
Abstract

Urbach–Wiethe disease (or lipoid proteinosis) is a rare, hereditary, systemic disorder having autosomal recessive inheritance, characterized by widespread deposition of hyaline-like material in skin and mucous membranes.1,2 Radiological findings have shown bilateral symmetrical horn-shaped calcifications in the mesial temporal region of the brain. 3 These calcifications are hypothesized to be associated with a wide range of neuropsychiatric manifestations like epilepsy, aggression, memory impairment, and paranoid symptoms. 1 The symptoms of paranoia seen here often share similarities with various presentations of schizophrenia. 3 There are around 400 documented cases of this disorder worldwide, with around 50 published cases demonstrating neurological and neuropsychiatric sequelae, with the largest cohort surviving in remote places in South Africa.4,5 We here present a unique report of two siblings, one with symptoms of paranoia and disorganized behavior, while the other demonstrating aggression and impulsivity, and both having typical intracranial calcifications concurrent with the findings of lipoid proteinosis.
Case 1
A 19-year-old boy, Mr. X, presented to the Psychiatry Outpatient Department with complaints of muttering, gesturing, and solitary smiling for two years, along with impulsivity and aggression episodes over the preceding year. He had paranoid ideations upon hearing nearby carpentry noises that people wanted to harm him, accompanied by fearful behavior in which he would shut the doors and windows of his house. Furthermore, he had occasionally displayed disorganized behavior, including collecting and shredding roadside materials, smearing feces on his body, and neglecting personal hygiene. Instances of inappropriate behavior, such as disrobing in front of relatives and family members and touching his aunt inappropriately, also occurred.
After six months of the said complaints, his parents noticed him standing with his hands in the air and stiff limbs, not moving in spite of his father’s verbal commands and physical force. He would maintain the same posture for hours, hampering his daily routine activities. He improved significantly on lorazepam and risperidone over two to three months.
Family members noticed some disturbance in his behavior before six months. Mother recalled instances where he used to speak endlessly without a pause. He used to sing songs of Maharana Pratap, saying he was the king and everyone around him was his servant. He would also repeatedly touch the feet of family members and loudly chant the name of God, “Jai Shree Ram,” by joining both hands. Instances of mimicking the sounds of various animals during conversation were also noted. Bursts of irritability were reported where he would use foul language, scream, and pick up fights with siblings for trivial matters. He would sleep just for two to three hours, wake up, and pace around the house.
The above complaints lasted for 15–20 days, after which they consulted a private psychiatrist. He was put on olanzapine, sodium valproate, and alprazolam, which alleviated sleep disturbances and manic symptoms temporarily but caused him to remain drowsy throughout the day.
Meanwhile, a history of hospital admission for various skin ulcers requiring surgical intervention was found. A familial history of a similar skin condition, alongside hoarseness of voice in a younger brother, depicted a genetic predisposition. His personal history revealed an uneventful birth history and developmental delay, particularly in speech, not achieving verbal communication until age three despite normal hearing. Additionally, his scholastic performance remained below average, with limited social interactions and a preference for solitary activities, suggesting impaired socioemotional reciprocity.
Physical examination revealed characteristic skin findings, including verrucous growth on the chin, multiple papules on both eyelid margins, and oral lesions with a thickened tongue. Persistence hoarseness of voice indicated longstanding mucosal involvement.
Mental Status Examination (MSE) highlighted the difficulty in establishing rapport, irritable mood, restricted affect, and concrete thinking. In areas of intelligence, his performance was average, with intact judgment.
The Brief Psychiatric Rating Scale (BPRS) 6 score was 34, with higher scores in suspiciousness and hallucinatory behavior. Mild autistic traits were found on the Indian Scale for Assessment of Autism (ISAA) 7 , with a score of 78. Binet Kamat Test 8 was used to test the intelligence quotient (IQ), on which he scored 91, indicating normal intelligence. The patient was diagnosed as having a psychotic disorder due to another medical condition as per the Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5). 9
His routine blood investigations and systemic examination were unremarkable.
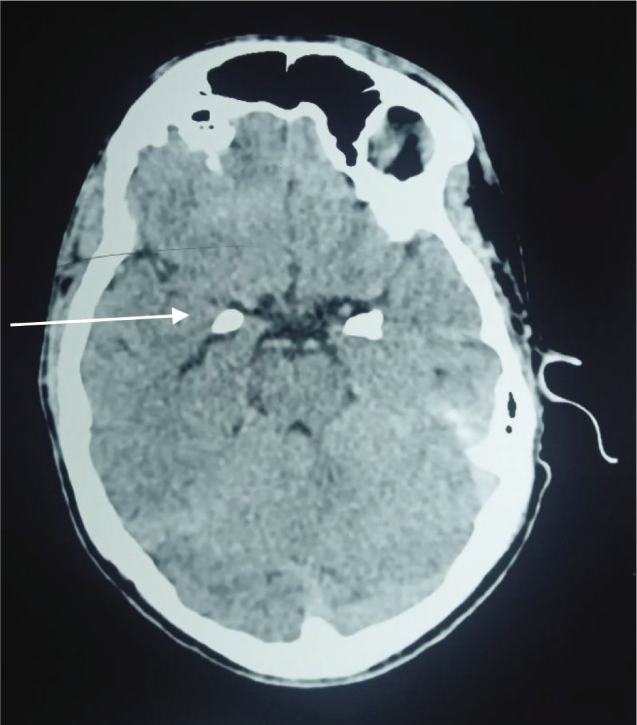
Brain imaging by computed tomography (CT) scan as shown in Figure 1 revealed bilateral symmetrical horn-shaped calcifications in the mesial temporal lobe.
Computed Tomography (CT) Scan Shows Typical Bilateral Symmetrical Horn-shaped Calcification in the Mesial Temporal Region.
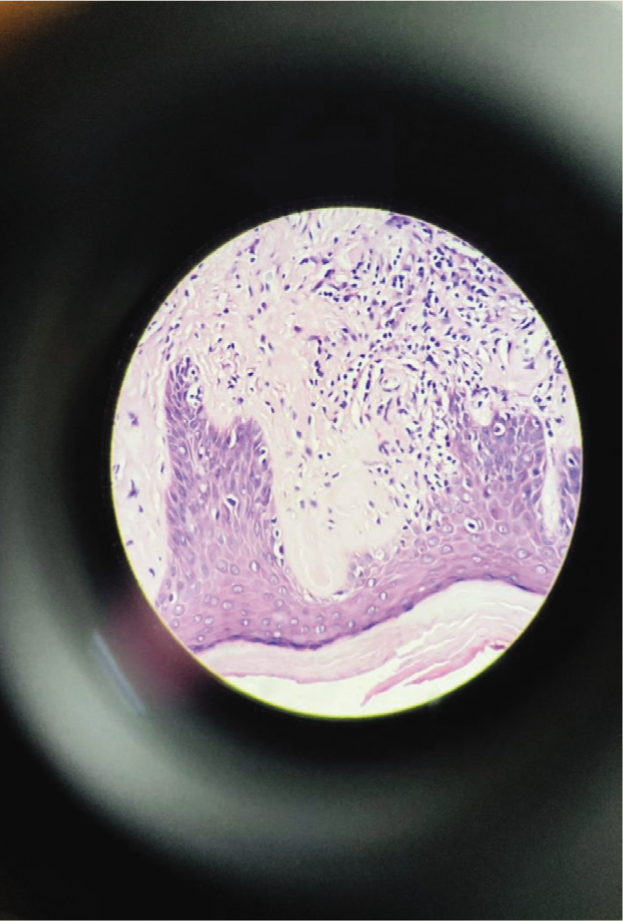
A dermatologist’s opinion on his skin condition and an otorhinolaryngologist’s opinion on his hoarseness of voice was sought. Histopathological examination of skin lesions as seen in Figure 2 exhibited depositions of pink hyaline Periodic acid Schiff (PAS)-positive material in the papillary dermis. Despite the unavailability of gene testing in our institute and related financial obstacles, targeted gene sequencing was outsourced. This revealed a pathogenic mutation in the extracellular matrix protein 1 (ECM1) gene, which confirmed the diagnosis of Urbach–Wiethe disease (lipoid proteinosis).
Histopathological Section Shows Deposition of Eosinophilic Homogenous Material in the Papillary Dermis of the Skin.
A 70-degree endoscopy showed a thickened, hard, and nonprotruding tongue; vocal cords were seen with difficulty, with the rest of the larynx being normal. The otorhinolaryngologist suggested a flexible endoscopy for further evaluation and laser ablation for the vocal cord lesion. He was started on fusidic acid cream and capsule acitretin for skin lesions.
Psychiatric management included pharmacological treatment for psychotic symptoms and behavioral interventions for mild autistic symptoms. Treatment commenced with tablet risperidone, lorazepam, and oxcarbazepine, keeping in mind the drowsiness reported on earlier medications. Mr. X is compliant with medications without any significant adverse effects. Social skills therapy and anger management training were started with regular consultations with a clinical psychologist. The patient has been in regular follow-up for the past four months now and has demonstrated substantial improvement in psychotic features and behavioral complaints with a BPRS score of 19. He interacts better, and his social functioning has improved. As seen in our patient, improvements in behavioral complaints are possible, but the overall condition of lipoid proteinosis tends to have a chronic and progressive course. 3
Case 2
This case involves a 16-year-old male, Mr. Y, who is the younger brother of Mr. X. He came to the Outpatient Psychiatry Department with his parents, where they reported concerns regarding his behavior for the past six months, where he would frequently indulge in verbal altercations, specifically with his mother and elder brother. At times, he would abuse them verbally as well as physically, which was unusual for his premorbid self. These behavioral outbursts would last for 30–40 minutes, after which the patient would be calm. At times, he would get aggressive for no reason. Furthermore, the patient would not comply with the mother’s requests regarding household chores and homework, leading to frequent conflicts among them.
He would typically not listen to his mother and rather do the opposite of what was told. There was no history suggesting aggression toward animals, deceitfulness, destruction of property, or hyperactivity. He had intermittent explosive symptoms but did not amount to a disorder.
He presented with various discrete skin lesions scattered across his body along with hoarseness of voice since early childhood. A notable family history of a similar skin-related neuropsychiatric condition was observed in his elder brother, as seen in the case mentioned above.
Birth, development, and scholastic history were age-appropriate. He was a thinly built male with whom rapport and eye contact were easily established. His mood was dysphoric without other significant MSE findings.
Blood investigation and systemic examination turned out to be normal.
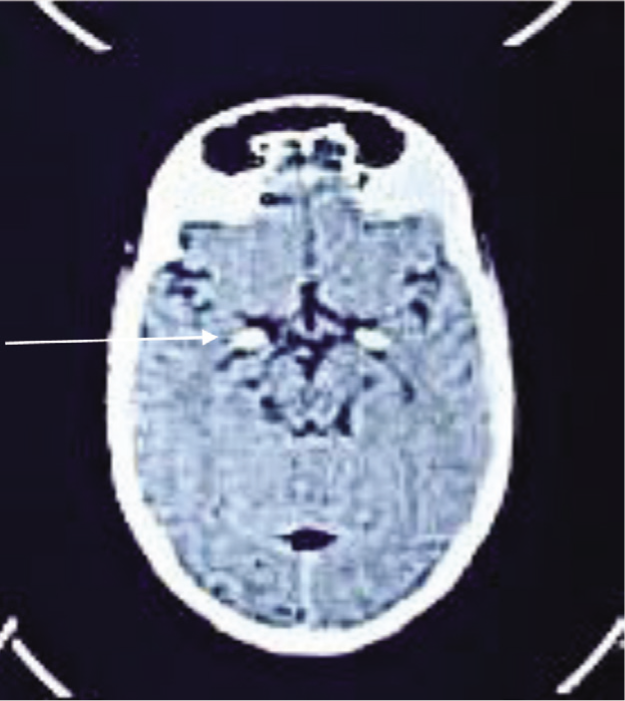
Neuroimaging was done, which showcased oval-shaped calcification involving the mesial temporal region and cisterna magna of the brain as seen in Figure 3. The dermatologist started him on capsule acitretin and fusidic acid ointment. The otorhinolaryngologist advised indirect laryngoscopy, which showed thickened vocal cords, for which carbon monoxide laser ablation was suggested.
Computed Tomography (CT) Scan Shows Bilateral Oval Symmetrical Calcification Involving the Mesial Temporal Lobe.
Histopathological examination of skin lesions showed deposition of pink hyaline PAS-positive material in the dermis, confirming the diagnosis of Urbach–Wiethe disease (lipoid proteinosis).
No psychopharmacological line of treatment was commenced immediately, but counseling sessions were conducted. Parents were psycho-educated regarding the symptomatology of neuropsychiatric sequelae of lipoid proteinosis. Cognitive behavioral therapy (CBT) focusing on anger management and operant conditioning was started. The parents report a gradual improvement in following commands. Further repeated sessions are arranged with the patient and his parents.
Discussion
Schizophrenia is one of the psychiatric disorders associated with lipoid proteinosis. 10
Paranoid psychosis is often seen as a manifestation of organic brain disorder of the medial temporal lobe. 11 Various studies have depicted the significant role of the medial temporal lobe in social cognition and fear processing.12-16 Thornton et al. suggest that the high prevalence of temporal calcifications in lipoid proteinosis is consistent with neuropsychological dysfunction as well as anxiety, psychotic, and mood disorders. 4 One of the reasons for the development of paranoid symptoms is also thought to be psychosocial, where patients may be reacting to their disfigurements and impairments caused by persistent skin lesions. 3
Among the medial temporal structures, the amygdala is the primary center for both emotional and sensory integrative functions, threat assessment, facial emotional recognition, and modulation of aggressive behavior.3,17 Studies have shown that amygdala damage is apparent in 50% of reported cases of Urbach–Wiethe disease. 18
Our cases of the two siblings with lipoid proteinosis highlight the distinctive clinical presentation, diagnostic challenges, and comprehensive management of this rare genetic disorder. The paranoid symptoms of lipoid proteinosis have similarities with schizophrenia phenomenological, as evidenced by biochemical and structural changes in brain areas consisting of the hippocampus, parahippocampal gyrus, and amygdala. 19
Both of our cases are siblings and first-degree relatives, and both of them mani-fested typical features of lipoid proteinosis such as hoarseness of voice, mucocutaneous lesions, and pathological intracranial calcifi-cations. In addition, both of them demonst-rated episodes of impulsivity, irritability, and behavioral disturbance. The elder brother showed features of grandiose and paranoid ideations, whereas the younger brother showed defiant behavior. Repeated regular follow-ups over six months were done. The rare occurrence of lipoid proteinosis limits the generalization of its findings.
Conclusion
To date, palliative and conservative treatment options are the mainstay of managing Urbach–Wiethe disease. Longitudinal studies with regular follow-ups of patients with lipoid proteinosis should be done to evaluate periodic changes in psychiatric symptomatology. Treatment incorporating pharmacotherapy and psychotherapy resulted in substantial improvements in chronic neuropsychiatric symptoms, demonstrating the effectiveness of a comprehensive approach.
Relevant imaging studies and investigations helped confirm the presence of characteristic brain calcifications and ECM1 gene mutations needed to diagnose this disease. Regular specialized consultations and referrals are helpful for a desirable outcome.
With these two cases, we want to convey that the onset of Urbach–Weithe disease is usually in childhood, with peculiar manifestations of hoarseness of voice and typical skin lesions, which can help in its early detection and timely management. Neuropsychiatric manifestations usually appear late (in adolescence) in the disease course, which can be better prevented and managed with early diagnosis and a holistic care approach. Furthermore, this case series will enrich the literature regarding neurocutaneous disorders with genetic predisposition.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration of Patient Consent
Informed written consent, as well as permission to use the patient’s clinical information and images for publication, has been taken. The patients understand that efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Declaration of the Use of Generative AI
Nil. We assume full responsibility for the entire content of the manuscript.
Funding
The authors received no financial support for the research, authorship and/or publication of this article. Informed written consent and permission to use the patient’s clinical information and images for publication have been taken. The patients understand that efforts will be made to conceal the identity, but anonymity cannot be guaranteed.