
Abstract
Background:
Electroconvulsive therapy (ECT) is a safe and effective treatment option for various psychiatric disorders. However, its widespread use is limited by prevalent negative attitudes and stigma, not only within the general public but also among healthcare professionals. This study aimed to develop and validate a workshop-based educational module, titled the “Basic Course in ECT,” for medical students.
Methods:
The curriculum development framework was used to develop the educational module. The content of the educational module was developed through expert consensus involving two rounds of the Delphi method. Faculty members provided feedback to validate the workshop content. A total 33 interns participated in the workshop. Student satisfaction was assessed using a feedback questionnaire.
Results:
Eight content areas were identified through a literature review. The Delphi consensus with 15 experts resulted in 10 topics being incorporated into the educational module. The module demonstrated strong face validity, as indicated by a content validity index of 1. Participants expressed high satisfaction with the workshop module regarding content, teaching methods, and time allocation. Feedback indicated an improvement in knowledge and a positive attitude toward ECT.
Conclusions:
The “Basic Course in ECT” was developed using expert consensus and validated for use with medical students. It can be integrated into the undergraduate curriculum.
Keywords
There is a lack of knowledge and prevalent negative attitudes regarding ECT among medical students. Training in ECT needs to be improved in the current undergraduate curriculum. The “Basic Course in ECT” was developed and validated for medical students and well perceived.Key Message:
Electroconvulsive therapy (ECT) is a safe and effective treatment option for several psychiatric disorders, including schizophrenia 1 and mood disorders. 2 It is a lifesaving option for psychiatric emergencies, such as suicidality and catatonia. Despite its proven efficacy, there is a prevalent negative attitude and stigma among the general public, partly fueled by negative portrayals in the popular media and cinema, 3 as well as the influence of antipsychiatry movements. 4 Widespread misconceptions, such as viewing ECT as a “cruel,” “barbaric,” and “outdated form of treatment” option that should be banned or associating it with “punishment for violent patients,” contribute to the prevailing negative sentiments. These factors limit the acceptability of ECT as a treatment option among patients. A similar negative attitude toward ECT is prevalent among medical students,5,6 which could be caused by insufficient training and exposure to ECT within the undergraduate curriculum.
Training in psychiatry for undergraduate medical students in India currently needs to be improved, with recent proposals to extend the existing four-week psychiatry posting to six weeks. 7 The undergraduate medical curriculum needs more exposure to ECT, which receives only cursory mention. Recognizing that medical students are future healthcare professionals, altering their perceptions regarding ECT could significantly impact the public understanding of ECT as a treatment option and its acceptability.
Influence from popular media, including cinema, is a common source of misinformation regarding ECT, often depicting it frighteningly with exaggerated portrayals that do not reflect actual clinical practice. 8 Furthermore, anti-ECT activism has further eroded public confidence in ECT.4,9 Addressing these negative attitudes requires multifaceted strategies, including awareness programs targeting patients, caregivers, and the general public.
Research indicates that firsthand experiences with ECT can reduce negative attitudes among patients and caregivers. Similar strategies have been used to educate medical and other health professionals about the usefulness of ECT. Some evidence suggests that brief educational interventions can improve knowledge and reduce negative attitudes toward ECT.10-12 Notably, the attitudes are more positive when the source of information is a health professional, potentially reducing stigma toward ECT and increasing its acceptability among medical students, which may translate into improved patient outcomes. There is currently no standard introductory course on ECT for undergraduate medical students in India. Hence, we aimed to develop and validate a workshop-based educational module, “Basic Course in ECT,” for medical students. We also studied medical students’ perceptions of the workshop-based educational module.
Materials and Methods
The framework on curriculum development by Thomas et al.
13
was used to develop the educational module. The following six steps were used for the study:
Problem identification and general needs assessment: The literature on knowledge and attitudes regarding ECT among the general population was reviewed to identify the need for educational intervention and to understand the current approaches to addressing this need. Needs assessment of the target learners: The literature on the knowledge and attitude toward ECT among medical students was reviewed. Additionally, the existing curriculum was examined to identify the need for formal training in ECT. Goals and objectives: The overall goal of the intervention was to improve knowledge and attitudes regarding ECT. Another objective was to evaluate the perceptions of medical students regarding the educational intervention. Educational strategies: The “curriculum content” was identified and validated using expert consensus. The content included discussions on myths and misconceptions about ECT, the standard procedure for assessment and treatment, and efficacy and safety data. The “educational methods” were chosen based on the feasibility of the intervention, incorporating interactive lectures, short videos, and case-based discussions. Implementation: Permission was obtained from the Dean for the educational intervention. A pilot study was conducted with a group of students to assess the feasibility of the intervention. Other faculty members were also involved in administering the intervention to the medical students. Evaluation and feedback: Feedback from the participants was collected regarding the curriculum content. This feedback will be incorporated into the educational module to enhance its quality. The educational module is planned to be integrated into the existing curriculum.
Development of the Educational Module
Educational interventions previously conducted to improve knowledge and change attitudes toward ECT were reviewed. Based on the identified deficiencies, the content of the educational module was prepared. The module was intended for medical students with no or minimal prior knowledge and exposure to ECT. A consensus method (the modified Delphi method), 14 using experts in the field, was used to finalize the curriculum content. The educational methods chosen were based on the module content. Initially, 24 experts in ECT were selected through purposive sampling. Two rounds of opinion generation were conducted. The experts were asked to suggest at least six components for the module. After the first round, the data were analyzed, and the summary of the results was sent back to the experts. Components with more than 70% agreement after the second round were included in the final module. 14
Validation of the Educational Module
Face validity was assessed through feedback from the faculty. A content validity index (CVI) 15 for the module was calculated based on the inputs from the experts using a 4-point Likert scale (1 = not relevant, 2 = somewhat relevant, 3 = quite relevant, 4 = highly relevant). The CVI was calculated as the number of experts rating the content as 3 or 4 (i.e., relevant) divided by the total number of experts. A CVI score of 1 was considered acceptable. 15
Perception of Students Regarding the Educational Module
Basic Course in ECT was delivered in a workshop format to a group of consenting interns at the Department of Psychiatry, Kasturba Medical College, Manipal, from December 2023 to January 2024. It was planned for 30 interns posted in the psychiatry, dermatology, or respiratory medicine department during the study period. The department faculty delivered the content in two sessions over half a day. Learning objectives were specified before the workshop. Participants completed an online Google form containing informed consent, sociodemographic details, and a feedback form. The feedback questionnaire included eight Likert-scale items ranging from “strongly disagree” to “strongly agree” and five open-ended questions for comments on positive and negative aspects and suggestions for improvement. This outcome measured only level 1 (reaction) on Kirkpatrick’s model of levels of learning evaluation. 16 Deductive content analysis 17 was conducted for the open-ended responses on the feedback forms.
Results
Based on the curriculum development framework by Thomas et al., 13 the needs of the learners were identified through a literature review. Then, the module was developed using a consensus method involving two rounds of Delphi for content generation.
Needs of the Learners Based on the Literature Review
Previous studies10-12,18-21 identified several deficiencies in the knowledge and attitudes toward ECT among medical students. These studies informed the development of the following content areas, which have been used in other intervention programs to enhance knowledge and attitudes regarding ECT: (a) relevance of ECT in modern psychiatric practice, (b) safety and efficacy of ECT, (c) administration of ECT, (d) practice standards in ECT, (e) legal aspects of ECT practice in India, (f) myths related to ECT, (g) how ECT is different from other forms of brain stimulation, and (h) recent advances in ECT. These areas were identified as critical for improving the knowledge and attitudes of medical students toward ECT, addressing existing gaps and enhancing the educational experience.
Experts’ Selection for Delphi Consensus
For consensus generation, 24 experts from various regions in India were invited via emails. Reminders were sent through WhatsApp and emails for prompt responses. Of the invited experts, 15 (62.5%) agreed to participate. Informed consent was obtained via email. Among the invitees, one (4.2%) refused to participate, one (4.2%) submitted a late response, and seven (29.2%) did not respond.
The First Round of Delphi
In the first round, the subject experts received a response sheet containing eight themes, which they could mark as “agree” or “disagree” and provide reasons or comments. Additionally, they could suggest other areas to be included in the module. Experts were requested to propose at least six topics to be covered. Fifteen participants completed the first round of the Delphi process. The analysis of the responses from the first round resulted in the identification of 17 topics suggested by the experts, including the eight topics initially proposed (Table 1).
Summary of the Delphi Consensus (N = 15).
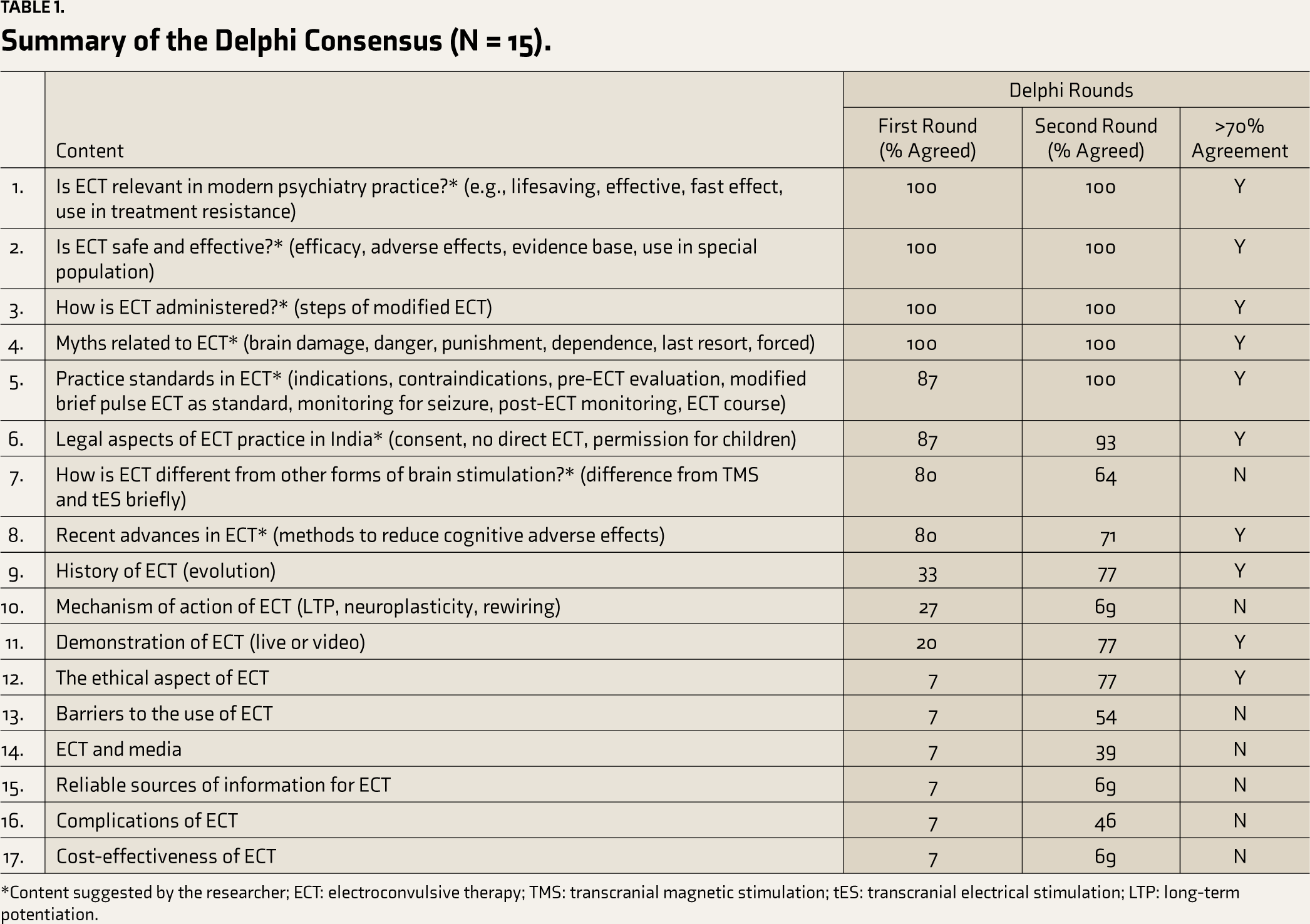
*Content suggested by the researcher; ECT: electroconvulsive therapy; TMS: transcranial magnetic stimulation; tES: transcranial electrical stimulation; LTP: long-term potentiation.
The Second Round of Delphi
The results of the first round were sent to all 15 experts, which included a list of 17 topics and the percentage agreement for each. Fourteen experts responded within the allotted time. From the summary of the second-round results, 10 topics reached the 70% agreement threshold established prior to the study (Table 1). Except for one topic “How is ECT different from other forms of brain stimulation?,” all other topics initially suggested by the researcher were endorsed by the experts.
ECT Workshop Modules
Based on the topics developed through the consensus process, two one-hour modules were developed (Table 2). The modules were delivered through interactive lectures. The specific learning objectives included: (a) to understand the evolution of ECT, (b) to understand whether ECT is relevant to modern psychiatry practice, (c) to understand whether modern ECT is safe and effective, (d) to explain the myths related to ECT, (e) to understand the practice standards in ECT, (f) to appraise the legal and ethical aspects of ECT, (g) to list the recent advances in ECT, and (h) to describe the procedure of ECT.
Content of the “Basic Course in ECT” Workshop Modules.
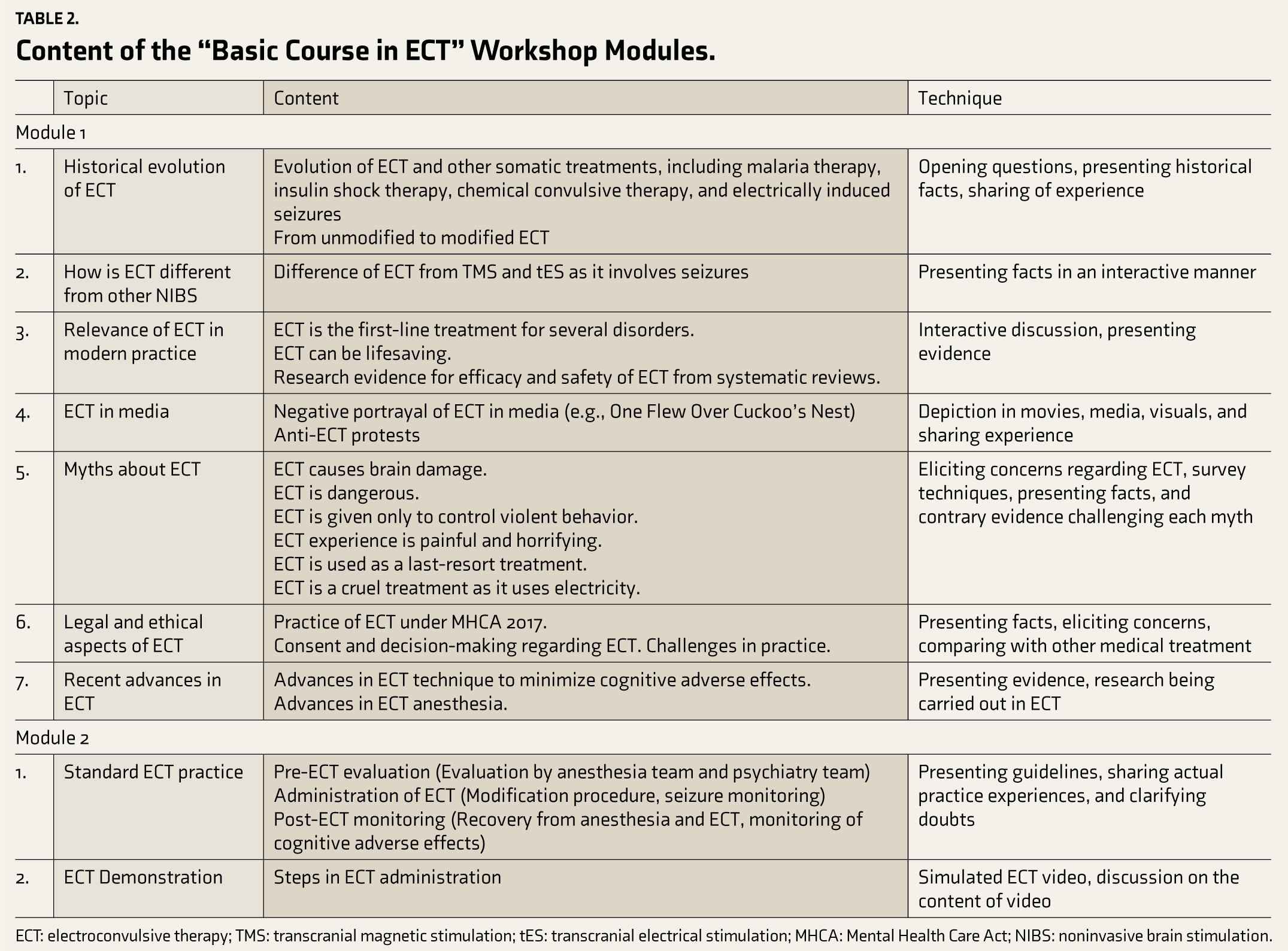
ECT: electroconvulsive therapy; TMS: transcranial magnetic stimulation; tES: transcranial electrical stimulation; MHCA: Mental Health Care Act; NIBS: noninvasive brain stimulation.
Validation of the ECT Modules
Face validity was assessed through feedback from three experts in the Department of Psychiatry. All three faculty members rated the content as highly relevant, with a score of 4. The CVI score was calculated to be 1, indicating good face validity.
Perception of Students Regarding the Workshop
During the study period, 33 interns attended the workshop. Participants (N=33) included 22 females (66%), with a mean age of 24.1 years (SD 1.9), mostly from urban backgrounds (93.9%), nuclear families (90.9%), and middle socioeconomic status (66.7%). Regarding prior exposure to mental illness, six participants (18.2%) had personal experience, 15 (45.5%) had a relative with mental illness, and 18 (54.5%) had a friend with mental illness. Only one participant (3%) reported prior experience with ECT administration in a friend. Most of the participants agreed that the module was relevant, participation was encouraged, content was well organized and useful, teaching methods were appropriate, and time was adequate (Table 3).
Feedback from Students on the Workshop (N = 33).
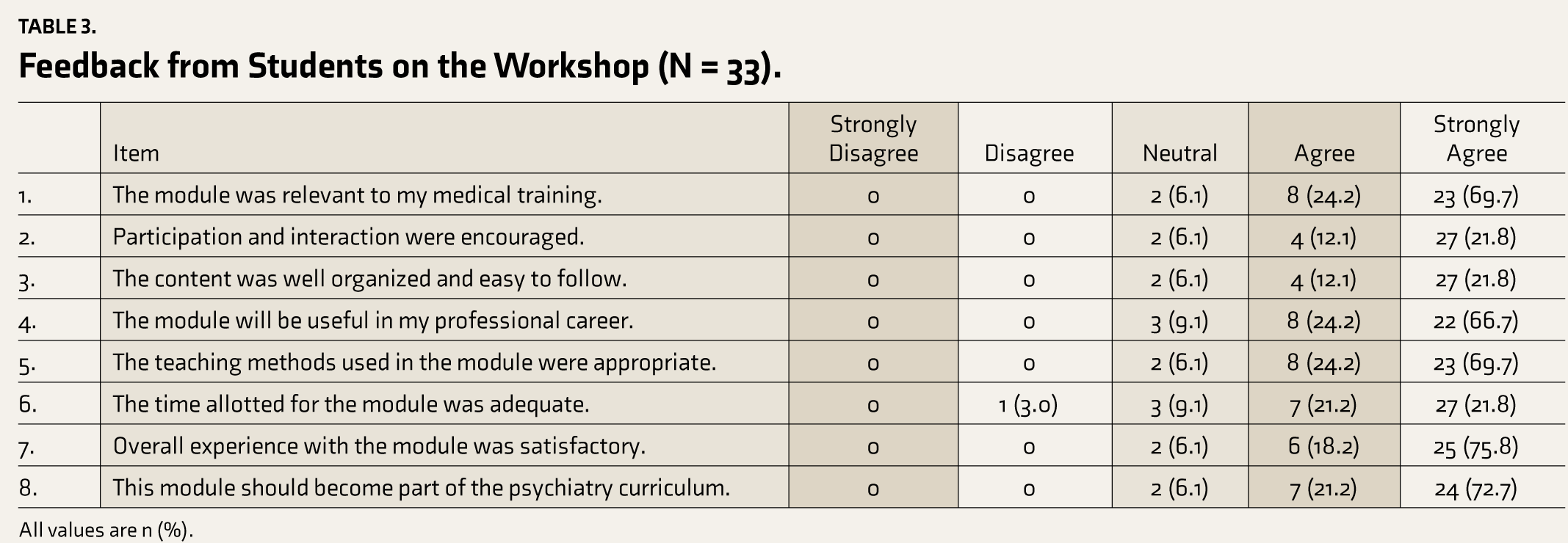
All values are n (%).
Content Analysis of the Qualitative Feedback
The qualitative feedback obtained is summarized below with examples.
How the workshop helped the participants: The workshop helped the participants gain knowledge regarding ECT and develop positive attitudes toward ECT.
Gained knowledge regarding ECT: Participants reported a better understanding of ECT in current practice.
After the workshop, four participants reported that they had gained specific knowledge regarding ECT. Some positive statements included:
“Gained the required basic knowledge about ECT to be able to answer relatives/patients.” (P2) “ECT can be a treatment modality, and contrary to the myths, it is rather a safe modality of treatment.” (P13)
Developed positive attitudes toward ECT: The participants’ negative attitudes toward ECT changed.
Six participants indicated that they developed a more positive attitude toward ECT and were more open to its use. Some comments were:
“Have a more holistic approach and opinion on ECT.” (P3) “Changed mindset about ECT.” (P21) “I would not hesitate to give ECT as a treatment option.” (P26)
One participant mentioned,
“Media portrayal of ECT has done a disservice to the procedure, and hopefully, I will not fall victim to similar disinformation campaigns.” (P11)
Seventeen participants acknowledged that they would educate others and advocate for ECT when clinically appropriate. Some statements were:
“To help people break their perception about ECT and actually use it as a line of treatment in psychiatric illnesses if required according to patient needs.” (P12) “Encourage ECT for people in need and attempt to remove the stigma surrounding it.” (P8) “Incorporate ECT into practice.” (P17) “Make people more aware of ECT.” (P23)
Positive feedback regarding the workshop: The positive feedback obtained included interactive style, interesting content, and positive intent.
Interactive style: Students appreciated the module content (n = 11) and the interactive presentation style (n = 11).
One student mentioned,
“How it focused on removing the negative image of ECT developed over the years due to false media and reassured through data that ECT is the safe and first-line treatment in many lifesaving scenarios.” (P10) Many (n = 7) felt that all doubts were clarified during the sessions. “… cleared the doubts efficiently.” (P9) “Clearing out myths which most people, including health professionals, have regarding ECT.” (P15) “Myths were tackled well.” (P27)
Interesting content: The content was appreciated by the participants, including the flow and video demonstration.
Another student mentioned,
“… Liked the part where the history of medical procedures was discussed. Helped ease into the discussion regarding how induction of convulsions as a therapy should not be seen farfetched ….” (P11) Several students (n = 5) expressed satisfaction with the video demonstration of ECT.
Positive intent: Participants recognized the intent of the researchers.
Two participants appreciated the intent behind the workshop:
“Intention of the staff to spread information for the benefit of the society.” (P6) “It is a novel idea to implant a seed in the minds of young doctors and dispel myths and educate them regarding ECT.” (P14) One student identified that it was not covered well in the curriculum, “Learnt a new concept never touched upon during ug course.” (P3)
Suggestions for change
Experiential content: This includes adding live demonstrations, videos, images, case studies, and patient experiences for experiential learning. Ten students suggested improving the module by including a live demonstration of ECT with an actual patient:
“I would have liked a more practical approach and have hands-on experience.” (P13) “The practical aspect could be done alongside a patient who has undergone ECT for a better understanding of the outcome.” (P5) Four participants suggested including more videos and images, and three suggested incorporating case studies. Balancing the content: Some older concepts can be reduced, while newer concepts can be added or elaborated. Two participants suggested reducing the historical aspects, and one suggested including details of the mechanism of action of ECT:
“As a course for medical students, a bit more information on the method by which ECT works would be beneficial. I am not aware whether it is well understood in the first place, but by the tenets of evidence-based medicine, I would be more confident recommending ECT if I were more aware of how it works.” (P11)
Discussion
The “Basic Course in ECT” was developed using the curriculum framework of Thomas et al., 13 which includes needs assessment, goal identification, content development through expert consensus and validation, appropriate educational strategies, feasibility testing, and feedback integration. Students appreciated the workshop, recognizing it as an effective means to change their knowledge and attitudes toward the use of ECT for the treatment of mental illnesses (Kirkpatrick’s level 1). 16
We used a modified Delphi technique14,22 to develop the contents of the educational module. The Delphi technique is particularly useful for obtaining consensus from a group, as suggested by Turoff. 14 This technique has been effectively used in developing educational content, such as the Stigma, Empathy, and Attitude educational module for medical students by Praharaj et al. 23 Our expert panel was selected based on their expertise and willingness to participate, with two-thirds of the invited experts agreeing to contribute. To enhance response rates and quality, we used written communication and sent reminders via emails and WhatsApp, as recommended in previous studies. 14 Responses with more than 70% agreement after the second round were included in the final module, following Sumison’s recommendation. 24 It is worth noting that other cutoffs have been proposed, ranging from less stringent (e.g., 50% by McKenna 22 ) to more stringent (e.g., 80% by Green et al. 25 ).
The “Basic Course in ECT” effectively improved knowledge and attitudes among medical students, consistent with the findings from previous studies on brief educational interventions.10-12,18-21 Balhara et al. 10 used a “Brief ECT Orientation Module,” comprising a one-hour lecture on ECT and, where feasible, a demonstration of modified ECT during psychiatry postings. This lecture covered “historical aspects, indications, mechanism of action, procedure, adverse effects, and effectiveness of ECT,” as detailed in standard textbooks. 10 In contrast, our module, developed through expert consensus, included additional elements such as myths, standard practices, legal and ethical aspects, and recent advances in ECT. Participant feedback highlighted their appreciation for these additional components. One notable feature of the module by Balhara et al. 10 was the actual demonstration of ECT, which our participants also suggested for more hands-on experience. This aligns with the concept of experiential learning, where learning is “situated” and practice-based, providing authentic experiences. 26 However, as Balhara et al. 10 noted, providing such exposure to a large group of students may be challenging.
A video demonstration of ECT could be a suitable alternative, as shown in our study. Similar video-based education for ECT was carried out by Nagarajan et al., 12 who used simulated patients for the caregivers of patients. Video-based educational materials have been used for training students regarding ECT in previous studies (e.g., Panwala et al. 20 and Kitay et al. 27 ) and have proven effective in improving knowledge and attitudes toward ECT. Indeed, Warnell et al. 19 demonstrated that both live demonstration and video-based methods were almost equally effective in improving knowledge and attitudes toward ECT, with live demonstration being marginally superior. They reported that the duration of clerkship is more important than the instructional methods. 19 It is possible that more time spent during actual postings increases interaction with psychiatry faculty, thereby significantly affecting the knowledge and attitudes toward mental illnesses, including ECT. In our study, students also identified “more interactions” and “effectively clearing doubts” as particularly helpful.
A similar “Brief ECT Orientation Module” for nursing students, comprising a lecture, video demonstration of direct and modified ECT, and preparation of patient and equipment during live ECT, was studied by Panwala et al. 20 and found to improve knowledge and positive attitudes toward ECT. Lecture-based methods alone may not be very effective in changing knowledge and attitudes, as shown by Kinnair et al., 18 who found that a combination of watching ECT and attending a lecture was superior to a “lecture-only” intervention. Another study from India by Sai et al. 28 found that interns who had observed ECT during their clinical rotations had more positive attitudes toward ECT.
The teaching methods employed in the workshop involved interactions leading to active engagement of the students, which the participants also perceived. Discussions during interactive lectures provided opportunities for participation, active learning, cooperative learning, and the development of critical thinking.29-31 Including common myths related to ECT helped engage the students in the discussion and offered more opportunities for clarifying their concepts and understanding of ECT. This was apparent in the feedback from one participant who noted, “How it focused on removing the negative image of ECT developed over the years due to false media and reassured through data that ECT is the safe and first-line treatment in many lifesaving scenarios” (P10). Challenging popular beliefs with scientific evidence can be an effective way to change negative attitudes among students. Additionally, debates could be another effective method to involve students in discussing controversial topics. 32
Implications of the Study
The “Basic Course in ECT” was found to be effective and acceptable among medical students. It can be integrated into the existing undergraduate curriculum after incorporating student feedback to refine the module and recommendations from the curriculum committee and undergraduate board of studies. Specific suggestions include discussing the mechanism of ECT in more detail, adding more videos and images, using case studies, and potentially including live demonstrations. The course can also be offered to medical students at other colleges to spread awareness about ECT. Furthermore, it can be suitably modified and offered to other course students in other disciplines, such as dental and nursing programs. Once this educational innovation is implemented, it will likely increase the awareness of ECT as a treatment modality among medical students and potentially reduce negative attitudes and stigma related to ECT. This could translate into greater awareness and acceptability of ECT among the patient population, thereby improving clinical outcomes.
Limitations
The study had a few noteworthy limitations. Although a wide range of experts were invited to participate in the consensus, researchers’ bias could have excluded potential experts, and some were excluded because of nonparticipation. Only the face validity of the workshop content could be established; therefore, more studies are needed to establish content and ecological validity. Additionally, because of feasibility issues, only interns could be included in this preliminary study.
Conclusion
The “Brief Course in ECT” was developed and validated using expert consensus. Preliminary findings from this study suggest that the content of this educational module is effective in improving knowledge and changing negative attitudes. The course was well received by the students and could be integrated into the psychiatry curriculum with suitable modifications. Further studies are needed to document the effectiveness of this educational intervention beyond Kirkpatrick’s level 1. Additionally, incorporating this “Brief Course in ECT” into nursing, dental, and other curricula could generalize its applicability in diverse settings.
Footnotes
Acknowledgements
We thank the Advance Course in Medical Education faculty, NMC Nodal Center for Faculty Development, Government Medical College, Kottayam for their suggestions on the study protocol, and the Dean and MEU faculty of Kasturba Medical College Manipal for the permissions and necessary support to facilitate the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
The authors assume full responsibility for the entire content of the manuscript. No parts of this manuscript were generated by any AI tool.
Ethical Approval
The study protocol was approved by the Departmental Scientific Committee and Institutional Ethics Committee of Kasturba Medical College and Kasturba Hospital (IEC 351-2023 dated 16.10.2023). Permission was obtained from the Dean of Kasturba Medical College, Manipal to conduct the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from all the participants.