
Abstract
Background:
Mental health conditions are highly prevalent, and both supply- and demand-side factors drive a high treatment gap. There is a dearth of socio-culturally appropriate measures to assess barriers to professional help-seeking in distressed non-treatment seekers. This study aimed to develop and validate the Barriers to Seek Professional Help for Mental Health Scale for distressed, non-treatment-seeking young adults experiencing common mental health concerns in the Indian context.
Methods:
The study was conducted in three phases: Phase I: development of initial measure; Phase II: scale try-out (N = 190); and Phase III: validating the factor structure (N = 172). Distressed, non-treatment-seeking young adults (20–35 years old) were recruited for the present study. Exploratory factor analysis (EFA) was used to identify the factor structure, and confirmatory factor analysis (CFA) was conducted to validate it.
Results:
EFA showed that a five-factor structure best fits the data, namely, stigma and minimization, instrumental barriers, problem perception, self-efficacy in service utilization, and negative service expectancies. CFA revealed that the model was a reasonably good fit. The scale was finalized into a 24-item measure. Internal consistency reliabilities of the scale and subscales were satisfactory. Correlation patterns of barriers subscales with help negation, help-seeking inclination, and distress support its convergent validity.
Conclusion:
The Barriers to Seek Professional Help for Mental Health Scale was developed, and preliminary evidence supports its reliability, construct, and convergent validity. The scale could prove valuable for assessing barriers to seeking professional help for mental health in the Indian context, developing help-seeking interventions, and examining their effectiveness in increasing the uptake of mental health services.
The Barriers to Seeking Professional Help for Mental Health Scale was developed to specifically capture socio-culturally relevant barriers to current distress among non-treatment-seeking young adults in urban India. Preliminary evidence suggests that scale is a reliable and valid measure for this target group. It can be used to evaluate barriers to seeking professional help for mental health in the urban Indian context, develop interventions, and examine their effectiveness in increasing the uptake of mental health services.Key Messages:
As per the National Mental Health Survey 2015–2016 of India, despite the high prevalence of common mental disorders, the treatment gap remains high. 1 From 2012 to 2030, India is projected to incur economic losses amounting to USD 1.03 trillion due to mental disorders. 2 The greatest share of mental disorders falls upon young adults, who make up the largest proportion of the productive sector in society. 3 The age of onset of more than half of the mental disorders is by mid-20s. 4 During this period, it is highly unlikely for young people to seek professional help, resulting in immediate and prolonged functional limitations, reduced education and career opportunities, and the possibility of comorbid conditions. 5
Various studies have investigated the factors underlying the reluctance to seek professional help.1-1 Among young adults, these barriers include stigma, limited knowledge about mental health, negative attitude toward mental illness, socio-cultural beliefs, strong inclination toward self-reliance, preference for informal support, concerns about confidentiality, doubts about the effectiveness of treatment, and structural barriers such as cost, travel, and accessibility.1,1,1
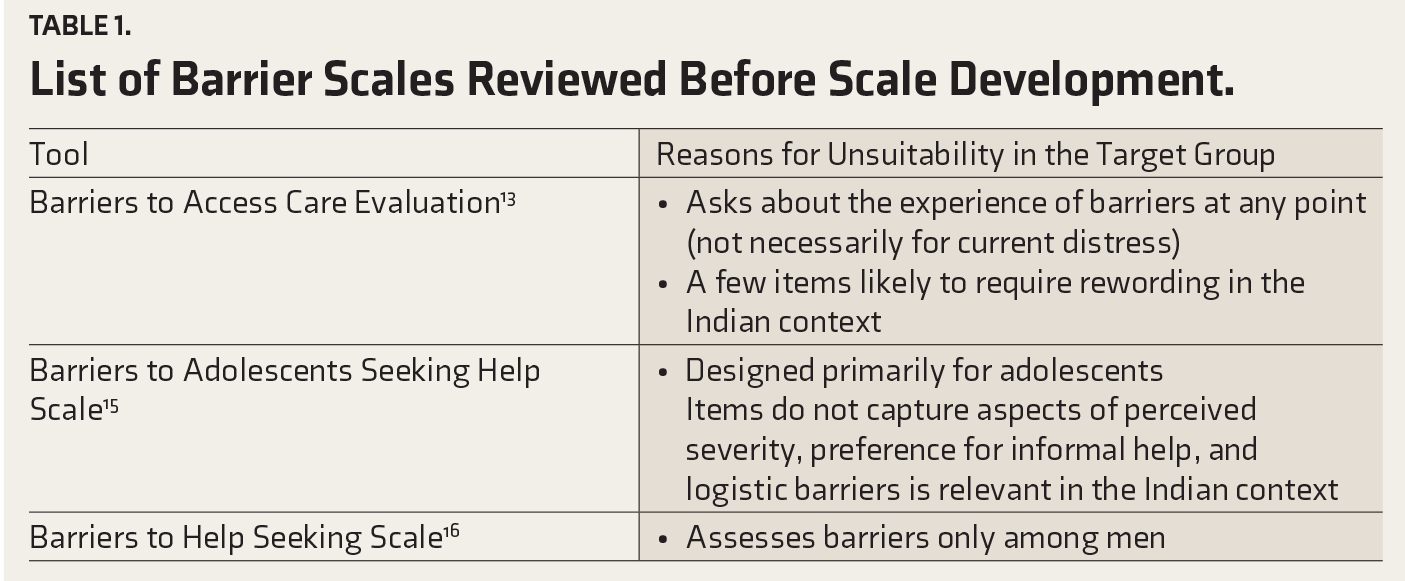
Studies have assessed barriers using surveys, semi-structured interview schedules, self-designed questionnaires,1-1 and standardized measures including Barriers to Access to Care Evaluation, 13 Perceived Need for Care Questionnaire, 14 Barriers to Adolescents Seeking Help Scale, 15 and Barriers to Help Seeking Scale, 16 among others. A scan of the literature revealed that although several assessment tools are available to assess barriers, these are either not worded to assess barriers related to current distress or do not target distressed young adults currently not seeking treatment. Additionally, some items in other measures were not socio-culturally appropriate for the Indian population (Table 1).
List of Barrier Scales Reviewed Before Scale Development.
Therefore, the present study aimed to develop and validate a new tool to address these lacunae. The Barriers to Seek Professional Help for Mental Health Scale (BSPH-MH Scale) was expected to cover a comprehensive range of barriers faced by distressed, non- treatment-seeking young adults (D-NTS) in the Indian context to seek professional help for mental health.
Methods
The present study was part of a larger research project on a pilot evaluation of a help-seeking intervention among D-NTS to reduce barriers and improve inclination and behavior for professional help-seeking for mental health. 17 The study was initiated after approval from the Institute Ethics Committee.
The study was conducted in phases: Phase I: development of the initial measure; Phase II: scale try-out; and Phase III: validation of the factor structure and convergent validation, as described below. Written informed consent was sought from all participants at various phases of the study. The data collection process began in January 2021 and ended in December 2021.
Phase 1: Development of the Initial Measure
An extensive literature review was conducted to understand help-seeking barriers in general, in the Indian context, and among young adults in particular.1-1 Various available measures and their constituent items that assess barriers to help-seeking for mental health were also scrutinized (Table 1). A checklist was developed following the discussions within the research team. This was used in a preliminary study to explore perceived barriers and enablers of professional help-seeking for common mental health concerns among the D-NTS in the urban Indian context. 21 Findings from this study helped to fine-tune the checklist items. These were then transformed into ratings to mark the strength of barriers on a 5-point Likert scale. An attempt was made to comprehensively incorporate the items relevant to distressed young adults, which span a broad range of barriers covered in systematic reviews.1,1 The items of the BSPH-MH Scale were developed based on the existing literature review assessing various factors, including attitudinal, psychological, and structural barriers to professional help-seeking for current psychological distress.
A useful method of trying out the initial version of a scale with a small number of individuals from the target population is known as cognitive interviewing. 24 Cognitive interviews involving the think-aloud technique were used for the draft version of the BSPH-MH Scale in a convenient sample of five D-NTS young adults. These individuals were recruited from the community and invited to provide feedback. This was done to assess whether the items were meaningful to the target population and whether participants could relate the questions to the response options. During the cognitive interviews, the participants were asked to report the mental processes used in providing their answers. Participants’ feedback consisted of simplification of the language of certain items and adding some barriers not included in the list. Based on their feedback, items were modified in discussion within the research team and again administered to two additional D-NTS participants. Items were further refined after seeking their feedback, leading to the retention of 24 items.
Phase 2: Scale Try-out
A total of 24 items were finalized for the initial try-out of the BSPH-MH Scale. The instructions required the participants to respond to each item by rating whether the given barrier prevented them from seeking professional help for the current distress on a 5-point Likert scale from “1 = not at all” to “5 = to a great extent.” The possible minimum–maximum total scores ranged from 24 to 120. A higher score indicated a greater number and strength of the barriers to consult a mental health professional for current distress.
The initial try-out was conducted on 190 D-NTS (20–35 years old) recruited using purposive sampling in the community setting. Participants needed to have at least 12 years of formal education with a self-report of the current experience of psychological distress for at least two weeks, should not be seeking professional help for their current distress, and have a working knowledge of the English language. These criteria were mentioned in an announcement message containing a hyperlink to the informed consent form and assessment measures circulated on social media platforms such as Facebook, Instagram, LinkedIn, and WhatsApp. The link included an informed consent form explaining the purpose of the study and contact details of the first author for any clarification/referral-related guidance. The form elicited socio-demographic information and included the Kessler Psychological Distress Scale (K10) 25 to assess current distress levels. The data of only those participants who scored above the cut-off for distress on K10 were used for the analysis reported. Additionally, the form contained the newly developed 24-item BSPH-MH Scale. The total time required to complete the online assessment was about 15 minutes.
Exploratory factor analysis (EFA) was carried out from the obtained data using the principal axis factoring via IBM SPSS 20. This was done to identify and express the data regarding factors contributing to barriers to professional help-seeking for mental health. Promax rotation with Kaiser normalization of the original factor matrix was used after that to ensure better interpretability of the factor structure. The Kaiser–Meyer–Olkin (KMO) measure and Bartlett’s test of sphericity were used to examine the sampling adequacy for factor analysis. The acceptable cut-off value for communalities was considered to be 0.275 based on Zeller. 26 The extent of cross-loadings, if any, between the factors, interpretability of factors, and presence of at least three items per factor was taken into account in arriving at the factors to be retained. 27 Criteria used for retaining the factors were factor loadings ≥ 0.32, minimum cross-loadings, 28 and factor reliabilities α ≥ 0.70. 29 Three items with cross-loadings were retained under the factor with the highest loading. These sets of items were further examined for conceptual relatedness. Once these were recognized as forming meaningful sets, the factors were named.
Phase 3: Validating the Factor Structure
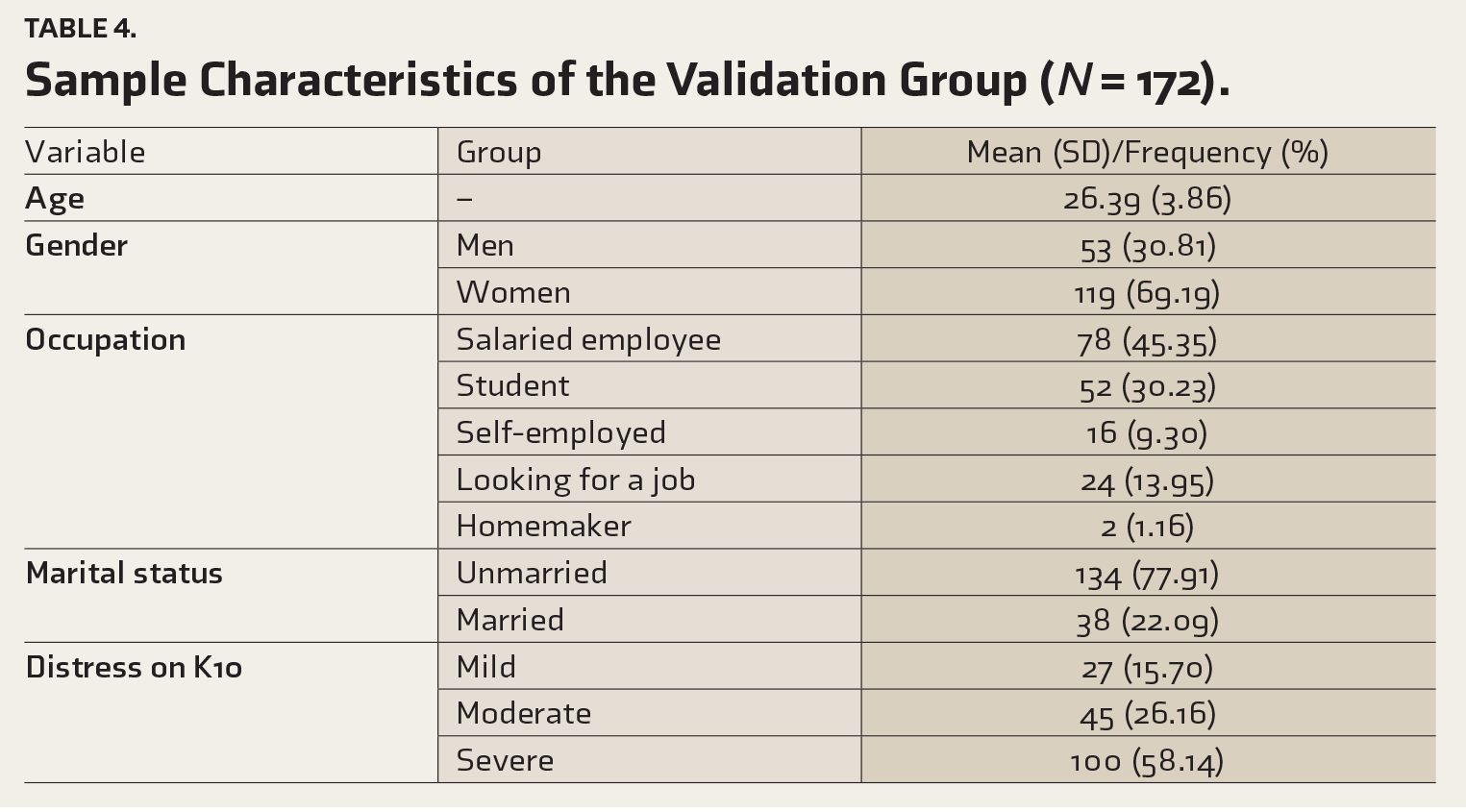
After determining the factor structure, the BSPH-MH Scale was further administered to a new sample of 201 participants, out of which 172 showed significant distress. Further analyses were conducted with these 172 participants. The same recruitment and data collection procedures as the previous phase were utilized. K10 was administered to ensure the analyzed sample was above the cut-off on distress level. In addition, two items from the General Help Seeking Questionnaire 30 on inclination to seek help from mental health professionals and help negation were also incorporated, which ask about the likelihood of seeking help for current distress on a 7-point Likert scale (1 = not at all, 7 = extremely likely). These items and total K10 scores were used to examine correlations with the barrier subscales to assess convergent validity, as these are theoretically expected to be associated with barriers and known to be related.1,1
Before conducting confirmatory factor analysis (CFA), a multivariate-normality assumption was assessed using the Doornik–Hansen test, and it was found that the data violated the assumption (χ(48) = 1,194; p <.01). Following the preliminary assessment, a CFA was conducted using the lavaan package 33 in the programming language R on the RStudio software (Version 2023.06.0). A diagonally weighted least squares (DWLS) technique was chosen to estimate the parameters of CFA models as this method is less sensitive to deviations from normality. The factor coefficient figure was prepared using Stata 18.0 (StataCorp, College Station, TX). The reliability of the subscales was examined using Cronbach’s alpha and McDonald’s omega (ω). Based on Hinton et al.’s 34 recommendations, reliability was interpreted as follows: α/ω ≥ 0.90, excellent reliability; 0.70 < α/ω < 0.90, high reliability; 50 < α/ω < 0.70, moderate reliability; and α/ω < 0.50, low reliability.
Results
Exploratory Factor Analysis
The sample characteristics of the try-out group have been described in Table 2.
Sample Description for Scale Try-out Group (
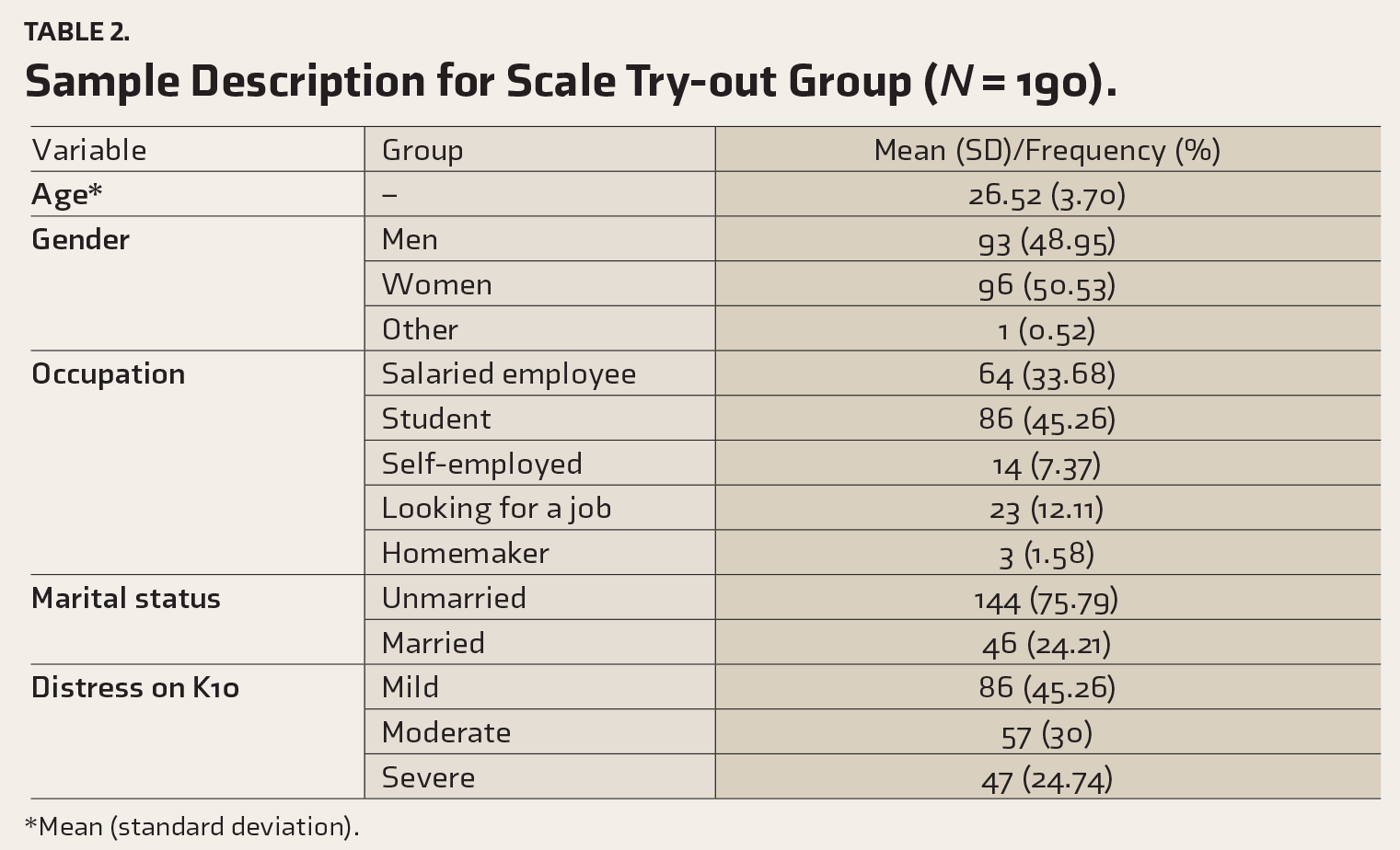
*Mean (standard deviation).
The average inter-item correlation was between 0.001 and 0.76, indicating the existence of multiple subdomains in this scale. The KMO measure verified the sampling adequacy (KMO = 0.87), and Bartlett’s test of sphericity was found to be significant (approx. χ2 = 2,340.43, p ≤ .001). Thus, the data were found to be suitable for factor analysis. 35 A five- factor structure was obtained through the principal axis factoring using Promax rotation with Kaiser normalization of the original factor matrix and explained 54% of the total variance (Table 3). The factor loadings ranged from 0.35 to 0.90. The commonalities were found to be in the acceptable range from 0.32 to 0.71. 26
Factor Structure from the Exploratory Factor Analysis.
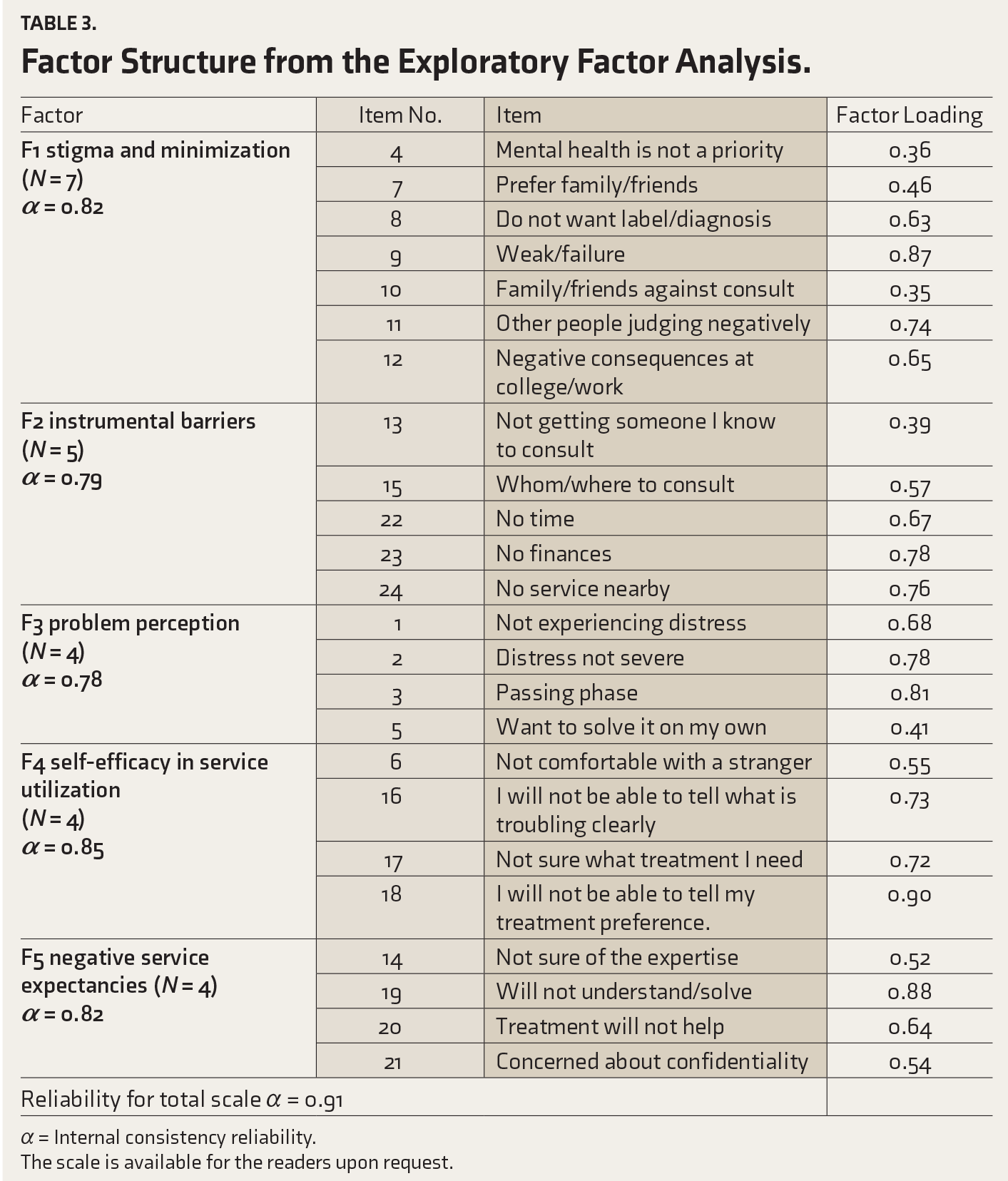
α = Internal consistency reliability.
The scale is available for the readers upon request.
Higher scores on subscales indicate higher levels of the respective factors as barriers. The first factor was named stigma and minimization, as most items here are about apprehensions of negative outcomes of disclosure to others/non-favorable views of significant others and self-stigma, in addition to an item on low prioritization of mental health. Items in instrumental barriers had to do with logistic/practical difficulties in accessing services. The problem perception subscale comprises items that reflect perceiving problems as mild and temporary; thus, self-reliance is considered satisfactory. Hence, higher scores on this subscale reflect the perception of the problem being of low severity and passing nature as the reason for not seeking professional help. All items in self-efficacy for service utilization factor had to do with low confidence in seeking professional help (e.g., difficulty articulating the problem or one’s preference). Higher scores indicate low self-efficacy, which serves as a barrier to help-seeking. The last factor comprised items that reflected low expectations of the utility of seeking professional help and were, hence, labeled as negative service expectancies. Higher scores reflect higher barriers related to negative expectancies of seeking professional help.
Validation of the Factor Structure
The sample characteristics of the validation group are described in Table 4, and the descriptive statistics of the measures used are described in Table 5. Except for the distress scores on K10, the data followed a non-normal distribution.
Sample Characteristics of the Validation Group (
Descriptive Statistics of the Measures Used (
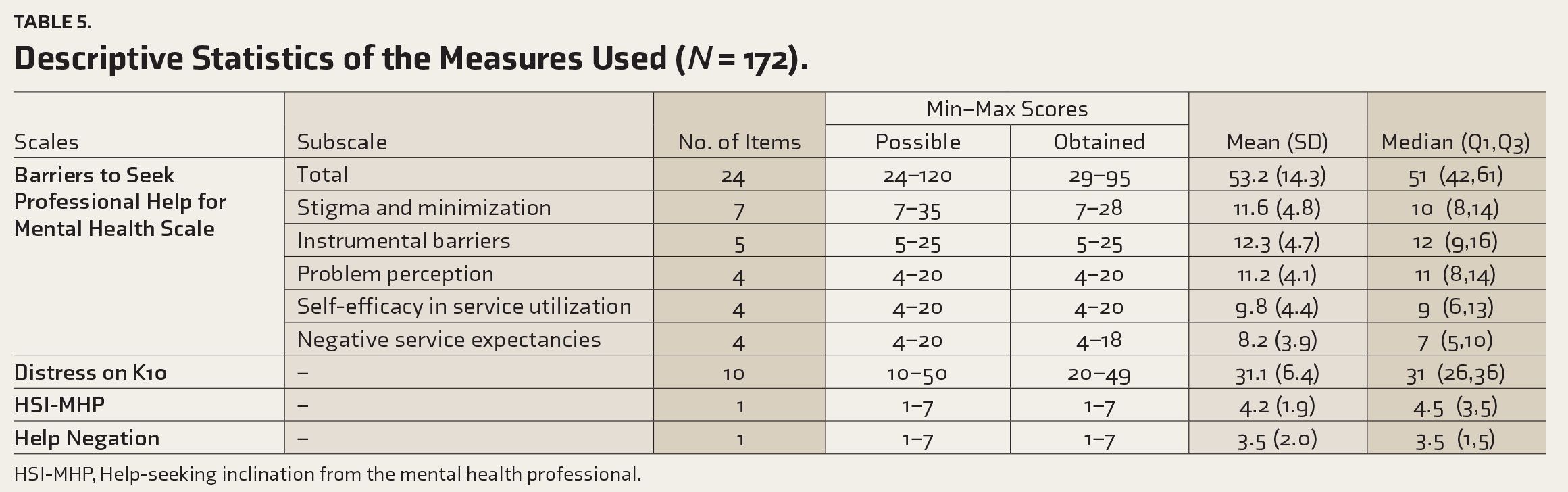
HSI-MHP, Help-seeking inclination from the mental health professional.
Confirmatory Factor Analysis
A CFA was conducted using the CFA function in the lavaan package in the RStudio software, which has a five-factor structure. The essential index values are reported in Table 6.
Indices Obtained on Confirmatory Factor Analysis.
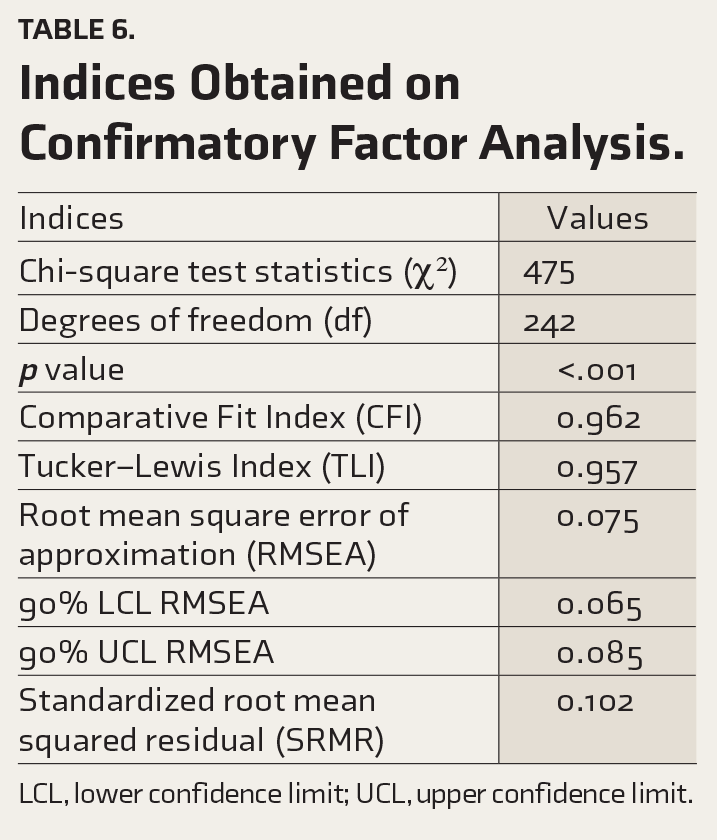
LCL, lower confidence limit; UCL, upper confidence limit.
According to Hair et al., 36 Tabachnick et al., 37 and Hu and Bentler, 38 the values of standardized test statistic/degrees of freedom < 3, CFI > 0.90, TLI > 0.90, RMSEA < 0.08, and SRMR < 0.08 are considered as acceptable fit of the CFA model to the data. The indices obtained in the current study were within the acceptable range except SRMR, which was slightly higher. Based on these findings, the model was considered a reasonable fit. Figure 1 illustrates the factor coefficients from CFA.
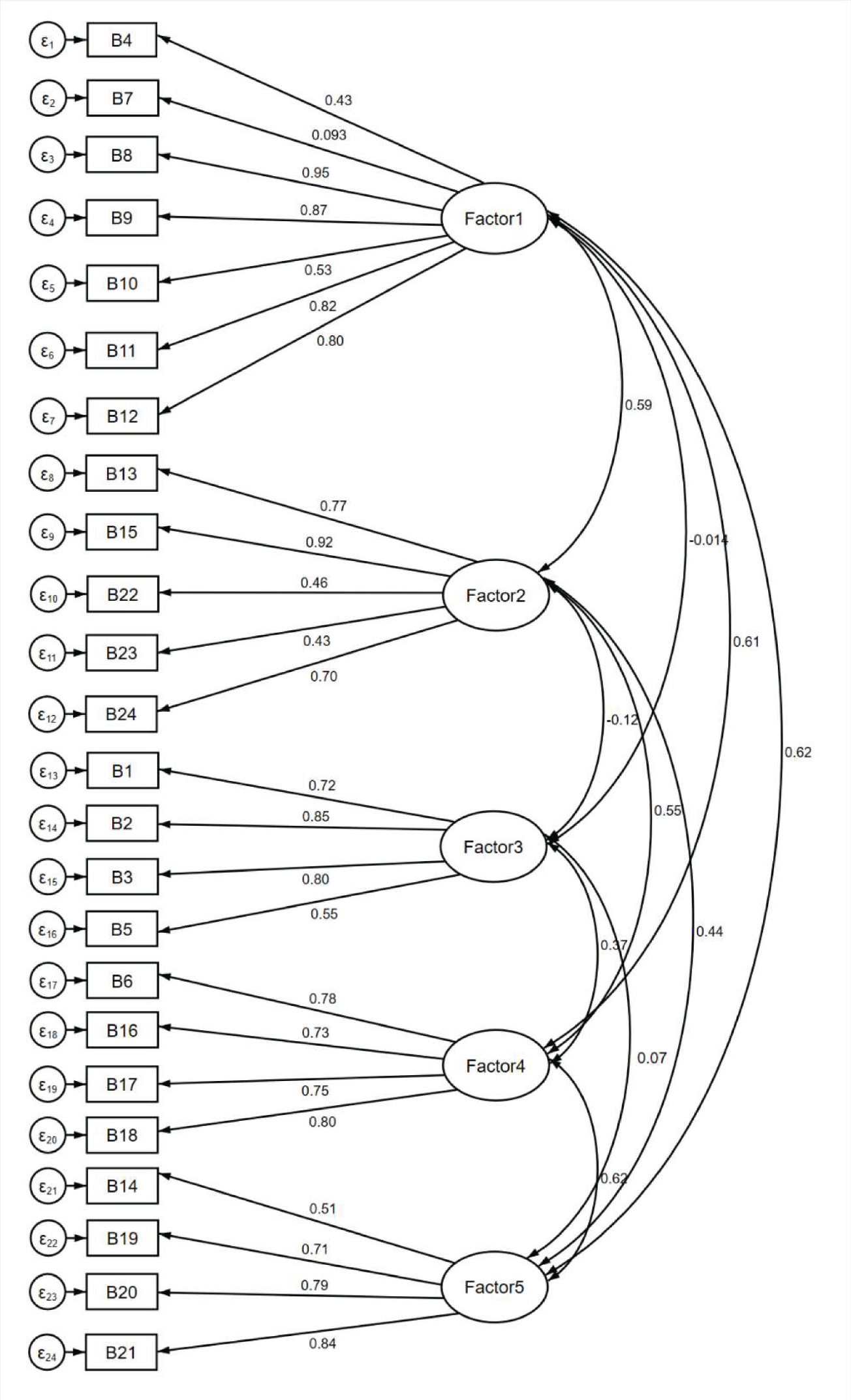
Factor 1: stigma and minimization; Factor 2: instrumental barriers; Factor 3: problem perception; Factor 4: self-efficacy in service utilization; Factor 5: negative service expectancies.
Table 7 presents McDonald’s omega for the validation sample of the total Barriers to Seek Professional Help for Mental Health Scale and its subscales, all exhibiting high reliability.
McDonald’s Omega Values of the Barriers to Seek Professional Help for Mental Health Scale and Its Subscales (
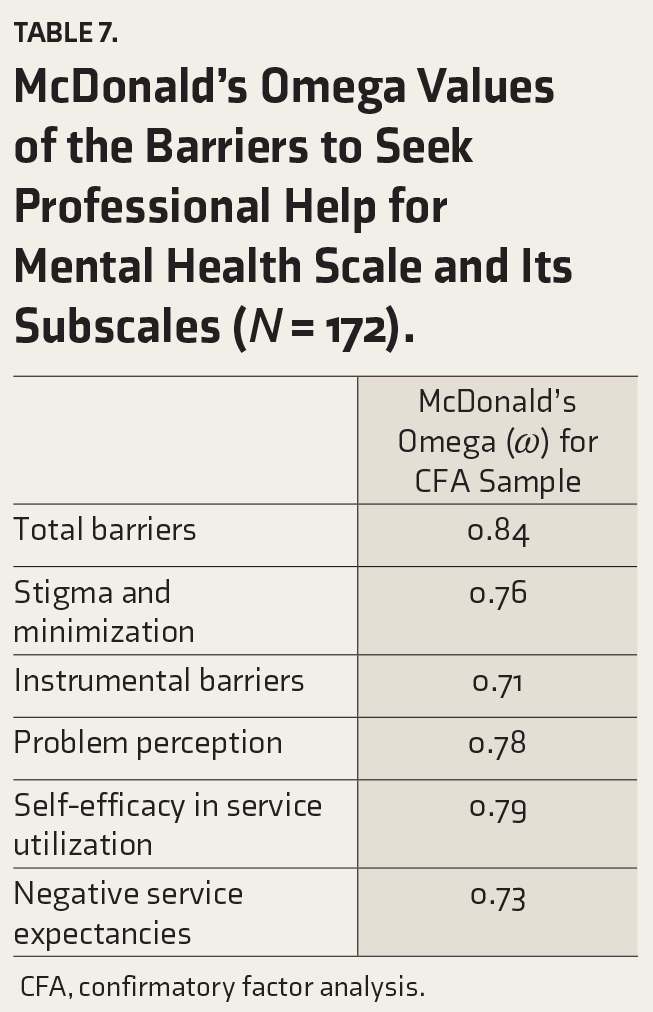
CFA, confirmatory factor analysis.
Convergent Validity
Table 8 depicts Spearman’s correlations among total scores on the BSPH-MH scale, its subscales (factors), total distress scores on K10, help-seeking inclination from mental health professionals, and help negation.
Spearman’s Correlations Among Barrier Subscales and Other Variables (
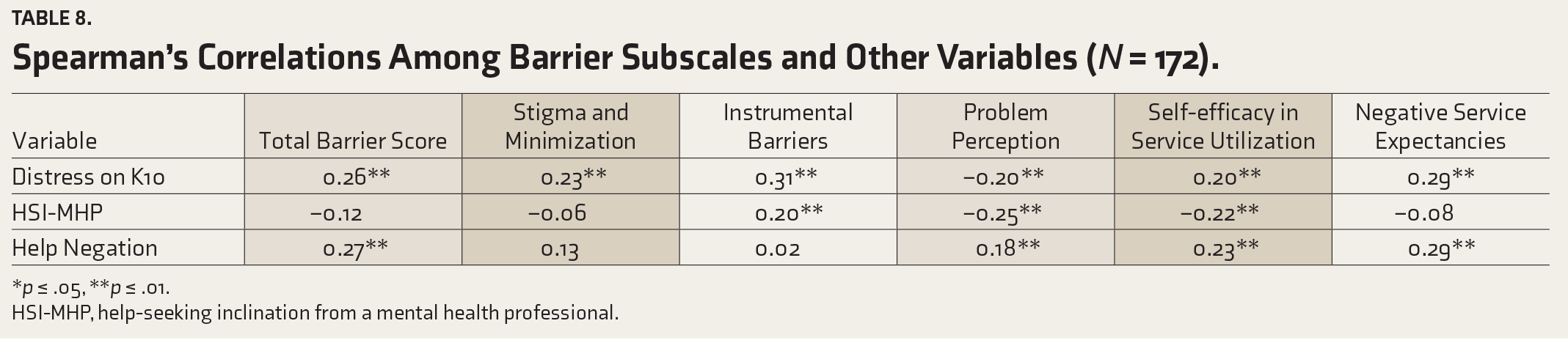
*p ≤ .05, **p ≤ .01.
HSI-MHP, help-seeking inclination from a mental health professional.
Higher distress positively correlated with total barriers and all the subscales except distress perception. Higher help-seeking inclination was significantly related in a negative direction to problem perception and self-efficacy in service utilization barriers and a positive direction to instrumental barriers. Higher help negation (inclination to not seek help from anyone) was positively correlated with total barriers, problem perception, and barriers to negative service expectancies. These findings will be discussed in the next section.
Discussion
This study aimed to develop and validate the Barriers to Seek Professional Help for Mental Health Scale for distressed, non-treatment-seeking young adults experiencing common mental health concerns in the Indian context.
The EFA findings revealed a five- factor structure, which explained 54% of the total variance. These were named stigma and minimization, instrumental barriers, problem perception, self- efficacy in service utilization, and negative service expectancies. Furthermore, CFA results showed that the model was a reasonably good fit. Similar domains have been reported in other barrier scales, for example, stigma and instrumental barriers in Clement et al. 13 and Kuhl et al. 15 However, barrier subscales similar to problem perception, self-efficacy in service utilization, and negative service expectancies have not been observed in other measures of barriers reviewed by the authors. The chi-square goodness-of-fit test of the hypothesized model was statistically significant (p < .001). However, an important limitation of this chi-square test in the context of CFA is its tendency to yield significance for data that deviates from the multivariate normal distribution. A CFA model is recommended to be considered a superior fit to the sample data if the ratio χ2/df is ≤2, a criterion our study has successfully met. 39 CFI and TLI were both above 0.95, suggesting a good fit. RMSEA was 0.075, which is within the acceptable range. The 90% confidence interval (0.065–0.085) was also reasonably narrow. The SRMR value (0.10) exceeded the conventional cut-off of 0.08. The conventional cut-offs of these indices were derived based on the ideal hypothetical scenario under certain assumptions. They may vary under different estimation techniques and the complexity of the model. The fit indices were favorable, with CFI, TLI, and RMSEA supporting a good fit. Future investigation may be performed to re-validate the factor structure with a larger sample size. 40
Stigma has been frequently targeted in help-seeking intervention studies.1,1 The BSPH-MH Scale elicited self-stigma and social stigma, which have been the leading causes of not seeking professional help. 10 The subscale of instrumental barriers involved perceived difficulty in seeking help due to time, financial constraints, lack of easy availability, and accessibility of services. These have been repeatedly noted in decades of research.1,1 This is also a significant cause for concern in low-resource settings like India. Whereas the items in the subscale of problem perception incorporated beliefs about one’s psychological distress, which could act as a barrier, for example, “thinking that my current problem is not severe stops me from consulting a professional.” Lack of perceived need for treatment has been noted as a primary barrier to not seeking help,1,1 and this is implied in the problem perception subscale in the present study. Self-efficacy in service utilization subscale covered items related to one’s belief in articulating various treatment-related processes and preferences. Negative service expectancies were seen to have elements of difficulty in using mental health services due to concerns including the expertise of the professional, perceived ineffectiveness of the treatment, confidentiality issues, etc. Similar barriers have been noted in the past.1,1
The barrier scores (total and subscales) had a significant positive correlation with distress scores, which aligns with the available literature in the Indian and global context.1,1 This also highlights the paradox that persons in distress who need professional help may experience stronger barriers in accessing such help, partly due to the salience of the barriers with increasing levels of distress. Help negation is widely known to impede help-seeking, 50 which was also observed in its significant positive relationship with the total score on the BSPH-MH Scale and three of its subscales.
Stigma as a barrier to seeking help was higher in persons experiencing higher levels of distress. However, it was unrelated to the help-seeking inclination. It is plausible that persons with high and low inclinations to seek professional help may experience stigma as a barrier. The literature is replete with studies on stigma and delays in help-seeking. 20 Whether the influence of stigma as a barrier becomes evident in the context of actual help-seeking behavior needs to be examined.
In the present study, which used a sample of distressed non-treatment seekers, a higher inclination to seek help went hand-in-hand with reporting higher instrumental barriers. Instrumental barriers may be a prominent reason for individuals not seeking help when experiencing significant distress and are inclined to seek such help. Perceived susceptibility and severity of problems are known to influence health-related behaviors. 51 In the present study, a significant negative relationship was observed between problem perception as a barrier with distress and inclination to seek professional help, along with a relationship in the reverse direction with help negation. As mentioned earlier, higher scores on this subscale indicate that perceiving one’s problems as low severity is a barrier to seeking help. Awareness that one is experiencing a mental health concern that may require treatment is the first step toward help-seeking. 52 This is likely to go hand-in-hand with higher severity of distress. Also, when an individual recognizes that the problem is not just a passing phase/and considers it significant (low score on problem perception barrier), the negation of help-seeking is likely to be lower, and the inclination to seek professional help will likely be higher. These relationship patterns align with the theoretical and empirical literature on help-seeking.1,1
Low self-confidence in utilizing services and negative service expectancies are likely to reduce the inclination to seek help, and the present study’s findings were in line with this. Tomczyk et al. 55 hypothesized that individuals with favorable views regarding the ease of accessing services have thought about seeking professional help or have amassed information, corroborating the study findings. On the other hand, individuals with vicarious or direct past negative experiences of help-seeking are likely to be reluctant to seek help.
The relationships between barriers and other variables (level of distress, help negation, and inclination to seek help from mental health professionals) were significant, albeit modest in strength. Previous studies suggest a complex relationship between variables leading to help-seeking.1,1 Similar trends regarding modest relationships between these variables have been noted in the literature.1,1 Overall, the observed patterns of relationships of the barrier subscales with other variables support the convergent validity of the new measure.
Most barrier scales have been validated on individuals already availing mental health services, 13 only students 15 or only men. 16 The scale developed in the present study was designed for and validated on distressed, non- treatment-seeking young adults. Moreover, an attempt was made to focus on comprehensive coverage of barriers that may be experienced by young adults in the urban Indian context who are known to bear a high burden of common mental health problems and exhibit low rates of professional help-seeking. The scale can aid in assessing the changes over time in barriers following the implementation of help-seeking interventions in a given population. Targeted intervention approaches to improve help-seeking in distressed non-treatment seekers via a reduction in perceived and actual barriers can be helpful in timely treatment access to reduce the treatment gap and improve quality of life.
The study has its share of limitations. Although there was heterogeneity in the sample, the generalizability of the findings needs to be examined further for non-English-speaking young adults from underprivileged and rural backgrounds and other age groups. Further studies could examine other relevant correlates of scores on the barriers scale, such as mental health literacy and attitudes, perceived peer norms, and perceived social support, to strengthen the nomological network of barriers to professional help-seeking. The nature of perceived barriers may differ in individuals with different levels of distress and inclination to seek help. For example, instrumental barriers may be more salient in those with relatively high help-seeking inclinations. Researchers need to examine such relationships by focusing on subscale scores to develop a nuanced understanding rather than relying on merely looking at the overall strength of barriers. Establishing sensitivity to change of this measure following interventions to improve help-seeking is another crucial area for further research. Development and validation of any scale are iterative processes requiring multiple trials and studies for refinement. 59 Further studies on larger and diverse samples can help strengthen the evidence base on the psychometric properties of the BSPH-MH Scale.
Conclusion
The Barriers to Seeking Professional Help for Mental Health Scale was developed to specifically capture culturally and socially relevant barriers to current distress among non-treatment-seeking young adults in urban India. Preliminary evidence suggests that the scale is a reliable and valid measure for this target group. The scale has potential utility for understanding the nature and severity of barriers in non-treatment-seeking distressed samples to inform the development of interventions and assess their effectiveness in enhancing the uptake of mental health services.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Ethical approval was obtained from the Institute Ethics Committee (Approval no.: NO.NIMH/DO/IEC (BEH. Sc. DIV)/2019).
Funding
The authors received no financial support for the research, authorship and/or publication of this article. However, the first author received a fellowship from the Indian Council of Medical Research to pursue her PhD course under the supervision of the second and fourth authors, and the present study forms a part of the PhD work.
Informed Consent
Written informed consent was sought from all participants at various phases of the study.