
Abstract
Background:
A pandemic poses a significant challenge to the healthcare staff and infrastructure. We studied the prevalence of anxiety and depressive symptoms among armed forces doctors in India during the COVID-19 pandemic and the factors that contribute to these symptoms.
Methods:
The study was conducted from March 30, 2020, to April 2, 2020, using a self-administered questionnaire questionnaire using the hospital anxiety and depression scale (HADS), which was sent through Google Forms. Responses were received from 769 respondents. Data were analyzed for demographic details and HADS scores using the chi-square test and backward logistic regression.
Results:
Anxiety and depressive symptoms were seen in 35.2% and 28.2% of the doctors, respectively. In doctors with anxiety symptoms, significant associations were observed with age (20–35 years, 39.4%, P = 0.01), gender (females, 44.6%, P < 0.001), duration of service (0–10 years, 38%, P = 0.03), and clinical versus non-clinical specialties (non-clinical, 41.3%, P < 0.001) as opposed to marital status, education level, and current department of work.
In doctors with depressive symptoms, significant associations were observed with age (P = 0.04), clinical versus non-clinical specialties (P < 0.001), duration of service (0–10 years, 30.1%, P = 0.03), and doctoral degree (P = 0.04) as opposed to gender, marital status, education level, and current working department.
Conclusion:
The study revealed a high prevalence of anxiety and depressive symptoms among armed forces doctors. The main contributing factors are female gender, young age group, non-clinical specialties, and having a doctoral degree.
A high prevalence of anxiety and depressive symptoms were found among armed forces doctors in India during the initial months of COVID-19 pandemic. We recommend training of non-clinical, young, and frontline doctors with adequate medical facilities. The support system for families of doctors should be enhanced.Key Messages:
The COVID-19 outbreak has created significant fear, distress, anxiety, and depression amongst the doctors as well as the general public. Doctors are particularly prone to develop various mental health disorders as compared to the general population.3–5 A study from Hong Kong brought out the stress levels among healthcare workers during the SARS outbreak in 2003. A higher level of anxiety symptoms (36.7%: moderate–severe, 14.4%: extreme–severe), and depressive symptoms (36.3%: moderate–severe, 4.4%: extreme–severe) were reported. 6
Recently, a study from China during COVID-19 pandemic on insomnia and related factors revealed the prevalence of symptoms of stress, anxiety, and depression amongst healthcare workers to be 73.4%, 44.7%, and 50.7%, respectively. 7 A study from China estimated that the prevalence of symptoms of anxiety, depression, and both among doctors were 25.67%, 28.13%, and 19.01%, respectively, during non-COVID days in 2014. 5 Various factors associated with psychological distress during a pandemic among doctors are uncertainty about disease course, high mortality, inadequate infrastructure, lack of adequate protective equipment, no proven definitive drug treatment or prophylaxis, apprehension of transmitting the disease to family members, no vaccine, and high incidence among frontline healthcare workers.8, 9
Although various surveys on the mental health of doctors are available across the world, no such specific survey has been conducted in India among armed forces doctors during the present COVID-19 pandemic. The present survey aims to evaluate the prevalence of anxiety and depressive symptoms among the armed forces doctors and the associated factors during the COVID-19 pandemic.
Methods
Study Design
The present study employs a quantitative approach. A cross sectional survey is used to access the prevalence of anxiety and depressive symptoms among doctors during the COVID 19 pandemic.
Sample Size Estimation
The sample size was determined by using the formula N = Z α 2 P (1−P)/d 2 . In this, α was 0.05, Z α was 1.96 (at 95% confidence level), and the estimated acceptable margin of error for proportion, d, was 0.05. Based upon a previous study on psychological health in doctors in China during SARS outbreak in 2003 and a COVID-19 study from China, the prevalence of psychological comorbidities was estimated to be around 37%.6, 7 Based on the above formula, the sample size was estimated to be a minimum of 358.
Data Collection
The sample for the survey consisted of doctors in the armed forces across India. The survey was carried out during the second phase of COVID-19 from March 30, 2020, to April 2, 2020. A self-administered questionnaire was sent through Google Forms to all respondents. The Google Form asked for demographic details like gender, age, marital status, education level, duration of service, clinical versus non-clinical specialty, and current working department, and a validated tool to assess the psychological health of doctors. We received a total of 769 responses from doctors. Out of these, 20 were removed during the cleaning of data, and 749 were analyzed.
Measures
A self-administered scale was used to assess anxiety and depressive symptoms. Hospital anxiety and depression scale (HADS) 10 has 14 items (7 each for depression and anxiety), with a score ranging from 0 to 21. The score of 0–7 is taken as normal, and 8–21 is taken as abnormal for both symptoms. The HADS was initially designed for use in hospital practice. However, its use with the general population is well validated. The Cronbach Alpha for anxiety and depression subscales is 0.83 and 0.82, respectively, with a mean correlation of 0.561. The HADS was not used for the diagnosis of anxiety and depression; it was only used as a screening tool for anxiety and depressive symptoms.
Statistical Analysis
The data was analyzed using the IBM SPSS Statistics 23 for windows (Version 23.0., IBM Corp., NY, USA). χ 2 analysis was used to analyze the descriptive statistics and their association with anxiety and depressive symptoms. Backward logistic regression analysis was used for variables with either bivariate comparison or subject of interest to the author. The results are reported as βs (coefficients of regression) and standard error (SE). A P value of less than 0.05 was considered to be statistically significant.
Ethical Considerations
Ethical clearance was obtained from the Institutional Ethics Committee. Written Informed consent was taken from all the respondents before filling out the questionnaire.
Results
Sociodemographic Characteristics
Descriptive Statistics for the Characteristics and Their Associations with Anxiety and Depressive Symptoms Using the Chi Square Tests
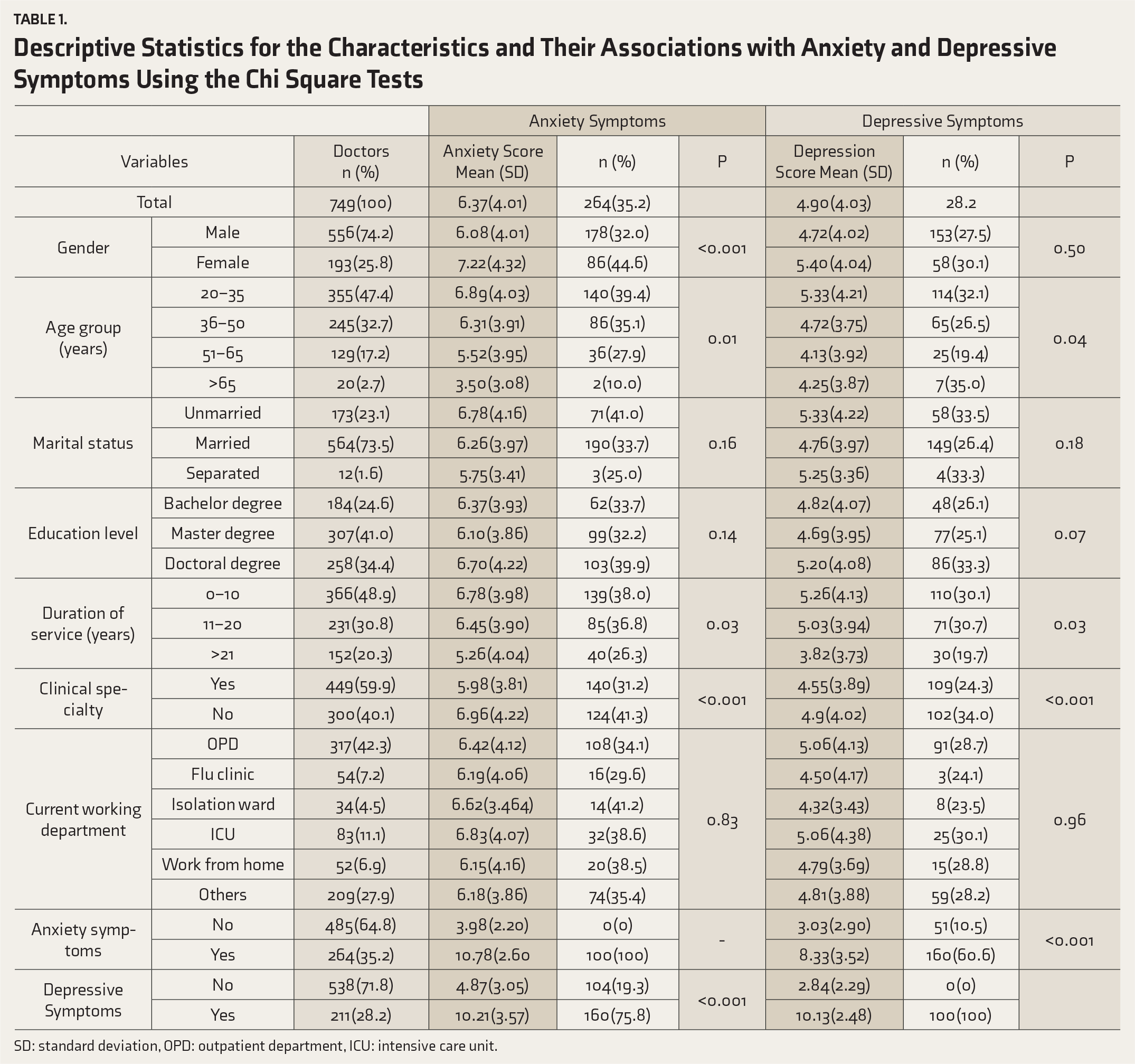
SD: standard deviation, OPD: outpatient department, ICU: intensive care unit.
All the participants were divided into two groups based on the HADS score. The participants with a score of ≤7 were assigned to the non-anxiety/non-depressive group, and those with score > 7 were assigned to the anxiety group or the depressive group. The mean (SD) anxiety score and the prevalence of anxiety symptoms were 6.37 (4.01) and 35.2%, respectively. The mean depression score and the prevalence of depressive symptoms were 4.90 (4.03) and 28.2%, respectively. In the anxiety group, significant associations were observed with age (P = 0.01), gender (P < 0.001), duration of service (P = 0.03), and clinical vs non-clinical specialty (P < 0.001). No association was found with education level (P = 0.14), marital status (P = 0.15), or current working department (P = 0.83).
In the depression group, significant associations were observed with age (P = 0.04), clinical vs non-clinical specialty (P < 0.001), and duration of service (P = 0.03). No association was found with gender (P = 0.50), education level (P = 0.07), marital status (P = 0.18), or current working department (P = 0.96).
Table 2 shows the multivariate analysis of the factors associated with anxiety and depression. Factors associated with anxiety symptoms were female gender, age less than 65 years, and having depressive symptoms. Similarly, factors associated with depressive symptoms were age more than 65 years, duration of service between 11 and 20 years, belonging to non-clinical specialties, with a doctorate, and having anxiety symptoms.
Discussion
Multivariate Analysis Showing the Factors Associated with Anxiety and Depression in Doctors
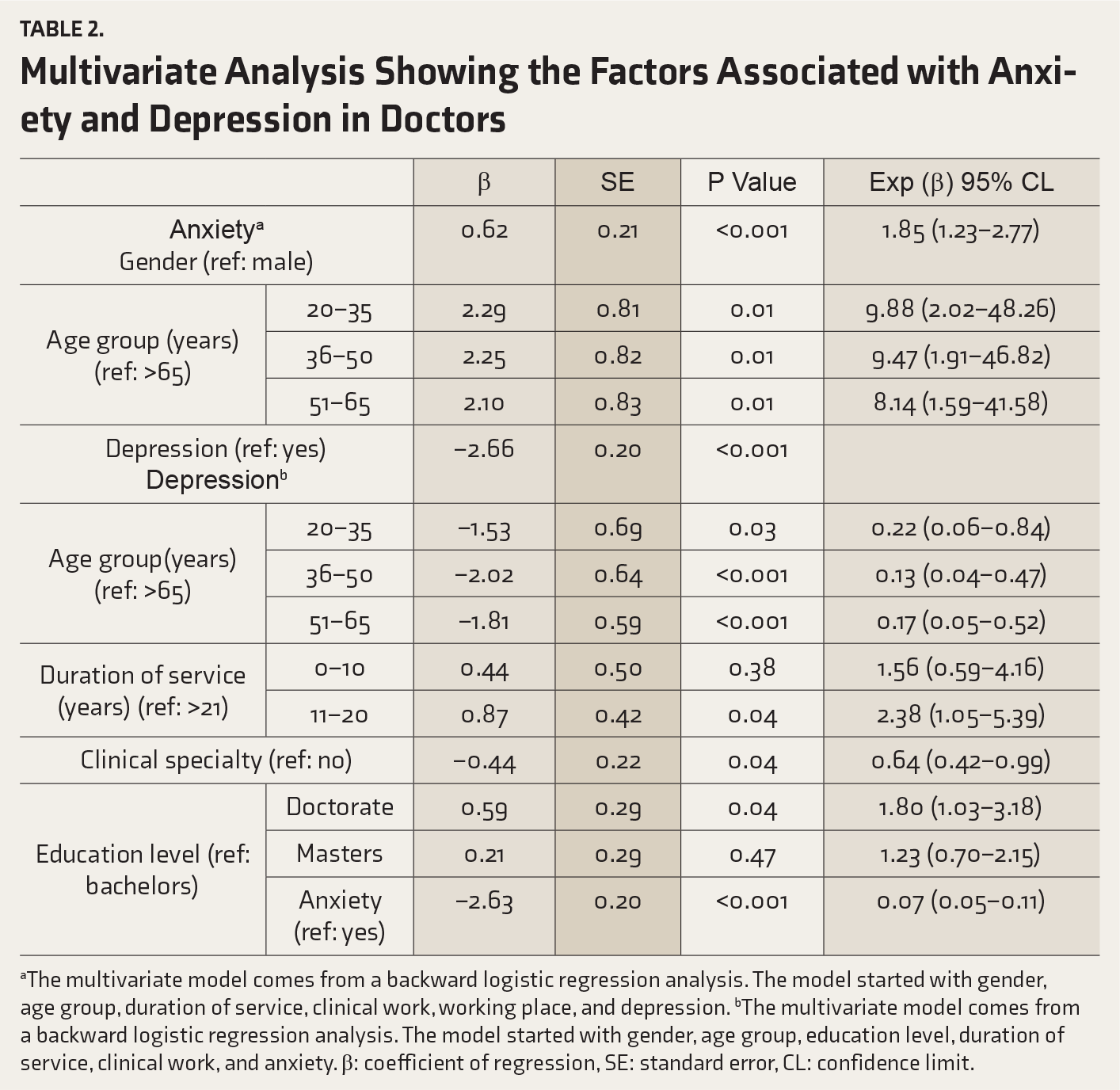
aThe multivariate model comes from a backward logistic regression analysis. The model started with gender, age group, duration of service, clinical work, working place, and depression. bThe multivariate model comes from a backward logistic regression analysis. The model started with gender, age group, education level, duration of service, clinical work, and anxiety. β: coefficient of regression, SE: standard error, CL: confidence limit.
A cross-sectional study from China during non-COVID days revealed the prevalence of anxiety and depression in doctors to be 25.67% and 28.13%, respectively. 5 Similarly, other studies from Norway, Canada, Britain, United States, Benin, and Japan revealed the prevalence of depression as 11%, 15.5%, 12%, 11.3%, 14%, and 8.8%, respectively.14–19 The present study revealed similar depressive symptoms as compared to the Chinese study during non-COVID days and a high prevalence of depressive symptoms as compared to other developed countries during non-COVID days. The reason behind this could be social and cultural differences, the level of healthcare infrastructure, and apprehension due to the pandemic. In general, doctors in India and other developing countries are overworked. They have long hours of duty, limited resources, demanding patients, medicolegal issues, apprehension of transmitting the disease to the family members, inadequate emotional support from family members, and less family time; this leads to an increase in burnout, anxiety, and depression.9, 20, 21 Our study has revealed a high prevalence of symptoms of anxiety and depression, which are likely due to uncertainty about disease course, potential mortality, inadequate infrastructure, lack of adequate protective equipment, lack of definitive drug treatment or prophylaxis, lack of a vaccine, and high incidence of infection among frontline healthcare workers.
The risk factors for anxiety were female gender, age groups of 20–35, 36–50, or 51–65 years, service bracket of 0–10 or 11–20 years, being in non-clinical specialties, and working in primary care hospital. A higher prevalence of anxiety symptoms in females is consistent with other studies from India and Western countries, and the reason could be gender discrimination, sociocultural factors, greater family responsibility, and perinatal factors.21–23 The reasons for higher anxiety symptoms in younger doctors are probably the direct exposure and their longer working hours. Also, doctors with service > 21 years have an advisory role, predominant administrative responsibility, and less direct contact with patients during the pandemic. A study on faculty doctors from the southern part of India revealed high perceived job stress among doctors aged <45 years (73%) compared to 18% of those aged >45 years. 24 Our study revealed that doctors in clinical specialties had fewer anxiety symptoms than those in non-clinical specialties. Marital status and the current working department had no significant impact on the prevalence of anxiety symptoms.
The risk factors for depressive symptoms were being in the service bracket of 11–20 years, age more than 65 years, and working in non-clinical specialties. No significant association of depressive symptoms was found with gender, marital status, education level, working place, or current working department. Our study revealed higher symptoms of anxiety and depression among armed forces doctors in non-clinical specialties as compared to clinical. A study on psychological stress among resident doctors and faculty doctors had revealed higher stress in clinical specialties.24, 25 Our results do not corroborate with the results of the studies mentioned above, likely reasons are the inevitable shortage of doctors and the apprehension among doctors in non-clinical specialties who are roped into work in COVID-19 OPD/wards in view of the pandemic. Our results are consistent with data reported from other studies; notable among them are Chinese study during the COVID-19 outbreak and study during the SARS outbreak, which revealed a higher prevalence of anxiety and depressive symptoms in healthcare workers.10, 26
To conclude, the present study has revealed a high prevalence of symptoms of anxiety and depression during the COVID-19 pandemic. No such studies are available on psychological stress among armed forces doctors during non-pandemic days; hence, the present prevalence of anxiety and depressive symptoms among armed forces doctors cannot be compared with pre-pandemic data. It is of paramount importance to prevent the attrition of limited doctors in the country. As such, prevalence of psychological stress is higher among armed forces personnel even in peacetime due to separation from family and unique working hours. 27 The present pandemic, as the study shows, is likely to augment their psychological stress further and requires measures to counter the same.
To reduce anxiety and depressive symptoms, we recommend training of non-clinical, young, and frontline doctors with adequate provision of personal protective equipment and medical facilities. The support system for the families of armed forces doctors should be enhanced too.
This study had some limitations. First, it was majorly conducted in hospitals of the armed forces of India, which limits its generalization to all doctors in the community. Secondly, this is a cross-sectional study and lacks long-/short-term follow-up. Thirdly, the tool used was for screening of psychological health and not for diagnosis. Lastly, the study was conducted within a very short time in the early phase of the pandemic, which might have caused underestimation of psychological stress.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.