
Abstract
Background:
Suicide results from complex interactions of various risk factors—reasons for dying (RFD)—and protective factors—reasons for living (RFL). Suicide is not necessarily a wish to die but may be an appeal for help. We analyzed RFD and RFL in persons who had attempted suicide, through their clinical records at a Crisis Intervention Clinic (CIC).
Methods:
We retrospectively analyzed demographic and clinical data, and classified RFD and RFL, among patients with either ideas or attempt of suicide registered at our CIC (N = 83). Using two open-ended questions from the clinical history data, we derived their RFD or RFL; (n = 53) completed these questions regarding RFD-RFL.
Results:
In the total sample, males and females were equally represented and educated, but males were significantly older. Most common diagnosis was nonpsychotic mood disorder. Commonest mode of suicide attempt was hanging. Family conflict vs. family responsibility, hope vs. hopelessness, stressful life events, and negative cognitions about the self and the world were important RFD. RFL included feeling responsible, love for family and for self, hope, career success, and religious beliefs,
Conclusion:
RFD and RFL could both be grouped in similar categories related to family, career, hope, etc.
The most common modes of suicide attempts were hanging, jumping from heights, or lying on railway tracks, followed by prescription medication or drug overdose. Both reasons for dying and for living could be grouped in similar categories, family conflict vs. family responsibility and hope vs. hopelessness. Reasons for living included feeling responsible for and love for family, hope, career success, and religious beliefs.Key Messages:
Every year, close to 800,000 people take their own life and many more attempt it. Every suicide is a tragedy that affects families, communities, and entire countries and has long-lasting effects on the people left behind. 1 India reports a high suicide rate, with numbers increasing annually. 2 Indian rate of suicides was 10.4 during the year 2019. 2 These rates are probably lower than real rates because suicide was considered a crime in India till the new Mental Healthcare Act was passed in 2017. 3
It is, therefore, imperative to obtain better data on suicide mortality and suicide attempts. Both well-quantified data and rich qualitative data are required to formulate a plan and come up with policies. We need to study the motivational processes that lead to suicide attempts and why some individuals cross the line. 4 The internal suicide debate hypothesis can be used as an approach to gathering data. 5 This hypothesis assumes that suicidal individuals are often engaged in a struggle over whether to die or live and weigh up between reasons for dying (RFD) and reasons for living (RFL). 4
In India, “family problems” (32.4%) and “illness” (17.1%) were the most common causes of suicide, followed by “marriage related issues” (5.5%), “drug abuse/addiction” (5.6%), “love affairs” (4.5%), “bankruptcy or indebtedness” (4.2%), “failure in examination” and “unemployment” (2.0% each), “professional/career problem” (1.2%), and “property dispute” (1.1%). 2 This seems to indicate that those who harbor suicidal ideas or attempted suicide have clearly defined RFD, perpetuating their suicidal thinking and increasing the possibility of future attempts. Assessing both RFD and RFL (both ends of the suicidality continuum) is important to study suicide risk and intervene to prevent suicide. 6
Among a group of Indian women undergraduate students, RFL (total score) were negatively but significantly correlated to suicidal thoughts. Concern for future and moral objections were strongly and negatively related to suicidal thoughts. The authors opined that strong and positive RFL are useful in preventing suicide. 7 It is therefore important to investigate RFL as well as RFD among those who attempted suicide, since a past suicide attempt is a significant predictor for future attempts.8,9
The main objective of the present study was to understand why people attempt suicide and, after the failure of the attempt, what makes them decide to continue living. These factors may help design suicide prevention programs in the future.
Materials and Methods
Study Setting and Design
A Suicide Intervention Clinic was initiated at the Department of Psychiatry of our tertiary care teaching hospital in 2016. Considering the stigma associated with suicide, which prevents help-seeking, 10 and the possibility of medicolegal case registration (since suicide was a criminal offence under section 309 of the Indian Penal Code at the time), it was named the Crisis Intervention Clinic (CIC). The CIC registers all persons—pre-evaluated in our regular psychiatry outpatient department, referred directly from the emergency or nonpsychiatric services of the hospital, or self-selected. Registered patients are worked up in detail by postgraduate students, evaluated, and diagnosed by a psychiatrist, and then referred to the clinical psychologists and psychiatric social workers for testing or psychosocial support, as required. We retrospectively analyzed all available CIC records of persons reporting suicidal ideation or a history of a suicide attempt. There were no exclusion criteria, except the nonavailability of the complete demographic and suicide record. Sociodemographic details (age, sex, education, marital status, religion, occupation, type of family) and clinical information, including reasons and modes for current and past suicide attempts, psychiatric diagnosis, family history of psychiatric illness, and history of contact with a health professional, were tabulated and analyzed. In the detailed workup, there were two open-ended questions (answers to be recorded verbatim by the interviewer to the extent possible during the clinical workup) about their reasons for attempting suicide and their possible RFL. All complete records, including these verbatims, were examined and classified.
The Institutional Ethics Committee, ABVIMS, Dr RML Hospital permitted the study.
Data Analysis
For the analysis of sociodemographic data, percentages were calculated and frequency distribution was carried out. Relevant statistical tests, such as t-test for continuous data and chi-square for categorical data, were used to compare the groups. For clinical details, the percentage of the characteristics was calculated.
Classification of RFD and RFL noted in the records as answers to the two open-ended questions was carried out by two authors blind to each other. They extracted and classified the themes after analyzing these verbatims, blind to each other. Similar contents were classified in the same categories. Then both the authors discussed their themes together along with the senior author, and a consensus was reached on the final classification.
Results
Sociodemographic and Clinical Information
Data from available records for the period between January 2017 and December 2019 were analyzed. A total of 83 records with complete sociodemographic and clinical information was included. Out of this, data for RFD and RFL was available in 53 records (about 63%) only. Those whose RFD and RFL were not available (n = 30) were comparable in age, sex, education in years, religion, marital status, type of family, and occupational status with those whose data (n = 53) was available. Data from records with available RFD and RFL is presented below.
The males were older than females and similarly educated. The vast majority were Hindus (90.4%), and the majority (56.6%) lived in nuclear families. Only one-third (35.8%) were employed (Table 1).
Sociodemographic Profile of the Study Participants Who Reported Reasons for Dying and Reasons for Living in the Present Study (N=30)
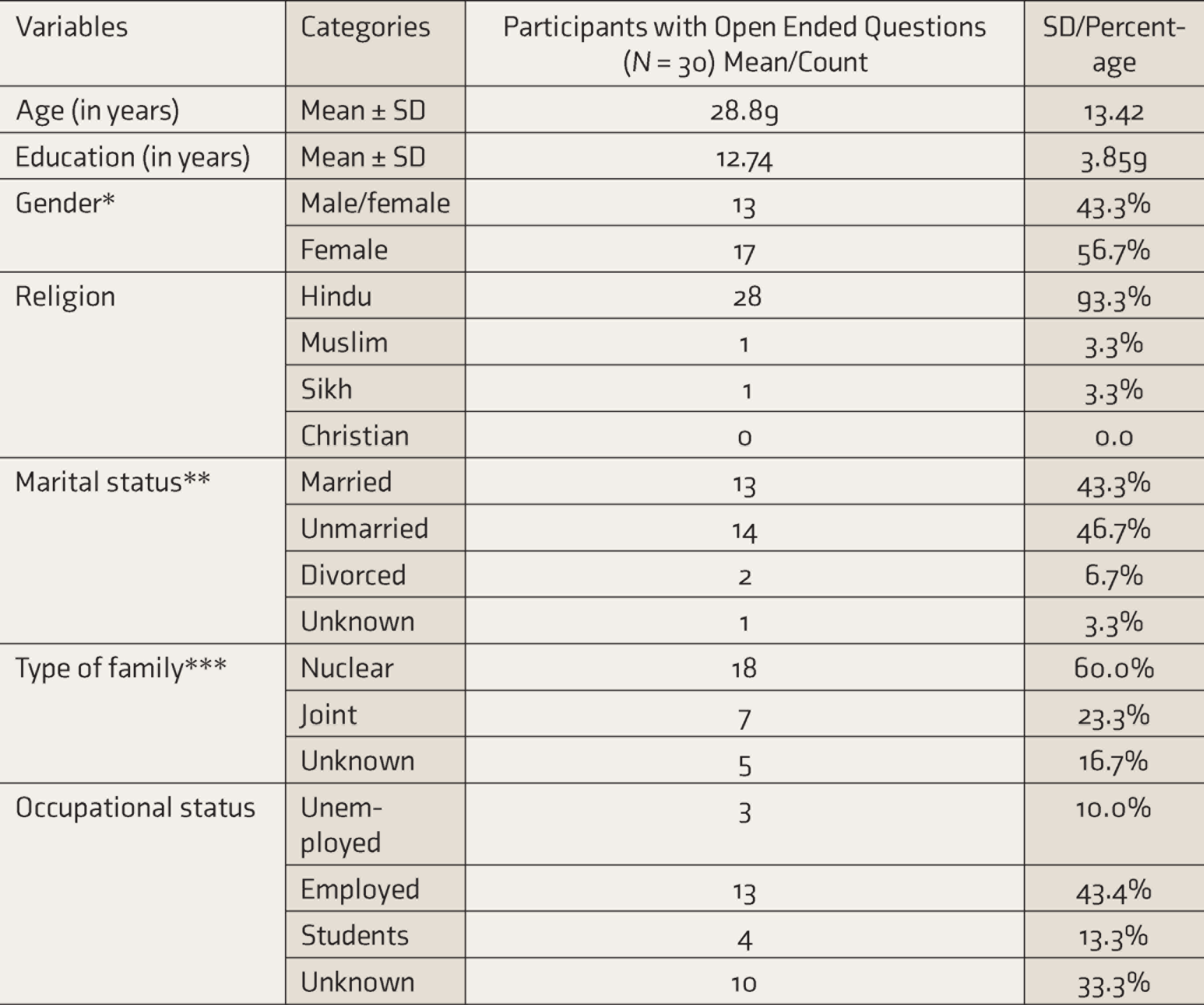
*No significant difference on gender participation. **Majority unmarried. ***Majority from nuclear families.
The majority were diagnosed clinically as nonpsychotic mood disorders 36%, (n = 19), 17% (n = 9) were either stress-related, adjustment disorder, anxiety disorders, or dissociative disorders, while 4% (n = 2) had a diagnosis of psychotic disorders (schizophrenia and psychosis NOS). Only 9% (n = 5) were diagnosed as suffering from personality disorders, while psychiatric diagnoses for 34% (n = 18) were not available.
Women in our sample reported suicidal ideation and suicidal attempt at an earlier age (26.65 ± 13.21) than men (33.85 ± 13.22). The difference between the two groups was found to be significant. Other details of the suicidality were that 39%, (n = 21) presented with a history of current suicide attempt, for 25% (n = 13) there was no suicide attempt recorded but suicidal ideation was detected, and data on suicidality was not available in 36% (n = 19) of the records. The modes of current suicide attempt (in the 39% (n = 21) who had such history) are as follows: hanging 29 % (n = 6), jumping off from heights or onto a railway track (n = 4), prescription medicine overdose (n = 4), consumption of poison (n = 3), wrist cutting (n = 3), and drug of abuse overdose (n = 1).
RFD and RFL
We classified data from 53 complete records for RFD and RFL (Table 2) as follows:
Reasons for Dying (RFD) and Reasons for Living (RFL) (N = 53) in the Present Study

Family conflict vs. family support: For 25% (n = 13), the RFD was family related. It included lack of support from the family, marital problems, familial disputes, and domestic violence. Yet, for 61% (n = 32) of patients, the major RFL was the family. For instance, this was noted: “There is no moral support from family, what will happen to me when I grow old? I am financially dependent on my son, the future is not secure. Nobody in the family needs me.”
RFL included their love for family members and the responsibility the attempter felt toward the family (the need to take care of the family, the fear of who will take care of the family if the patient died by suicide).
One record mentioned (male): “I have responsibility towards mother and the mother loves me a lot.” Another record mentioned “Parents will not live without me, whatever success I wish to get in my life I will not be able to achieve. I loved my younger brother a lot how will he live without me.”
Hopelessness vs. hope: For 24%, (n = 13) the RFD was all about negative cognition. It included reasons such as dissatisfaction with the self and the world, hopelessness, feeling angered very easily, sadness, and not being able to get along with people. One note said: “I have sadness. Life is a drama. There are frequent fights with husband and husband has substance abuse.”
For 15% (n = 8) of the patients, the RFL was hope for the future and also to live for themselves. One note expressed the reason as follows: “By living I can prove that I was not wrong. I have to stand in society and get back my house. I have to get back reputation in family & society and get married.”
Stressful career vs. successful career: Career-related issues were why 4% (n = 2) wanted to die, while 11% (n = 6) wanted to live because they felt they were good at their career and could sustain themselves because they were successful.
Stressful life events: For 22% (n = 12), this was the RFD. Major stressful events recorded were breakups, death of a loved one, detention in jail, (“I was not guilty yet they called me a criminal or drug addict. Nobody believed me even they who should believe in me”), and betrayal by friends (“I can’t take humiliation”). One record explained that the participant was tortured in jail. Another narrated that “Everyone teases me since the age of 14 years due to imprisonment. Everyone is selfish.”
Other reasons: Health-related issues, including both medical and psychiatric illness, and associated distress contributed as RFD to 18% (n = 10) of the cases. Some records mentioned: “I want to die because I am suffering from OCD, which is getting severe. With OCD, I can’t suffer further in life. Due to this problem, everyone is troubled by me. It feels I am a burden.”
Other RFD included financial difficulties (6%, n = 3) and impulsivity (1%, n = 1). One example of impulsivity, given by a girl, was that her mother beat her because she saw the girl with a boy at night.
Other RFL were religious beliefs (6%, n = 3), such as “the life given by God is precious, and we should not end it.” Another person said (“life is precious and one gets human life only after 84 lakh lives,” as per Hindu belief). The wish to travel and liking for entertainment was an RFL for 7% (n = 4).
While 34 records reported more than one RFL, 37 reported more than one RFD. Records that noted the same RFL and RFD were 7 out of the total sample of 53. The main reason to both live and die was family for all these seven cases. Family responsibility and love for the family were the RFL for them, and family conflicts and family fights were the RFD for all of them.
Discussion
In our sample, women attempted suicide at an earlier age than men. This is in accordance with age of suicide reported in India, younger ages in women (median age 25 years) than in men (median age 34 years) in India. 11 A larger proportion of adult suicide deaths occur between the ages of 15 and 29 years, 1 especially among women. 12
RFD and RFL
In our study, the major reason for dying was the family. It included reasons such as felt lack of support from the family, domestic violence and familial disputes, marital problems, and interpersonal difficulties. The Indian national database also reports “family problems” as a major reason for suicide. 2 Even among men in Norway, the main trigger for the suicidal act were problems in intimate relationships and family issues. 13
Other reasons to die were negative cognitions such as hopelessness, sadness, lack of meaning in life, dissatisfaction from the current state of life, low self-esteem, and stressful events. These included events such as detention in jail, death of a loved one, betrayal, a feeling of being trapped in a suffering present, with no better future possible.
Some people may choose suicide as a way out of feeling hopeless or trapped, such as an escape from an overwhelming life situation beyond their ability to manage. 17 Psychosocial stressors such as interpersonal, financial, and occupational stressors, clashes with the law, and pending court litigations were causes of suicide in North India. 15
Stressful life events also can trigger self-harm or help-seeking behavior. While they may not predict suicide, stressful life events can gradually become the reasons to die. 16 Health problems become RFD for some people when illness seems incurable. People who attempt suicide weigh their options.
Studies on suicide indicate the importance of RFLs as protective factors against suicidal ideations and attempts. Conversely, persistent RFD may increase suicidal thinking and suicidal attempts. 4 An important RFL in our sample was “family,” including love felt for the family, moral responsibility towards the family, need to meet family responsibilities, and fear of the chaos the family may undergo as well as the future concerns related to the family if she/he committed suicide. Responsibility to family and child-related concerns had the highest mean (protective) scores in suicidal thinking. 17 In another study, those who had not attempted suicide had more child-related future concerns than those who had. 18
After family, the next reason to live was hope: being hopeful that things would change in the future, a will to live for the self as things were expected to change. Being career-oriented and developing a successful career, “a factor to be relied upon” was another reason to live. The next few reasons were love for travel and entertainment, and religious beliefs. The findings of our study are in line with previous studies. The presence of hope is not only protective but may reduce or negate suicidal ideation and prevent such ideation from translating into a suicide attempt in patients with depression. 19 Religion has been reported as a protective factor against suicide in India. 11 In a study among students with serious suicidal ideation and/or a previous suicide attempt, the strongest RFL was the strength of religious faith. 20
Many RFD responses were strongly related to increased suicide ideation but as expected RFL were inversely related to suicide ideation and reattempts. 4 In our study, the RFD were larger in number, indicating that our sample may have perceived more reasons to die as compared to reasons to live. RFL, which are protective factors, may be less in number, but reasons as to why a person chooses to die can be numerous. Therefore, reasons to die may be important motivational drivers in the suicidal process.
Health care providers should, therefore, study reasons to die as well as emphasize reasons to live. It was rewarding to note that all our complete records had both reasons to die as well as reasons to live mentioned.
Psychiatric diagnosis and suicidality: It is estimated that 147 out of every 100,000 inpatients in units of psychiatric hospitals attempt suicide, considerably higher than in the general population (11.4 per 100,000 people). 21 Therefore, the relationship between suicide risk and psychiatric diagnosis is well documented, consistent with the findings of our study. However, most of our patients were diagnosed with mood disorders (depression most commonly) or psychotic disorders. All these diagnosed patients were living in the community.
Negative cognition about the self, others, and the future as a reason for dying was reported in 24% of the cases in our study. Negative cognition is an important factor underlying depression. Another RFD is negative cognition among patients with depression. Previous retrospective studies on the analysis of suicide notes of patients who died of suicide found “guilt” in the suicide note as a strong possible indicator of depression. 22
There is an alarming increase in the frequency of suicide attempts among younger adults to the extent that the World Health Organization selected prevention of suicide as a major goal. 23 Knowledge of why people decide to end their lives, compared to what they want to live for when they survive, may help design better-standardized suicide intervention programs and patient-specific plans to prevent suicide attempts. 13 We attempted to evaluate both reasons to die as well as reasons to live but were constrained by the scarcity of data available in records of our tertiary care general hospital outpatient department, as a large number of records could not be traced. However, among records available, men and women were similarly represented.
Limitations
The main limitation of the study is the small sample. Since this was a retrospective study, there was missing data. Another limitation was that this is only a hospital-based sample. A structured clinical interview to determine diagnosis to study reasons of living and dying would give more specific results.
Conclusion
A majority of our community-dwelling sample suffered from a nonpsychotic mood disorder. The most common modes of attempting suicide were hanging, jumping from heights, or lying on railway tracks, followed by prescription medication or drug overdose. Both RFD and for living could be grouped in similar categories, for example—family conflict vs. family responsibility and hope vs. hopelessness.
Footnotes
Acknowledgements
We are thankful to Mrs Navneet for her input in this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Salary support for JRF was from Indian Council of Medical Research under capacity building projects for National Mental Health Program, ICMR-NMHP. Salary of Triptish Bhatia was supported by “Cross-Fertilized Research Training for New Investigators in India and Egypt” (D43 TW009114), funded by Fogarty International Centre, NIH.