
Abstract
Background:
Looking at the alarming increase in the incidence of attempted suicide worldwide, having adequate expertise in managing people with attempted suicide is imperative. Therefore, healthcare professionals, specifically nurses, must be provided training exclusively on managing patients with attempted suicide and preventing suicide in the near and distant future. Nursing staff play a major role as a point of first contact for suicide survivors, and therefore, it is of utmost importance that they are adequately trained and knowledgeable in this area. To understand their knowledge, the authors decided to do this study to measure knowledge, attitude, and practice (KAP) among nurses in suicide survivors.
Aim:
The aim of this article was to study the KAP of nursing staff toward patients with suicide attempts.
Methods:
A hospital-based cross-sectional, quantitative study was conducted among nursing staff. All nurses (n = 300) were approached in small groups between July and November 2023 via a convenient sampling. Written informed consent from participants was taken. The semi-structured questionnaire included sociodemographic details, their professional experience, their training and experience in managing suicidal patients, and KAP questions. The KAP questions were on patients with suicide attempts and were derived from the suicide knowledge and skill questionnaire (SKSQ), suicide attitude questionnaire, and practice guidelines of the American Psychiatric Nurses Association. Data was analyzed by using MS Excel version 6.2.14.
Result:
In this study, a total of 200 nursing staff participated. The majority were female (80%), with a mean age of 37 years and a mean professional experience of 12 years. Out of all participants, 68% had experience managing patients with suicide attempts, but only 27% of them were trained in suicide prevention. The mean score of knowledge and attitude among study participants were 65.25/100 and 3.24/5, respectively. Nursing staff had higher scores in questions of suicide risk assessment and statements related to attitudes like “they deserve respect in society.” In practice assessment, more than 80 % of nurses were keenly observant, empathetic, and nonstigmatized for hospitalized patients of suicide attempts. The nurses took measures like restricting access to harmful objects (medicines, sharp objects) and giving medicines under supervision.
Conclusion:
The nursing staff had adequate knowledge, a nonstigmatized attitude, and appropriate clinical practices toward patients with suicide attempts, but they lacked formal training. So, hands-on training for suicide management at regular intervals is the need of the hour.
Regularly training for nursing staff on suicide prevention strategies will significantly contribute to suicide prevention.Key Message:
Suicide is a major public health issue around the world. The suicide rate worldwide is 9.0 per 100000 population, and a total of 800,000 people end their own lives yearly. 1
Indian figures show that 170000 people commit suicide yearly (2022). India witnessed a significant surge of 4.2% suicides in 2022, which is 4.2 % higher than in 2021. The overall rate of suicide in India was 12.4 % in 2022. The suicide rate in Gujarat state was 12.7% in 2022, which is 19.4% of total suicides in India. 2
The sex ratio of suicide among males and females was 71.8:28.2 as per National Crime Record Bureau data (India -2022). The most vulnerable age group for suicide was 30–45 years (34%), the leading cause of suicide was a family conflict (31%), and among all professions, daily wage earners were the most committing suicides (26.4%). 2
It is important to understand that these staggering figures of suicide undermine the actual number of people attempting or contemplating suicide; literature suggests that for every 31 Americans with suicidal ideation, only 1 commit suicide (National Institutes of Health). Additionally, a prior suicide attempt is a risk predictor for possible suicide attempts in the future, so identifying and addressing this risk factor are of utmost importance for an ideal suicide prevention program. 3
Broadly mentioning, the term suicide is defined as “Death caused by self-directed injurious behavior with intent to die as a result of the behavior.” 4
Nursing staff are the first contact in a hospital for suicide survivors, so initial encounters with patients are of utmost importance for managing suicidal behavior. Nursing staff can play an important role in preventing further suicide attempts through various measures like effective communication with patients and relatives, behaving empathetically, putting in place stringent rules and procedures to prevent added risk, and creating a safe environment for patients. Literature suggests that suicide survivors pose a significant challenge to the healthcare delivery system concerning management in various aspects. They also face a negative attitude toward hospital staff in medical settings. The more negative attitudes expressed toward repeated suicide attempters, the more the risk of subsequent attempts.5,6
However, the Indian Nursing Council (INC) curriculum includes “therapeutic communication skills with mentally ill patients” in general. The curriculum does not include “specific communication skills training with suicidal patients,” which contains empathetic communication and a nonjudgmental approach toward patients with suicide attempts. 7 Nursing staff is not formally trained in suicide risk assessment and is still expected to work in this area. A recent survey of nursing students found that nursing students had negative and stigmatizing attitudes toward people who attempted or committed suicide. 8 Another study from rural northern India reported an empathetic attitude in nurses toward persons who attempted suicide, but they were not skilled in handling patients with suicide attempts. 9
It has been observed that inadequate knowledge of the potential signs and risk factors of suicide negatively affects the ability of healthcare professionals to recognize patients at risk of suicide. It also impacts healthcare and patient safety. Additionally, the values and attitudes of nursing staff toward suicide may affect their willingness and ability to provide care.
Literature showed that it was mostly focused on the knowledge or attitude of healthcare workers toward suicide behavior, but the exact practices were not explored.9,10,11
This study was planned to focus on nurse’s knowledge, attitude, and practices related to patients they serve with a history of attempted suicide. This would allow the researchers to understand better the nurses’ knowledge as well as their feelings and practices toward patients with attempted suicide, which is one of the foremost areas in addressing suicide prevention. Also, as nurses get maximum opportunities to interact with attempted suicide patients firsthand, they can play a major role in recognizing and preventing further suicide behavior as they work near patients round the clock.
Materials and Methods
The study was conducted in an 850-bed tertiary care teaching hospital from July 2023 to November 2023.
All the nurses working in this tertiary care teaching hospital were invited, and consenting nurses were included in the study.
The sample size was calculated through the survey system program. 12 The required sample size was 169. The calculator was set at a confidence level of 95% and a margin of error was 5%. The researchers then finalized 200 as a sample size for this study.
It was a quantitative, cross-sectional study.
The study used a convenience sampling technique. All the nurses were approached consecutively as per their availability and duty timing, and all the consenting nurses were included till the final sample was achieved.
Study Questionnaire
The study instrument examined the nursing staff’s knowledge, attitudes, and practices toward suicidal patients. The semi-structured questionnaire consisted of three parts.
This part included sociodemographic data, including gender, age, marital status, qualification, experience, and workplace.
Part 2 consisted of a total of six questions. The first three questions were regarding their exposure to mental illness or suicide in near or distant family members. The last three questions were related to their training and education about suicide prevention and management and their experience in handling suicidal patients or close relatives.
This part included a knowledge, attitude, and practice (KAP) questionnaire, which was adapted from standardized data collection instruments like the suicide knowledge and skill questionnaire (SKSQ), 13 suicide attitude questionnaire, 14 and essential competencies for assessing and managing individuals at risk for suicide by American Psychiatric Nursing Association 15 and modified accordingly. It consisted of a total of 30 questions related to KAP (10 in each category). The questionnaire was developed after an appropriate literature review, and consensus was reached from experts in the field. Different researchers translated it into the local language, that is, Gujarati, and back-translated it to English. The back-translated English version was compared with the original, and the English tool was adapted for consistency. Before starting the study, the Gujarati questionnaire was also pilot-tested on 10 nurses to check for difficulty reading and understanding the questionnaire.
The knowledge questionnaire was based on “the suicide knowledge and skill Questionnaire (SKSQ).” 13 SKSQ includes two scales: the suicide knowledge subscale with nine true or false statements and the suicide skills subscale that estimates how confident participants were in their training, skills, and supervision while handling suicidal patients. Current studies have utilized the first part of the scale for knowledge assessment. Modification was done in item no. 1, 6, and 9. Item 1 was replaced with family history as one of the risk factors of suicide; item 6 was replaced with a common myth of suicide, that is, people who talk about suicide will never commit it; and item 9 was changed to a simplified version in place of borderline personality disorder changed to attention seeker. This study has added one item, no.10, related to the linking of social media usage and suicide. This modification was based on feedback responses from experts in the field. More than 50% of the right answer score is considered adequate knowledge. The correct and incorrect responses were calculated using MS Excel version.6.2.14.
The attitude questionnaire was based on a suicide attitude questionnaire by Huang et al. 16 . The Cronbach Alpha coefficient reported was 0.834, which means high reliability. The original scale consisted of 13 questions. We adapted 10 questions from the original version. Items 5, 11, and 13 were removed as neither matched the study objective nor repetition and practice-related statements. This was done after taking feedback from subject experts. The response was marked on a 5-point Likert scale from strongly agree to strongly disagree. A score of more than 50% on this questionnaire is considered a positive attitude, whereas a score of less than 50% is considered a negative attitude.
The practice questionnaire was developed on the basis of the literature of the American Psychiatric Nurses Association. 15 The questionnaire included essential competencies for assessing and managing risk for suicide. A total of 10 questions were marked on a scale of 1 to 4, where 1 means never and 4 means always. A cumulative mean for each question was calculated. Overall, more than 70% score in is considered the right practice.
Study Procedure
After obtaining permission from the institutional human ethics committee and nursing superintendent, participants were approached at their convenience and according to their duty timing. None of them were specialized in mental health nursing. A nonprobability convenient sampling technique was used. The participants were briefed about the study, and then written informed consent was obtained from them. Study participants were explained the procedure and informed that this study would maintain anonymity and confidentiality. Answers given by them would not influence their professional life in any way. This questionnaire was only for research purposes, so it required honest responses to minimize the study participants’ hesitancy while answering. Study participants were asked to fill out the questionnaire based on their experience of handling patients with suicidal attempts. While filling out the questionnaire, inter-participant discussion was not allowed. The questionnaire was collected when the participants completed it. Data was analyzed (calculated mean, standard deviation) using MS-Excel version 6.2.14
Results
This study measured KAP in nursing professionals working in tertiary care teaching hospitals about handling patients with suicide attempts. Of the 200 nurses that participated in the study, their sociodemographic data can be seen in Table 1.
Sociodemographic Characteristics and Years of Work Experience of Study Participants.
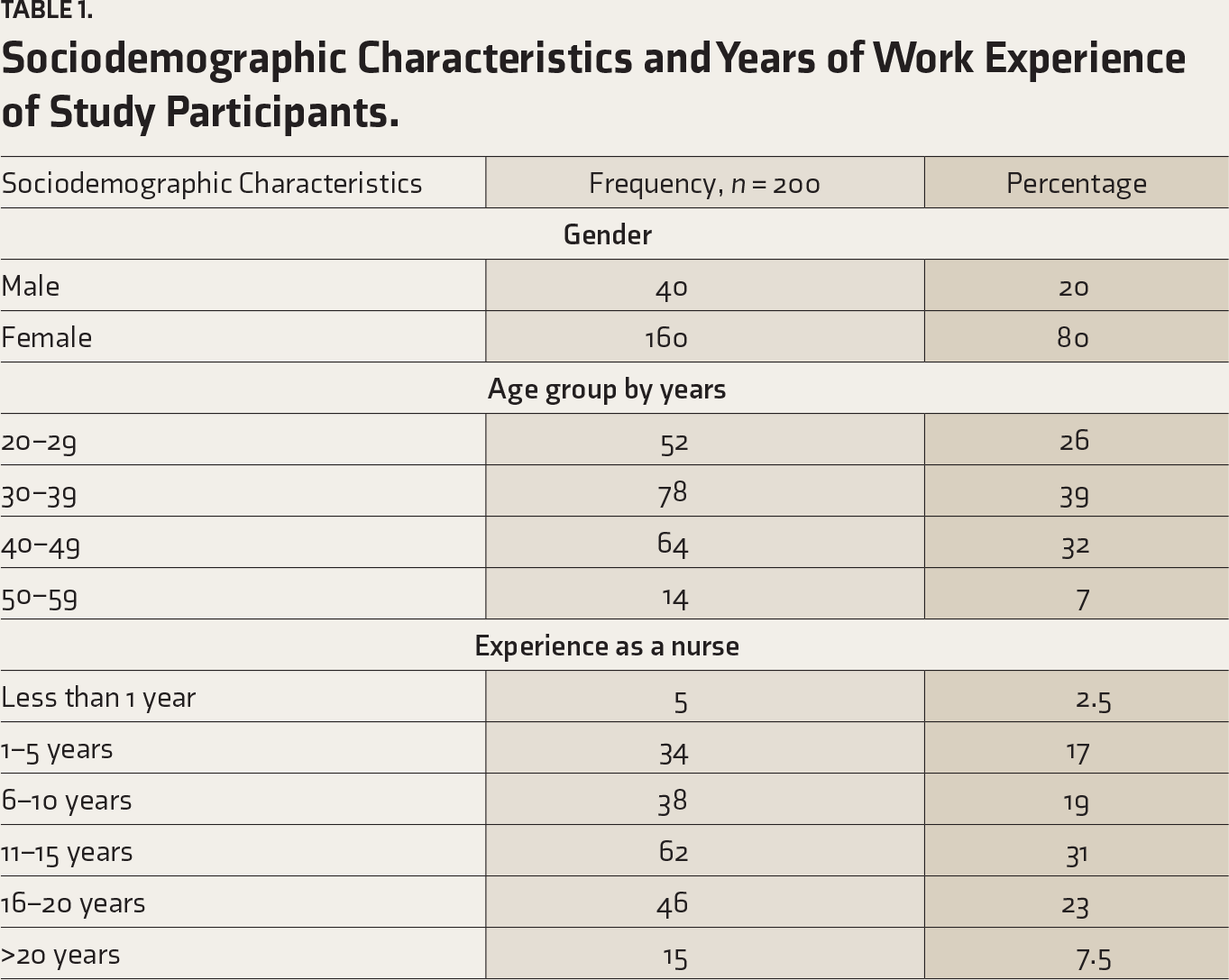
Table 1 illustrates the sociodemographic data of participants, of whom the majority were female participants (80%). The mean age of the study participants was 37 years, and the mean professional experience of the participants was 12 years as a nurse in various clinical departments.
Table 2 shows nurse’s exposure to suicide-related behavior and training aspects. Of their exposure to suicide behavior, 11.5% had a history of suicide committed in the family or close circle, and 7.5% had witnessed suicide attempts. During hospital duties, 68% of nurses have managed patients with suicidal attempts. Formal training on the management of suicide was taken by 27% of nursing staff.
Nurses’ Exposure to Handling Patients with Suicide Attempts and Training on Suicide Management.
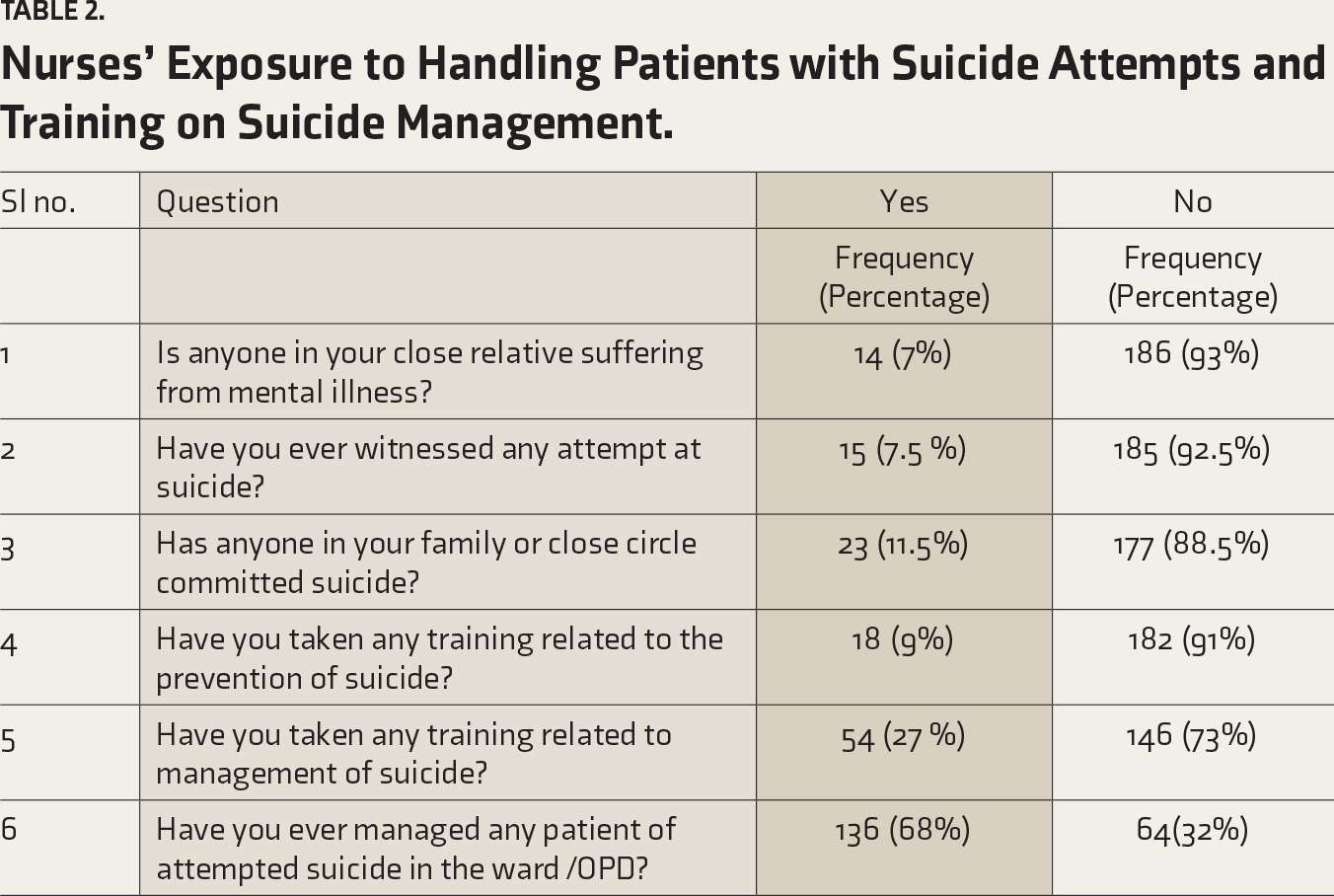
Table 3 represents the knowledge of nursing staff on patients who had attempted suicide. Questions were of True or False type. The majority of participants answered correctly for questions related to the role of family history (Q1), epidemiological aspects including vulnerable age group (Q.2), psychiatry illnesses (Q.3), and questions on suicide myths and misconceptions (Q.6,8,9,10). However, a significant number of nurses (64%) were not confident about asking about suicidal ideation in depressed patients as they feared that such questions might further motivate them to attempt suicide. Sixty-seven percent of nurses believed that suicide is unpredictable.
Knowledge Assessment of Nursing Staff on Suicide.
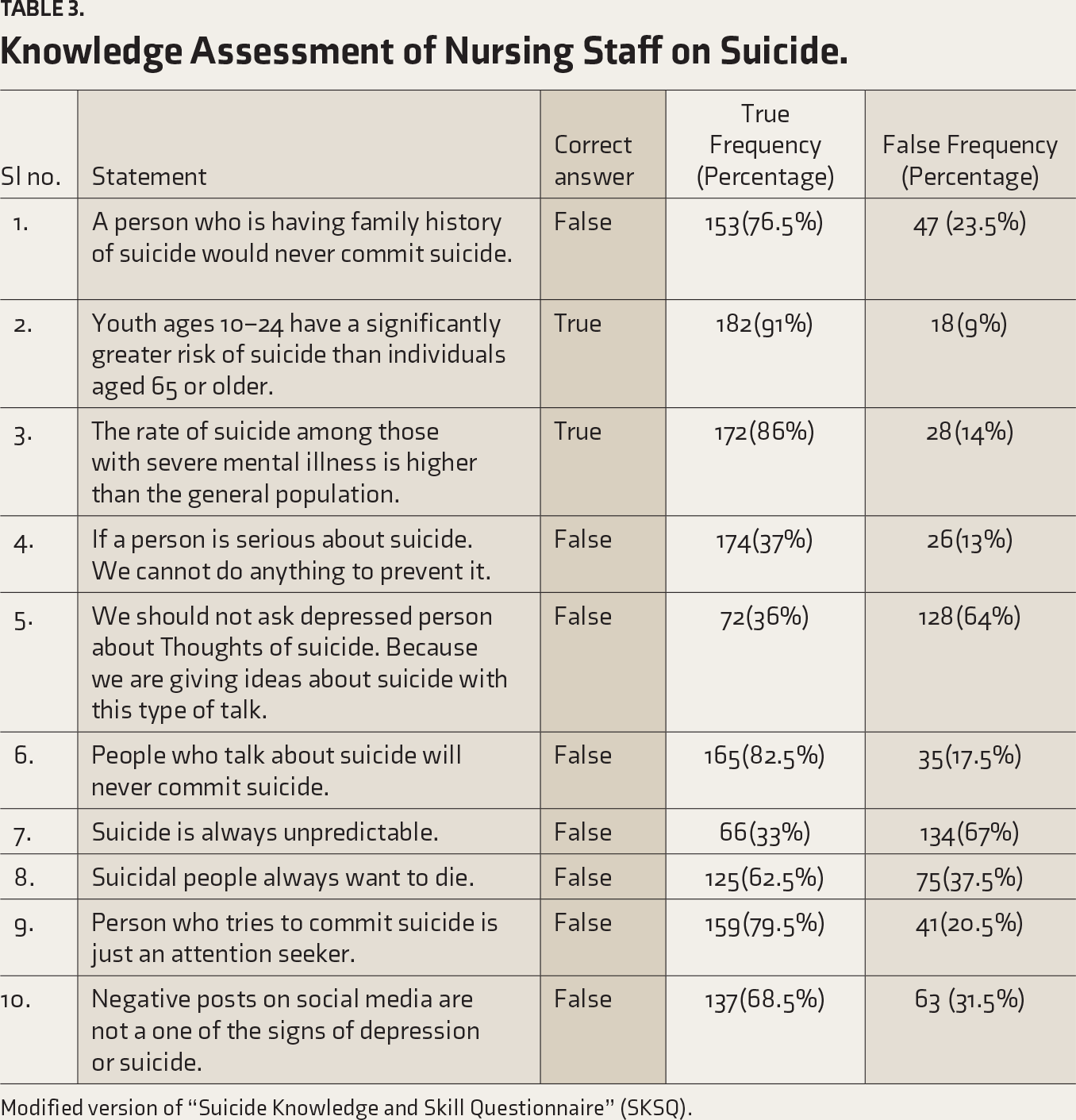
Modified version of “Suicide Knowledge and Skill Questionnaire” (SKSQ).
Table 4 depicts assessing nursing staff’s attitude toward suicidal patients, more than 50% of them believed that patients who attempted suicide were lonely and depressed. Many nurses (49.5%) believed that suicide survivors deserved respect from society. However, nearly 40% of participants yet believed people who attempted suicide had weak personalities.
Attitude Assessment of Nursing Staff Toward Suicide Behavior.
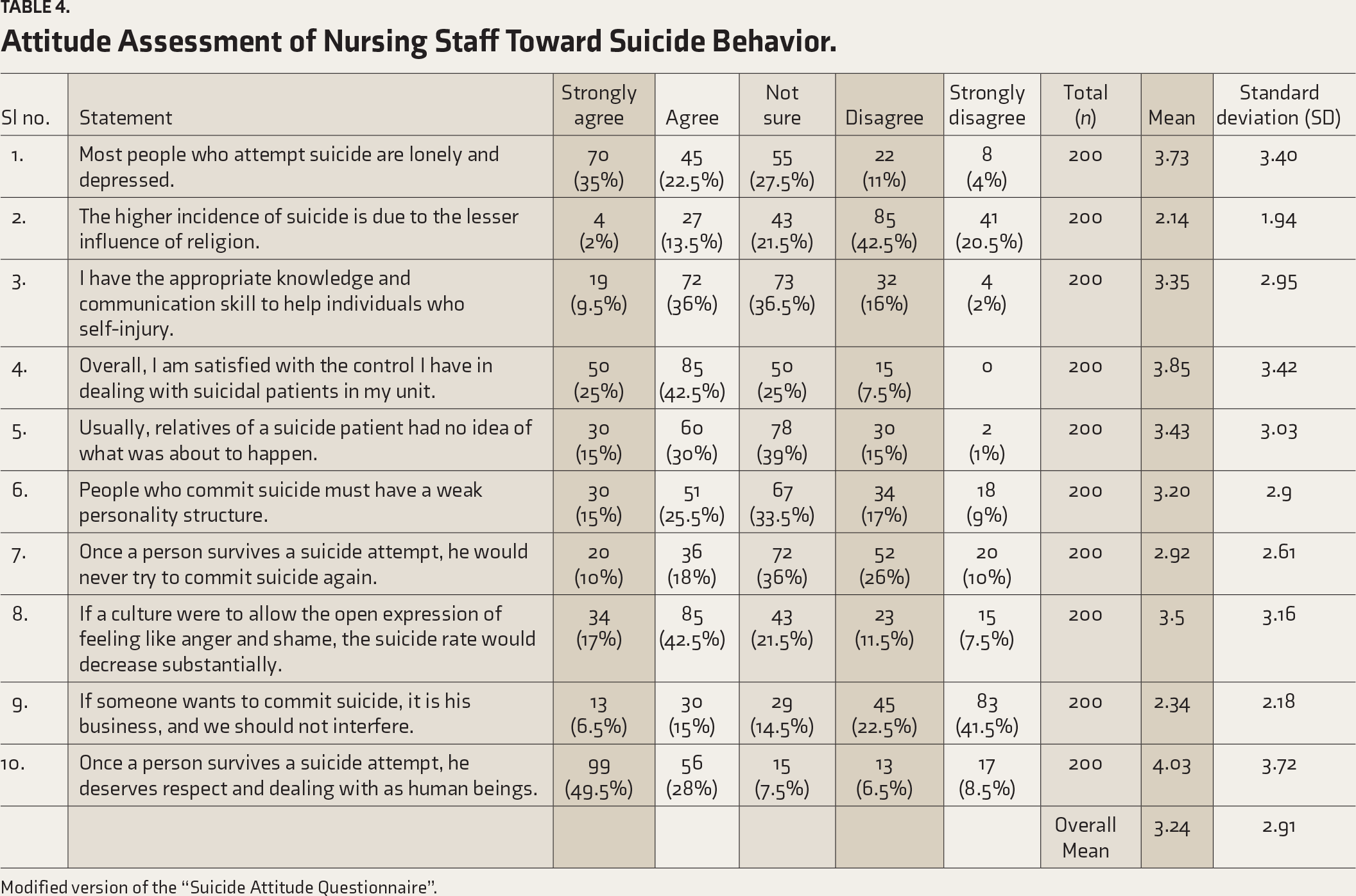
Modified version of the “Suicide Attitude Questionnaire”.
Table 5 depicts the current nursing practices while handling patients with suicide attempts. They have had the right practices like keeping one-to-one observation, being vigilant about the patient’s way of communication and behavior (Question 6,7) in the ward, and timely reporting. They instructed their colleagues for keen observation while giving over (Question 1), but at the same time, they had difficulty talking about the patient’s suicidal behavior (question 2). So, overall, they followed the right practices toward such patients, like educating relatives about the risk of suicide behavior but feeling hesitant while talking to patients about it.
Practice Assessment of Study Participants Toward Patients with Suicidal Behavior.
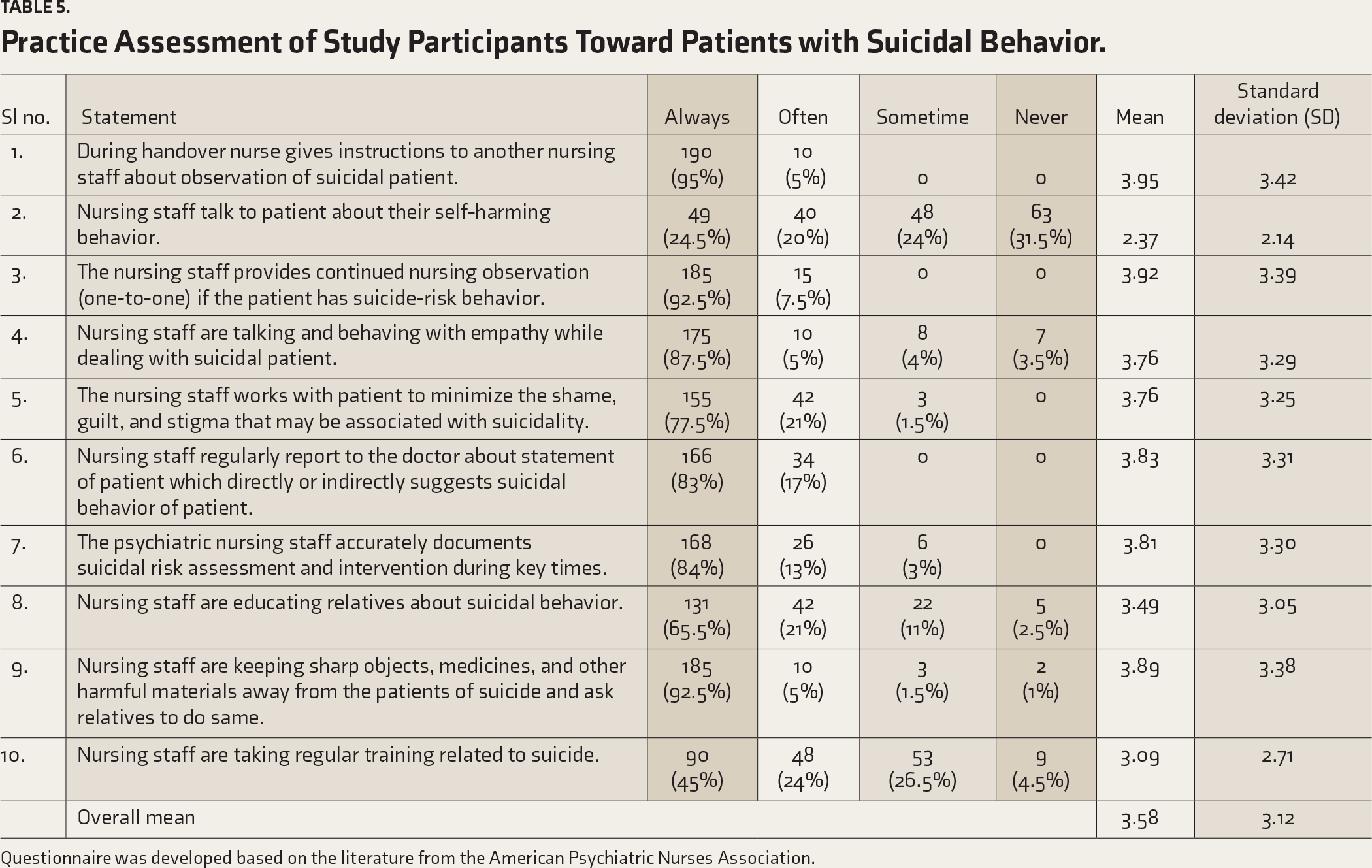
Questionnaire was developed based on the literature from the American Psychiatric Nurses Association.
Discussion
This study cross-sectionally examined the KAP of nursing professionals toward patients with suicide attempts. Most participants were female (80%) with more than ten years of professional experience (60%). Their overall knowledge and attitude score toward suicide patients was average (mean knowledge score was 65 % and mean attitude score was 3.24). In a study by Huang et al., 16 nursing staff had below average knowledge scores (50 %) but a mean attitude score of 3.40, which was better as compared to the present study. This might be due to a lack of updating their knowledge regarding suicide, but more work experience reflected a proper attitude toward patients with suicide attempts.
Knowledge
Nursing staff had good knowledge about managing suicide attempt patients (65.25%), and this was similar to the findings reported by Van Landschoot et al..20 (77%) and Huang et al. 16 (>50 %). However, a Study by Aljedaani et al. 17 (35%) and Rebair et al. 19 reported poor knowledge about suicide in nurses as compared to this study; this may be due to a lack of formal training for the nurses on managing suicide behavior. In our study, an area that reflected a lack of knowledge was that 33% believed that suicide was always unpredictable; this is similar to findings reported by Lodha et al. 8 One can say that varied knowledge scores in various studies can be due to different methodology, study design, and different tools used to evaluate knowledge.
Attitude
All nursing staff had an overall positive attitude toward suicide risk behavior in the present study, which was similar to the study by Nebhinani et al. (2013), 9 Aldalaykeh et al. 2021 21 and Aljedaani et al. 17 Few older studies in India had reported negative attitude.Results show a very restrictive attitude in Madras, rejecting the right to commit suicide, nearly always judging suicide as a cowardly act, and rejecting the idea of assisted suicide. On the other hand, in Vienna a more permissive attitude was found.22 Recent Indian studies reported positive attitudes 9,14,16,17,21 which might be due to increasing awareness and reducing stigma related to mental illnesses, while few international studies reported negative attitudes (Banfield et al. 2018, 23 Giacchero Vedana et al.). 18 This variation in attitude may be due to methodological differences in the tool, different scales for measuring attitude, and cultural variation. In the present study, only 38 % of nursing staff believed that suicide happened because of the lesser influence of religion, which is in contrast with Aldalaykeh et al. 21, which showed that 86% of Jordanian nursing staff believed that suicide happened because of lesser influence of religion. Mental Health Care Act (2017) 26 has decriminalized acts of suicide, but patients with suicide attempts have been reported and investigated by police. Such involvement of police and investigating procedures created a stigma among patients, relatives, and nursing staff.
Practice
Our study found appropriate nursing practices when attending to a patient with a suicide attempt, like providing one-to-one observation in such patients (92.5%). This finding was similar to the study by Aljedaani et al. 17 In this study, we found that while discussing with the patient about their suicide attempt, nursing staff were not very confident, and this finding is in contrast to the finding of a study by Bohan and Doyle et al..24
Our study found adequate knowledge, attitude, and practice among nursing staff in the majority of areas studied. The areas requiring to be addressed in nursing staff were stigma and misbelief regarding suicide. The reason for this may be that all the nursing staff had not taken formal training for suicide-related management. Previous studies showed that training improved their knowledge, attitude, and practice.6,25 Our findings indicate that imparting regular training to nurses would improve their knowledge, attitude, and practice in handling patients who have attempted suicide.
Limitations
As the research was conducted at a single institute and a convenient sampling technique was used, it limits the generalizability of the findings. The cross-sectional design may limit the ability to identify and explore cause–effect relationships. This study was prone to “recall bias” and “social desirability bias” by the nursing staff as it was a questionnaire-based study. So, multicentric, longitudinal, and intervention-based studies could be done. The effectiveness of “communication skill training with suicide patients” with the controlled group and assessing short-term as well as its long-term impact can be studied.
Conclusion
The nursing staff studied had adequate knowledge, appropriate attitudes, and practices when managing patients with attempted suicide. However, their stigmatized attitude toward certain items of suicide made them feel uncomfortable while interacting with such patients. Only a few nursing staff have taken formal training for the management related to suicide, so more training for nurses should be organized so that they can play a significant role in effective suicide prevention.
In the general nursing curriculum, a section should be added on how to handle patients coming to a hospital with attempted suicides. 7 In their curriculum, practical aspects like “communication skills training with suicidal patients” should be incorporated. Novel teaching methods like role plays and hands-on training should be incorporated while training them about suicide risk assessment and management.
Footnotes
Acknowledgements
The authors would like to thank medical superintendent and nursing superintendent of GMERS Medical College Gotri, resident colleagues of department of psychiatry, and student participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
Artificial intelligence (AI) tools were not used to collect or analyze data, produce images or graphs, or write this article. We assume full responsibility for the entire manuscript’s content.
Ethics Committee Approval
This study received ethical approval from “Institutional Human Ethics Committee” (approval no. IHEC/23/OUT/SRPG077) on 07/05/2023. Informed consent had been taken from the participants.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.