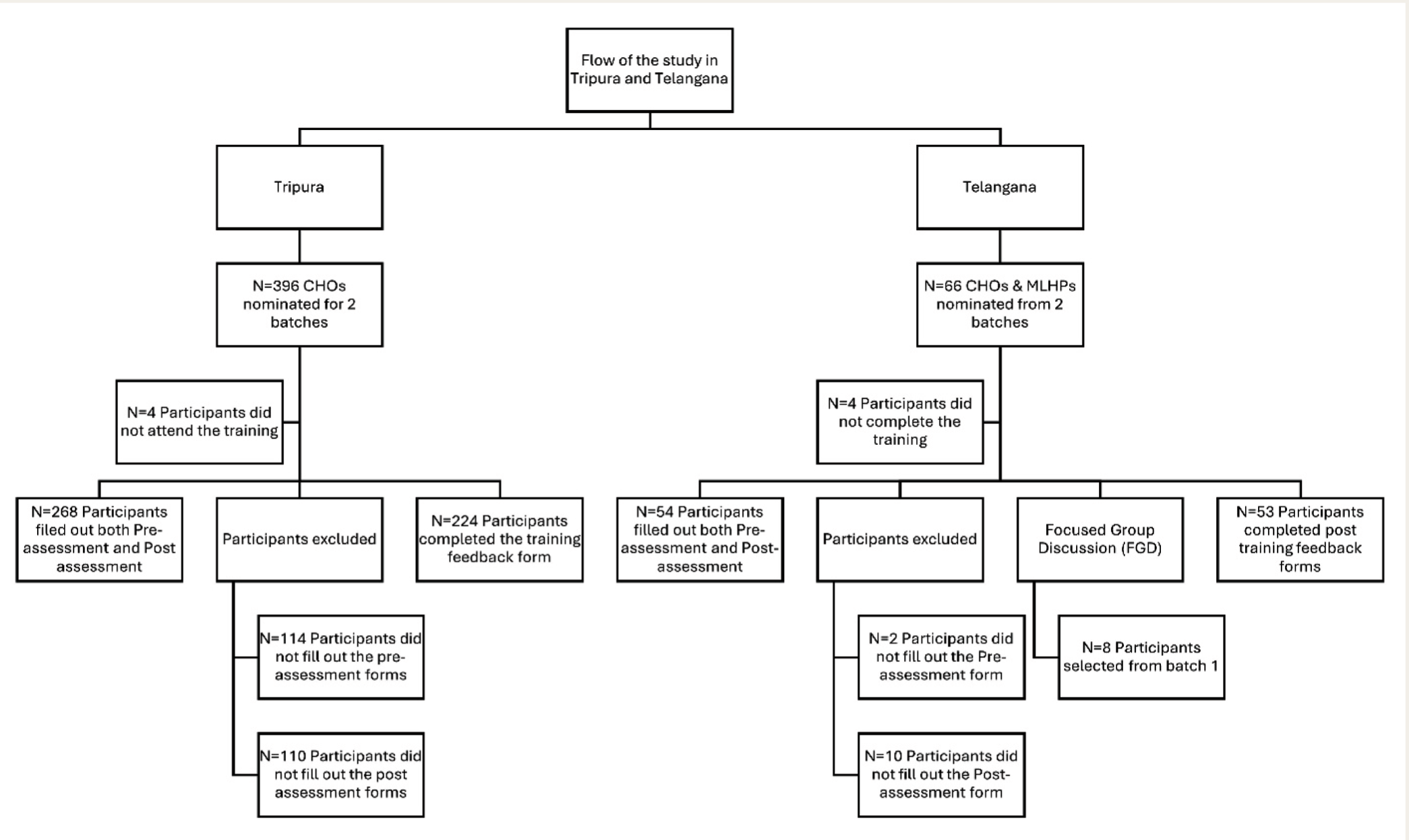
CHOs: Community health officers, MLHPs: Mid-level health providers.
Training Curriculum
The training module included a comprehensive curriculum, including both theoretical and practical modes. The theoretical training mode included didactic lectures, case-based group discussions, and interactive question-and-answer sessions. Practical mode of training included hands-on learning experience through role-plays and case scenarios.
Training Modules for CHOs and MLHPs
In line with the MNS Training Module.
Orientation to various signs and symptoms of mental illness and application of the MERIT Screening Tool. 14
Common mental disorders (CMDs): Depression and suicidal risk assessment and management
CMDs: Generalized anxiety disorder, panic disorder, and somatization disorder
Severe mental disorders (SMDs)
Substance use disorders (SUDs): Alcohol and tobacco addiction
Pandemic, disaster preparedness, Tele-MANAS, and Collaborative Care-District Mental Health Program (DMHP)
Data Collection
Quantitative Data
Pre-assessments and post-assessments were completed by the trainees before and after the in-person training sessions, respectively, which assessed the Knowledge (K), Attitude (A), and Practices (P) related to training content. Pre and post (KAP) questionnaires were shared through WhatsApp before and after training, after obtaining informed consent. A structured assessment tool was developed based on established mental health guidelines and literature. It was validated by two senior psychiatrists in the team. The tools comprised multiple-choice questions and case-based scenarios to evaluate CHOs’ baseline understanding of CMDs, SMDs and SUDs. Continuous supportive handholding was done with the help of instant Collaborative video/audio consultations extending up to 3 months post-training. Eligible participants who have attended 2 days of the training sessions, who have filled out both pre- and post-assessments, and who have done at least one Collaborative video/audio consultation were awarded certification of completion of the training program. A feedback form was sent to the participants who completed the training.
Qualitative Data
For the batch 1 participants from the state of Telangana, an Online Focused Group Discussion (FGD) was carried out post-training to obtain feedback from the participants. The FGD included an interview guide including questions and probes about the structure, methods of training, and other challenges faced. Participants were selected through a purposive sampling method to represent a sample of CHOs and MLHPs who attended the in-person mental health training. The faculty in charge had vetted these discussion points, and further training sessions were initiated accordingly for batch 2. The FGD was audio- and video-recorded and transcribed verbatim. Anecdotes from feedback forms were collected about the program’s training.
Data Analysis
Quantitative Data
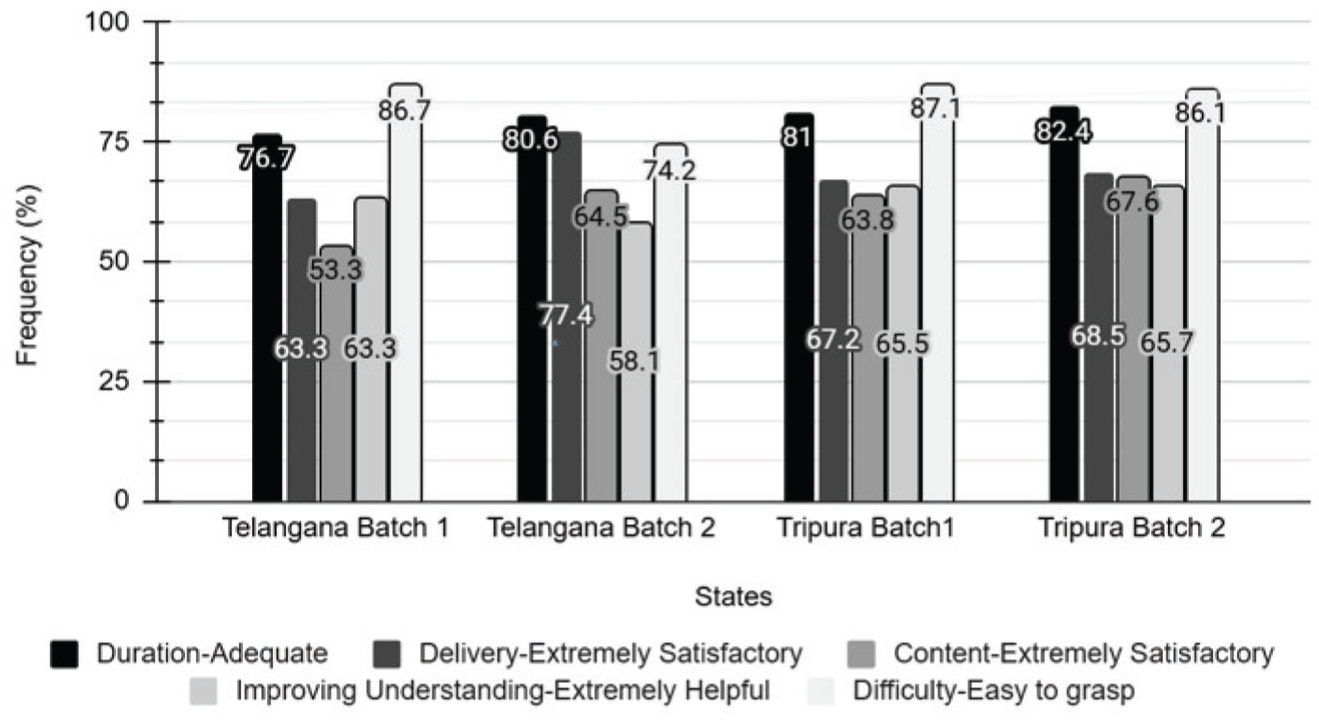
Participant demographics across the states are analyzed through descriptive statistics. Paired t-tests were used to compare pre- and post-training KAP scores for both states. Descriptive Statistics were employed to analyze CVC data and participant feedback forms (Figure 2). The SPSS licensed version 29 was used to analyze the quantitative data. This included performing descriptive statistics and inferential statistics (t-test). 15 Participants with missing data were excluded from paired analyses.
Participants’ Feedback Frequencies Regarding the Training.
Qualitative Analysis
Thematic analysis was conducted on the FGD transcripts and feedback forms. Audio recordings of the FGD were transcribed using Turboscribe software. Data were manually coded, sub-themes and themes were identified, and the findings were interpreted as per the Braun and Clarke Inductive Thematic analysis. 16
Results
The study involved CHOs nominated by Telangana (66 participants) and Tripura (396 participants). A total of 54 participants from Telangana and 268 participants from Tripura completed both pre- and post-training assessments and were included in the paired KAP analysis. These numbers reflect participants who filled out both the pre- and post-assessment forms. In contrast, 2 participants in Telangana and 114 in Tripura did not complete the pre-assessment, while 10 in Telangana and 110 in Tripura did not fill out the post-assessment forms. These participants were excluded from the paired analysis. The mean age of CHOs was 30.4 years in Telangana and 31.2 years in Tripura. Gender distribution in Telangana showed 35 males (57.3%) and 26 females (42.6%). In Tripura, there were 144 males (36.7%), 247 females (63%), and one participant (0.2%) who preferred not to specify their gender.
The pre- and post-KAP score improvements were observed in both Telangana and Tripura. The mean KAP score difference was statistically significant in both states (p < .01) (Table 1).
Pre KAP and Post KAP Scores of CHOs and MLHPs from Telangana and Tripura.
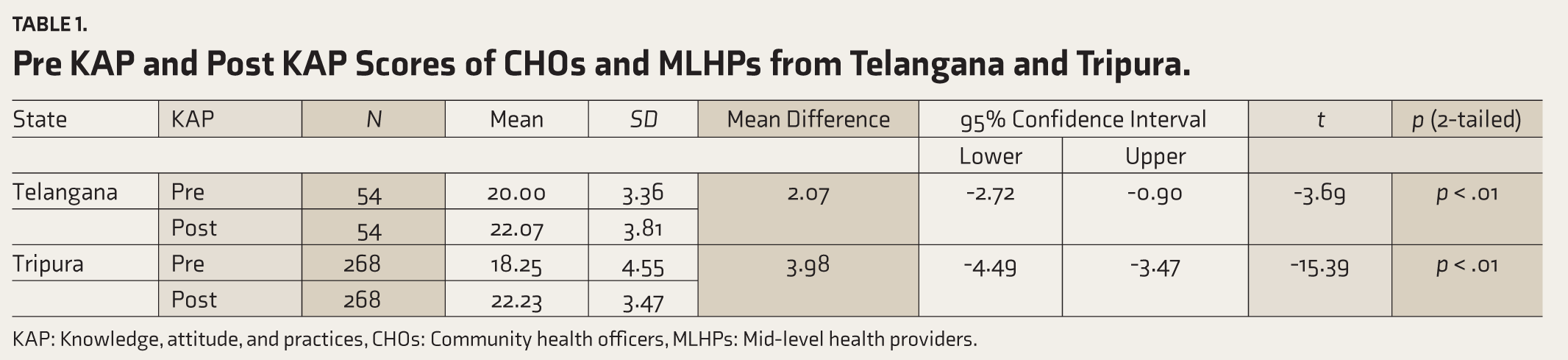
KAP: Knowledge, attitude, and practices, CHOs: Community health officers, MLHPs: Mid-level health providers.
The majority of the patients were first-time visitors (91.84%), and the patient demographic showed a predominance of adults aged over 18 years (97.9%), with a slight male population (62.5%) (Table 2).
Socio-demographic Characteristics of the Patients Taken Through CVC for Both Telangana and Tripura.
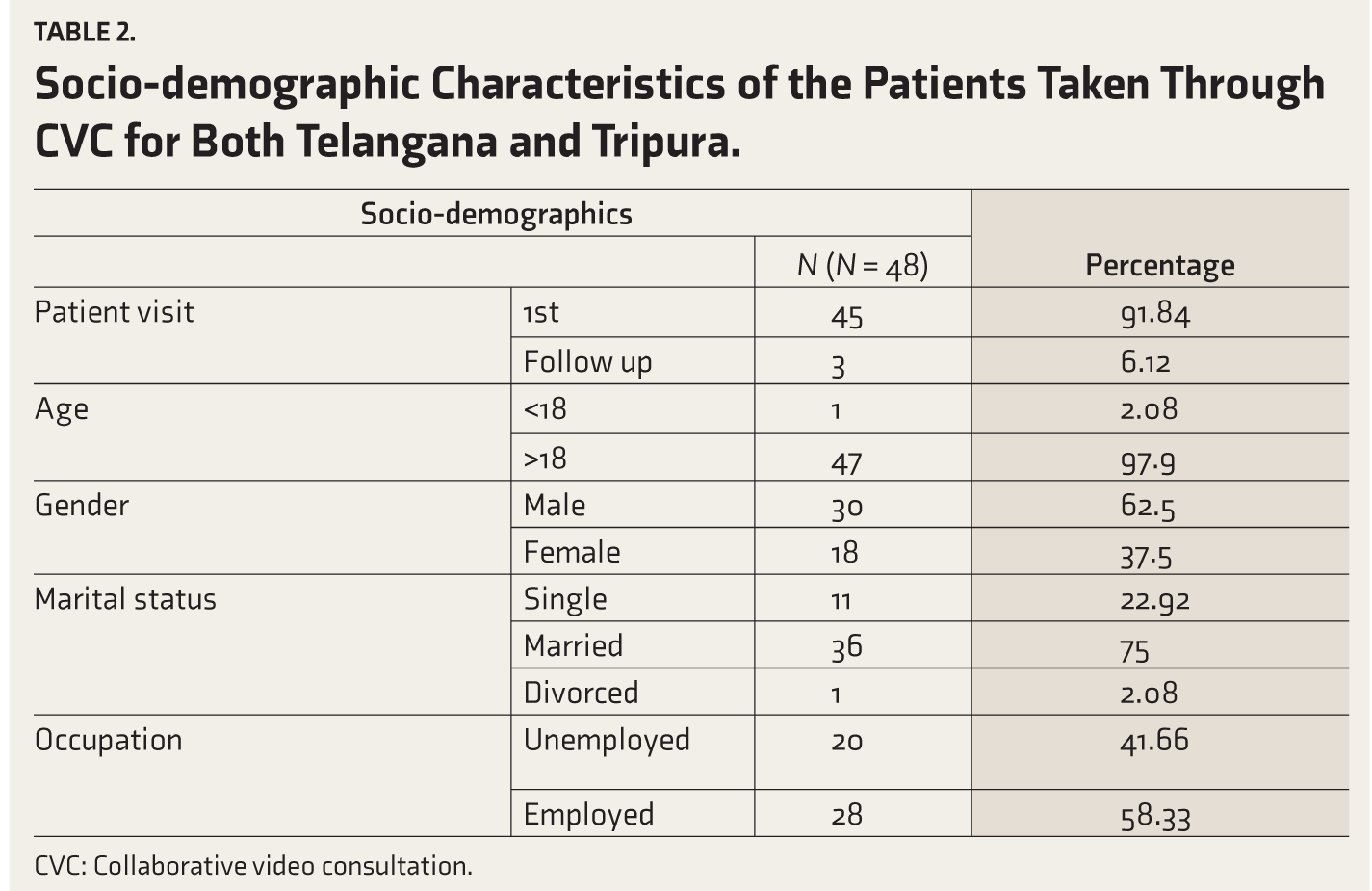
CVC: Collaborative video consultation.
In terms of diagnostic categories, most patients screened positive for substance use disorders (SUDs), specifically alcohol dependence (31.25%), followed by CMDs, including depression and anxiety (27%) (Table 3).
Clinical Impression Made by MHPs on CVC with CHOs and MLHPs.
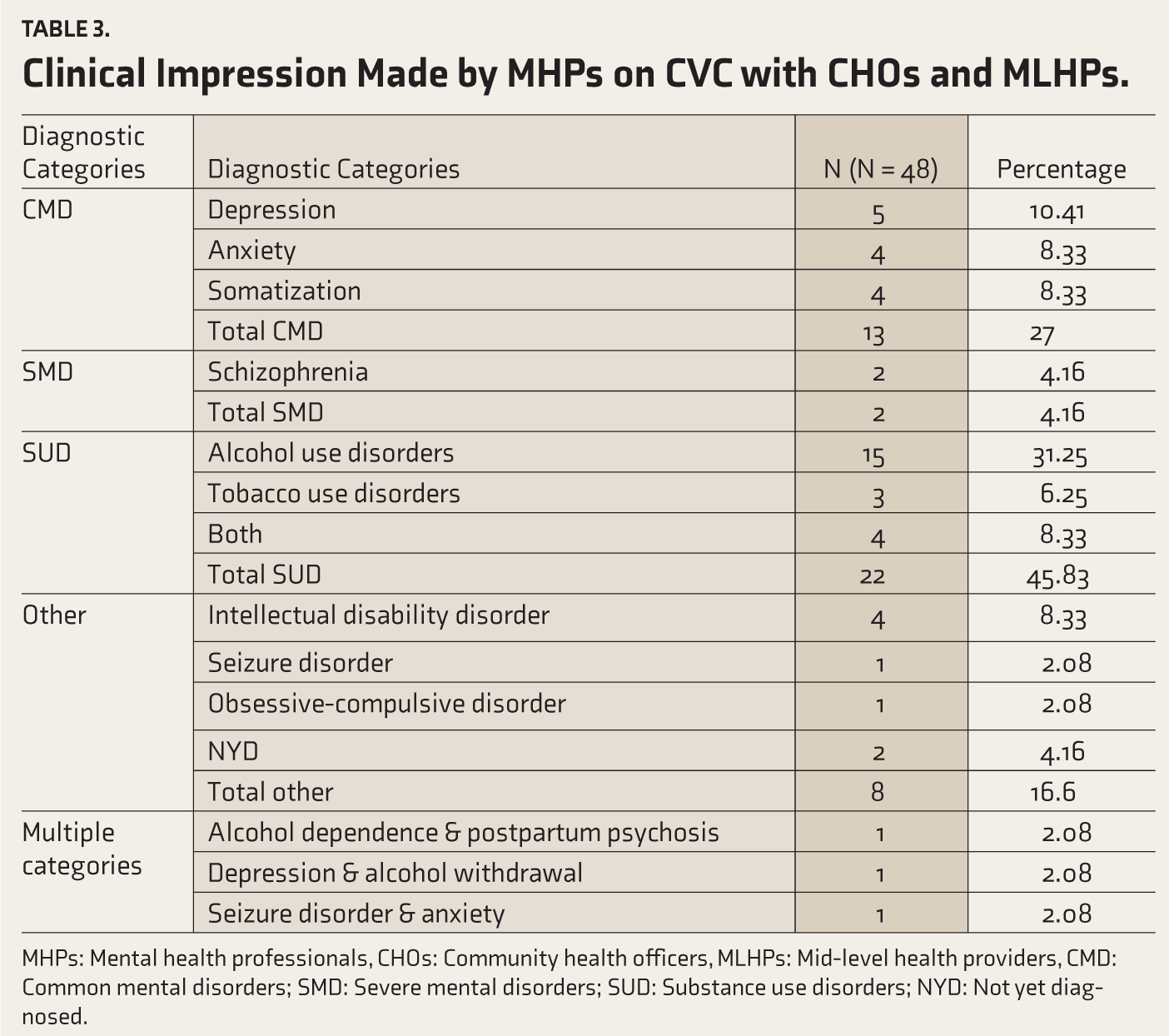
MHPs: Mental health professionals, CHOs: Community health officers, MLHPs: Mid-level health providers, CMD: Common mental disorders; SMD: Severe mental disorders; SUD: Substance use disorders; NYD: Not yet diagnosed.
The treatment advice and referral data indicated that most patients (89.58%) were referred to a Medical Officer/Psychiatrist, while psychoeducation and counseling were provided to 60.41% of patients. The follow-up rate for CVCs was 6.25%, indicating that only 3 of the 48 patients returned for a subsequent consultation (Table 4).
Treatment Advice and Referral Provided by the CHOs and MLHPs of CVC Patients.
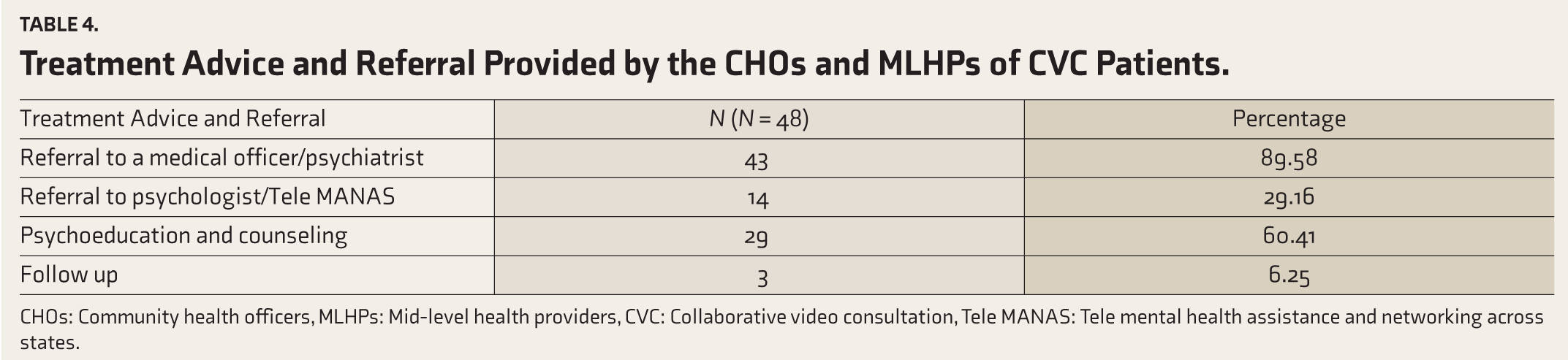
CHOs: Community health officers, MLHPs: Mid-level health providers, CVC: Collaborative video consultation, Tele MANAS: Tele mental health assistance and networking across states.
FGD Findings from Telangana CHOs—Major Themes and Sub-themes
Mental Health Awareness and Perception Among CHOs
CHOs’ understanding of mental health within their communities plays a critical role in creating awareness; hence, their perception and attitudes toward mental health are worth considering.
Public Awareness and Education
CHOs highlighted the lack of mental health awareness within the community, stressing the need for public education to demystify mental illness. CHOs also requested additional informational resources, especially in local languages, to foster broader community understanding.
In the present-day scenario, many people have mental illness. Each person should know what mental health illness is and how to deal with it.
It will be good if there are 30-50-second videos in Telugu… If it reaches all of us, it will automatically reach the public as well.
Stigma and Societal Perceptions
Stigma surrounding mental health was identified as a significant barrier in rural communities, where cultural beliefs often lead families to dismiss mental health conditions. CHOs noted that counseling is critical for helping patients and their families overcome this reluctance.
In villages, they will be branded as some sort of psychiatric disorder, so they are not willing.
Difficulty in convincing patients of the severity of their condition due to cultural norms and initial presentation with non-psychiatric symptoms.
Distinction Between Mental and Physical Health
The training helped CHOs improve their ability to differentiate between physical and mental health issues, leading to better treatment decisions.
We should know the distinction between a physical disease and a mental disease. Otherwise, treating the patient unnecessarily with other drugs adds to other causes. For a case of psychosomatic disease, if we do not identify the underlying condition, the patient will move from one doctor to another without addressing the mental illness. Correct diagnosis and treatment are critical in mental health cases to avoid unnecessary medication and to offer proper counseling.
Healthcare Workforce at AAM and Training
It is essential to explore the role and challenges of CHOs as frontline mental health providers in rural areas and focus on the impact of mental health training on their professional development.
Role and Challenges Perceived by CHOs
The CHOs acknowledged their role as being important to screen patients for mental illness, but discussed the heavy workload they face, which extends to ASHAs and ANMs (Auxiliary Nurse Midwives). This workload often leads to stress, burnout, and frustration among health workers, highlighting the need for improved workload management strategies.
Because we are the people who are on the front line to treat the public. So, first of all, we should identify a mental disease.
ASHAs and ANMs, even their work pressures are high. So, they are quite overworked and overburdened with a lot of health issues, both physical and mental health. Streamlining their work can help with targeted questions. Even MLHP is getting overburdened. Everyone is getting anxious and frustrated during meetings. Overburdened colleagues are getting anxious and frustrated.
Training and Professional Development
Training has significantly improved CHOs’ awareness and ability to manage psychiatric cases. Participants benefited from interactive, practical training methods, such as role plays and CVCs, which have enhanced their confidence and skill in diagnosis and referrals. However, participants highlighted the need for continued professional development.
Actually, before this training session, we used to see patients. Nevertheless, not from a psychiatric point of view, we know that something is wrong with them. So, after this training session, we are not letting them go.
We need more training sessions on how to handle the cases when we approach, and also in terms of the medication.
Service Provision and Resources
CHOs addressed the structural and resource-related challenges that they face in providing mental health care. Infrastructure limitations, lack of resources, and accessibility barriers were recurrent points of discussion, with the following key areas:
Resource Limitations and Accessibility
CHOs reported that the current infrastructure at PHCs is inadequate to address the rising demand for mental healthcare. Limited access to psychiatric resources, a lack of sufficient medical professionals, and an overall scarcity of facilities make it challenging to provide consistent and reliable mental health care.
We need better infrastructure at the PHC levels for effective mental health treatment. The lack of availability of specialists at the PHC level is a major limitation.
Diagnostic and Screening Tools
The MERIT tool has empowered CHOs to more accurately identify mental health conditions, increasing their confidence in diagnoses. They have also shared this tool with ASHAs, enabling them to identify cases at the community level effectively.
The MERIT screening tool is highly useful in identifying mental health issues and substance abuse. ASHAs are now trained on the MERIT screening tool, and they use it in their local language to communicate effectively with patients.
No difficulty in using the tool; it has made it easier to distinguish between mild, moderate, and severe cases.
Substance Abuse Management
Substance abuse, particularly tobacco, was identified as a common issue in the region. CHOs stressed the need for additional support and security measures when managing these cases, as they often disrupt PHC environments.
Substance abuse is common here, especially with tobacco … it causes disturbances at PHCs. Handling substance abuse cases at PHCs requires better security and support.
Patient Care and Treatment Approaches
This theme delves into the approaches CHOs use to provide patient care, emphasizing the training’s impact on their diagnostic, counseling, and referral practices. It also discusses the importance of non-pharmacological and rehabilitative interventions, which are essential in mental health care.
Diagnosis and Treatment Pathways
CHOs reported that the training enhanced their ability to identify and manage mental health cases. They discussed using counseling as a first-line intervention and referring severe cases to specialized centers, where families are willing to accept treatment.
We emphasize counseling and rehabilitation over medication wherever possible.
Referrals are reserved for severe cases and those willing to quit substance abuse.
It is challenging to manage cases where family members are reluctant; they often resist referrals.
Non-pharmacological Interventions and Integrative Medicine
CHOs have implemented lifestyle interventions like yoga and pranayama as part of their mental health support strategies. These practices, coupled with basic counseling skills, have proven effective in managing mild cases.
Lifestyle modifications, yoga, and pranayama can be included in counseling to support mental health.
The need for rehabilitation centers was emphasized as critical for comprehensive care, with suggestions for integrating Ayurvedic treatments into patient care. CHOs see these centers as essential to address both physical and mental health holistically.
Ayurvedic treatments like Panchakarma and Shirodhaara can support patients in managing depression and stress. NGOs have agreed to establish Panchakarma centers in the community, which could benefit mental health care.
Handling Stigma and Patient Care
CHOs discussed the complexities of managing mild cases, particularly in situations where families resist acknowledging mental illness due to cultural beliefs. They suggested that specialized mental health units at PHCs could create a more welcoming environment for patients, enabling better management of severe cases. Empathy was highlighted as a critical skill in their training, reinforcing the importance of a compassionate approach in mental health care.
Family reluctance makes it difficult to manage mild cases.
Empathy is the first thing we should have towards a patient with any illness, but it is even more critical in mental health care.
Patients often hesitate to travel to district hospitals due to distance; if mental health care were integrated at the PHC level, they would feel more comfortable seeking treatment.
Collaboration and Integration in Mental Health Care
Effective collaboration and integration are essential for strengthening mental health care delivery at the grassroots level. There has been a strong emphasis on cohesive partnerships across government agencies, NGOs, and community leaders to address existing gaps in mental health services and education.
Collaboration with NGOs
CHOs advocated for integrating specialized mental health units, such as utilizing NGO spaces for community and health official sessions, which were discussed as viable solutions for expanding mental health outreach.
NGOs can provide space for public sessions and health official engagement, offering an opportunity to enhance mental health outreach.
Medical colleges are starting de-addiction centers, but currently, there is no provision to contact local NGOs for collaboration.
Community Outreach and Education
CHOs have been proactive in community outreach, engaging local leaders, and conducting sessions to increase awareness. They focused on areas like exam-related stress, particularly among students, to educate young people on managing mental health and stress.
We organized camps for students to address mental stress related to exams, helping them understand mental health issues. Working with village leaders has helped us motivate community members to seek mental health support.
Ongoing Efforts and Future Directions
Participants noted that current efforts in Telangana, such as awareness programs targeting substance abuse, have been impactful but require sustained support and scaling to reach broader populations.
There are programs currently focusing on awareness for substance abuse in Telangana. Additionally, we have a suggestion to provide contact numbers for substance abuse rehabilitation centers in sub-centers.
Request for more emphasis on treatment aspects in future sessions and detailed discussion on treatment methods.
Feedback Analysis of the Training Program—Major Themes
Positive Impact of Training Content
Participants appreciated the training content for its relevance and quality, noting that it strengthened their understanding of mental health disorders and equipped them for community work.
Training sessions were beneficial in my understanding of the common and severe mental disorders.
Extremely informative and enhanced my knowledge on mental disorders.
Engagement and Teaching Style
The interactive and creative teaching methods, including role plays and activities, were highly praised for making complex topics accessible and memorable.
Easy to understand, role plays were the best.
Fun activities were excellent; please increase one more activity.
Appreciation for Trainers’ Expertise
Many participants expressed gratitude for the trainers’ expertise and professionalism. They appreciated the trainers’ ability to explain complex topics with patience and clarity.
All are very well experienced in teaching others… thank you, team.
The instructors explained everything very well; thank you for such satisfactory training.
Suggestions for Content Expansion
Many participants suggested adding topics like screen time addiction, stress management for frontline workers, and childhood mental disorders, as well as practical examples and videos.
Can add regarding current problems like screen time and mobile addiction.
Please include content on childhood mental disorders.
Requests for Ongoing Training
Participants expressed interest in future sessions, requesting courses to continue enhancing their skills.
Request for this type of training at least once a year.
I want this type of refresher training in the future.
Learning Tools and Format Improvements
Suggestions included adding more video materials, organizing lectures sequentially, and providing digital access to presentations.
Organize lectures in the order of the MERIT.
Request for more videos to be used for educational purposes.
Discussion
This study evaluated the effectiveness of an In-person mental training program and Tele-mentoring for CHOs and MLHPs from the states of Telangana and Tripura. The significant increase in pre- and post-Knowledge, Attitudes, and Practices (KAP) observed in both States (p < .01) demonstrates the program’s success in enhancing mental health literacy and care strategies among CHOs. These findings corroborate previous research by Garg et al., 17 which reported similar improvements in diagnostic skills among primary care doctors following blended psychiatric training programs. Such programs combine didactics, case discussions, and outpatient-based learning to develop practical competencies. 17 These results highlight the necessity of tailored training programs to address the mental health needs of underserved populations, positioning CHOs as key intermediaries in expanding access to mental health care. The training program was particularly effective in equipping CHOs with the skills to identify signs and symptoms of a mental illness and apply MERIT. Participants valued the program’s interactive learning methods, which included case vignettes and role-play videos, reinforcing their understanding of mental health disorders and referral practices. These findings align with Nirisha et al., who emphasized the effectiveness of similar interactive methods in training Accredited Social Health Activists (ASHAs). 10 Furthermore, the program’s design resonates with the “See-it-yourself, Try-it-yourself, Do-it-yourself” (STD) Acharya teaching model used in tele-OCT training, which has been shown to enhance skill application through sequential and hands-on methodologies.18,19 The integration of practical tools and experiential learning ensured that CHOs could effectively incorporate mental health care tasks into their broader responsibilities.
Additionally, the CVC model provided a novel approach to extending mental health care to underserved areas. This study demonstrated that 91.84% of the patients accessing the CVC model were first-time users of mental health services, with a majority being adults (97.9%). These findings indicate the substantial unmet need for mental health care in rural populations. Moreover, the high frequency of psychiatric conditions treated through CVCs, such as SUDs (31.25%, primarily alcohol dependence) and CMDs (27%, including depression and anxiety), underscores the relevance of integrating mental health services into primary care settings. These results are consistent with previous reports on the burden of psychiatric conditions in primary care. 20
The positive outcomes observed in the CVC model can be attributed to periodic collaborative engagements, including video and audio consultations, which facilitated real-time diagnostic and treatment support for CHOs. These findings align with research by Manjunatha et al., who highlighted the value of telepsy chiatry in identifying and managing CMDs and substance use problems. 21 However, the low follow-up rate (6.25%) observed in this study suggests the need for improved mechanisms to ensure continuity of care. Addressing both the demand-side (patient engagement) and supply-side (resource allocation) challenges will be crucial for sustaining these benefits.
While the training program effectively enhanced CHOs’ skills, systemic barriers such as high workloads, resource limitations, and stigma in rural communities persisted. These challenges highlight the importance of developing multi-pronged strategies, including stigma-reduction campaigns and the expansion of infrastructure to support mental health services. The findings are aligned with the broader objectives of the DMHP, which emphasizes outreach, psycho-social interventions, and continued care for mental disorders at the community and district levels. 22
As part of training skills translating to practice, CHOs’ preferred counseling and lifestyle interventions, such as yoga and Ayurveda, align with the NIMHANS model of integrative healthcare. This model advocates for the inclusion of yoga and other traditional practices as formalized clinical disciplines. 23 Incorporating culturally relevant practices can reduce stigma and improve treatment acceptability among rural populations. Additionally, Ayurvedic practitioners who serve as CHOs bring valuable expertise in holistic care, which can further enhance the integration of traditional treatments.
Given treatment provision on a larger scale at the sub-center level, the CHOs emphasized the importance of partnerships with NGOs and government programs to address resource gaps. Programs like “Maanasadhaara,” which provide rehabilitation services for chronically mentally ill patients, demonstrate how collaborative efforts can augment public health initiatives. 24 CHOs’ active involvement in community outreach underscores their role in linking underserved populations with essential mental health services.
The study findings also align with the idea of collaboration and integration of mental health services into primary care through the DMHP. By empowering CHOs as intermediaries between patients and specialists, the training program addressed a critical gap in mental health service delivery. The results underscore the need for continuous training, mentorship, and resource allocation to sustain these gains.
Future Directions and Implications
The current training program for CHOs and MLHPs can be scaled and integrated into the DMHP to strengthen mental health care delivery at the grassroots level. By replicating the training curriculum, emphasizing hands-on learning through CVC, and leveraging existing frameworks like MNS modules, this model can enhance care at sub-primary levels, including AAMs.
To implement this model, DMHP must focus on building capacity through recruitment and training, supported by partnerships with NGOs, medical institutions, and telemedicine platforms. Regular monitoring and evaluation of outcomes, such as patient follow-up rates and practitioner competency, will ensure the program’s impact and sustainability. This approach aligns with national mental health policies and positions CHOs and MLHPs as pivotal in integrating mental health into primary care, addressing stigma, and improving access for underserved populations.
Strengths
The research article effectively addresses a critical gap in India’s healthcare landscape by integrating mental health services into primary care through innovative in-person training and tele-mentoring for CHOs and MLHPs. The study is highly relevant, targeting resource-constrained and culturally diverse regions such as Telangana and Tripura. The methodological rigor of the mixed-methods approach combines quantitative and qualitative data, offering comprehensive insights into the program’s impact. The use of tele-mentoring introduces a novel, scalable method to extend mental health care to underserved areas. The study also demonstrates strong feedback mechanisms, collecting actionable insights from participants to improve future training sessions.
Limitations
The extensive resource requirements for in-person training can be a hindrance to replicating this model, but leveraging existing resources, such as DMHP and a hybrid mode of training, can mitigate this challenge, making it more scalable for a larger population. The study also suffers from high attrition rates in pre- and post-assessments, which reduces the reliability of the KAP score comparisons. The reliance on self-reported data for these assessments of Attitudes and Practices introduces the risk of bias, particularly social desirability bias. Due to the training-based setting, complete anonymization of assessments was not feasible.
Conclusions
This study highlights that in-person mental health training programs and tele-mentoring can provide sustained support and be scalable, equipping CHOs and MLHPs with the skills needed to address the mental health needs of underserved populations at the community level.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Same as the “Introduction” article of this issue (Indian J Psychol Med. 2026;48(1 suppl)).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Channaveerachari Naveen Kumar is the Principal Investigator of this project and supplemental issue. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Declaration Regarding the Use of Generative AI
The authors used the Truboscribe AI Transcription Tool to translate and transcribe video and audio data of the focus group discussions and Chat GPT to paraphrase and formalize the text. After using this tool, the authors reviewed the translated and transcribed content, edited it as needed, and took full responsibility for the content of the publication.
Ethical Approval
The study was approved by the Institutional Ethics Committee (IEC) (Approval No. NIMHANS/ 43rd IEC (BEH.SC.DIV) 2023, dated 8th December 2023).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Corporate Social Responsibility Grants of a multinational company.
Patient Consent
The patient and participant consent statement is already included in the Methods section of the manuscript and has been highlighted for clarity.
Registration
Registered with the Clinical Trial Registry of India (Registration No. CTRI/2024/02/062906).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.