
Abstract
Introduction:
Exposure to sexually explicit media influences the sexual knowledge, attitudes, and behavior of youth, so studying this among medical students is of utmost importance.
Aim:
To study sexual knowledge, attitudes, behaviors, and sources of influence among medical students.
Methodology:
A descriptive, cross-sectional, analytical, web-based study was conducted to assess sexual knowledge, attitudes, behaviors, and sources influencing sexuality in medical students via Google Forms. The form consisted of three parts: the first part was an information sheet and consent form, the second part included the participant’s sociodemographic data and the third part related to two study tools, the Sexual Knowledge and Attitude Questionnaire-II (SKAQ-II) and the sexual behavior and sources of influence scale.
Result:
A total of 300/950 (31.5%) medical students responded to the Google questionnaire. Their mean age was 20.43 ± 1.87 years (range: 18–26 years). The mean score for sexual knowledge and attitude was 24.35 ± 4.93 and 23.79 ± 4.87, respectively, which suggested that they had good sexual knowledge and liberal attitudes toward sexuality with female preponderance. As student’s academic year progresses, their sexual knowledge improves. There was a significant strong positive correlation between sexual attitude and knowledge with a Pearson correlation of r = 0.95, P = 0.004, which means the higher the knowledge, the better the attitude. Medical student’s engagement in sexual behaviors with self- and others was at age 18.45 years. The internet was the major source for getting information related to sexual behaviors for them, but they relied on doctors and friends for guidance.
Conclusion:
Medical students had adequate sexual knowledge, which was the reason for their liberal attitude toward sexuality. Their major source of sexual knowledge was the internet, although they confided in doctors for sexual doubts.
Medical students’ adequate sexual knowledge, their proper attitude toward sexuality, and appropriate sexual practices are of utmost importance as they influence their own health as well as the community’s positive health at large because they are future healthcare providers to the community.Key Messages:
Sexuality is one of the most basic human experiences where every individual has their views, thoughts, beliefs, and attitudes about sex. 1 Sexual knowledge refers to the knowledge regarding sexuality, myths, and misconceptions about reproduction, pregnancy, masturbation, abortion, fertility, methods of contraceptive use, and sexually transmitted diseases.2,3 Sexual attitude refers to a person’s attitude toward sexuality or sexual behaviors. 4 In one study about sexual knowledge, attitudes, and behaviors of urban youth, knowledge about the physiology of the sexual response cycle, conception, and pregnancy was less than masturbation, contraception, etc. and boys had liberal attitudes and more frequent sexual behavior than girls. 2 Another study of knowledge, attitude, and behavior about premarital sex in the young population of urban slums, only 17% were aware of safe sex, and 22% reported that first-time intercourse might lead to pregnancy. 5 Sexual health is crucial for the overall well-being of college students. Lack of adequate knowledge and skills for protection leads to unwanted pregnancy, unsafe abortions, sexually transmitted infections, and mental health issues. 6 As future healthcare providers, medical students must possess proper sexual knowledge and attitude to provide supportive, non-judgmental information to patients. Nevertheless, because of cultural and social taboos, their subjective discomfort, embarrassment, and perceived lack of time and training, they are unable to discuss sexual health. 7
In India, sexual and reproductive health services are not easily available or provided in a way that makes recipients feel embarrassed or unwelcome. Open communication about sexuality with teachers and parents is lacking, leading to reliance on other sources like peers, pornographic materials, books, magazines, the internet, media, etc. 1 There is a paradigm shift of sexual health from a religious outlook for procreation to satisfying basic human urges without commitment. Easy availability of explicit sexual content may develop undesirable sexual behavior. 8
Thus, lack of proper knowledge about sex, less influence of religious and cultural factors, rapid urbanization, early age of sexual maturation, and easy availability of sexually explicit content to young people than ever before increase their vulnerability to being involved in risky behaviors. Few studies has been conducted on sexual knowledge, attitude, and behavior,4-6 and very few studies reports the sources of influence on their knowledge, attitude, and behaviors. 9 So, we aimed to explore current sexual knowledge, attitudes, and behaviors among medical students and their sources of influence, and also the relationship among these variables, if any.
Objectives
To study sexual knowledge, attitudes, behaviors, and sources influencing sexuality in medical students.
To assess the relationship between knowledge, attitudes, behaviors, and sources of influence with other variables.
Methodology
Study Population
The study was conducted in a single medical college in the western part of India, with a recent annual intake of 200 seats. A total of 950 medical students were invited to participate.
Study Design
Descriptive, cross-sectional, analytical, web-based study.
Study Period
Three months from June to August 2023, including a data collection period of 1 month, that is, 1st June to 30th June.
Inclusion Criteria
Medical students consenting online to participate in the study.
Study Procedure
Approval from the Institutional Human Ethics Committee was obtained before the commencement of the study. All medical students approached batch-wise via a preexisting WhatsApp group through messages explaining the nature and purpose of the study and were invited to take part. A link to the Google form with written informed consent was sent to medical students. Reminders were sent at intervals of 7 days up to a total duration of 30 days.
Study Questionnaire
The Google form consisted of three parts. The first part was the participant information sheet and consent. After consenting, the participants were directed to the second part, which included sociodemographic data such as age, gender, religion, marital status, education, domicile, etc. The third part was related to two study tools: the Sexual Knowledge and Attitude Questionnaire-II (SKAQ-II) and the sexual behavior and sources of influence scale.
Study tools:
SKAQ-II:4,15 A self-administered SKAQ in Hindi was constructed and standardized by Avasthi et al.
4
to assess sexual knowledge and attitude of the North Indian population toward sex. It was developed as an adaptation from the original tool, the Sex Knowledge and Attitude Test, by Lief & Reed.
10
SKAQ-II tool widely utilized and standardized in North Indian population11-13 and other Indian populations.9,14-19 We utilized a self-administered English-translated version of SKAQ-II,
15
as our study population was medical students. Kumar et al.
15
used the English version of SKAQ-II to find out the sexual knowledge and attitudes of undergraduate medical students. It includes a 35-item knowledge part consisting of dichotomous scoring with the maximum attainable score of 35. The attitude part has 20 items, scored on a three-point linear scale (0–2), with a maximum obtainable total score of 40. Higher scores, better knowledge, and a more liberal attitude. Its test-retest reliability is 0.43 for attitude and 0.66 for knowledge. Sexual Behavior and Sources of Influence Scale:
9
It was developed by Dutt et al.
9
in 2017 to assess sexual behavior and sources of influence. The scale was divided into two sections: one for assessing sexual behavior and the other for assessing sources of influence. The scale was scored on a five-point Likert scale. The sexual behavior section was further divided into three subsections: (a) sexual behaviors through various sources of media, (b) sexual behavior with self and others, and (c) lack of interest in sexual activity. The assignment of “low,” “moderate,” “high,” and “very high” for the subsection sexual behaviors through media was 6–12, 13–18, 19–24, and 25–30, respectively; for the subsection sexual behaviors with self or others, it was 15–30, 31–-45, 46–60, and 61–75, respectively.
Statistical Analysis
Descriptive statistics were shown with the help of mean and standard deviation for quantitative data, and qualitative data were described with frequency and percentage. For dependent continuous variables, unpaired T-test and ANOVA were used with post hoc Tukey HSD. Pearson correlation between both quantitative scores of sexual knowledge and sexual attitude was determined. Data analysis was done using MS Excel. P <0.05 was considered statistically significant.
Results
This study examined sexual knowledge, attitude, behavior, and sources influencing sexual behavior cross-sectionally via Google Forms. A total of 300 (31.5%) medical students out of 950 responded to the Google questionnaire. The mean age of medical students was 20.43 ± 1.87 years (range: 18–26 years). 168 (56%) were female, 132 (44%) were male participants, and participant rates were 35.59% for females and 27.61% for males. Participants’ academic year of study were 83 (27.7%) in 1st year, 96 (32%) in 2nd year, 46 (15.3%) in 3rd year, 36 (12%) in third final, and 39 (13%) in an internship. The majority of the medical students were Hindu [274 (91.33%)], single, not in a relationship [247 (82.30%)]; from urban India [226 (75.30%)]; residing in hostel [198 (66%)].
Sexual Knowledge and Sexual Attitude
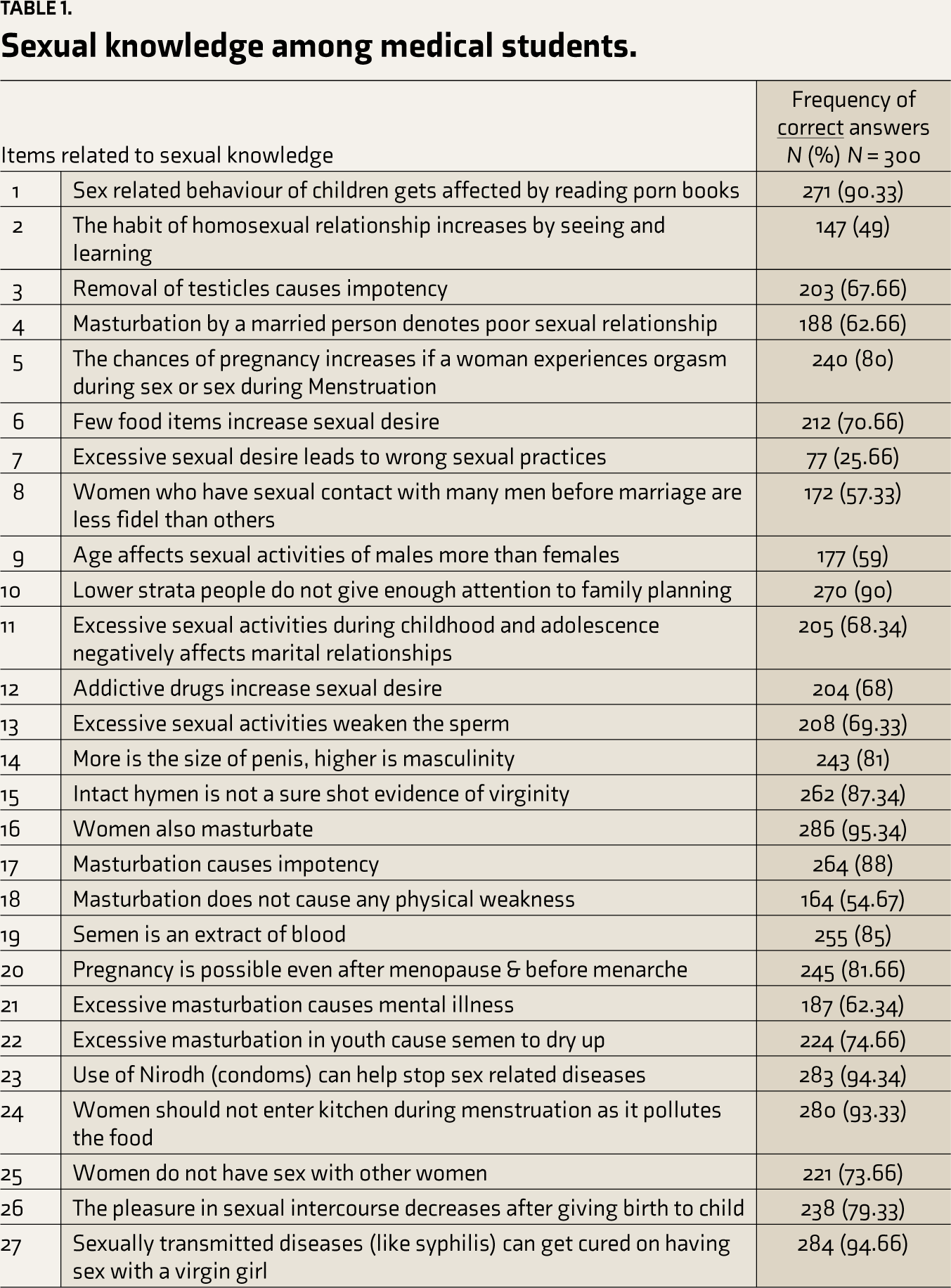
The mean score for sexual knowledge was 24.35 ± 4.93, which suggested that medical students had adequate sexual knowledge. The Current Study found that participants residing in urban areas have more sexual knowledge and liberal attitudes than rural ones. As per Table 1, in item analysis, a maximum number of students reported correct answers in areas related to sexually transmitted illnesses (94.5%), body anatomy/physiology (84.44%), and masturbation (61%). Around 49% believed that masturbation may lead to mental disturbances and excessive sexual desire, leading to wrong sexual practices (75%). 93.33% of participants did not believe in the isolation of females during menstruation.
Sexual knowledge among medical students.
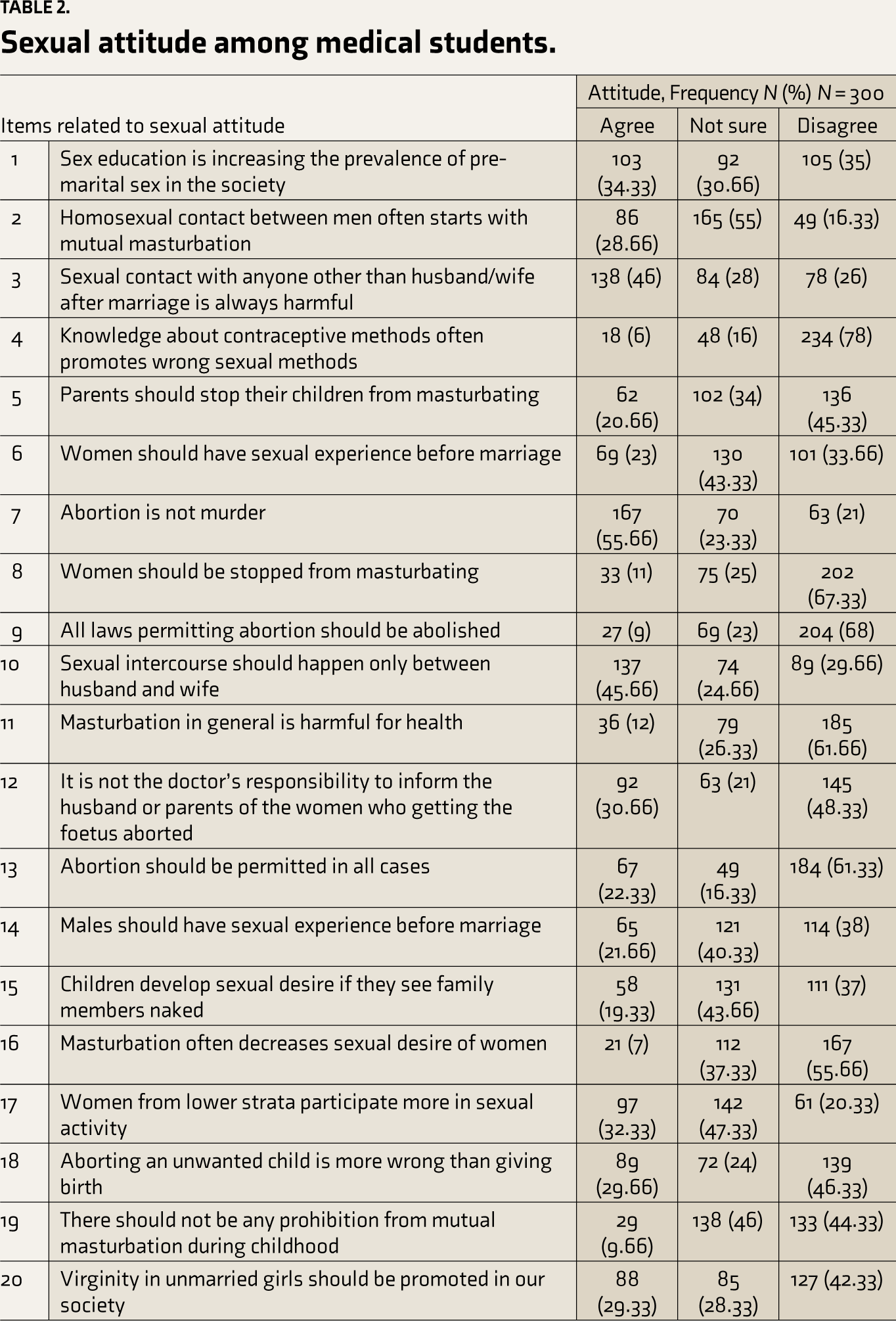
The mean score for sexual attitude was 23.79 ± 4.87, which suggested that participants had a liberal attitude toward sexuality. As per Table 2, the item analysis showed that 46% of them agreed that it is always bad to engage in extramarital sex; sex education was the reason for premarital sex (34%), and women should not indulge in premarital sex (33%). The overall attitude toward abortion was liberal; 55% of participants agreed that abortion is not murder, and 61% of participants believed that abortion should not be permitted in all cases. 42% disagreed that virginity should be encouraged in our society. They reported a liberal attitude toward masturbation also.
Sexual attitude among medical students.
Correlation Between Sexual Knowledge and Attitude
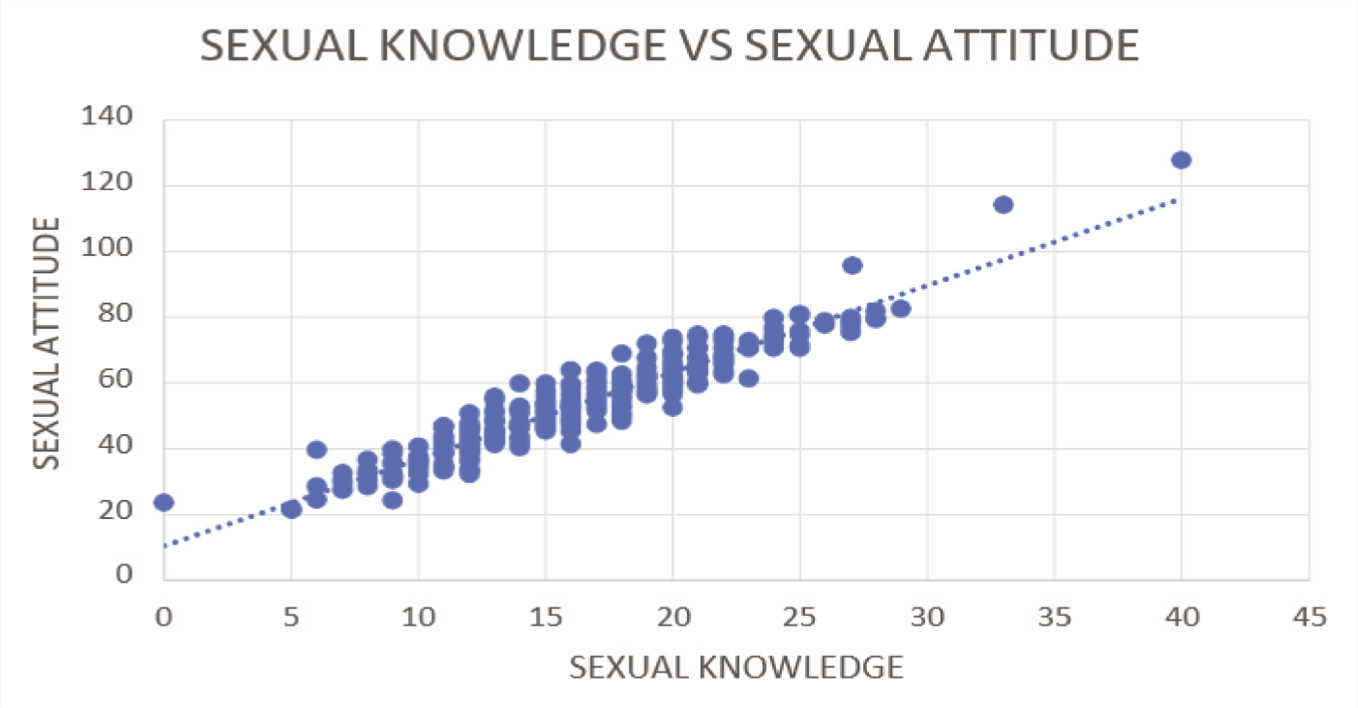
Figure 1 show that there was a significant strong positive correlation between sexual attitude and knowledge with a Pearson correlation of r = 0.95, P = 0.004. That means the higher the knowledge, the more positive and better the attitude.
Correlation between sexual knowledge and sexual attitude among medical students.
Relationship of Sociodemographic Variables on Sexual Knowledge and Attitude
We assessed relationship of sociodemographic variables with sexual knowledge and attitude. A one-way ANOVA was performed to evaluate relationship of sociodemographic variables likes gender, academic year, locality. The mean and standard deviation of sexual knowledge and attitude with each sociodemographic variables were shown in Table 3. There was a significant effect of gender on sexual knowledge, t = 3.61, P = 0.0003; There was a significant effect of gender on sexual attitude, t =1.8, P = 0.006. A one-way ANOVA was performed to evaluate the relationship between academic year and sexual knowledge. The ANOVA was significant at the 0.05 alpha level, F = 3.87, P = 0.0044. A post hoc Tukey HSD test indicated that the mean of the 2nd year was significantly higher than that of the 3rd-year Q = 3.97, P = 0.042. A one-way ANOVA was performed to evaluate the relationship between academic year and sexual attitude. The ANOVA was significant at the 0.05 alpha level, F = 2.48, P = 0.043. A post hoc Tukey HSD test indicated that the mean of the intern was significantly higher than that of the 3rd-year Q = 4.57, P = 0.011. A one-way ANOVA was performed to evaluate the relationship between residence and sexual knowledge. The ANOVA was significant at the 0.05 alpha level, F = 5.36, P = 0.005. A post hoc Tukey HSD test indicated that the mean of the rural residence was significantly higher than that of outside India residence Q = 5.22, P = 0.0007 A one-way ANOVA was performed to evaluate the relationship between residence and sexual attitude. The ANOVA was significant at the 0.05 alpha level, F =10.28, P = < 0.001. A post hoc Tukey HSD test indicated that the mean of the rural residents was significantly higher than that of outside India residents Q = 7.16, P = < 0.001 (Table 3).
Relation of sociodemographic variables with sexual knowledge and attitude score.
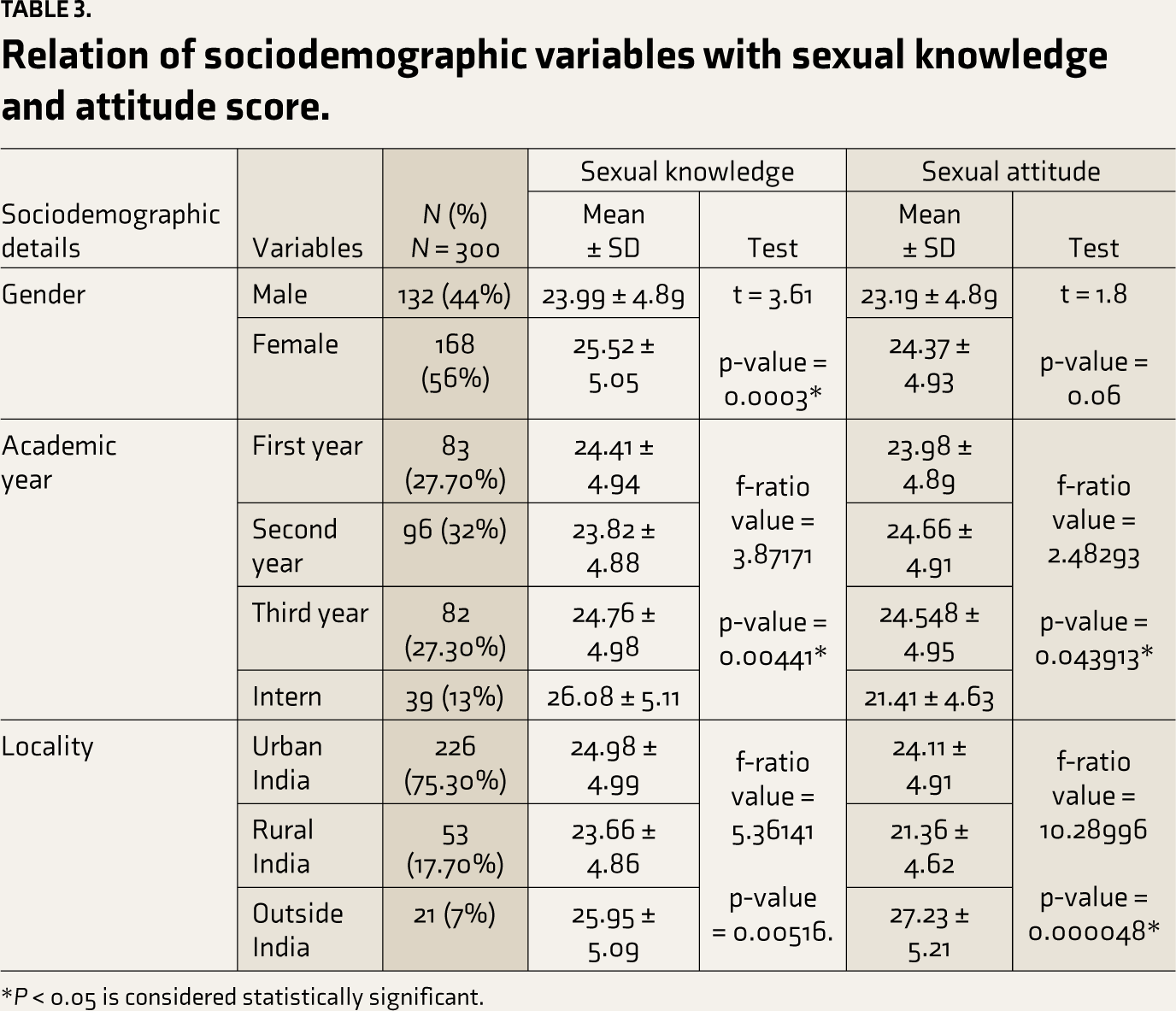
*P < 0.05 is considered statistically significant.
Sexual Behaviors
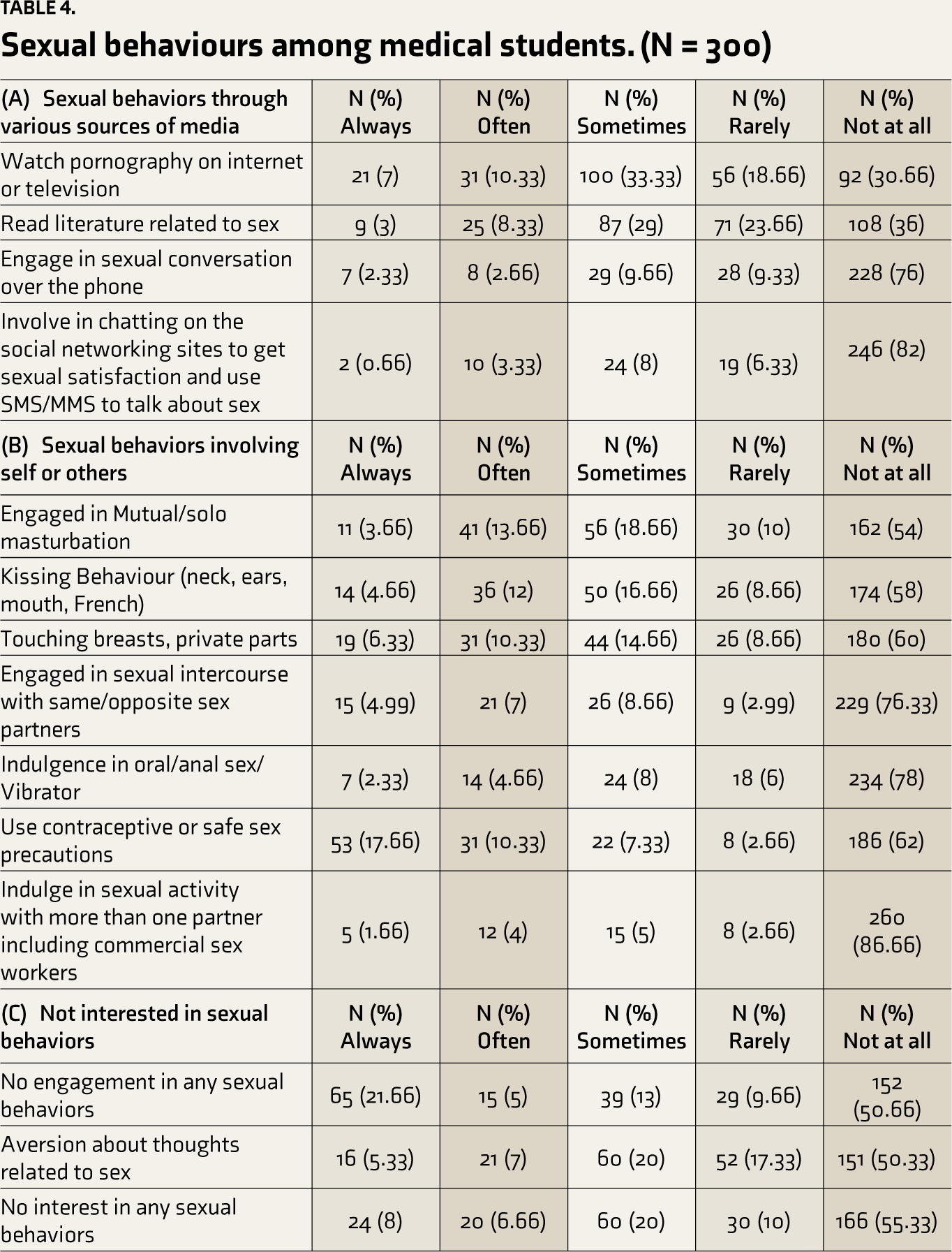
The mean score for sexual behaviors through media was 8.76 ± 3.70, suggesting a low level of indulgence in sexual behaviors using media. The mean score for sexual behaviors with self and others was 26.22 ± 13.85, suggesting a low level of indulgence. The mean age for involvement in sexual behaviors with self and others was 18.45 years. The mean score for not interested in sexual behaviors was 6.39 ± 3.43, indicating the level of aversion to sexuality (Table 4).
Sexual behaviours among medical students. (N = 300)
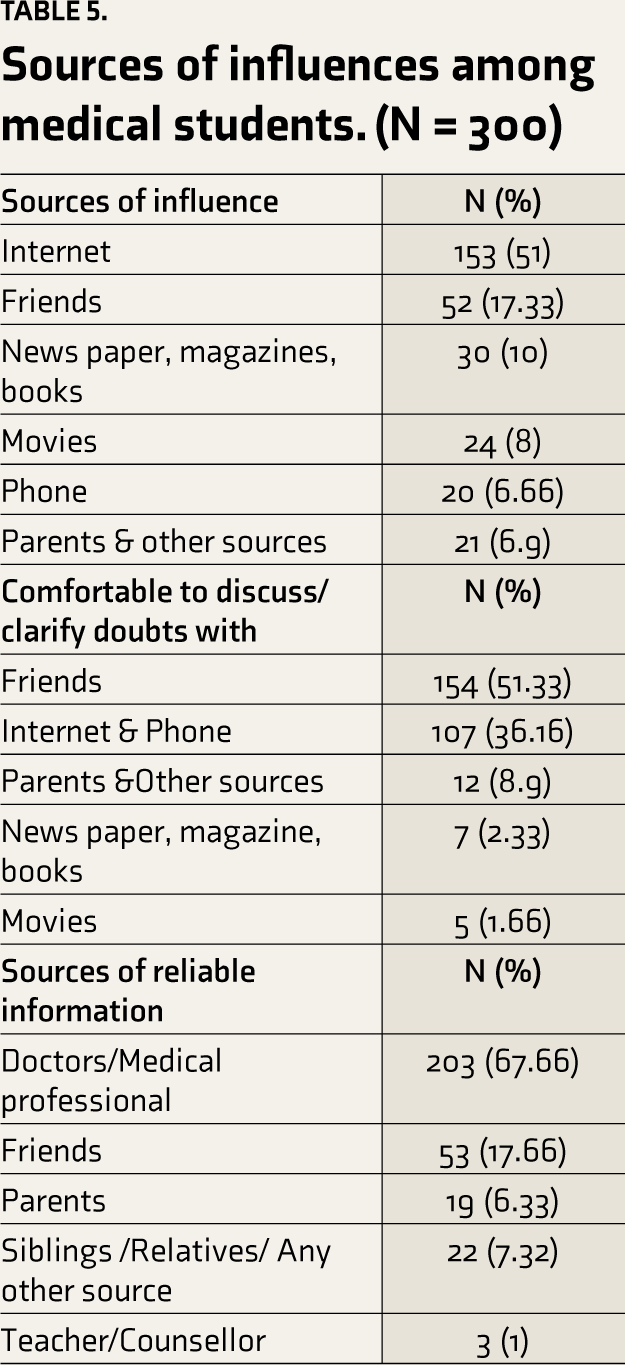
Sources of Influences
The young generation prefers to get information regarding sexuality from the internet, friends, newspapers, magazines, books, movies, and phones rather than from parents and other family members. Out of 300 medical students, 226 (75.33%) students were comfortable discussing or clarifying their doubts, most of them relied on friends and the internet, and the least preferred source was parents and another family member. They trusted doctors or medical professionals as the most reliable source of information, followed by friends, parents, and siblings, compared with other sources (Table 5).
Sources of influences among medical students. (N = 300)
Discussion
Our study aimed to map medical students’ sexual knowledge, attitude, behavior, and sources of influence on sexuality. We have very few responses despite a 1-month period of open Google links and repeated reminders. It shows that sex has been a forbidden topic for discussion even today. Similarly, very low participation was found in a very recent study of medical students. 8
In this study, female participants had more sexual knowledge and liberal attitudes regarding sex. The findings of Kumar et al. 15 had similar results; however, Sharma et al. 19 and Baumeister et al. 20 reported that males have better sexual knowledge and liberal attitudes towards sex than females. In a study by Kacha et al. 17 and Sidi et al., 21 no significant difference in overall knowledge between males and females was found. These results may be due to different study populations and education levels.
In this study, we observed that as participants’ academic year increases, their sex knowledge increases. These findings were consistent with Kumar et al., 15 Mahadik et al., 16 and Sidi et al. 21 These results may be explained as students acquire more knowledge.
The current study found that participants residing in urban areas have more sexual knowledge and a liberal attitude than those in rural areas. The study findings of Kumar et al. 15 and Mahadik et al. 16 support our result, but Sidi et al. 21 observed no difference in sex knowledge between rural and urban areas. The difference in results may reflect that the majority of our participants were from urban domiciles.
In this study, 60% of students believed that rapists have more sexual desire. Study findings of Kumar et al., 15 Kacha et al., 17 and Dutt et al., 9 reported that 69%, 80%, and 75%, respectively, found that rapists have more sexual desire. An increased incidence of rapes and excessive media coverage of the same may influence these results.
Our findings suggested that medical students had adequate sexual knowledge. In item analysis, a maximum number of students reported correct answers in areas related to sexually transmitted illnesses (94.5%) which was similar to the finding by Mahadik et al., 16 and five times better than the study by Kumar and Tiwari 5 and Kumar et al. 15 study found adequate knowledge regarding sexuality in female participants, body anatomy/physiology (84.44%), and masturbation (61%) which was similar to finding by Dutt et al., 9 93.33% of participants did not believe in the isolation of female during menstruation, knowledge about Sexually transmitted diseases was very good in all studies mentioned above. Regarding sexual desire, we had mixed findings. Nearly 70% of students believed that certain food items and addictive drugs increase sexual desire, which was true, but they wrongly believed that excessive desire means abnormal sexual practice (75%). Overall, knowledge was good; the reason for that may be this is a medical population whose source for sexuality is through authorized and scientific textbooks, whereas, in other populations, sources were unscientific, which leads to misguidance. Although in Gujarat, the study zone of Jamnagar (Kumar et al., 2020) 15 and Ahmedabad (Kacha et al., 2019), 17 knowledge about the same reported was poor. It is difficult to interpret these differences in findings exactly, but it showed rapid changes in knowledge within the span of 2–3 years. Variability in knowledge scores of various studies might be due to different methodologies, study designs, and different tools utilized to evaluate knowledge.
The majority of participants in the study had a liberal attitude towards contraception and abortion; these findings are similar to those of Kumar and Tiwari, 5 Dutt et al., 9 and Mahadik et al. 16 But reported conservative attitudes toward extramarital sexual contact and virginity. Study results are consistent with the findings of Kumar et al., 15 Kacha et al., 17 and Shah et al. 18 The majority of participants view pre/extramarital sex as sinful.
The majority of participants in the study who sought information on sexual topics did so through the Internet; this may be due to the convenience of online information access. This outcome was consistent with research by Jha et al., 8 Dutt et al., 9 Mahadik et al., 16 and M’imaita et al. 22 M’imaita found that pornographic images and text, clothing and fashion, sex styles, and contraceptive usage were among the information obtained by teenagers through the media. 22 The internet had provided a plentiful supply of pornography and sexual content that was challenging to control. 23
Many of the young people in the study learn things through friends. This may be the case because young people prefer to talk to their friends about sexual issues. After all, it’s considered taboo to discuss them freely with parents or other family members. 24 The fact that only a very small fraction of them obtain information from parents and other relatives further supports this. Dutt et al. 9 and Mahadik et al. 16 study findings also support these results.
In addition, half of the participants learned about sexual issues through movies. Even while movies were one of the essential sources of information, 25 also promote misunderstandings since the content they provide might be skewed with regard to attitudes about romance, typical teenage sexuality, sexual performance, and gender stereotypes. 26 Less than one-third of participants get information through books, magazines, and newspapers; the study findings of Dutt et al. 9 and Mahadik et al. 16 were like ours. The most popular sources of sex information, according to Joshi et al., 2 were books, periodicals, and peers. Due to the availability of electronic media in a variety of formats, access to the internet was preferred over print media for information.
Participants identified talking or clarifying with friends as the most comfortable option, followed by the Internet for clearing up sexuality-related questions or experiences. This may be due to the youth’s perception that their friends may have had their doubts or experiences because they were close in age and spent much time together, making it possible for them to feel comfortable talking about private matters. 24 Due to the stigma surrounding discussing sexual issues in our society, a very small number of them talked about these issues with their parents, teachers, and other family members.27,28 Similar findings were found in a study by Dutt et al. 9 and Mahadik et al. 16
According to participants, the most reliable source for sexual information was doctors or medical professionals, followed by friends, which was contradictory to the findings of Dutt et al. 9 and Mahadik et al., 16 who reported friends were more reliable.
Studies show that participants’ sexual indulgence was low. However, the percentages for various indulgences revealed that the majority of them used the internet, television, and reading material and engaged in sexual conversation over the phone to satisfy their sexual needs. A smaller percentage of participants admitted to using social networking sites for a conversation, making friends on sexual discussion forums, and sending SMS or MMS to themselves in order to experience sex; it clearly showed a trend toward increased use of electronic media for sexual fulfillment. The findings of Dutt et al. 9 and Mahadik et al. 16 were also similar. We felt there had been a need to control/modify the material in various media in order to promote positive attitudes, accurate knowledge, and healthy behaviors.
With respect to sexual behaviors with self or others, the average score falls under the category of a low level of indulgence. Analysis of each behavior shows that 5%–6% of them were involved in various sexual behaviors, including masturbation and sexual behaviors with same-sex and opposite-sex partners, which was contradictory to Dutt et al., 9 Mahadik et al., 16 and Smith et al., 29 findings, according to which 7%–16% youth involve in same. This may be due to various cultural beliefs and the average age of the participants being younger.
The study found that indulging in safe sexual activity was higher than unsafe sexual practices. Also, nonpenetrative sexual activity like kissing was more than penetrative sex, which matches the findings of Dutt et al. 9 and Mahadik et al. 16 Broadly, these results were positive as compared to Abraham et al. 30 So, over a period of time, safe sexual practices have increased.
Limitations
As this is a single college study, the generalizability of our results is limited. Although less likely due to the web-based survey, there is still a possibility of social desirability bias in the students’ responses. The majority of its participants had urban backgrounds, which restricted the study’s focus to young people from rural areas. We utilized an English-translated version of SKAQ II, 15 so we have not done any formal validation process for the tool.
Conclusion
Medical students had adequate sexual knowledge and a liberal attitude toward sexuality. Their major source for gathering information was the internet, and they were more likely to clarify doubts about sexuality through discussions with friends. They believed doctors or medical professionals were the most reliable sources of information. Having greater sexual knowledge was more likely to influence a liberal view of sexuality.
Supplemental Material
Supplementary material for this article is available online.
Footnotes
Acknowledgements
The authors would like to thank Dr. Saurabh shah, Assistant Professor, resident colleagues of department of psychiatry and student participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the use of Generative AI
AI tools are not used to collect or analyze data, produce images or graphs, or write this article, and we assume full responsibility for the entire content of the manuscript.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethics Committee Approval
This study received ethical approval from “Institutional Human Ethics Committee” - GMERS Medical College and Hospital, Gotri, Vadodara, Gujarat, India (Approval No: IHEC/23/OUT/SRPG076) on 21/06/2023.
Informed Consent
Informed consent had been taken from the participants for sharing the findings with scientific community.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.