
Abstract
Background:
Although early maladaptive schemas (EMSs) have been suggested as potential vulnerability markers for alcohol dependence (AD), there is less emphasis on addressing these schemas in substance abuse treatment programs. We thus aimed to examine the change in schemas in response to cognitive therapy in individuals with AD.
Methods:
In this an open-label randomized controlled study, individuals with alcohol dependence syndrome (ADS, n = 84) were randomized to the intervention group (n = 45), which received six cognitive therapy sessions combined with treatment as usual (TAU), or the control group (n = 39), which was on TAU only. Participants were assessed on the measures of EMSs, alcohol use severity, and perceived stress at baseline and posttreatment.
Results:
The intervention group showed significant improvement in 5 out of 18 EMSs, that is, emotional deprivation, defectiveness, self-sacrifice, unrelenting standard, and negativity, compared to the control group, at the end of the treatment. There was a significant between-group effect for perceived stress but not for alcohol use severity.
Conclusion:
EMSs can be changed with cognitive therapy in individuals with AD and could be a crucial area to address in treatment programs. Further studies with long-term follow-up are warranted.
The trial was registered with the Clinical Trials Registry—India (CTRI/2015/12/006441) on December 17, 2015.
This is the first study exploring change in early maladaptive schemas following cognitive therapy in individuals with AD. Cognitive therapy combined with TAU shows promising results in schema change than TAU alone. Addressing schemas could be a crucial component of the AD treatment program.Key Messages:
Anational survey reported the prevalence of alcohol dependence (AD) as 2.7% in the general population and 19% among current alcohol users. 1 Despite addressing a wide range of causal factors, the risk of relapse after treatment remains substantial.2, 3 As a result, addressing additional underlying vulnerability factors for AD is essential for its effective management.
The cognitive model stresses the significance of cognitive processes in psychological problems as both causal factors and therapeutic transformation mechanisms. Cognitive processes linked with continued alcohol use have usually been addressed. 4 However, substance abuse is a complex process characterized not just by substance-related maladaptive beliefs but also by deeply held, persistent, dysfunctional basic beliefs or early maladaptive schemas (EMSs). 5 The maladaptive schemas can lead to biases in the interpretations of events and ultimately result in various psychological problems, including AD. 6 Numerous studies reported a higher prevalence of schemas in alcohol and other substance use disorders than in the nonclinical population.7–9
Literature suggests that addressing maladaptive schemas may improve substance use outcomes because of their integrity with personality structure and underlying impact on substance use.10–12 Dual focus schema therapy (DFST) was developed by Ball11, 12 to modify EMSs among chronic substance users with comorbid personality disorders. DFST is a six-month-long treatment that integrates strategies from schema therapy 6 and relapse prevention. 13 It has shown promising results in reducing the severity of substance use. Unfortunately, implementing a long-term substance abuse treatment program in a hospital setting where most patients come from a low socioeconomic background and also have a low educational level could be challenging because of issues such as financial constraints, travel time, employment-related concerns, inadequate knowledge, and understanding of psychotherapy, etc.
Limited previous research studies have examined the schema change in substance abuse treatment programs. 14 To date, only two studies have examined the change in the maladaptive schema following substance abuse treatment. Roper et al. 8 used a psychoeducational program for alcohol abuse in a residential setup and found significant changes in 13 out of 15 maladaptive schemas. Shorey et al. 15 implemented a 4-week residential 12-step facilitation therapy among males with alcohol or opioid dependence and demonstrated a decline in 8 of 18 maladaptive schemas. However, concern was raised about the mechanism of schema change (whether it was because of remaining sober while being in a residential setup or increased coping skills following treatment) and about the use of a single group, pre–post design in each of these studies. Moreover, even though schemas are resistant to change without psychological intervention,16, 17 none of those two studies used cognitive therapy, which is specifically developed to reframe maladaptive schemas. 18 Addressing EMSs in AD may contribute to improved treatment outcomes, 19 particularly in terms of reducing the risk of relapse, as these fundamental beliefs determine how an individual responds to different circumstances. Hence, the present study aimed to address EMSs and examined the change in the schema and other outcomes following cognitive therapy in individuals with AD. The study hypothesized that individuals receiving combined cognitive therapy and treatment as usual (TAU) would have a significantly greater decline in the severity of maladaptive schemas and a greater improvement in other treatment outcomes than individuals receiving TAU alone.
Material and Methods
This was an open-label randomized controlled trial, prospectively registered with the Clinical Trials Registry—India (CTRI/2015/12/006441) and approved by the Institute Ethics Committee. The data were collected between January 2016 and April 2018.
Study Participants
Participants were recruited from the inpatient and outpatient departments of a WHO-collaborated National Drug Dependence Treatment Center (NDDTC) in north India. They were diagnosed with alcohol dependence syndrome (ADS) according to The International Classification of Diseases 10th revision criteria 20 and were receiving treatment for the same. The participants had to be males aged 20 to 50 years with basic reading and writing skills. Participants were excluded if they had a major psychiatric disorder or other substance use disorder (excluding nicotine) in the past or present, as determined by the Mini International Neuropsychiatric Interview 7.0.1 21 ; a serious medical condition that could interfere with their participation or had received a structured form of psychotherapy in the past 12 months. Eligibility criteria were modified after trial commencement, and participants who had an uncooperative attitude for assessment or psychotherapy were also excluded from the study.
Outcome Measures
Primary Outcome: Early Maladaptive Schemas
Young Schema Questionnaire—version three of the short form (YSQ-3SF) 6 was used to assess EMSs. It has 90 self-report items that measure 18 schemas categorized under five domains. Each of these items is rated on a 6-point Likert scale: 6 = describes me perfectly, 5 = mostly true of me, 4 = moderately true of me, 3 = slightly more true than untrue, 2 = mostly untrue of me, and 1 = completely untrue. The score on each schema varies from 5 to 30. YSQ-3SF has a Cronbach coefficient (α) of 0.84 in the Indian population 22 and strong construct validity.
Secondary Outcomes: Alcohol Use Severity and Perceived Stress
The Addiction Severity Index (ASI), 5th edition, 23 was used to assess the severity of alcohol use (composite score). The ASI has high interrater reliability for composite scores, ranging from 0.83 to 1.00 across different areas, and adequate validity. 23 The Perceived Stress Scale (PSS)—10 24 was used to measure perceived stress (score ranges 0 to 40). The PSS-10 demonstrates adequate internal consistency reliability (α = 0.78) and validity. 24
Treatment Satisfaction
Treatment satisfaction was assessed using a five-point Likert-type scale to obtain feedback about the cognitive therapy program, where one stands for least and five stands for most, on the following dimensions: interesting, understandable, suitability and satisfaction, usefulness, promising for self-use, applicability in the future, applicable in different circumstances, and applicable out of the clinical setup.
Treatment
Cognitive therapy sessions emphasized the advanced cognitive-developmental model of substance abuse treatment. 6 This model takes into account not just substance-related maladaptive beliefs but also the role of childhood experiences and underlying maladaptive basic beliefs in the development of continued alcohol use. Therapy is primarily focused on the cognitive restructuring of distorted basic cognitions by collaboratively generating alternative balanced thoughts to induce an adaptive change in behavior. The therapist moved back and forth several times in identifying and modifying various layers of maladaptive cognition. 25 The process of orientation to cognitive therapy was made flexible depending on each individual’s aptitude for self-examination. For some patients with a concrete cognitive style, diagrams, drawings, analogies, and simple examples from our daily lives were employed to explain the cognitive concepts and related processes. The concepts of thoughts, feelings, and behavior were simplified, and a variety of typical instances were utilized to demonstrate them. Several cards depicting cognitive distortions were developed to make the procedure of spotting distortions much easier. These cards provided pictorial representations of cognitive distortions and examples of distortions in the Hindi language. Homework was assigned in all sessions using thought record sheets and an alcohol diary. Feedback was provided at the end of each session to motivate the participants to challenge their thoughts and, subsequently, their behavior. The cognitive therapy comprised six individual weekly sessions of 50 min to 1 h duration. All the assessments and therapy sessions were conducted in Hindi by a licensed clinical psychologist (G.S.) registered with the Rehabilitation Council of India and qualified from a premier government mental health institution in India. The therapist had extensive training in CBT and five years of clinical experience. The entire therapy process was supervised by an expert committee comprised of a team of consultant clinical psychologists and psychiatrists. The details of the therapy session are presented in an online-only supplementary file.
In addition, TAU involved pharmacotherapy and/or basic counseling for the treatment of AD. There was no active intervention in the TAU condition. Participants in TAU condition continued to visit their psychiatrist every two weeks or as their psychiatrist recommended. During these visits, only their medications were reviewed and no psychotherapy sessions were conducted. A few of them received basic counseling from psychiatrists during their initial visit to the treatment center. Each of these visits lasted 15 min to 20 min.
Procedure
Participants were provided information about the nature and purpose of the study and were allowed to clear any doubts. Following that, written informed consent was taken. Participants were randomly assigned to either intervention (cognitive therapy with TAU) or control (TAU only) group based on a simple randomization method using a computer-generated random number table. The random number table consisted of an open list of a random sequence of numbers ranging from 0 to 9. However, only numbers 1 and 2 were considered for the random allocation process. Furthermore, a coin toss was done only once to determine whether number “1” would be named the “intervention” or “control” group. As a result of a coin toss, number “1” was named “intervention group,” whereas number “2” was named the “control group.” The recruited participants were assigned to the intervention group whenever number 1 appeared in the list of a random sequence of numbers, whereas they were assigned to the control group whenever number 2 appeared in the list. However, no steps were performed for allocation concealment. Assessments were conducted at the baseline and posttreatment (between 6th and 10th weeks). We ensured that each group should have at least 30 treatment completers, that is, those participants who completed the postassessment. Participants in the intervention group who attended less than six cognitive therapy sessions or reported more than a three weeks’ gap between two consecutive therapy sessions were considered dropouts. All the self-rated measures used in the study were translated into Hindi using the WHO translation–back-translation method.
Statistical Analysis
Statistical analysis was carried out using the Statistical Package for the Social Sciences (SPSS) 23.0 version (IBM Corp., Armonk, NY, USA). Group comparison at the baseline and postassessment was conducted using 2 × 2 mixed factorial ANOVA with time (baseline and postassessment) as a within-subject factor and group (intervention and control) as a between-subject factor. The statistical significance level was set at P < 0.05. Multiple comparisons (n = 19) were carried out, increasing the risk of Type-1 error. As a result, the Bonferroni correction was applied using the formula: original P-value divided by the number of comparisons performed, that is, 0.05/19. This set adjusted the P-value to 0.003. Intent to treat analysis was carried out using the method of the last observation carried forward. Thus, all the randomized participants were included in the analysis. Effect sizes were examined using partial eta squared (ηp 2 ). Effect sizes of ≤0.02 were interpreted as small, ≥0.26 as large, and those in-between as medium.26, 27 For data following nonnormal distribution, the Wilcoxon signed-rank test was applied for within-group comparison and the Mann–Whitney U test, for between-group comparison.
Results
Attrition Rate
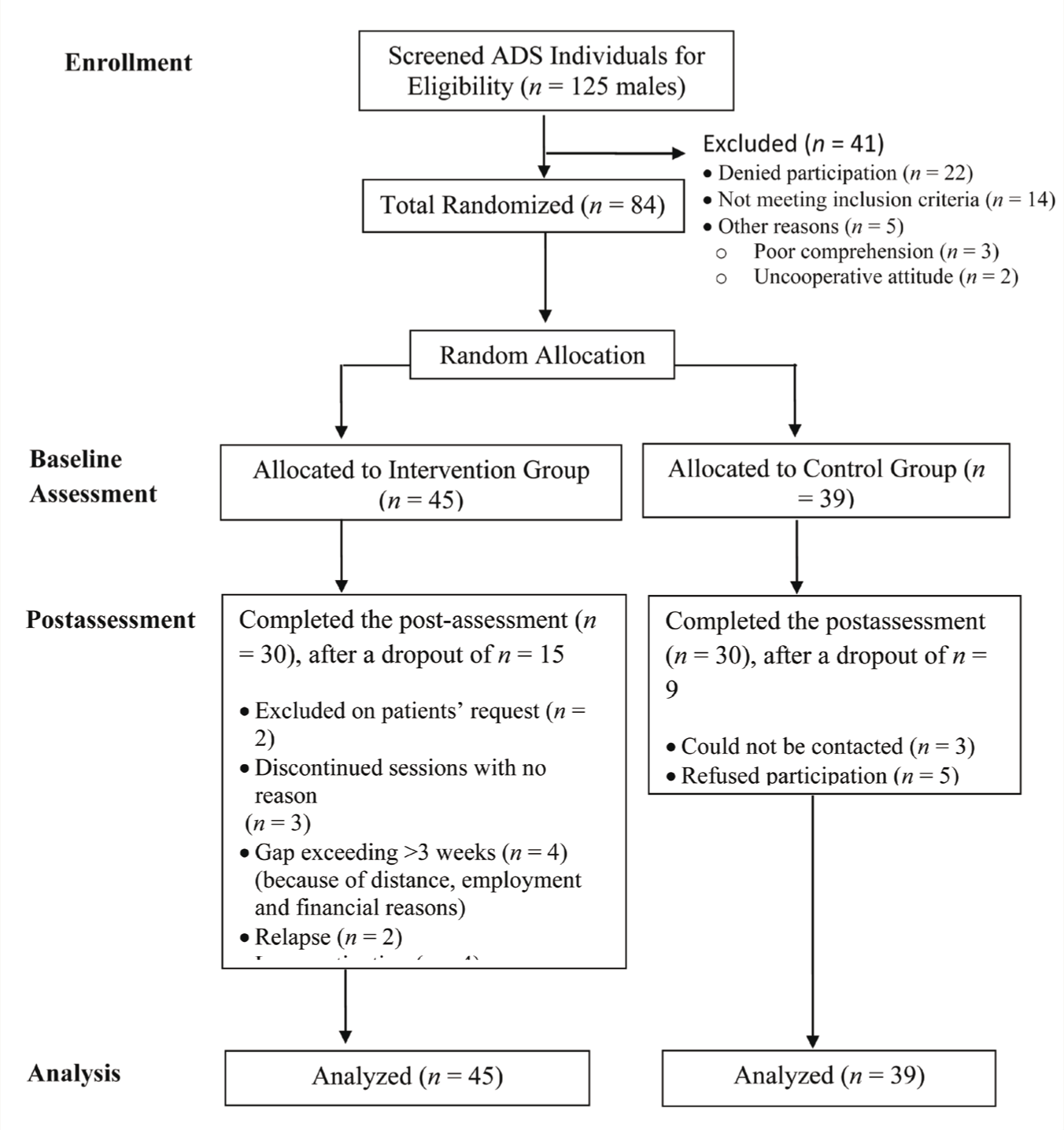
A total of 84 participants were randomly allocated into the intervention (n = 45) and control (n = 39) groups; all of them completed the baseline assessment (Figure 1). The intervention group had 15 (33%) participants who missed postassessment, whereas the control group had 9 (23%). There was no significant difference in the number of dropouts between the two groups: X 2 (1, N = 84) = 1.08, P = 0.34.
Sociodemographic and Clinical Profiles
Participants assigned to the intervention group did not differ from those in the control group on sociodemographic or clinical characteristics (Table 1). There was no significant difference between the groups in terms of average units of alcohol consumed/day (U = 821, z = 0.51, P = 0.18) or the number of days abstinent at the time of intake (U = 675, z = −1.94, P = 0.05). Most participants were educated between 10th to 12th standard, were married, and hailed from urban areas. Of the overall sample, 29 (34.52%) were from the residential setting and 55 (65.48%) were from the outpatient setting. Participants’ mean (±SD) daily use of alcohol was for 6.93 years (±4.47). None of them had received any structured form of psychotherapy in the past.
CONSORT Flow Diagram for Participants’ Recruitment and Retention
Sociodemographic and Clinical Profile of Participants by Treatment Groups
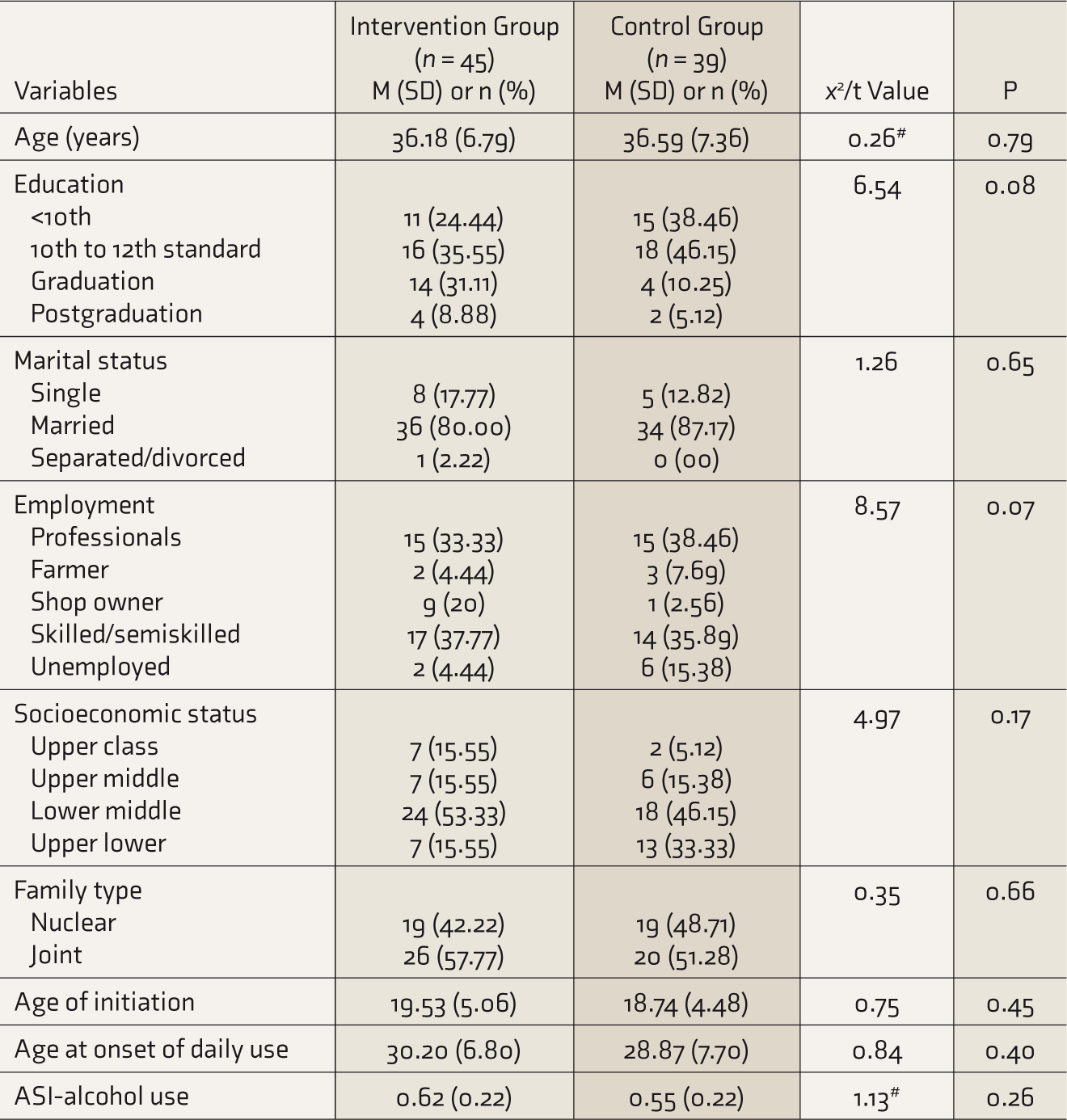
# t value.
M, mean; SD, standard deviation; n, number; ASI, addiction severity index.
Change in EMSs
There was a statistically significant interaction effect of group × time on self-sacrifice schema F(1, 82) = 14.89, P < 0.001, ηp 2 = 0.15, as well as main effects of group F(1, 82) = 12.21, P = 0.001, ηp 2 = 0.13, and time F(1, 82) = 17.02, P < 0.001, ηp 2 = 0.17 (Table 2). Simple effect analysis for the interaction revealed no difference by treatment groups on baseline self-sacrifice schema F(1, 82) = 0.46, P = 0.50, ηp 2 = 0.01, but the groups showed a significant difference on the postassessment F(1, 82) = 22.41, P < 0.001, ηp 2 = 0.21. The intervention group showed a significant decline in self-sacrifice schema, whereas no significant change was observed for control group participants.
Early Maladaptive Schemas: Main Effects of Groups and Time and Their Interaction Effects
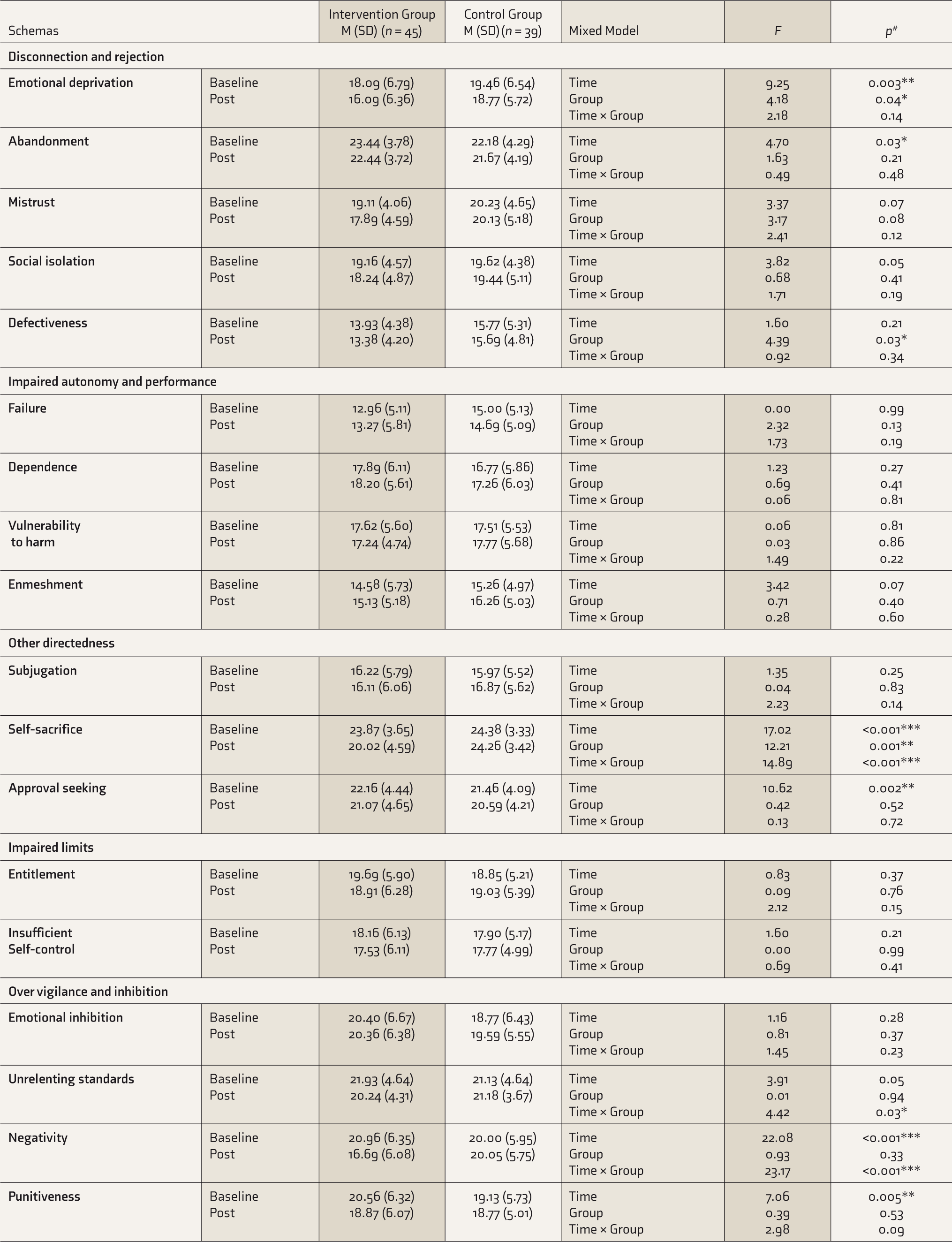
*significant at < 0.05 level, **significant at < 0.01 level, ***significant at < 0.001 level.
M, mean; SD, standard deviation; #Bonferroni correction applied.
Similarly, there was a statistically significant interaction effect of group × time for schema of negativity F(1, 82) = 23.17, P < 0.001, ηp 2 = 0.22, as well as main effects of time F(1, 82) = 22.08, P < 0.001, ηp 2 = 0.21. Simple effect analysis for interaction revealed no significant difference between the treatment groups on the baseline negativity schema score F(1, 82) = 0.50, P = 0.48, ηp 2 = 0.01, but the groups showed a significant difference on the postassessment F(1, 82) = 6.72, P = 0.01, ηp 2 = 0.08. As with the self-sacrifice schema, the intervention group had a significant decline in their negativity schema after treatment, whereas the control group showed no significant change. There was also significant interaction effect of group × time on unrelenting standard schema F(1, 82) = 4.42, P = 0.03, ηp 2 = 0.05. Simple effect analysis for the interaction revealed that the intervention group showed a significant decline in the self-sacrifice schema F(1, 82) = 8.97, P = 0.01, ηp 2 = 0.10, whereas no significant change was observed for control group participants F(1, 82) = 0.01, P = 0.93, ηp 2 = 00.
Furthermore, findings revealed a significant main effect of the treatment groups on the schema of emotional deprivation F(1, 82) = 4.18, P = 0.04, ηp 2 = 0.05 and defectiveness F(1, 82) = 4.39, P = 0.03, ηp 2 = 0.05. In addition, there was a significant main effect of time on the schema of emotional deprivation F(1, 82) = 9.25, P = 0.003, ηp 2 = 0.10, abandonment F(1, 82) = 4.70, P = 0.03, ηp 2 = 0.05, approval seeking F(1, 82) = 10.62, P = 0.002, ηp 2 = 0.16, and punitiveness F(1, 82) = 7.06, P = 0.005, ηp 2 = 0.08.
Change in Alcohol Use Severity and Perceived Stress
Both the intervention (Z = −4.10, P < 0.001) and control (Z = –2.55, P = 0.001) groups improved significantly in their composite score for alcohol use severity from baseline to postassessment, and there was no significant difference between the intervention (Mdn = 0.26) and control (Mdn = 0.17) groups (U = 797, z = –0.73, P = 0.47) at the end of treatment.
There was a significant interaction effect of group × time on perceived stress, F(1, 82) = 14.84, P < 0.001, ηp 2 = 0.15, with significant main effects of group F(1, 82) = 4.78, P = 0.03, ηp 2 = 0.06 and time F(1, 82) = 29.09, P < 0.001, ηp 2 = 0.26. Simple effect analysis showed no significant difference by the treatment groups on baseline perceived stress F(1, 82) = 0.03, P = 0.86, ηp 2 = 0.01. But the groups differed significantly F(1, 82) = 14.14., P < 0.001, ηp 2 = 0.15 at the end of treatment. The intervention group showed a significant reduction in their perceived stress from baseline (M = 26.31, SD = 3.19) to posttreatment (M = 22.40, SD = 3.49, P < 0.001), whereas no significant change was observed for control group participants from baseline (M = 26.18, SD = 3.49) to postassessment (M = 25.56, SD = 3.33, P = 0.07).
Treatment Satisfaction
The cognitive therapy program received the greatest ratings on the parameters of “being interesting” (89%) and “usefulness” (84%). The parameter of “applicability in different circumstances” received the lowest score (74%), followed by “self-use” (76%).
Discussion
This study is the first of its kind that carried out a randomized controlled trial to examine the change in EMS following cognitive therapy in individuals with AD. The study reported a significant decline in 5 out of 18 EMSs following cognitive therapy combined with TAU over TAU alone. The intervention group revealed a significantly higher decline in schemas of emotional deprivation, defectiveness, self-sacrifice, unrelenting standard, and negativity. The effect size difference for most of these schemas fell into the small range.
In line with previous research, the present study suggests that in individuals with AD, schemas decline with the effective use of intervention.8, 15 Although a previous study revealed a change in the number of schemas after a brief residential treatment (3–4 weeks) for substance abuse, the present study reported a decline in the relatively lower number of schemas, despite providing sessions of cognitive therapy, which is specifically developed to modify dysfunctional cognitive processes. 17 The decline in schemas contrasts with the theory that explains schemas as being extremely rigid and resistant to change in nature.6, 12, 17 However, changes observed in a small number of schemas after psychotherapy, on the other hand, could be a reflection of the schema’s stability and resistance to change.
It is enlightening to discuss the nature of EMSs that showed a significant decline following the treatment process and the potential mechanism of their change. Schemas of emotional deprivation and defectiveness belong to the domain of “disconnection and rejection.” Individuals who endorse these schemas have most likely had traumatic childhood experiences, and as adults, they either engage in various self-destructive relationships or entirely avoid closeness in relationships. Literature suggests a strong association of traumatic childhood experiences and interpersonal relationship difficulties with the development of substance abuse.28, 29 Therapeutic relationship, which is recognized as a potential vehicle for any sort of psychotherapy, remains crucial to the treatment of substance abuse 6 . Therefore, the therapy process may possibly have led to a decline in these maladaptive schemas. The self-sacrifice schema characterizes an excessive focus on meeting the needs of others rather than one’s own. It is frequently associated with low self-efficacy 6 and further may contribute to the initiation and maintenance of substance abuse,30, 31 possibly as a way to cope with a lack of personal fulfillment.6, 9 The therapy process involved a focus on enhancing self-efficacy, which could have resulted in a change in the self-sacrifice schema. The negativity schema indicates a tendency to persistently focus on the negative aspects of life while ignoring or underestimating the positive ones. 6 Studies have reported negativity as a risk factor for drinking motives.32–34 Certainly, the cognitive approach challenges the individuals’ cognitive processes about themselves and their situations. It promotes objective evaluation of the situation by examining evidence for and against a situation-specific negative thought, which may have resulted in a reduction in negativity schema.
In the other examined symptom domains, such as perceived stress, cognitive therapy combined with TAU performed better than TAU alone, consistent with previous studies35, 36 that have shown the efficacy of cognitive-behavioral approaches in reducing the perceived stress level. However, alcohol use severity did not differ at the end of treatment by the type of treatment received, because both groups showed improvement from baseline to posttreatment. It appears that all the individuals were already on pharmacotherapy for AD at the time of recruitment; therefore, there was little room for a between-group significant difference in alcohol use severity in such a brief period of six weeks.
The present study revealed no significant difference in the number of dropouts between the intervention and control groups. However, the intervention group’s dropout rate (33%) was slightly higher than the control group’s dropout rate (23%). The difference can be attributed to the fact that the intervention group participants were required to visit the researcher more frequently for weekly therapy sessions, whereas the control group participants were only required to visit for postassessment after a baseline assessment, which could be the reason for the higher attrition rate for the intervention group participants. Furthermore, the percentage of treatment completers (67%) in the intervention group was higher than that in many of the previous studies conducted in the addiction area (36%–64% early phase retention).37–39
The present study has several strengths compared to previous studies.8, 15 With the addition of a control group, it can be more precisely explained that the schema changes were because of the cognitive therapy rather than other factors such as the passage of time, the effect of mood state, or reduced severity of alcohol use. Previous studies investigated schema change in the residential setting, where individuals remain confined to a space with limited social interaction and are unable to participate in their daily life activities. Assessment of schema in a residential setting may not provide an accurate picture of an individual’s cognition because they may not have been exposed to circumstances that trigger their schemas. 15 Hence, the present study expanded on earlier research by involving individuals from both residential and outpatient settings to obtain a relatively accurate representation of their cognition. Unlike the previous study, the present study involved an outcome evaluation of schema change and improvements in other symptom domains, such as alcohol use severity and perceived stress.
Although the study reported positive findings, it must be interpreted in light of some limitations. The study had a small sample size and exclusively involved male participants, which limited the generalizability of the findings to a diverse population. There was no long-term follow-up to assess the persistence of schema change and the long-term sustainability of the reduction in alcohol use severity. Other limitations were the absence of an independent assessor and the lack of a formal sample size estimation method. Furthermore, because the therapist and participants could not be blinded, subjective biases on the outcome measures may have occurred as participants were aware that they were receiving therapy and therefore reported changes in the schema and stress level because of the social desirability effect.
Despite these limitations, the study’s findings are promising as it concludes that EMSs can be modified with cognitive therapy in individuals with AD. Thus, a treatment that targets maladaptive schemas may lead to the development of a more balanced and adaptive appraisal of the situations in individuals with AD and, subsequently, improved coping skills to deal with the situations that could otherwise trigger alcohol use. The study further validates Ball’s 11 recommendation to address both substance use and schemas to improve treatment outcomes. Future research is needed to examine whether the decline in the schema and other domains sustain over time with a lower rate of relapse. Research studies can further investigate the relationship between the individuals’ stage of motivation and change in their maladaptive schema and other treatment outcomes.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors thank all expert panel members for their guidance and support. The authors appreciate Dr Anamika Sahu for her valuable input and suggestions.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author, upon reasonable request. Data will be available in Mendeley data repository (doi: 10.17632/x757xsgfjr.1) from the date of publication of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning this article’s research, authorship, and publication.
Funding
This study received financial assistance from the University Grant Commission, Government of India.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.