
Abstract
Lipoid proteinosis (LP) is a rare inherited multisystem disease. Classical clinical features include beaded eyelid papules, laryngeal infiltration, and neurological symptoms. Here, we report the diagnosis and treatment of a female patient with LP in order to improve physician awareness and understanding of this disease.
Introduction
Lipoid proteinosis is a rare autosomal recessive genodermatosis. It is also referred to as Urbach-Wiethe disease or hyalinosis Cutis et mucosa, and was first described in 1929 by Urbach and Wiether of Vienna. 1 The name lipoid proteinosis originated from the pathological features of skin tissue that showed abnormal lipid and protein deposition. The lesions of lipoid proteinosis mainly involve the upper respiratory mucosa and skin. Hoarseness is usually the primary clinical manifestation of this disease. Lipoid proteinosis is found throughout the world and approximately 400 cases have been reported. 2 Because of its rarity, many physicians are not familiar with its signs and symptoms, which may cause the disease to be misdiagnosed as chronic hypertrophic laryngitis or laryngeal amyloidosis.
Case Report
A 58-year-old female presented at the Ear, Nose, and Throat Clinic with hoarseness since childhood. Fourteen years earlier, she underwent a vocal cord operation at a local hospital; however, detailed diagnostic and treatment information were not available. During the past two months, the patient had suffered from increased hoarseness. In order to observe the vocal cords, a fibrolaryngoscopy was performed and showed widespread lipoid proteinosis infiltration, which had led to areas waxy yellow plaques on the back of the soft palate, the posterior pharyngeal wall, the bilateral palatoglossal arch, the full length of bilateral vocal cords, and the laryngeal posterior commissure (Figure 1A-1C). Mucosal edema could be seen at the bilateral vocal fold edges, and the right edges showed changes consistent with Renke’s edema (Figure 1D). The movement of bilateral vocal cords was normal, but the lesions led to a reduced vocal fold mucosal wave, stiff mucosa, and incomplete glottic closure. Multiple beaded papules could be seen along the upper eyelid margins (Figure 2A, 2B). The oral floor mucosa was infiltrated and the lingual frenum was shortened and stiff (Figure 2C). Bilateral elbows showed thickening and pigmentation (Figure 2D, 2E). Subsequently, the patient underwent direct laryngoscopy under general anesthesia. The bilateral vocal cord edema and partial infiltration lesions were removed and the patient’s voice improved. Biopsies posterior pharyngeal wall and vocal cord tissue supported a diagnosis of lipoid proteinosis (Figure 2F, 2G). To explore family history, we investigated a total of 25 people in the patient’s family tree dating back three generations. The patient’s parents were not close relatives and she had four sisters, one brother, and no children. Only the eldest sister of the patient had suffered from hoarseness since childhood. Unfortunately, all family members did not agree to genetic testing. Fibrolaryngoscopic features of the patient. A, Lipoid proteinosis infiltration of the soft palate (a) and posterior pharyngeal wall (b). B and C, Lipoid proteinosis infiltration of bilateral palatoglossal arch (B: right; C: left). D, Lipoid proteinosis infiltration of bilateral vocal cords and the posterior commissure ; Renke’s edema changes of the right fold edge. Typical characteristic images from the patient examinations. A and B, Multiple beaded papules along upper eyelid margins (A: left; B: right). C, Lipoid proteinosis infiltration of the oral floor mucosa and stiffness of the lingual frenum. D and E, Pigmentation of bilateral elbows (D: right; E: left). F, The mucosal stroma shows diffuse pink homogenous deposits, and the vascular wall is thickened and denatured (H&E×200). G, PAS ( + ) ×200.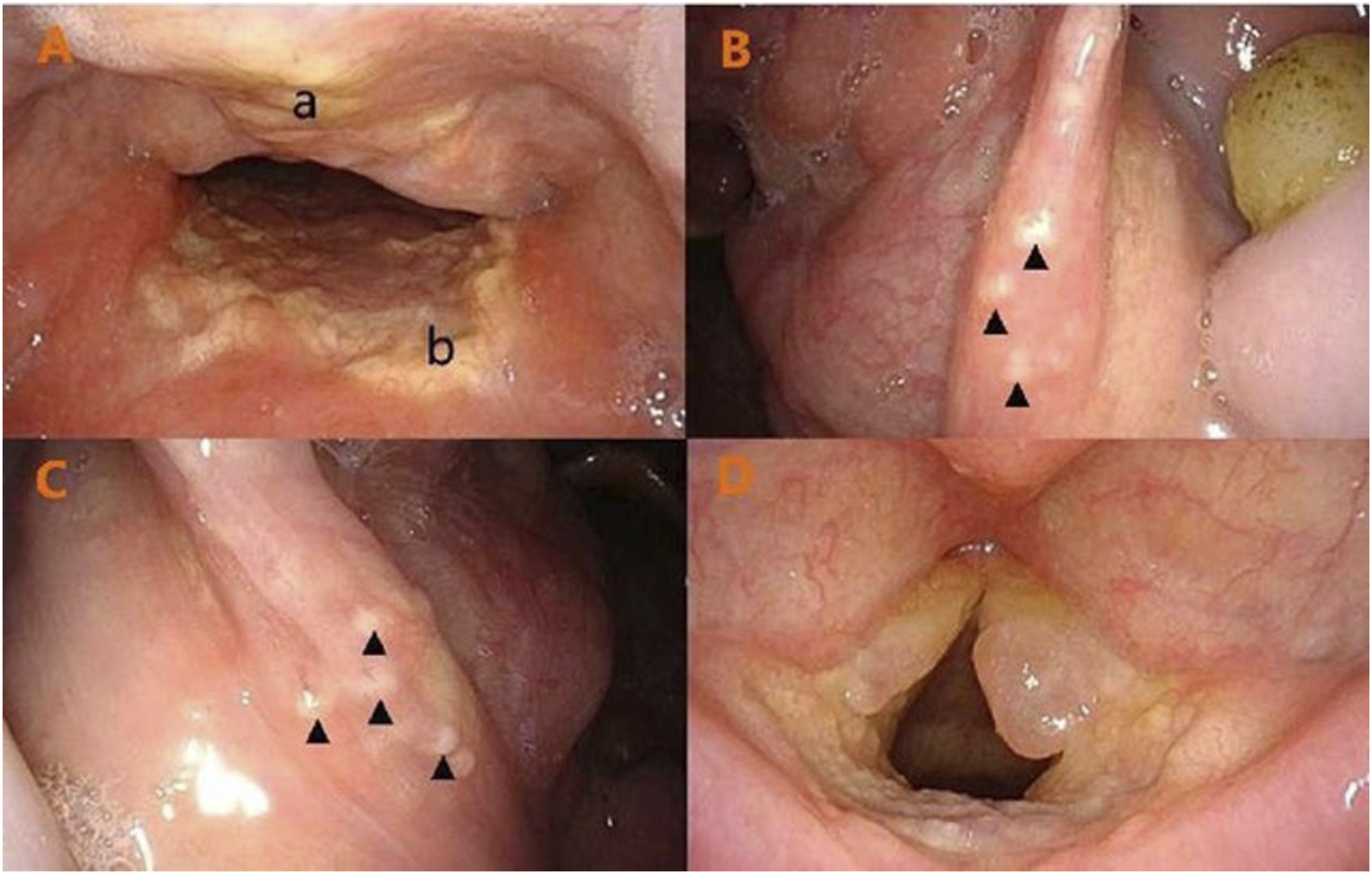

Discussion
Lipoid proteinosis usually presents with features related to injury of the skin, mucosal membranes of the upper respiratory tract, and the neurological system. The mucosal lesions mainly manifest as yellow waxy plaques under the mucosa. Hoarseness may be the predominant sign of a laryngeal abnormality. Infiltration of the tongue frenum may lead to tongue inflexibility and shortening, which affects movement of the tongue. Obvious thickening of local skin is the main feature of the skin lesions, and is especially found on the elbows, knees, and armpits. Beaded papules occur when infiltration involves the eyelid. Neurological abnormalities include schizophrenia, depression, anxiety, epilepsy, memory loss, and schizophrenia. Bilateral circumscribed and symmetrical calcification in the medial temporal may be detected by MRI. However, such neurological symptoms are not common and patients rarely undergo MRI; therefore, the neurological signs of lipoid proteinosis can be easily ignored.
In recent years, molecular genetic studies have shown that the extracellular matrix protein 1 (ECM1) gene located on chromosome lq21 can mutate into the pathogenic gene associated with lipoid proteinosis. 3 Because it is a rare progressive autosomal recessive disorder, the clinical manifestations of lipoid proteinosis are diverse and atypical, and especially in the early stage. ECM1 gene analysis is an efficient way to diagnose lipoid proteinosis 4 ; however, genetic testing has the disadvantages of high price and the need for family blood collection, thus tissue biopsy is more widely used in the clinic to make the diagnosis. The typical pathological feature of proteinosis is extensive deposition of transparent substances in the dermis, submucosa, and around blood vessels. The transparent substances stain PAS positive and Congo red negative.
Because lipoid proteinosis is a genetic disease, there is currently no effective treatment. While the reported experimental treatments include oral steroids, oral dimethylsulfoxide, oral D-penicillamine, and oral acitretin, 5 no such study has enrolled a large cohort of patients and any evidence for treatment effectiveness is insufficient. Although treatment is difficult, the life expectancy of individuals with lipoid proteinosis is normal. Surgical treatment is appropriate for some specific cases, such as those involving infiltration of the vocal cords and beaded papules on the eyelids. In the present case, the patient’s hoarseness was not only due to lipoprotein deposition, but also due to Renke's edema, which together led to severe abnormal pronunciation. Lipoprotein deposition combined with Renke’s edema is very rare, and anatomical abnormalities and compensatory vocal efforts may contribute to those lesions. Renke’s edema and some lipoprotein deposits were removed during the operation, and the edges of the vocal cords were trimmed, which improved the patient's pronunciation.
In summary, lipoid proteinosis is a rare disease involving multiple systems. Its symptoms are atypical and can be easily misdiagnosed. Therefore, it is necessary to improve the understanding of the disease and conduct more intensive research.
Footnotes
Declaration of Conflicting Interests
The authors declared having no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethics Committee of Yuhuangding Hospital, Yantai, Shandong province, China.
Informed Consent
The patient’s privacy was protected and the patient herself provided signed informed consent for her anonymized information to be published in this article.