
Abstract
Background:
Preterm birth trauma has become a growing concern in achieving the sustainable development goal targets for mental, maternal, and child health. Although obstetric and developmental complications associated with preterm birth have received a great deal of research attention over the years, subjective trauma experiences of mothers are often understudied. This qualitative study aims to fill this gap by adopting a phenomenological design to explore the traumatic experiences of mothers from pregnancy to care after childbirth of preterm babies in a low-resource economy.
Methods:
This was an Interpretative Phenomenological Analysis (IPA) of 22 mothers.
Results:
The results revealed three superordinate and six subordinate themes: pregnancy-related (Primary pregnancy-related complications and secondary pregnancy-related factors), healthcare-related (Trauma from invasive procedures performed on babies and trauma from the poor physical health status of the babies at NICU), and parenting-related trauma (Initial shock and denial and feelings of inadequateness and helplessness in caring for their babies).
Conclusions:
The study shows the complex nature of the birth trauma experienced by mothers of preterm babies. The study recommends client-centered, culturally sensitive, and trauma-focused mental health support within the maternal health system.
Birth trauma among preterm mothers involves complex emotional, cognitive, and behavioral responses to distressing and overwhelming events. Pregnancy-related trauma included pregnancy-related complications like bleeding and general life trauma like the loss of a family member during pregnancy. Healthcare-related trauma stemmed from invasive procedures on babies and the poor physical health status of babies in the NICU. Parenting-related trauma involved the initial shock and denial, along with feelings of inadequacy and helplessness in caring for their babies.Key Messages:
Motherhood is a critical, life-changing journey that spans pregnancy, delivery, and childcare, profoundly impacting women across various cultures and ages.1,2 This experience is particularly intense in developing countries like Ghana, where the psychological, physiological, and socioeconomic demands on mothers are substantial. 3 The transition to motherhood is marked by significant biological changes and diverse sociocultural roles influenced by age, culture, and societal expectations.4,5
For mothers with full-term pregnancies, the journey to childbirth is often smoother compared to those who experience preterm births. Women who give birth prematurely frequently face serious complications that lead to early delivery. 6 According to recent WHO statistics, 7 152 million babies were born before reaching 37 weeks gestation between 2010 and 2020. The global burden of preterm births is heavily skewed toward countries in Southern Asia and sub-Saharan Africa, which together account for 65% of these cases. 7
Preterm or premature babies, as defined by the WHO, 8 are born before 37 weeks of gestation. The complications leading to these early births stem from numerous risk factors. These include a history of preterm deliveries, multiple births, psychosocial stress, physical injuries, in vitro fertilization pregnancies, and maternal age extremes. Chronic diseases such as hypertension and diabetes, pregnancy-related complications, and preconception weight issues also contribute significantly.9,10 Despite the presence of these risk factors, most preterm births occur unexpectedly, leaving mothers unprepared for the challenges ahead. 11
The experience of preterm pregnancy and delivery is often described as traumatizing by mothers and families alike. 12 Preterm delivery complicates between 5% and 18% of pregnancies globally and is a leading cause of mortality and morbidity among pregnant women and their babies.7,13 The stress of preterm parenting is compounded by factors such as maternal and child health issues, inadequate social support, rigid social norms, parenting stress, and financial difficulties.14,15 Consequently, the trauma associated with preterm parenting is typically greater than that experienced by mothers of full-term babies. 16
Preterm motherhood often begins with a series of sudden and traumatic events, disrupting women’s preparedness for complications, birth, and parenting. 17 Many women who deliver preterm babies undergo emergency cesarean sections to ensure a safe birth due to severe pregnancy-related complications. Researchers 18 highlight that poor birth preparedness and complication readiness negatively affect maternal mental health, potentially straining the mother-child bond. Adu-Bonsaffoh et al. 19 found that mothers of preterm babies at the Korle-Bu Teaching Hospital in Ghana reported significant psychosocial distress. These findings underscore the argument that the traumatic experiences of pregnancy, delivery, and NICU hospitalization can lead to ongoing psychosocial challenges in mothers after discharge. 20
This study is essential in global health efforts to meet Sustainable Development Goal Three targets for mental, maternal, and child health. Our research delves into the challenges faced during pregnancy, birth preparedness, complication readiness, and delivery for mothers with preterm babies. By shedding light on these experiences, we aim to inform better support systems and care strategies for mothers navigating these complex and demanding circumstances.
Conceptualizing Traumatic Preterm Childbirth
The current study is grounded on the Middle Range Theory of Traumatic Childbirth developed by Cheryl Tatano Beck to explain the traumatic process and stressful birth outcomes. 21 In this theory, Beck 21 attempts to explain the complex phenomenon of traumatic childbirth by considering the enduring chronic implications on mothers, the child, the family, and healthcare providers at large. As part of the core concepts in the middle-range theory of traumatic childbirth, Beck 22 developed axioms for the theory. Core to these assumptions is the perception of traumatic childbirth as an extreme stressor that can lead to posttraumatic and secondary traumatic stress, with some chronic effects on the well-being of women. 21
Beck’s 21 theory further postulates that traumatic childbirth experiences could significantly affect women’s physical and mental well-being. The theory further posits that the traumatic childbirth experiences of women are mainly personal and unique to each woman. Therefore, each woman’s experience is expected to require a specific person-centered approach to address their traumatic childbirth crises and needs. Besides, it is vital to consider an individual’s duration and intensity of traumatic childbirth experiences. 21 Despite the duration and intensity of traumatic childbirth experiences, the theory stresses the importance of a woman’s perception of control and the availability of professional care and family support during childbearing as a barrier against the development of posttraumatic stress disorder (PTSD). 21
Beck 21 highlights the impacts of secondary traumatic stress beyond the woman. She further indicates that family and healthcare providers who witness traumatic childbirth could also be negatively affected by the negative impacts of the woman’s trauma. Therefore, affected healthcare professionals and family members, such as fathers of children, are also important in defining the extent of traumatic exposure and should be considered in the planning of recovery care. In addition to the secondary or vicarious nature of traumatic childbirth, the anniversary of the traumatic childbirth could trigger PTSD symptoms among mothers, family members, and clinicians present at the traumatic birth. 21 Based on this assumption, healthcare providers need to assess possible triggers and clinical manifestations of PTSD during follow-up care for management. 21
Considering the traumatic nature and PTSD consequences of preterm childbirth aligns very well with the concepts and axioms of the Middle Range Theory of Traumatic Childbirth.12,21 For example, maternal perception of traumatic childbirth among women with preterm deliveries in O’Donovan and Nixon’s 12 study affirms the subjectivity of perceived threat during and after birth. The literature has already established that the traumatic childbirth experiences of mothers with preterm deliveries are unique and complex compared to those with full-term gestation.12,13 Applying this theory in our study guided the conceptualization and explanations of the traumatic birth experiences of mothers who had given birth to preterm babies. We also conceptualized that the traumatic preterm birth experiences of women can be traced from their pregnancy, delivery, admission of their children to the NICU, and caring for them at home after discharge.
Methods
Study Design and Setting
This qualitative study adopted the phenomenological design to capture the lived experiences of mothers of preterm babies in Ghana. This design was suitable, observing that this is one of the first studies that explored mothers’ trauma experiences from pregnancy through delivery to care of their preterm babies after birth.
Sampling and Sample Size
We purposively sampled mothers seeking care at a regional hospital in Ghana. As part of our inclusion and exclusion criteria, we selected all mothers who had given birth to preterm babies not more than 2 years old. However, we excluded those who were clinically diagnosed with memory or other psychological disorders like postpartum depression. These criteria have been adopted over the years by similar qualitative studies that adopted the Interpretative Phenomenological Analysis (IPA).12,23 These authors12,23 justified that these women have sufficient experience to share their psychosocial distress and sociocultural challenges.
Participants
Twenty-two mothers between 23 and 42 years old who met the criteria for inclusion were selected for the study. Among the participants, 64% of them forming the majority were Akans. Also, Gas and Ewes represented 14% each, while Dagombas and Mamprusis recorded 4% each. Furthermore, children’s weights at birth ranged between 0.9 kg (900 g) and 2.1 kg (2100 g), while current weights at the time of data collection ranged between 3.82 kg (3820 g) and 11 kg (11,000 g). See Table 1 for a detailed description of participants’ demographic characteristics.
Participants’ Demographic Characteristics.

Interview Guide
We constructed a semi-structured interview guide based on existing instruments by O’Donovan and Nixon 12 and Sakyi et al. 23 Our guide included four sections: A, B, C, and D. Section A explored participants’ demographic data (e.g., Tell me about your baby’s weight at birth). Section B explored the lived psychological distress experiences of the participant during pregnancy, delivery, postpartum, and care of the child (e.g., Would you kindly tell me about your pregnancy experience?). Section C elicited participants’ experiences about sociocultural factors like social stigma, support systems, occupational demands, family interactions, and community reactions toward a preterm baby (e.g., Would you kindly tell me about your experience with the support systems you received while caring for your child?). Lastly, we sought information about the preterm motherhood representations of participants based on their unique cultural perspectives, resources, and coping methods in Section D (e.g., How would you describe your role as a mother of a baby who was born preterm?). Please see Appendix A.
Procedure
We obtained ethical approval from the Research Ethics Committees of the University and a regional hospital in Ghana. After sharing our study’s purpose, objectives, and methodology, we commenced our interview session following the hospital management’s approval. We also obtained written informed consent from our participants as they visited the hospital for routine reviews.
Interviews usually began face-to-face at the clinic or hospital. Since most participants traveled from other towns to the regional capital, Koforidua, where the hospital is located, we rescheduled the continuation of interviews via telephone at a time convenient to the participants at home. The interviews with participants lasted between 40 minutes and 1 hour.
Upon completion of the interviews, the data were transcribed verbatim. We also assigned pseudonyms to participants and deleted any potentially identifiable details from the transcripts. To maintain the quality of our qualitative research, we subscribed to the Consolidated Criteria for Reporting Qualitative Research checklist. 24
Data Analysis
The interview data were analyzed using Pietkiewicz and Smith’s 25 IPA framework to explore participants’ sense-making processes and the researcher’s interpretations. This approach involved multiple iterations of listening to recorded interviews and transcribing them until data saturation was achieved. To ensure confidentiality, all participant names mentioned in the interviews were replaced with pseudonyms during transcription. Preliminary summaries and observations were noted in the margins of each transcript, facilitating the identification of emergent codes. These codes were derived from the data through detailed analysis and were subsequently grouped into initial themes based on their thematic relationships. Repeated or irrelevant responses were removed through iterative data verification and member checking to refine the thematic structure. 25
Emergent codes encompassed primary pregnancy-related complications that were experienced due to participants’ gestation, such as high blood pressure, twin fetal death, pre-eclampsia, abnormal amniotic fluid levels, and proteinuria. Secondary pregnancy-related factors included traumatic events that were directly due to their pregnancy, like previous child loss, and emotional stressors, such as the loss of a spouse. Healthcare-related trauma emerged from codes within participants’ NICU experiences and interactions with healthcare professionals, such as discomfort with invasive procedures performed on infants and distress over the physical health status of babies. Parenting-related trauma themes included codes connected with mothering experiences, which included initial shock and denial upon seeing the premature baby’s appearance and size, as well as feelings of inadequacy and helplessness in caring for these fragile infants.
These emergent codes and themes were systematically organized into superordinate (major) and subordinate (sub) themes, reflecting the interconnected experiences of mothers with preterm babies. Table 2 in the Results section provides a detailed presentation of these major and sub-themes, ensuring transparency and replicability of the analytical procedure. 25 This rigorous analytical approach enabled a comprehensive exploration of the complex psychosocial experiences faced by mothers throughout the stages of preterm pregnancy, delivery, and early parenthood.
Results
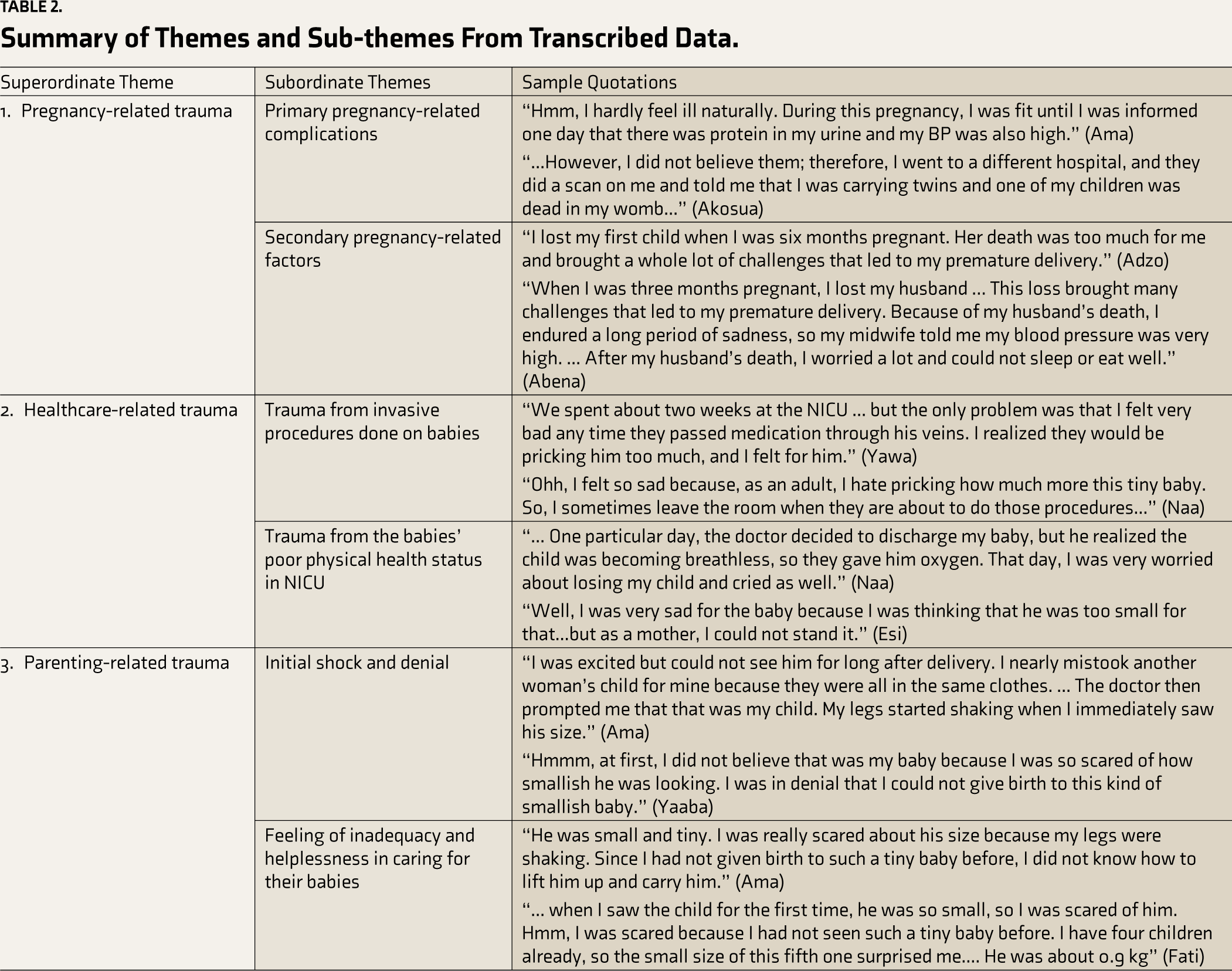
Birth trauma, like all forms of traumatic experiences, encompasses complex emotional, cognitive, and behavioral responses from distressing and overwhelming events.12,26 As a multifaceted psychological phenomenon, the traumatic experiences of preterm birth as the aim of the study can be traced through three superordinate and six subordinate themes: pregnancy-related (Primary pregnancy-related complications and Secondary pregnancy-related factors), healthcare-related (Trauma from invasive procedures done on babies and trauma from the babies’ poor physical health status at NICU), and parenting-related trauma (Initial shock and denial and feeling of inadequacy and helplessness in caring for their babies). Due to the subjectivity in trauma perception, it is important to view participants’ narratives as responses resulting from solitary incidents or protracted experiences from pregnancy to parenting preterm infants.12,27 A summary of the themes and corresponding extracts is presented in Table 2.
Summary of Themes and Sub-themes From Transcribed Data.
Discussion
Our study aimed to explore the traumatic experiences of mothers from pregnancy to care of preterm babies after childbirth. As found in the findings of the current study, the mothers expressed their preterm births as traumatic with unanticipated psychological demands. This finding aligns with the Middle Range Theory of Traumatic Childbirth across the different stages of preterm motherhood: pregnancy, delivery, and parenting. 21
In this present study, mothers of preterm babies experienced several pregnancy-related complications like high blood pressure, death of a twin fetus, pre-eclampsia, bleeding, abnormal levels of amniotic fluid, sugar in the urine, intrauterine fetal distress, infections, and placental abruption. These factors likely augmented the traumatic experiences of these mothers.13,28,29 Twin pregnancies, for example, inherently carry a higher risk of complications such as intrauterine fetal distress and placental abruption, leading to an increased sense of vulnerability and trauma. Also, pregnant women with pre-existing medical conditions, such as hypertension or diabetes, may face compounded risks during pregnancy, making them more anxious, which can exacerbate feelings of helplessness and trauma. Similarly, elderly primiparas, or first-time mothers of advanced maternal age, are more susceptible to complications like pre-eclampsia and gestational diabetes, further intensifying the psychological and physical stress they endure. These augmented factors underscore the need for tailored antenatal and postnatal care that addresses the specific risks and emotional needs of these high-risk groups, aiming to mitigate the traumatic impact of preterm births. As observed in studies by Gonçalves et al. 13 and Laelago et al., 28 pregnancies leading to preterm delivery are full of complications, which clinically risk the lives of pregnant women and their unborn babies. The complex physiological demands of preterm pregnancy lay a burden on the mental and social well-being of mothers, even in developed countries like the United States. 29
Similar to the developed countries, mothers who experienced preterm deliveries in fast-growing economies like China experienced complications like hypertension, abnormal levels of amniotic fluid, intrauterine fetal distress, placental abruption, and infections.30,31 These complications leading to preterm deliveries are comparable to the experiences of mothers who had given birth to preterm babies in East Africa, 28 Southern Africa32,33 and West Africa,34,35 where Ghana is part. 9 Additionally, the series of pregnancy-related complications among these mothers and, often, emergency surgery to ensure a safe birth can disrupt their mental, physical, and social health. 18 Evident in this current study, most participants reported that their trauma as mothers was heightened to the point where they had to undergo surgery without sufficient birth preparation and complication readiness. In alignment with the findings, Greek mothers who gave birth to preterm children through emergency surgery were observed to have an increased likelihood of experiencing PTSD than those with elective birth surgeries. 18
Globally, the traumatic and unanticipated events experienced among these mothers in this specific type of birth are even associated with the terminologies “preterm” (before reaching full-term pregnancy) or “premature” (before reaching maturation). 7 Overall, the sudden nature of birth prior to getting the full gestation period of 9 months (36–41 weeks of gestation) is always precipitated by a series of pregnancy-related complications that often risk the lives of both mothers and children. A study by Misund et al. 36 reported that 52% of mothers with preterm babies in Norway presented posttraumatic stress symptoms after delivery. The delivery of a preterm newborn in Ghana requires admission to the NICU as part of care protocols. The admission of newborn preterm is required due to prematurity physiological complications like apnea, respiratory distress, low blood pressure, difficulty feeding, jaundice, and hypothermia.37-39
Narratives of respondents in this study also indicated that another traumatic and unanticipated transition after preterm delivery is admission to the NICU. Most of these mothers were not able to accompany their babies during their admission due to their recovery state from surgery. It can be inferred from the results that respondents expressed that they were traumatized by their first entry into the NICU after experiencing separation and by seeing their babies’ sizes as smaller than they expected. This finding aligns with the results of maternal traumatic experiences at the NICU by Ncube et al. 40 in Botswana, Yu et al. 41 in China, Yismaw et al. 42 in Ethiopia, Sih et al., 43 in South Africa, and Afeadie et al. 38 in Ghana where the present study is situated. Corresponding findings were found in the study of Amadu et al. 44 in the Northern Region of Ghana. They reported that mothers whose babies were on admission to the NICU were traumatized due to their perceived fear of injuring their fragile babies as they held them and the fright from machines and instruments.
The NICU environment could be supportive and destructive to the mothers’ well-being. The NICU physical environment in most Ghanaian health facilities comprises beeping incubators, monitoring devices, tubes, suctioning devices, breathing support machines, and special gowns for mothers and healthcare staff.38,44 Although these materials and instruments are needed to conduct procedures or provide support to preterm babies who need critical care, they have been reported to pose diverse problems for mothers of preterm babies.38,44 In this present study, respondents were uncomfortable with the NICU environment and invasive procedures as they felt helpless as mothers and had to rely entirely on healthcare professionals. In essence, healthcare workers are at the center of the level of trauma experienced by mothers at the NICU, and their support could help alleviate maternal distress. This finding supports the results reported by Afeadie et al. 38 study in the Greater Accra Region of Ghana. In their research, for example, the nature of healthcare professionals’ interactions with mothers during hospitalization at the NICU was reported as fundamental to their well-being and bonding with their children. 38
Besides the trauma experienced by mothers due to the hospitalization of their preterm babies at the NICU, all participants in the study expressed some form of parenting trauma as they transitioned prematurely into motherhood. The premature entering into mothering of babies that are small in size and seemed fragile and the thoughts of being incapable of handling them as mothers worried all of them. This finding also aligned with the results from O’Donovan and Nixon 12 that mothers of preterm babies recognized their parenting roles as traumatic. Notwithstanding the several innovations in neonatology, the process of caring for preterm babies in literature consistently shows a consistent pattern of a highly challenging and traumatic experience. According to the findings of O’Donovan and Nixon, 12 this trauma experienced during parenting is complex because of how mothers perceive a close interconnectedness between their babies’ physical and emotional health and their well-being. As a confirmation of their findings among participants in Ireland 12 and Canada, 45 the Ghanaian mothers in this present study expressed that their initial trauma during parenting often revolved around the feeling of inadequacy and helplessness in caring for their babies.
Besides being subjective, the perception of parental inadequacy and helplessness in this current study was similar among first-time mothers and those with previous experience of motherhood. It became more apparent that all mothers experienced, perceived, and responded to the shock and challenges of caring for their preterm babies both at the hospital and at home. It was evident from the participants’ narratives that the sense of shock was mainly due to the denial that they could give birth to babies whose sizes were smaller than full-term babies. This shock seemed to be worsened by the initial separation and less involvement of mothers in the care of their babies at the NICU. From their accounts, they felt powerless and doubted their capacity to bear the needs of their perceived fragile babies successfully, as done by the healthcare professionals as they went home.
In contrast, mothers of preterm babies do not enjoy the opportunity of nursing and caring for their babies immediately after birth like mothers with term babies. They solely depend on the directions and advice of healthcare professionals at the NICU. Correspondingly, O’Donovan and Nixon 12 also described that parents of preterm babies in Irish NICUs saw medical staff as “gatekeepers” (p. 581) to parental access and contact with their infants. These negative perceptions among the current study’s participants bred worry, stress, sadness, fear, and other psychosomatic pain symptoms as they catered and watched their babies thrive. In line with these findings, Candelori et al. 46 reported that Italian mothers who had given birth to preterm babies experienced higher levels of anxiety symptoms than the fathers of the babies.
Limitations
Like all qualitative studies, the current study selects few participants, which limits the generalization of the study’s findings. Furthermore, our study failed to capture the voices of fathers and other members of the family, who are also affected by the birth of a preterm baby. Future studies should consider quantitative approaches to sample large populations. Also, fathers, siblings of preterm babies, and other extended family members like grandmothers must be considered in future research to explore their traumatic experiences.
Implications of the Study
Based on participants’ lived experiences, our study’s findings have several significant implications for policy, clinical practice, and future research.
Policy Implications
The findings call for policies to strengthen the existing antenatal care in Ghana regarding comprehensive birth preparedness and emergency readiness interventions. Furthermore, policies should mandate the establishment of robust mental health support systems for mothers of preterm babies, including psychological counseling and social support services. Also, policies should address the physical and psychological needs of mothers within NICUs to be more mother-friendly and ensure that mothers are provided with the necessary support to stay close to their babies during hospitalization.
Clinical Practice Implications
Regarding clinical practice, doctors and nurses/midwives who care for mothers will benefit from additional mental health training to support those with preterm babies with psychological first-aid during traumatic crises. In addition, there should be multidisciplinary care delivery where professional psychological services will be integrated into the routine care provided at the antenatal, NICU, child-wellness, and sick-baby clinics.
Research Implications
Based on the findings, future research should consider longitudinal studies to track the long-term psychological and social impacts of psychological trauma on mothers of preterm babies. Also, researchers should consider developing and testing interventions aimed at reducing trauma among mothers of preterm babies. This could include mental health interventions, educational programs, and support groups.
Conclusion
We used the phenomenological design to capture the lived experiences of mothers of preterm babies. Guided by the Middle Range Theory of Traumatic Childbirth, 21 our study found that mothers of preterm babies faced varied traumatic experiences across the different stages of preterm motherhood: pregnancy, delivery, and parenting. Participants’ narratives also indicated that all the women in the study never anticipated that their pregnancies were going to be challenging and, thus, were unprepared for the psychological demands that accompanied their crises and final preterm delivery. Also, they all felt that their inability to anticipate the challenges was mainly due to the poor birth preparedness and emergency readiness interventions offered to them during the antenatal visits. The medical advice for an emergency delivery intervention usually came after they were referred from their facilities, often at the primary level, to the regional hospital (secondary-level facility).
Furthermore, the mothers expressed that they were traumatized by the admission of their babies into the NICU as they worried about their babies’ survival, frightening procedures, machines, and instruments in the NICU environment. Besides, their stressors and distress continued after their babies were discharged as they felt inadequate to care for their babies as they had not taken complete charge of their care at the NICU. As an essential measure, policymakers, healthcare workers, extended families, traditional leaders, and other stakeholders ought to support and empower mothers to embrace their new role of parenting preterm babies.
Footnotes
Acknowledgements
We acknowledge the management and staff of Eastern Regional Hospital and mothers of preterm babies for consenting to participate in the study. We are also thankful for the support offered by the University of South Africa during the study period. This article forms part of the studies conducted in the first author’s doctoral thesis, supervised by the second author.
Data Availability
Transcripts used for analysis are available from the corresponding author upon request, following the requirements of the Research Ethics Committees of the University of South Africa and the Eastern Regional Hospital, Ghana.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
All procedures contributing to this project are per the ethical standards of the relevant national and institutional committees on human experimentation and the Helsinki Declaration of 1975, as revised in 2008. Ethical approval was mainly obtained from the Research Ethics Committee of the University of South Africa, with reference number 14084961_CREC_CHS_2022. The study also received relevant local ethics approvals and permissions from relevant institutions prior to data collection.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Appendix A. Interview Guide
Section A: Biographical Data:
Would you kindly tell me your age? What is your current marital status? What is your religion? What is your last level of education? What is your current occupation? What is your ethnic background? How many months/weeks were you pregnant before delivery? Tell me about your baby’s sex, age, and weight (at birth & present). Section B: Psychological Experiences Would you kindly tell me about your pregnancy experience? How were your feelings affected by the health problems/complications you experienced? How did you cope during pregnancy? How was the delivery process—how were you prepared for it? How did you cope during the delivery process? Tell me about your NICU and postpartum experiences—how did you feel after you first saw your child? How did you feel as you watched your preterm child go through painful procedures like pricking? How did the hospital staff treat you? Can you share how you felt as you cared for your child at home—What were your fears as you cared for your child? How did the kangaroo mother care procedure affect your emotions toward your child? How did you cope with the demands at home? Section C: Sociocultural Experiences Tell me about how your community members reacted because you gave birth to a preterm baby—Were you gossiped about? Were you called names by people? Was your baby laughed at? How did you feel about their behaviors toward you and your child? Would you kindly tell me about your experience with the support systems you received while caring for your child? In what ways did your partner assist you? How were you assisted by members of your extended family and community? What support did you receive from the medical support of hospital staff like doctors, nurses, psychologists? How sufficient was the maternity leave? Were you able to combine work with the care of your child? Section D: Representations of Preterm Motherhood Experiences Would you kindly share how you see your mothering of a preterm child based on your experiences so far – are the roles of a preterm mother in your community different from mothering a baby born after 9 months of pregnancy? How do you describe your role as a mother of your baby who was born preterm?