
Abstract
Background:
There is increasing evidence of the need for treatment engagement between Persons with Severe Mental Illnesses (PwSMIs) and Mental Health Professionals (MHPs). This therapeutic process involves collaborative work between patients and MHPs, which improves the condition. Community nurses are uniquely positioned to facilitate this process as they act as the focal point of interaction between patients and the health system.
Methods:
This qualitative study explored the community nurses’ experiences in treatment engagement with PwSMI through eight group interviews of 35 community nurses from District Mental Health Programs (DMHPs) across Karnataka (South India) from February 2020 to March 2020. The audio recordings of the interviews were transcribed and coded to arrive at themes and subthemes.
Results:
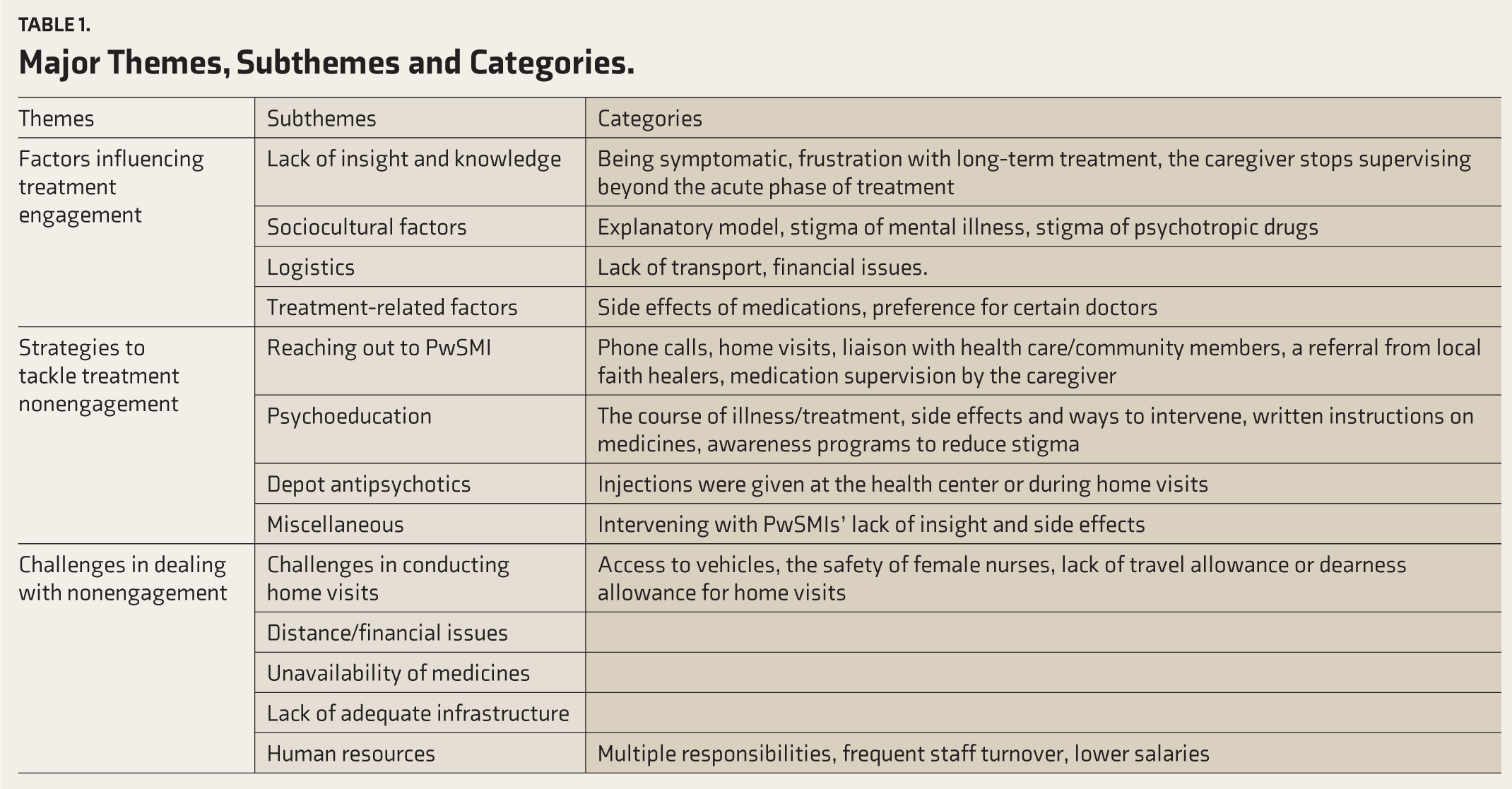
The major themes identified were factors influencing treatment engagement, strategies to tackle treatment nonengagement, and challenges in dealing with nonengagement. The reasons for nonengagement were lack of insight and lack of knowledge of sociocultural, logistic, and treatment-related factors. The DMHP teams contacted patients through phone calls, home visits, and liaisons with health workers and intervened with them through education and depot injections. The major challenges were difficulty conducting home visits, distances, the unavailability of medications, and the need for adequate infrastructure and human resources.
Conclusion:
Community nurses address a few factors of nonengagement, such as insight, sociocultural factors, and treatment-related factors. Addressing the systemic challenges and adequate training of nurses in intervening in the dropped-out PwSMIs would help to reduce the treatment gap.
Keywords
The major reasons for nonengagement were patient- and family-related, sociocultural, logistic, and systemic issues. Though the teams are working to improve engagement, there is a need to address systemic issues by adequately allocating funds, improving salaries, conducting periodic appraisals, and enabling more coordination and support to local NGOs. Streamlining the treatment engagement interventions and implementing cost-effective strategies must help to reduce the treatment gap.Key Message:
Perspectives of Community Nurses on Treatment Engagement of Persons with Severe Mental Illnesses (PwSMI): A Qualitative Study from South India
Severe mental illnesses (SMIs) are chronic, require lifelong treatment, and leave residual disability. In India, their current prevalence is 0.8%, and the treatment gap for them is 73.6%. 1 Recent South Indian studies reveal that 36.2% of psychiatric patients drop out of treatment after first contact and 34.1% within 12 months. 2 The dropout rates in rural and urban Karnataka were 17.3% and 43.8%, respectively. 3 Several patients drop out of treatment due to a lack of knowledge regarding illness/course of treatment, lack of insight, inadequate supervision by family, stigma, and lack of community acceptance.3,4 Treatment nonengagement can result in poor functioning and psychopathological outcomes and lead to relapse and rehospitalization.5,6
Promoting treatment engagement with the help of mental health professionals (MHPs) and ensuring medication adherence can help reduce the treatment gap. 7 Treatment engagement is a committed therapeutic process where persons with severe mental illnesses (PwSMIs) actively collaborate with the MHP to improve their condition. It means consistently attending the arranged sessions, adhering to specified treatment, and engaging with the MHP through phone calls, telemedicine sessions, or home visits.8,9,10,11
In India, the District Mental Health Program (DMHP) was set up to decentralize mental health services and provide them at the community level by incorporating them into primary health care. 12 The DMHPs’ multidisciplinary team includes a psychiatrist, psychologist, social worker, and two nurses. The community nurses, as a part of their role in the DMHP, are involved in the health care needs of persons with mental illnesses (PwMI) through psychiatric clinics in Primary Health Centers (PHCs) and Community Health Centers (CHCs), track follow-up of patients seeking treatment at CHCs and PHCs, train health personnel of CHCs and PHCs as per guidelines issued by National Mental Health Cell and through outreach activities such as school mental health, police training, and awareness programs on mental health. 13 Nurses are uniquely positioned to address treatment nonengagement as they can act as a liaison between the doctor, patients, and their family members. 14 Moreover, there are almost no studies on treatment engagement from India except for a paper on the SERWICE model at the National Institute of Mental Health and Neuro Sciences, Bengaluru (NIMHANS) for ensuring continued engagement with OPD patients attending rehabilitation services. 15 The lack of adequate literature on treatment engagement warrants exploration into the understanding/experiences of community nurses in this area.
Material and Methods
This study is part of a PhD research that aimed to develop, validate, and pilot test a tele-training module for community nurses on treatment engagement with PwSMI. The first phase aimed at understanding the perspectives of community nurses on treatment engagement among PwSMI through a qualitative study. The community nurses (from various DMHPs of Karnataka) who visited researchers’ parent hospital as part of in-service training were recruited to the study by purposive sampling.
Ethical Considerations
The researchers obtained the permission and approval of the Mission Director, National Health Mission, Bengaluru, and the Institutional Ethics Committee. Written informed consent was obtained from the community nurses after explaining the study, its objectives, and methods and clarifying their doubts.
Data Collection
The interview guide (see online-only appendix) explored the community nurses’ experiences with treatment engagement by PwSMI. It was prepared based on a literature review and validated by three experts in the field (two psychiatrists and a psychiatric nurse). Eight group interviews (each group consisting of 5–7 nurses) were conducted from February 2020 to March 2020. Group interviews were used as the researchers had to finish the data collection in 1 week (the nurses were staying at the researchers’ parent hospital for 1-week in-service training). Group interviews are time-saving, decrease interviewer bias, help in better standardization of interview situations, obtain a larger spectrum of subjects’ opinions, and can be a source of validation of the observed events. 16 The available nurses were divided into eight groups of five to seven for each day, based on their availability and willingness to come for an interview on a particular day. For each group, the researcher described the purpose of the study and clarified doubts about the concept of treatment engagement. Each nurse was encouraged to introduce themself. Ice breaking was done through a general discussion of work at each DMHP, followed by common reasons for treatment dropout and the strategies used by the community nurses to intervene in them. The interviewer asked each question and allowed time for each member to respond. They were requested to speak one at a time, be respectful, and maintain confidentiality of what was discussed. A total of 35 nurses participated in the interviews, of which 33 completed the interview. Data saturation was achieved by the end of the sixth group interview. It was conducted in the local language by Revathi Somanathan (hereafter RS) under the guidance of Deepak Jayarajan (hereafter, DJ).
RS underwent PhD coursework and had attended two hands-on qualitative workshops. The coauthors are experienced in qualitative research. Each interview lasted 60–90 minutes. Field notes were made after each interview. The interviews were audio recorded, transcribed, and translated into English. For each of the quotations, repetitions and stutters were removed and grammar was corrected.
Data Analysis
Qualitative analysis was done using ATLAS.ti 9.7.2 version. An inductive analysis was done; the interviews were read several times to understand the concepts. Using the software, RS coded the data; codes were discussed and finalized between RS and Thanapal Sivakumar (hereafter, TS) for three interviews and RS and DJ for one interview to reduce the risk of bias. The rest of the four interviews were coded by RS and categorized. Around 200 codes were formed, of which similar codes were merged, and insignificant ones were deleted. The final number of codes was 71. Categories were formed out of similar codes. The subthemes and themes were derived after comparisons within and between various categories. To ensure rigor, member checking and intercoder agreement were carried out. Member checking was done by sending the results to four community nurses who participated in the interview; the intercoder agreement was arrived at by sharing the transcripts with another expert and discussing the codes.
Results
The three major themes were factors influencing treatment engagement, strategies to tackle nonengagement in treatment, and challenges in dealing with nonengagement.
The age of the community nurses ranged from 27 to 52 years; the mean age was 34.5 years. The majority of the nurses were females (72%). There were twenty-one nurses with a qualification diploma in nursing (general nursing and midwifery), seven with BSc (N), four with PcBSc (N), two with MSc (N), and one with diploma in psychiatric nursing. The years of experience ranged from 2 to 24 years, with a mean experience of 8.2 years.
The major themes and subthemes derived from the content analysis are listed in Table 1.
Major Themes, Subthemes and Categories.
Factors Influencing Treatment Engagement
The subthemes under factors influencing treatment engagement were:
Lack of Insight and Knowledge
Lack of insight and being symptomatic were repeatedly mentioned as the most common cause for nonengagement in treatment. One of the nurses expressed,
… Due to lack of insight and being symptomatic, the PwSMI had stopped medication for the past six months …. So my colleague and I did a home visit and explained the illness and the importance of medication. However, she attributed the illness to physical symptoms and refused to continue medications ….
Another nurse said, “Mr G, a psychosis patient, refused oral medicines and depot injections as he was suspicious of the team’s intent for the home visit…”
Families consider stopping medicines when the patient is symptomatically better: “My patient’s caretakers stop supervising medication intake once the patient is symptomatically better …. Patient reduces the dose himself, leading to relapse and rehospitalization.”
Due to a lack of knowledge of mental illness and the need for long-term treatment, they may think medicines are ineffective if they do not find a rapid resolution of symptoms. The patients feel frustrated about taking treatment for many years.
Sociocultural Factors
A few patients/families believe in black magic/spirit possession and spend a substantial amount on folk remedies. A nurse said: “The family members thought that God possessed her…She was kept in a separate room … was taken to a temple…I had seen marks on her body that indicated that she was beaten up ….”
Another obstacle to adherence is the stigma surrounding mental illness and psychiatric drugs. The community nurses often face families who would not let them for a home visit. Sometimes, the patients may not come to the DMHP camp for fear that their acquaintances may notice them. Due to the stigma, patients stop the medicines while preparing for marriage, as stated by a nurse.
“Some people stop taking medications in preparation for marriage as they fear refusal of the proposal once the bride’s/groom’s family comes to know of the illness …. Neighbors advise marriage as a solution for mental illness.”
Stigma about psychiatric medicines is rampant in the community. The nurses reported that neighbors and relatives often discourage the patient from taking medication, believing that it may affect the kidney and the liver or that he or she may become addicted to the medicine. This, in turn, discourages the patient and family from regular medication and follow-up.
Lack of family support, difficulty in medication supervision when symptomatic, and family members not taking responsibility for the patient’s treatment subsequently cause nonadherence and relapse of symptoms.
Logistic Issues
Most nurses reported difficulty reaching patients from rural Karnataka’s interior areas, especially villages adjacent to forests. They also mentioned that people faced financial problems and could not afford travel costs to DMHP camps.
“… Many of the patients are from remote areas, where the buses are only at 8 a.m. and 4 p.m.… If they miss it, they will have to arrange a vehicle to come to the DMHP camp …”
Families with multiple mentally ill patients have difficulty managing themselves and consistently following instructions from the psychiatrist.
“…There is a very poor family with three psychosis patients and only one caregiver. All are ladies…So they find it difficult to come for follow-up and collect medicines…”
Treatment-Related Factors
Side effects of medication and perceived fear of side effects are the major hurdles to medication adherence. Commonly reported side effects were weight gain due to second-generation antipsychotics, drowsiness, irregular menstrual periods, and so on. The treating team was often unaware of the patients taking a reduced dose of medicine unless they approached the team due to the relapse of symptoms. Certain patients miss appointments if their preferred doctor is not available. One nurse said, “… If the patients are not happy with the medicines or advice given … they may drop out and start consulting private practitioners or district hospital psychiatrists …”
Multiple medicines confuse the caregivers, especially the illiterate ones, regarding when to administer them. A nurse said, “Mr. S’s mother is uneducated. She gets confused about what medication to be given and when…She is ready to supervise Mr. S’s medicine, but Mr. S is suspicious of her.”
Strategies to Tackle Treatment Nonengagement
Nurses were asked about the strategies the DMHP team usually followed to bring back the dropped-out patients or re-establish engagement. The following subthemes were identified:
Reaching Out to Patients and Family Caregivers
Some nurses reported that the team members attempted re-engagement of dropped-out patients through phone calls and by informing them of the next follow-up date. The patients’ details are maintained at the DMHP office. The PHC medical officers, Accredited Social Health Activists (ASHA) workers, and health workers are also involved in identifying new cases and dropout cases and engaging patients going through a relapse.
If, with these attempts, the patients did not come to camp, a nurse or social worker would conduct home visits to enquire about reasons for not taking treatment and to supply medications as advised by the DMHP psychiatrist.
“… Wherever needed, I took the tablets to the patient’s home and ensured that the patient swallowed them, as in the case of a psychosis patient who was poor and stayed with her grandparents.”
Some teams request local faith healers to refer cases of suspected mental illness. “The people of rural areas follow the rituals mentioned by this sister. So, we now try to include faith healers in the decision- making regarding treatment ….”
Another way of reaching out is by engaging the caregiver; obtaining help from the patients’ relatives, neighbors, and community members; monitoring the medication intake; assisting in traveling to and back from the camp, and convincing the patient to take medications. A nurse quoted an occasion where the medication of the patient, who stays at the bus stop, is supervised by the nearby shopkeeper. They also employ strategies such as pairing up patients from the same village to come for follow-up. “Having to travel long distances for consultation is also cited as a reason—so we advise them to pair up with another patient coming for follow-up from the same village.”
The nurses believe that the patients’ engagement in treatment will improve if self-efficacy can be encouraged by reinforcing them to go to regular work and actively participate in family matters. One nurse mentioned encouraging her patients to pursue jobs by informing them of relevant job vacancies. “…She had been telling me about her aspirations, and I had provided her with addresses and phone numbers to check for any possible vacancies. Finally, she got a job after many trials…She was not taking tablets regularly, but now she is regular with her medications and work…”
A few nurses share their phone numbers, so that patients can clarify doubts regarding medicines, which builds trust and improves engagement. Disability certification and initiation of pension are used as a reinforcement for regular involvement in treatment.
Health Education
The nurses educate the patients and family members regarding the nature, course, and duration of the illness, the medications prescribed, their side effects, and ways to intervene. A nurse said, “…We educate patients and caregivers about illness and medicines according to their level of understanding. When we give individual attention and care for their needs, I have seen that they comply with the suggested treatment.” For ease of understanding, the nurses compare the nature of mental illness and the pattern of medication intake with other noncommunicable diseases (such as diabetes and hypertension) and also give written instructions in Kannada regarding the intake of medicines.
The DMHP teams often reduce stigma by conducting awareness programs and through television advertisements, hoardings, and calendars with details of mental illnesses and observance of Mental Health Day, Drug Abuse Day, and so on. One nurse stated, “…We have a slum area where people do not come for consultations due to stigma…So, we do a community visit, provide awareness for the people there, identify the cases, and treat them…We use Information Education Communication (IEC) materials and take help of ASHA workers for the same …”
Depot Antipsychotics
In DMHPs, Inj. Fluphenazine Decanoate 25 mg/mL is supplied free of cost. These are provided to patients who are consistently disengaged from treatment at the clinic or during a home visit. As a nurse said, “… There are also people without family .… Mr. R stays at the bus stop … It is difficult to monitor his oral medication daily…We administer depot injections.” Shifting from depot injections to oral tablets once the patient becomes regular with medicines is widely practiced.
Miscellaneous
Other strategies employed by the team are:
Interventions for PwSMI Lacking Insight
The patients with lack of insight are engaged based on their understanding of the symptoms; a few who are in complete denial may require admission or depot injections. Patients who report physical symptoms such as insomnia or tiredness are encouraged to take medicines to improve them or the body’s general health. Caregivers mix the medication with food if the patient completely refuses it.
Interventions for Side Effects
For patients who want to stop the medication due to sedation, the nurses advise them to take the evening dose by around 7 p.m. For weight gain, patients are advised to exercise/go jogging/do brisk walks/do yoga; consume fiber-rich, low-calorie food; and monitor their weight regularly. Women on antipsychotics having irregular periods are worried about the same and tend to stop medications. The DMHP psychiatrist refers such cases to a gynecologist.
The nurses address the patient’s inability to attend the camp for reasons such as family functions, death, or celebrations by scheduling another day for the consultation or prescribing extra medicines.
Challenges in Dealing with Nonengagement
The major hurdles to applying the above strategies were:
Challenges in Conducting Home Visits
Access to Vehicles
Some nurses reported access to vehicles as an issue because the vehicle may be simultaneously required for various other programs the team is working on. In such situations, they take public transport for the visits. A nurse said, “…There are places with infrequent bus services…We are required to have our vehicle or hire an auto and make them wait for the return trip…”
A few nurses also expressed a need for travel and dearness allowances. However, many other nurses reported that teams plan home visits together and use the vehicle provided by the state for conveyance.
Safety of Female Nurses
There are also concerns about the safety of female nurses while conducting home visits to interior rural/isolated areas. A nurse mentioned, “One of the houses for the home visit was in an interior area; I initially called the caregiver, but he did not pick up the call…The area was very deserted. A person came in a two-wheeler and offered a lift; I was confused about his intentions and got terrified…”
Distance and Financial Issues
Those facing financial issues stop coming after the acute phase. “… Even if they get free medications, travel to the DMHP clinic is an issue…In areas where bus facility is not available, an auto costs Rs.100 ….They require money for transportation …. Finally, they drop out …”
Unavailability of Medicines
Due to the inadequate stock of psychotropic drugs or depot injections at PHC, the patients are sometimes advised to buy medicines from private pharmacies. Those who are not financially capable end up dropping out from/or becoming nonadherent to treatment. A nurse said, “… Medicines indented for the PHC earlier will expire next month. Medicines may not be regularly available; it takes at least six months to 1 year to procure the stocks—by then, patients would have dropped out of the treatment loop ….”
Lack of Adequate Infrastructure
The team sits together while intervening with the patients, and there is a lack of privacy/comfort and time to have one-on-one sessions with the patients. A nurse said, “When there are too many patients, we cannot concentrate on one person for a long time. It is difficult. Moreover, we don’t have separate rooms; we all sit around a common table and intervene with the patients ….”
Human Resources
The DMHP team utilizes the help of PHC medical officers and ASHA workers to reach out to patients who are irregular with follow-up. The ASHA workers are found to be reluctant to follow up on mental health cases owing to multiple responsibilities and lack of incentives.
Frequent staff turnover and staff leaving for maternity leave affect the smooth functioning and quality of engagement of the patient. Lower salaries than the clinical side lead to high turnover as these nurses search for greener pastures.
Discussion
This qualitative study gathered community nurses’ experiences and perspectives on treatment engagement of PwSMI.
Reasons and Strategies to Improve the Treatment Nonengagement
The most frequently reported reasons for nonengagement were financial factors (16 quotes), followed by the side effects of medications, lack of insight, symptoms interfering with treatment, and lack of knowledge. Financial factors have been found in previous studies too to be a common reason for dropout from treatment,3,17,18 which is curbed to some extent by government hospitals’ supply of free psychotropic drugs. 19 Facilitating free bus passes in liaison with the social workers and providing telepsychiatry consultations or home visits as and when the need arises can help prevent dropouts due to financial issues and long travel to DMHP camp.
Most nurses stated that the patients stopped medication when symptomatically better or assumed that medication is ineffective when the symptoms are not resolved; this may be due to a lack of knowledge on the course and duration of treatment. 20 The nurses and other team members routinely educate the patients regarding the long-term nature of the illness and the bio-psycho-social model, comparing it with diabetes/hypertension and clarifying doubts regarding psychotropic drugs. A tailor-made approach involving discussion on treatment and prognosis, reassessment, reflection/clarification of doubts, and education on possible side effects is essential. 21 PwMI sometimes seeks peer support to decide on the continuation of treatment. 22 Encouraging anecdotes from previously nonadherent PwSMI who are currently adherent would motivate better engagement in treatment.
Because of side effects or perceived fear of side effects, patients tend to consume an inadequate dose of medicine without the knowledge of MHPs. Executing adherence assessments (e.g., checking empty pill strips and informing the date for the next dose of depot injection) as part of routine nursing care is crucial.
Family-related issues such as lack of responsible caregivers, 3 families forcing patients to stop the medication due to cultural shame/stigma, and difficulty in marriage prospects were other reasons for nonengagement, as observed by the community nurses.23,24 Sometimes, the community members also have a stigma toward psychotropic medicines; they think the medicines can adversely affect the vital organs and are dangerous for the patient, and encourage them to stop medicines. Studies have effectively used psychoeducation to improve treatment adherence related to mental illness.3,25. Community nurses working at the grassroots, being more connected with local people, can address stigma-related issues through frequent awareness programs. 26 Yet, the reachability of these programs in interior rural areas is questionable. This, in a way, is countered by the use of social contact strategies by the DMHP team, such as engaging ASHA workers in case management of the PwSMI, leading to greater awareness of mental illness among the local people. 27
Belief in black magic and attributing mental illness to spirit possession is common in rural Karnataka; patients often visit faith healers before approaching the local mental health team. Local sociocultural practices violate the Mental Health Care Act 2017 28 ; the DMHP has set up steps to provide mental health care for people visiting faith healers to treat mental illness. The Dawa-dua (medicines-prayers) model (pioneered by Government of Gujarat) is practiced at Chikkaballapur district of Karnataka DMHP, where the team collaborates with local faith healers to bring back nonadherent patients to the treatment loop. The Dawa-dua model combines psychiatric medicine and faith healing. 29
In mental health, there are multiple treatment opportunities such as government hospitals, private practitioners, general physicians, NGOs, and faith healers. 30 There is a disproportion between the rural and urban populations in accessing these services due to their proximity and affordability issues. 31
In contrast to our view that medication adherence may be lower in rural areas due to issues with accessibility and shortage of mental health resources, some studies3,32 have shown that adherence is relatively higher (6% to 13%) there than in urban areas.
Lack of family support and the presence of multiple PwSMIs in a family make engaging in treatment difficult for an individual. Educating and involving a family member in medication supervision and patients’ treatment from the first session 33 has been found to be effective23,34,35,36 in resource-constrained settings. 37
The patients’ lack of insight makes it difficult to ensure medication adherence. A few nurses handled this by entrusting caregivers to supervise medications, while others preferred to intervene based on the patient’s level of insight. The authors opine that even if the PwSMI refuse treatment but is regular to follow-up, having positive regard toward the patient and priming them toward change would help them reconsider their decision on medication.
Depot injections and surreptitious medication ensured adherence in patients who lack insight, refuse treatment, or are symptomatic; however, Inj. Fluphenazine was the only depot injection supplied by the government. As per the principle of beneficence, there is an obligation to provide adequate treatment despite a lack of insight. 38 Nevertheless, it contrasts the rights of PwMI as per the Mental Health Care Act (MHCA) 2017. Hence, it is essential to initiate a Community Treatment Order (CTO) in India. 39 The DMHP psychiatrist refers highly uncooperative symptomatic patients to district hospital psychiatric units.
The routine method to address dropout from treatment used across the DMHPs in Karnataka is through phone calls and home visits. It was observed that around one-third of patients came for follow-up after a phone call from a team member. 3 During the field visits, RS observed that in many DMHPs, home visits are only done if they are essential, and there are practical issues around the nurses using their personal phones to call nonadherent PwSMI. This necessitates the provision of official mobile phones and informing the patient and family beforehand that they may be called within working hours, so that the nurses can freely give their official numbers to all patients to coordinate their follow-up.
Though the team carried out various engagement interventions, education, depot injections, and liaison with health professionals, 3 the inclusion of shared decision-making and motivational interviewing would help in equal participation and better engagement by the PwSMI.
Some studies have found that a lack of rapport/therapeutic alliance leads to treatment dropouts.23,24,35 Contrary to this, there was no report of a lack of rapport/therapeutic alliance in the current study. It may be due to the fact that people of rural areas place the doctor or MHP in a higher position than themselves and expect the therapist to advise the treatment. On the one hand, this concept helps PwSMI and the family follow the MHP’s advice with complete devotion, leading to better adherence. On the other hand, the PwSMIs may not be aware of the treatment options available and thus not participate in decisions about their own treatment. 40
The community nurses use available resources such as ASHA workers, relatives, neighbors, Anganwadi teachers, and local shopkeepers to secure treatment engagement with the patient. Engaging one’s patients by helping them find jobs and motivating them to work is noteworthy.
Challenges in Dealing with Nonengagement
During the interview, the nurses recollected several instances where, even after implementing engagement strategies at various levels, the PwSMI again relapsed due to medication nonadherence. This may be due to patient-related factors such as lack of insight, being symptomatic, the explanatory model of illness, 41 stigma, and attitude toward taking psychotropic drugs. Sometimes, the explanatory model of patients or caregivers affects their expectations from the MHPs, leading to dropping out of treatment. 17
The systemic challenges can be addressed by ensuring an adequate supply of medications, addressing the morale of team members, and linking them with grassroots workers.
Adequate allocation of funds for community mental health programs, improving team members’ salaries, conducting periodic appraisals, and enabling more coordination and support to local NGOs are recommended.
The challenges in conducting home visits, such as inaccessibility to vehicles, patients staying in interior rural areas, and the safety of female nurses traveling to isolated places, were also reported by Menon et al. 17 The team’s use of help from ASHA workers is sometimes compromised as they are involved in multiple programs, such as Tuberculosis (TB) and Maternal and Child Health (MCH). In these programs, they are incentivized for each case. Adding mental health programs to it has increased their work, leading to reluctance to follow up with psychiatric patients. We suggest incentivizing ASHA workers to identify new PwMIs and for continued engagement with mentally ill patients, as it has been proven successful. 42
Strengths and Limitations
This study gave insight into various strategies devised and used by mental health professionals of the DMHP team. Certain unique strategies identified were utilizing community resources, which can be modeled in other community mental health settings. The study’s qualitative nature helped us understand community nurses’ novel experiences in dealing with treatment engagement issues.
The significant limitation is the possibility of the nurses giving socially desirable answers as the interviews were conducted in groups and during a visit by these nurses for in-service training at the researchers’ parent hospital. Exploring the patients’ perceptions regarding reasons for nonengagement and triangulating the data with nurses’ perceptions would have helped to view the issue differently and reduce potential bias.
Conclusion
As per the community nurses, treatment disengagement by PwSMI was mostly due to a lack of insight and knowledge about illness and treatment, stigma, and attitude toward psychotropic drugs. Strategies such as home visits and educating PwSMI and caregivers on the importance of medication adherence are believed to have improved adherence to treatment. However, certain interventions are unique to specific DMHP teams. There is a need to streamline these interventions to be uniformly applied across all DMHPs. Developing a range of nursing interventions in the treatment engagement of PwSMI and training the community nurses may facilitate the dropped-out PwSMI returning to treatment.
Footnotes
Acknowledgements
We thank the community nurses for participating in the study and Dr Krutideepa Mohanty, Assistant Professor, College of Nursing, Berhampur, for supporting with analysis using ATLAS.ti.
Author Contributions
The authors confirm the contribution to the article as follows:
All authors reviewed the results and approved the final version of the manuscript.
Compliance with Ethical Standards
All authors certify that they were involved in the study, analysis, and preparation of the manuscript and have seen and approved the final manuscript. We meet the definition of an author, as stated by the International Committee of Medical Journal Editors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval
Approval was granted by the NIMHANS Institutional Ethics Committee (NIMH/Psy/DESC/RS/2019/02).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed consent
The author certifies that written informed consent has been obtained from the community nurses.