
Abstract
Background:
Young adulthood (18–25 years) represents a critical developmental stage marked by heightened vulnerability to psychiatric disorders. Despite this, there is limited data on the clinical and demographic profiles of young adults seeking mental health care in India. This study analyzed trends and associations in the demographic and clinical characteristics of young adults participating in Collaborative Video Consultations (CVCs) at Primary Healthcare Centers (PHCs) across nine Indian states.
Methods:
Data from 120 CVCs conducted between November 2022 and September 2024 were analyzed. Patients aged 18–25 were assessed using intake forms, clinical evaluations, and self-reports. Diagnoses included Common Mental Disorders (CMDs), Severe Mental Disorders (SMDs), Substance Use Disorders (SUDs), and other conditions. Associations between demographic factors, sleep disturbances, Deliberate Self-Harm (DSH), and diagnostic categories were explored.
Results:
CMDs, predominantly depression and anxiety, were the most frequent diagnoses. Females were more likely to be diagnosed with CMDs, while males had higher rates of SUDs. Occupation showed significant associations: CMDs were common among students, SMDs among non-earning individuals, and SUDs among earning individuals. Sleep disturbances were significantly associated with CMDs (p < .001). DSH was also prevalent in CMDs (p = .003).
Conclusion:
The findings underscore the clinical significance of early detection and gender-sensitive, occupation-specific mental health screenings at PHCs for young adults. Expanding teleconsultation models, such as CVCs, could help bridge care gaps for underserved populations.
We analyzed demographic and clinical profiles of young adult patients who received collaborative video consultations at primary healthcare centers. Females had more CMDs, men had more SUDs; students had the highest CMD rates, non-earning individuals had the highest SMD burden, and earning individuals had the highest SUDs. PHCs need targeted mental health screening based on gender and occupation; CVCs improve access to care in resource-constrained settings.Key Messages:
Asignificant proportion of India’s population comprises young adults. According to the 2011 Indian Census, individuals aged 20–24 comprise 9.2% of the adult population, representing the largest proportion of adults. 1 Typically classified as “young adults” in literature,2,3 this age group generally encompasses individuals aged 18–25. This period is marked not only by economic productivity but also by significant life transitions, including the assumption of adult responsibilities, often with ongoing academic and financial dependencies. 2
International data underscores the extent of mental health challenges in this demographic. Data from the National Survey on Drug Use and Health (NSDUH) in the United States reveal that individuals aged 18–25 have the highest prevalence of mental illness (MI) at 36.2%, compared to 29.4% among adults aged 26–49 years and 13.9% among those aged 50 and older. 4 Furthermore, young adults in this age range also experience the highest rates of severe mental illness (SMI) at 11.6%, significantly higher than the 7.6% prevalence in adults aged 26–49 and 3% in those aged 50 and older. Despite these elevated rates, young adults are less likely than other age groups to receive mental health services. 5
In India, the National Mental Health Survey (NMHS; 2015–2016) estimates a lower prevalence of mental disorders among individuals aged 18–29 years (7.5%), 6 which may reflect a trend of delayed help-seeking behaviors common in this age group. 7
Primary Healthcare Clinics (PHCs) frequently serve as the first point of contact for young adults seeking healthcare, positioning Primary Healthcare Professionals (PHPs) uniquely to facilitate early detection and intervention for mental health concerns. However, despite the frequency of young adults presenting to primary care with psychological and behavioral problems, limited data are available in India on the specific clinical and demographic characteristics of this group, particularly as they relate to common mental health diagnoses.
Telepsychiatry has demonstrated significant potential in bridging the gap between limited mental health resources and underserved populations, especially in low- and middle-income countries. In recent years, the rapid advancement of digital technologies has paved the way for much-needed innovation in mental health care. 8 It enables remote diagnosis, consultation, and management of mental health conditions, reducing geographical and socioeconomic barriers to care. 9 However, despite the promise of telepsychiatry, challenges such as inadequate infrastructure, lack of training among primary care providers, and limited follow-up care often hinder its effectiveness. 10 Instant and live Collaborative Video Consultations (CVCs) address these gaps by integrating real-time consultations between Mental Health Professionals (MHPs) and PHPs. This model facilitates the Direct Skill Transfer (DST) from MHPs to the primary care system to enhance early detection and tailored interventions, particularly in resource-constrained settings where access to mental health specialists is sparse. 11
CVCs with these PHPs provide a unique dataset for examining the status of mental healthcare provision for young adults in PHCs, allowing in-depth clinical profile analysis. This study aims to identify and analyze patterns of mental health issues among young adults who were a part of CVCs and to explore how these patterns correlate with demographic factors such as gender, marital status, and occupation. By examining these associations, this article seeks to provide valuable insights into the psychiatric landscape of young adults in India and to inform future interventions and policy development.
Methods
The institute’s Institutional Ethics Committee approved the study. Data for the study were taken from a pan-India digitally driven capacity-building program for primary mental healthcare. Verbal informed consent was sought from all participants, including the PHPs and patients.
This study uses a cross-sectional design. We used the STROBE cross-sectional checklist when writing our report, and it is uploaded as “STROBE Complete Checklist.” 12
Study Design
This study employed a quantitative, cross-sectional design with convenience sampling. Data from CVCs involving young adult patients was analyzed from the project’s inception in November 2022 until September 11, 2024. CVCs are synchronous audio/video consultations between PHPs and MHPs, including psychiatrists, clinical psychologists, social workers, and psychologists. These consultations were initiated by PHPs across three cadres: Medical Officers (MOs), Community Health Officers (CHOs), and Field Level Workers (FLWs). MOs conduct clinical evaluations and prescribe medication. CHOs also perform clinical assessment and, in some cases, dispense medications. FLWs, on the other hand, support home visits and community care. The data was collected from nine states: Bihar, Goa, Karnataka, Kerala, Maharashtra, Telangana, Tripura, Uttarakhand, and West Bengal.
Sample
The sample comprised young adult patients aged 18–25 who visited primary healthcare settings with prior or current psychiatric symptoms and consented to CVCs between November 2022 and September 11, 2024. The project received a total of 1,289 CVCs within that time frame. A total of 120 CVCs were identified as eligible for this study.
Variables
Demographic Variables
Data on participant age, gender, marital status, and occupation were collected through intake forms (Appendix A) during CVC consultations.
Primary Diagnostic Category
Diagnoses were classified into: Common Mental Disorders (CMD), Severe Mental Disorders (SMD), substance use disorders (SUD), and other diagnoses, which included Intellectual and Developmental Disability (IDD), Seizure Disorder with psychiatric symptoms, and diagnoses that were Not Yet Decided (NYD). The MHP carried out this categorization as per ICD-10.
Sleep Disturbance
Sleep patterns were documented based on patient self-reports during consultations. Sleep disturbance was coded as present or absent.
Deliberate Self-harm (DSH)
The DSH incidents were documented based on patient self-reports during consultations. DSH was coded as present or absent.
Treatment Recommendations
Treatment advice provided by MHPs during consultations was categorized into medication advice, psychoeducation, referral for specialized care, and psychosocial management recommendations.
Procedure
Data were collected retrospectively from records of CVCs with young adult patients. The data extraction process involved reviewing CVC records from November 2022 to September 11, 2024 and identifying eligible cases. Demo-graphic and clinical data were transcribed into a structured database, coded, and verified for accuracy.
Statistical Analysis
Data analyses, including descriptive and inferential statistics, were carried out using the licensed SPSS version 29. 13 Cross-tabulations examined associations between demographic factors (e.g., gender, occupation, marital status) and primary diagnostic categories. Chi-square tests, including Fisher’s Exact tests where appropriate, were used to determine the statistical significance of these associations. The significance level was set at p <.05. Findings were reported with Chi-square and Fisher’s p values for significant associations. Missing data were analyzed separately.
Results
The project received 1289 CVCs during the study period, of which 120 were eligible for this study. This indicates a prevalence rate of 9.3%. Among these, 65% (n = 78) of the CVCs were conducted with CHOs, 29.16% (n = 35) were conducted with MOs, and 5.83% (n = 7) with FLWs.
The sample comprised a higher proportion of females (52.5%, n = 63) compared to males (47.5%, n = 57). Most participants were unmarried (70%, n = 84), while 27.5% (n = 33) were married, and 2.5% (n = 3) had missing marital status data. Occupationally, 8.33% (n = 10) of participants had missing data. Among the remaining participants, a notable segment of the sample (30%; n = 36) reported being non-earning. This group was closely followed by students, representing 28.33% (n = 34) of the participants. Additionally, 16.66% (n = 20) reported being homemakers, while another 16.66% (n = 20) were employed in various sectors. This latter group included individuals in labor-intensive roles—such as farmers, laborers, mechanics, and delivery workers—as well as office staff and professionals.
Clinical Profile
Table 1 illustrates the primary diagnostic categories of young adults diagnosed through CVCs. The most common category was CMDs, with depressive disorder being the most frequent diagnosis, followed by anxiety disorders. SMDs and SUDs were relatively less prevalent. A significant portion of the sample was categorized under Other. Among all participants, 19.16% (n = 23) were already receiving treatment at the time of the CVC, while 80.83% (n = 97) had not received prior therapy. Additionally, 28.33% (n = 34) of participants reported sleep disturbances. A history of DSH was reported by 15% (n = 18) of the participants.
Primary Diagnostic Categories (ICD) of Young Adult Patients Discussed in CVCs (n = 120).
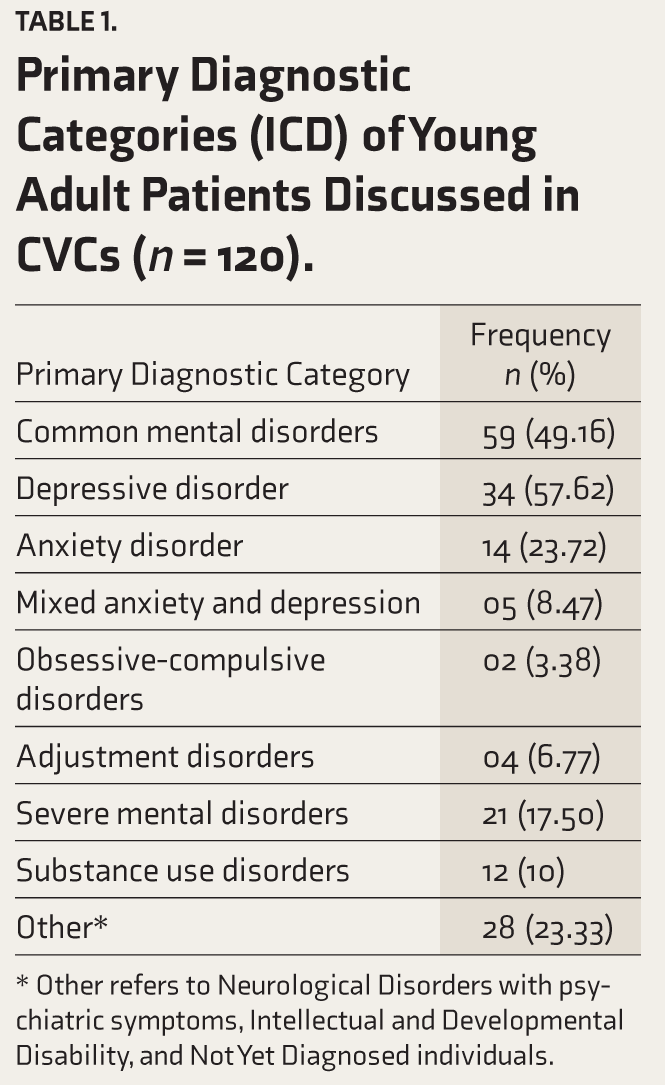
* Other refers to Neurological Disorders with psychiatric symptoms, Intellectual and Developmental Disability, and Not Yet Diagnosed individuals.
Treatment Advice
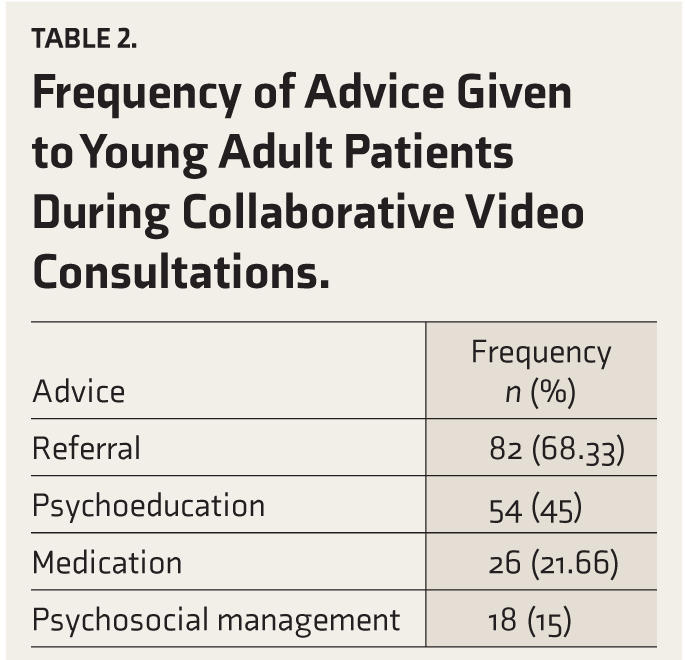
Table 2 summarizes the advice provided to participants. The most common recommendation was referral for further care, followed by psychoeducation. Both medication and psychosocial management were less frequently recommended.
Frequency of Advice Given to Young Adult Patients During Collaborative Video Consultations.
Associations Between Primary Diagnostic Categories and Demographics, Clinical Features, and Advice
Chi-square tests were conducted to examine associations among primary diagnostic categories, demographic factors, diagnoses, and clinical features. Several significant associations were found. Table 3 illustrates that a higher proportion of females were diagnosed with CMDs, while males were more likely to have SUDs. Students were predominantly diagnosed with CMDs, homemakers with SMDs, and non-earning individuals had a notable proportion of SUDs. Unmarried individuals were more likely to be diagnosed with CMDs, and married individuals were more often diagnosed with SMDs. A higher proportion of those with sleep disturbances were diagnosed with CMDs, while those without sleep disturbances were more likely to be diagnosed with SUDs. Individuals reporting DSH were more likely to have CMDs, while no cases of self-harm were observed in those with SUDs.
Associations Between Primary Diagnostic Categories, Demographic Variables, and Clinical Features.
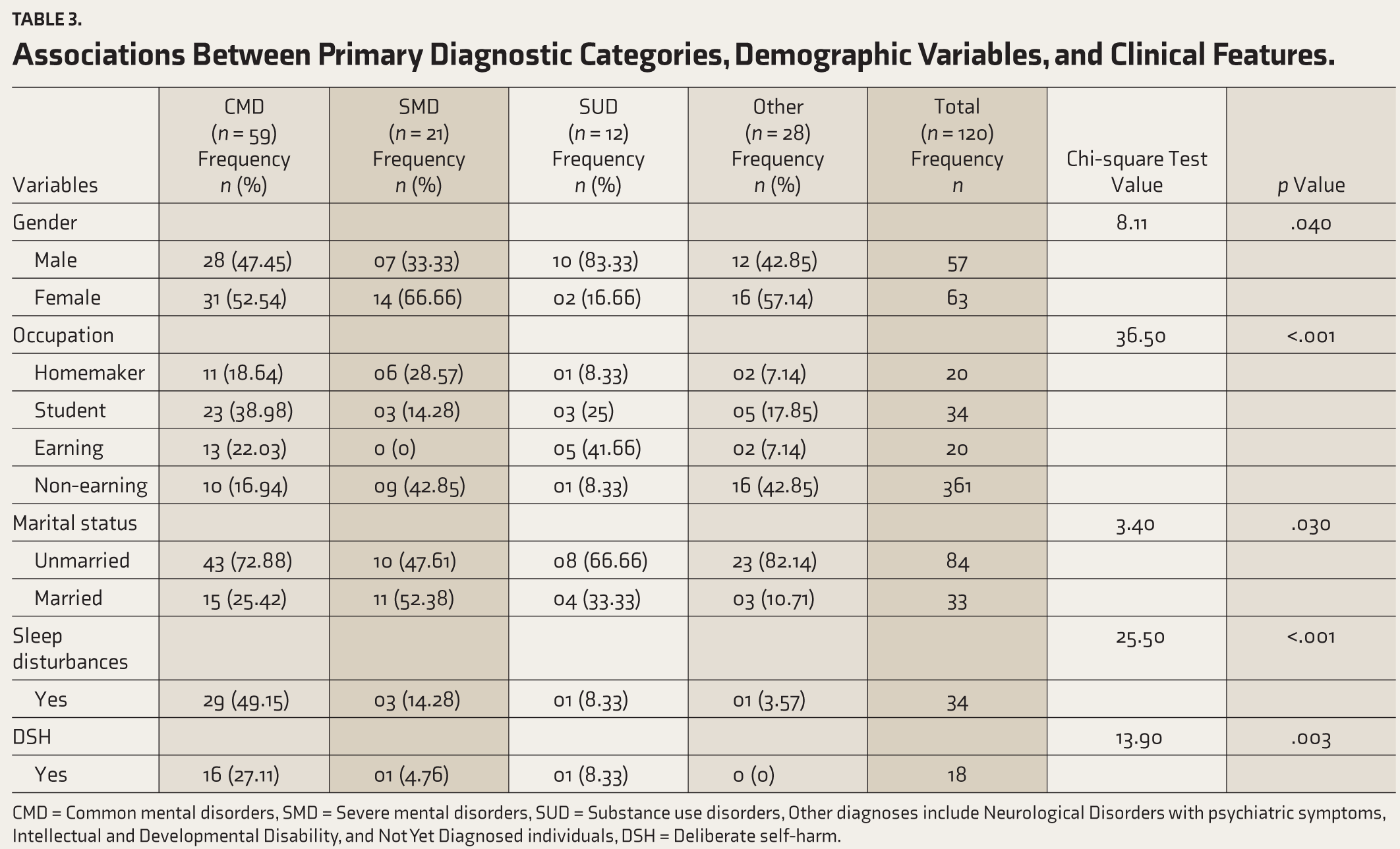
CMD = Common mental disorders, SMD = Severe mental disorders, SUD = Substance use disorders, Other diagnoses include Neurological Disorders with psychiatric symptoms, Intellectual and Developmental Disability, and Not Yet Diagnosed individuals, DSH = Deliberate self-harm.
No significant association was found between being on previous medication and primary diagnosis (χ² = 2.39, p = .496). Table 4 shows that individuals diagnosed with CMDs were more likely to receive referrals for further care, medication advice, and psychosocial management. No significant relationship was observed between psychoeducation advice and primary diagnosis.
Associations Between Treatment Advice and Primary Diagnostic Categories.
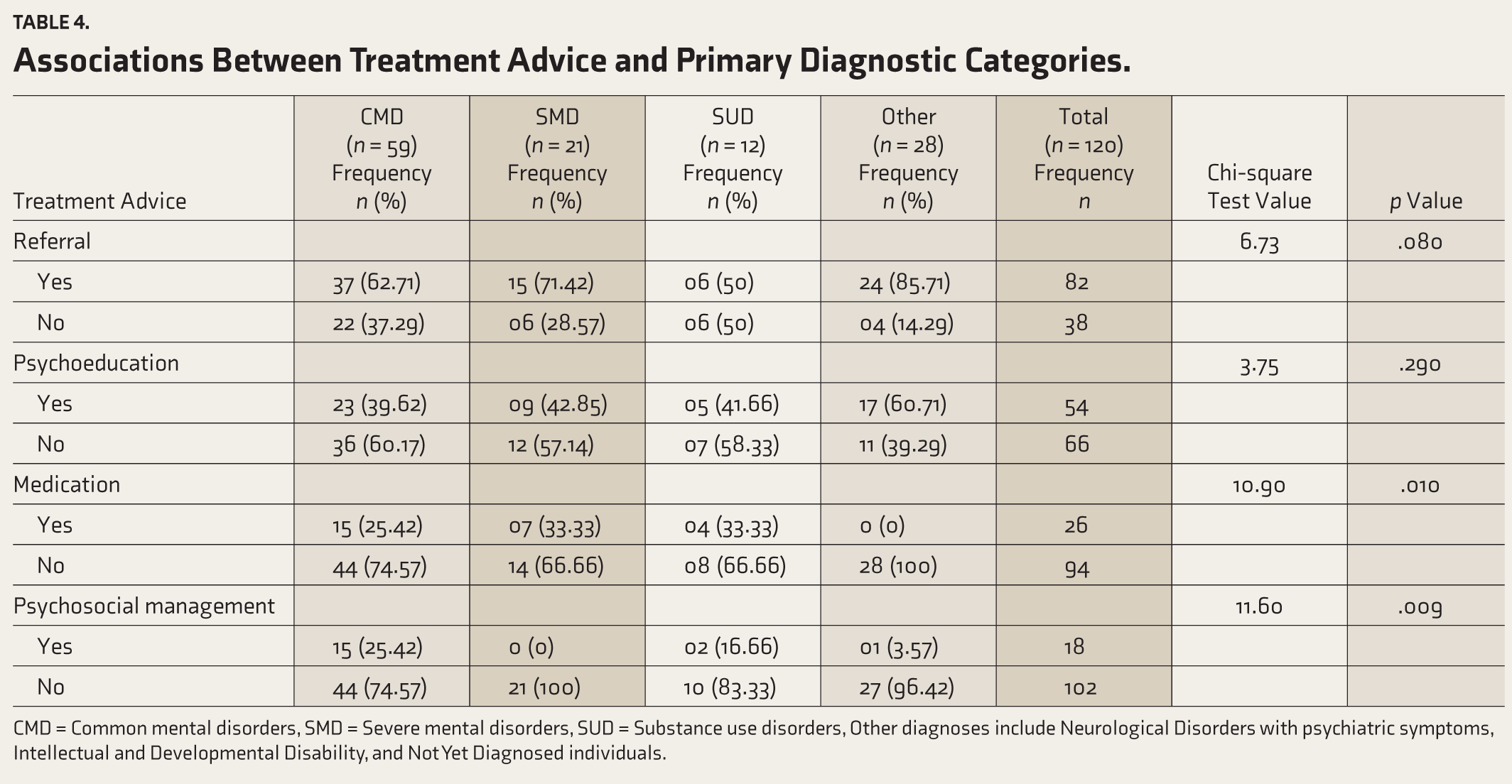
CMD = Common mental disorders, SMD = Severe mental disorders, SUD = Substance use disorders, Other diagnoses include Neurological Disorders with psychiatric symptoms, Intellectual and Developmental Disability, and Not Yet Diagnosed individuals.
Associations by Gender
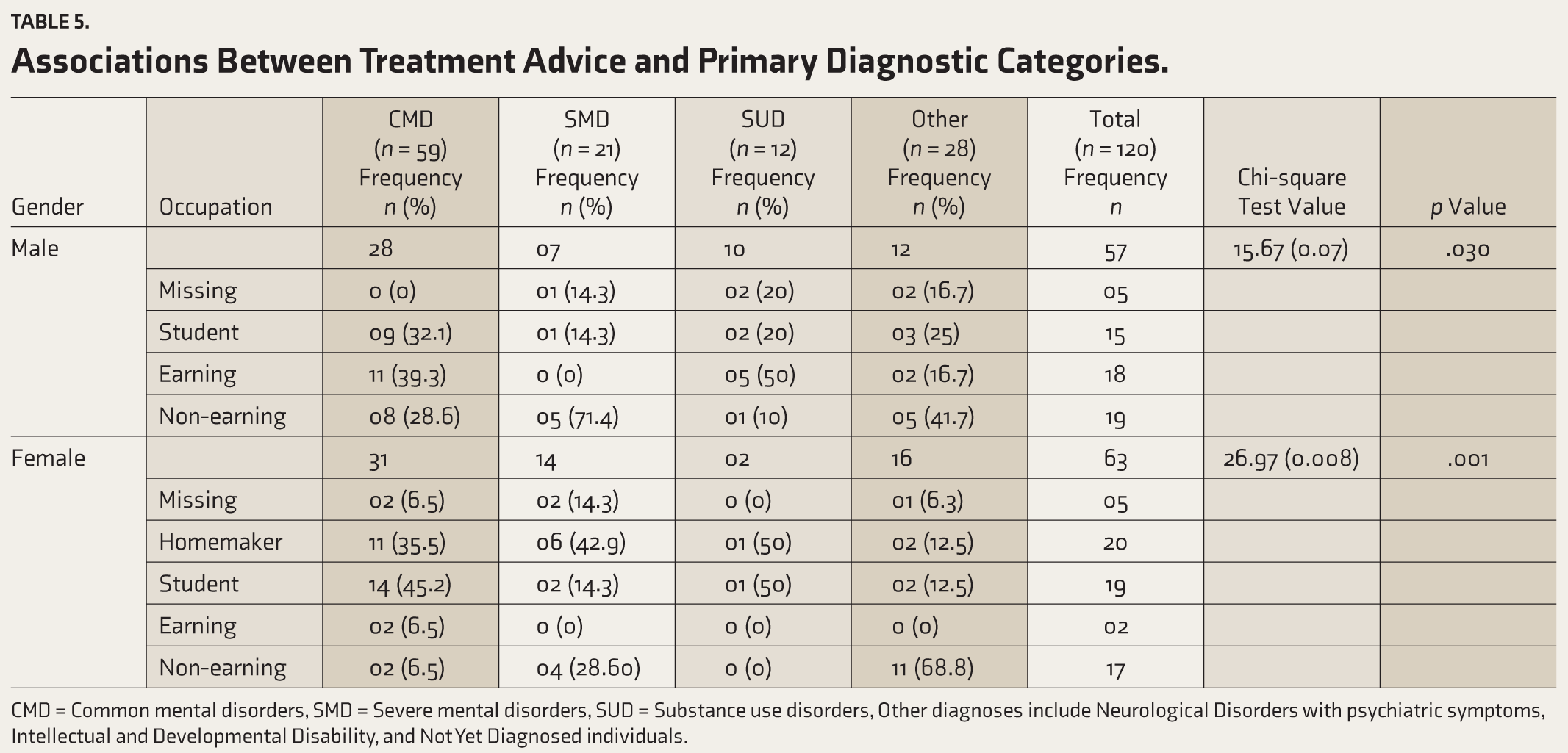
Table 5 demonstrates that when the analysis was stratified by gender, distinct patterns emerged. Significant associations were found between occupation and primary diagnostic category for both males and females (Fisher’s Exact Test: p = .032 for males, p = .001 for females). In males, non-earning patients had the highest rates of SMDs, while both CMDs and SUDs were more frequently diagnosed in earning males. Male students also accounted for a significant proportion of those diagnosed with CMDs. Among females, CMDs were more common among students, while homemakers were particularly represented in the SMD category. Associations between marital status and primary diagnostic category were found to be non-comparable. A significant association between sleep disturbance and primary diagnosis was found for females (p < .001). Females reporting sleep disturbances were predominantly diagnosed with CMDs, while those without sleep issues more frequently had SUDs or other diagnoses. For males, no significant relationship was found between sleep disturbance and primary diagnosis; however, CMD was still the most common diagnosis among those with reported sleep issues.
Associations Between Treatment Advice and Primary Diagnostic Categories.
CMD = Common mental disorders, SMD = Severe mental disorders, SUD = Substance use disorders, Other diagnoses include Neurological Disorders with psychiatric symptoms, Intellectual and Developmental Disability, and Not Yet Diagnosed individuals.
Discussion
The present study aimed to examine the demographic and clinical profiles of young adults seeking mental health services at PHCs in India who have undergone CVCs. Young adulthood is a crucial developmental stage often marked by heightened vulnerability to mental health disorders due to transitions in social, educational, and occupational roles. 14 Additionally, this age also represents a period of biological vulnerability for mental health disorders. Studies indicate that the lifetime prevalence of mental illnesses peaks during late adolescence. 15 Given the duration of untreated conditions and the average interval before individuals seek professional intervention, it follows that initial consultations tend to occur during young adulthood.7,16 The biological underpinnings of this vulnerability, coupled with psychosocial stressors, make targeted screening and early intervention particularly crucial in this population. This study highlights essential correlates relevant to tailoring models of care and interventions in primary care settings.
As per the NMHS 2015–2016, the lifetime mental morbidity rate stood at 9.54% and the current rate was reported to be 7.39% for individuals aged 18–29. 6 The observed prevalence of psychiatric disorders in this young sample was 9.3%. This difference in current rates may reflect differences in clinical versus community-based samples. Studies have demonstrated that the prevalence of MI among clinical outpatients is significantly elevated due to the higher morbidity typically observed in clinical settings. 17 Furthermore, the prevalence observed in the study is considerably lower than the NSDUH-reported rate in the United States (36.2%).0 This variation may be influenced by cultural differences in help-seeking behaviors, which often result in delayed or crisis-driven care. 18
In the findings of this study, CMDs emerged as the most common diagnostic category, with depression being the predominant diagnosis, followed by anxiety. These findings align with previous studies suggesting that depression and anxiety are the most prevalent mental health issues among young adults globally.19,20 Significant gender differences were noted in diagnostic categories: females were predominantly diagnosed with CMDs, while males exhibited higher rates of SUDs. These findings are in line with previous findings, which indicate that women have a higher mean level of internalizing disorders. In contrast, men have a higher mean level of externalizing disorders, reflecting broader sociocultural dynamics, influenced by societal expectations and stigma. 21 Occupation also influenced diagnostic patterns: CMDs were common among students, likely due to academic stress and developmental challenges during emerging adulthood. 14 Non-earning individuals were more likely to present with SMDs, reflecting employability challenges and social isolation. 22 Earning individuals demonstrated higher SUD prevalence, aligning with NSDUH data, 23 possibly due to workplace stress and increased access to substances. These findings highlight the need for occupation-specific mental health interventions.
The treatment advice provided to participants was influenced by the cadre of PHPs engaging in the CVC. Referrals were the most frequently suggested intervention, underscoring the need for a robust referral network and access to specialized care. Psychoeducation was often recommended, highlighting its importance in bridging mental health literacy gaps. Medications and psychosocial management were less commonly advised due to limitations in PHPs’ training and scope of practice. The findings underscore the importance of capacity-building initiatives to enhance PHPs’ ability to manage mental health conditions comprehensively.
Sleep disturbances were strongly linked to CMDs, reinforcing their role as clinical markers and highlighting the bidirectional relationship between sleep and mental health. In contrast, individuals with SUDs reported fewer sleep disturbances, likely due to the masking effects of substances. 24 Additionally, DSH was significantly associated with CMDs, particularly depression, supporting the view that DSH serves as a maladaptive coping mechanism. 25 These findings underscore the importance of integrating assessments of sleep and self-harm in routine primary care evaluations. Despite a high proportion of participants presenting in crisis with DSH, most had not received prior treatment, which highlights the critical role of PHC in mental health. The high referral rate (68.3%) indicates a gap in PHC’s capacity to meet mental health needs, suggesting a need for enhanced training and resources for PHPs.
Limitations
Despite these insights, the study has certain limitations. The cross-sectional nature of the data limits conclusions regarding causality, and potential self-report biases might affect the accuracy of some variables, such as DSH and sleep disturbance. Future research should aim to address these limitations by incorporating larger, more diverse samples and longitudinal designs to explore the stability and progression of these diagnostic patterns over time. Missing data on key demographic variables, such as occupation for some participants, further constrains interpretability. Additionally, qualitative studies exploring barriers to help-seeking among this age group could complement these findings and inform culturally sensitive interventions. Furthermore, as this study was conducted within the framework of a larger mental health program, findings may not fully reflect the broader primary care landscape in India.
Strengths
However, a major strength of this study is its use of real-world data from CVCs spanning nine states, which provides a diverse and representative sample of young adults presenting to PHCs, thereby ensuring generalizability. The inclusion of gender- and occupation-stratified analyses allows for nuanced insights into the associations between demographic factors and primary diagnoses.
The implications of these findings for clinical practice are notable. The observed patterns suggest the need for gender- and occupation-sensitive screening practices within primary care settings. For example, given the higher rates of CMDs and associated symptoms among women, it may be beneficial to implement routine assessments for DSH and sleep quality for female patients. For male patients, targeted screening for SUDs could enhance early identification and treatment. Additionally, the study underscores the utility of teleconsultation models in bridging mental health care gaps in resource-constrained settings. CVCs, as demonstrated in this study, offer an accessible, scalable approach for implementing these targeted interventions.
Conclusions
These findings strongly underscore that young adults are not a monolith, but a diverse group facing multi-faceted challenges. Although multiple ministries in India acknowledge the significance of mental health, their efforts remain fragmented, highlighting the need for comprehensive strategic planning to enhance screening, early detection, treatment, and referral systems. Institutional and community-based care models should be re-envisioned to incorporate holistic approaches that extend beyond the purely biomedical framework. 20 By focusing on young adults—at the intersection of risk and opportunity—primary care systems can play a transformative role in reducing the burden of mental health disorders while promoting long-term well-being.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Same as the “Introduction ” article of this issue (Indian J Psychol Med. 2026;48(1 suppl)).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Channaveerachari Naveen Kumar is the Principal Investigator of this project and supplemental issue. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Declaration Regarding the Use of Generative AI
The authors used the Grammarly AI Paraphrasing Tool to enhance and formalize the text. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Ethical Approval
Institutional Ethics Committee (IEC). Approval number with date: Approval No. NIMHANS/43rd IEC (BEH.SC.DIV) 2023, dated December 8th, 2023. Appropriate permissions from the concerned authorities: Registered with the Clinical Trial Registry of India (Registration No. CTRI/2024/02/062906).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study’s data were derived from a project funded by the CSR grants of a multinational company.
Appendix A
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.