
Abstract
Background:
Perinatal depression (PND) is often under-treated and under-recognized. It has a negative impact on infant development and mother–child interactions. This study aims to estimate the prevalence of PND during pregnancy and in the postpartum period and the effect of sociodemographic factors, psychosocial stressors, and obstetric and neonatal factors on PND.
Methods:
166 antenatal mothers attending tertiary center, who completed the 1st-trimester, were evaluated on baseline sociodemographic, psychosocial, obstetric, neonatal, and post neonatal factors by using a semi-structured questionnaire. Periodic prospective assessments were done using Hamilton depression rating scale (HAMD) at the end of the second and third trimesters and first and sixth weeks of the postpartum period.
Results:
Prevalence of PND was 21.7%, 32.2%, 35%, 30.4%, and 30.6%, at the end of the first trimester, during second, and third trimesters, and first and sixth week postpartum, respectively. Factors significantly associated with depressive symptoms included history of previous children with illness (P: 0.013, OR—5.16, CI—1.3-19.5) and preterm birth (P: 0.037, OR—3.73, CI—1.1- 13.2) at the time of recruitment; history of abuse (P: 0.044, OR—3.26, CI—1.1-10.8) and marital conflicts (P: 0.003, OR—3.2, CI—1.4-6.9) by the end of second trimester; history of miscarriages (P: 0.012, OR—2.58, CI—1.2-5.4) by the end of third trimester; lower SES (P: 0.001, OR—3.48, CI—1.64-7.37), unsatisfied living conditions (P: 0.004, OR—2.9, CI—1.4-6.04), alcohol use in husband (P: 0.049, OR—2.01, CI—1.1-4.11), history of depressive episodes (P: 0.049, OR—2.09, CI—1.1-4.46), history of high-risk pregnancy (P: 0.008, OR—2.7, CI—1.29-5.64), history of miscarriages (P: 0.049, OR—2.04, CI—1.1-4.2), stressful events in the postpartum period (P: 0.043, OR—2.58, CI—1.01-6.59), IUD (P: 0.002), preterm birth (P: 0.001), congenital malformations (P: 0.001), dissatisfaction with the sex of the child (P: 0.005, OR—3.75, CI—1.42-9.91), poor family support (P: 0.001), and low birth weight (P: 0.001, OR—16.78, CI—6.32-44.53) in the postpartum period. These analyses are purely exploratory.
Conclusions:
PND is highly prevalent from the early antenatal period onwards; this warrants periodic assessment of depression among high-risk mothers, using a validated tool, for early diagnosis and management.
The prevalence of PND is high, especially during 3rd trimester. Hence, it is very important to assess the mental health of all pregnant women.Key Messages:
Depression is the most common mood disorder in the general population and is approximately twice as common in women. 1 Worldwide, about 10% of pregnant women and 13% of women after childbirth, and in developing countries, 15.6% during pregnancy and 19.8% after childbirth, have experienced depression; postpartum depression (PPD) is also common with higher estimates in low- and middle-income countries. 2
Perinatal depression (PND) is one of the most common medical complications during pregnancy and the postpartum period, affecting one in seven women. 1 In research contexts, the postpartum period is less rigidly defined, with the WHO classifying PND as occurring during pregnancy or within the 12 months following delivery. 2 ICD-10 (F53) and ICD-11 (6E2) categories deal with mental and behavioral disorders associated with the puerperium (commencing within six weeks of delivery). PND often goes unrecognized because changes in sleep, appetite, and libido are attributed to changes normal in pregnancy and postpartum. Hence, clinicians may miss such symptoms, and mothers may be reluctant to report changes in their mood. Untreated PND and other mood disorders can have devastating effects on women, infants, and families.3, 4
According to DSM 5 diagnostic guidelines, to diagnose PND, there should be at least two weeks of either depressed mood or loss of interest or pleasure in nearly all activities, with at least five additional minor symptoms, “with peripartum onset.” 5 The optimal time to screen for PPD is between 2 weeks and six months after delivery. 6
PND has been associated with lower quality interactions between mothers and children, missed pediatric appointments, greater use of emergency services, higher levels of psychiatric disturbances among children, and greater child insecurity in attachment relationships.7, 8
Even though, in most cases, the mother’s PND had remitted by around 6-8 months postpartum, children continue to have an insecure attachment, behavior problems, and poorer cognitive outcomes up to 18 months.9-13 In the STAR*D study, the risk of offspring depression increased markedly with both the chronicity and severity of maternal depression. 13 PND has a negative impact on infant development and mother–child interactions, including touching, smiling, and vocalizations, and increases the risk of being underweight.14-16 Low socio-economic status, being a single mother, poor social support, general life stress, unwanted and unplanned pregnancies, stress in relationship with the partner, gender of the child, previous stillbirth, miscarriage, and premenstrual dysphoric disorder have been associated with PND.17-21
The global prevalence of PPD is 100–150 per 1000 births, and the overall pooled estimate of the prevalence of PPD in Indian mothers is 22%.
18
There is a very limited number of prospective studies on Indian population that have included periodical assessments from the early antenatal period, for estimating the various risk factors. The objectives of this study were:
To estimate the prevalence of PND by the end of the I, II, and III trimesters and first and sixth week of the postpartum period. To estimate the association of sociodemographic factors, psychosocial stressors, and obstetric and neonatal factors with PND.
Material and Methods
This prospective follow-up study enrolled all pregnant mothers who completed the first trimester, attending the Obstetrics and Gynecology (OG) outpatient department of PSG Institute of Medical Sciences and Research, a tertiary care medical college hospital in Coimbatore. Considering the prevalence of PND as 10%, 18 with a confidence interval of 95% and additional 20% attrition rate, we arrived at a sample size of 166. Institutional Ethical Committee clearance was obtained. As there is no rigid definition for the postpartum period, we took six weeks postpartum as per ICD-10. We primed our OG department faculties regarding PND, the need for assessments, and the study design. Participants were recruited by convenient sampling during the study period, January 2019 to June 2020. A postgraduate trainee in psychiatry, trained in administering the Clinician-rated Hamilton Depression Rating Scale—17 items (HAMD-17), visited the OG outpatient department and recruited all pregnant women who gave consent and fulfilled our inclusion and exclusion criteria and followed them up until six weeks postpartum.
All women aged 18 years and above who had confirmed intrauterine pregnancy by USG and could understand Tamil or English were recruited. We excluded women who were physically unwell due to acute medical complications or had cognitive deficits or mental retardation.
Baseline sociodemographic profile and psychosocial, obstetric, peripartum, and neonatal factors were recorded by semi-structured questionnaire (Figure 1). These factors were chosen based on the literature review,18,22 and we adopted a self-report method to assess them. HAMD-17 was applied by the end of the first trimester, during second and third trimester, end first week of postpartum, and end of sixth week of postpartum. An HAMD-17 item score of 8–16 is considered mild depression, 17–23 as moderate depression, and > 23 as severe depression. All who scored ≥8 were referred to psychiatric OPD for further evaluation and treatment after informing their primary therapist, with the consent of the patient and caregivers.
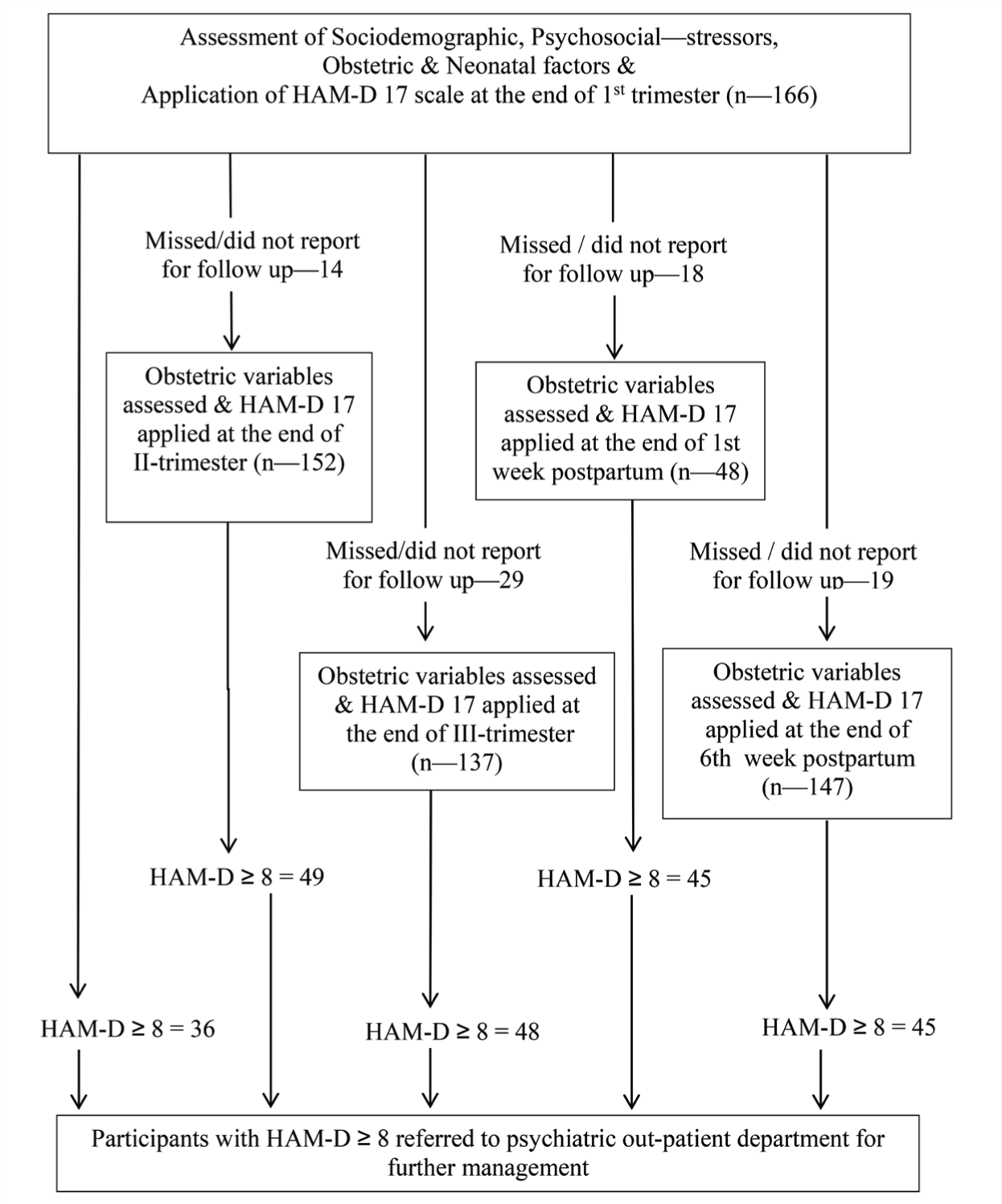
HAM-D 17: Hamilton Depression Rating Scale (17 items).
Data analysis was done using SPSS 21 version. Prevalence rates of PND by the end of each trimester, first week, and sixth week of the postpartum period were calculated by descriptive statistics. The statistical significance of various variables was assessed by the chi-square test and their odds ratio was calculated for each timeline of assessment. P value <0.05 was considered statistically significant. These analyses are purely exploratory.
Results
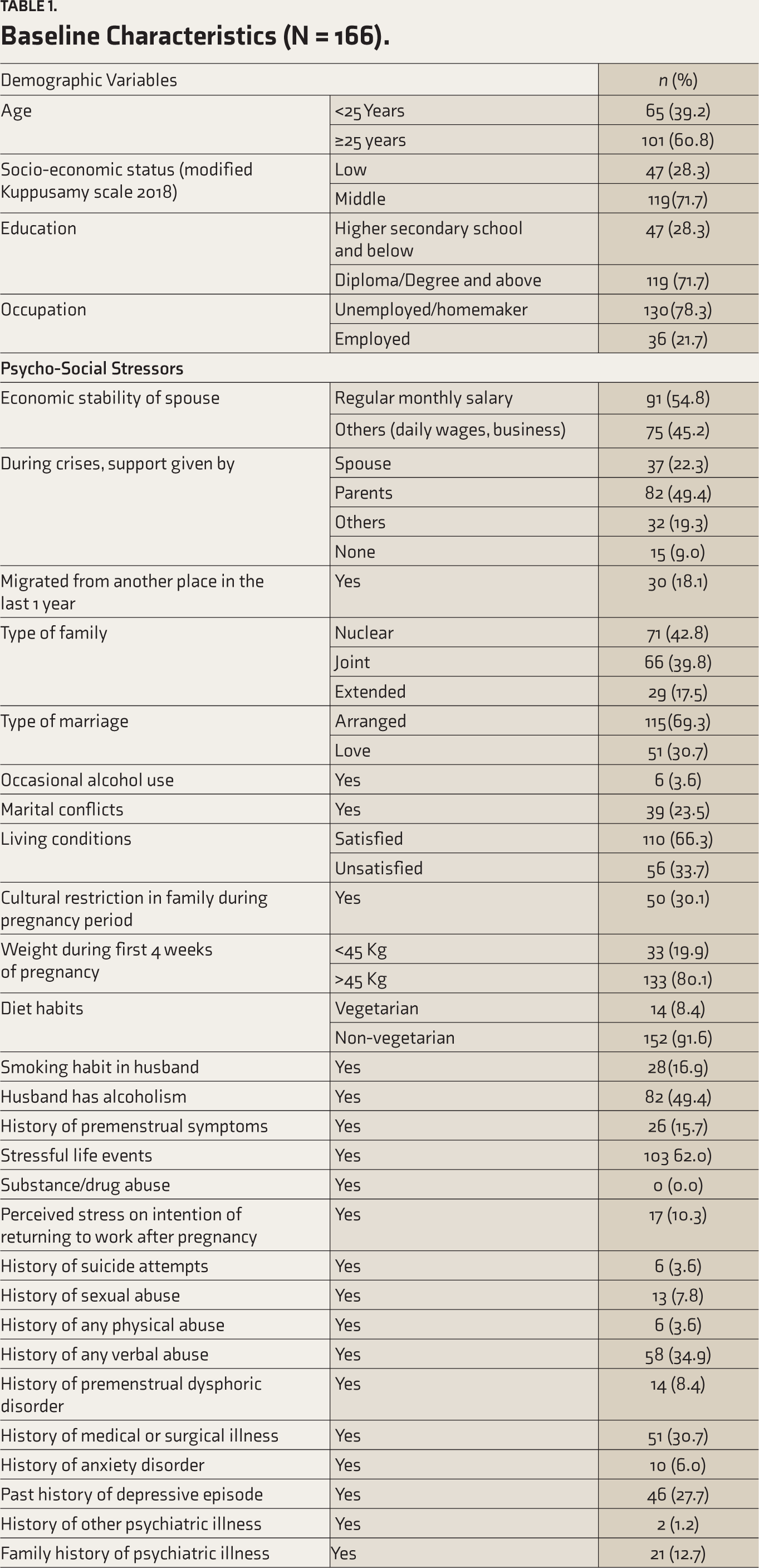
Of the 166 participants, 60.8% were ≥ 25 years, 71.7% belonged to middle socio-economic status, 71.7% were diploma/degree holders, and 78.3% were unemployed/homemakers (Table 1).
Altogether, only eight mothers among those with depressive episodes showed willingness for consultation at Psychiatry OPD for further treatment. All participants, irrespective of their willingness for treatment, were included in the further follow-up and assessed using the HAMD-17.
Regarding the psychosocial stressors (Table 1), 45.2% of the participants were not regularly salaried; 9% had no one to support them during a crisis; 33.7% had unsatisfying living conditions; 30.1% had cultural restrictions in food, travel, and exercise during pregnancy; 19.9% were underweight during their conception; 16.9% and 49.4% reported their husband had a smoking habit and alcohol use, respectively; 23.5% had ongoing marital conflicts; 62% had experienced a stressful life event in recent one year; 27.7% had past history of depressive episode; 3.6% had past history of suicidal attempts; 7.8% reported they were sexually abused, and 34.9% and 3% had experienced verbal and physical abuse, respectively, at the time of recruitment.
Regarding the distribution of obstetric factors, 46.4% were primi, 16.9% had history of infertility, 30.1% had history of high-risk pregnancy, 18.5% were not satisfied with the sex of the previous child, 36.6% have had miscarriages, and 23.7% had experienced stressful life events in their postpartum period (Table 1).The present pregnancy was unplanned in 23.5%; 41.2% reported excess fear of labor; 63.3% currently had complications including hypothyroidism, subclinical hypothyroidism, gestational diabetes mellitus, pregnancy induced hypertension, oligohydramnios, anemia, etc.; 40.5% had caesarean section, and 20.9% traumatic experience like postpartum hemorrhage and sepsis.
Baseline Characteristics (N = 166).
Four mothers had intra uterine death in the present pregnancy, 22.1% of the newborns had low birth weight, 20.5% had neonatal complications, 28.8% required neonatal ICU admissions, 45.1% had breastfeeding difficulties, and 14.6% of mothers were not satisfied by the sex of the newborn. Prevalence of depressive symptoms increased from the first to third trimester, and then there was a slight declining trend during the first and sixth week postpartum (Table 2). Most of them had only mild depressive symptoms, the prevalence of mild depression was 21.1%, 29.6%, 34.3%, 25.6%, and 27.2% at the end of the first trimester, during second, the third trimester, and first, and sixth week of postpartum, respectively. None of them had severe depression. The attrition rates ranged 8% –17% during the follow-up period, the maximum being at the third-trimester follow-up.
Prevalence Rates of Perinatal Depression.
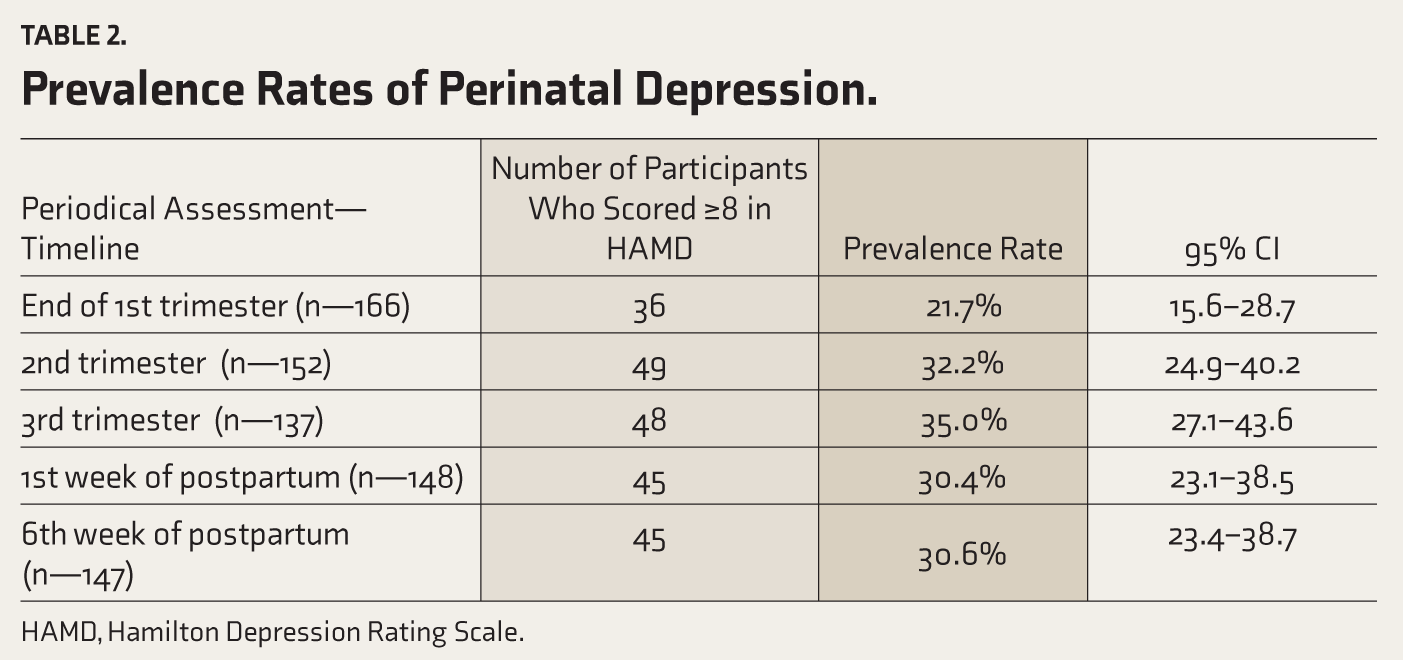
HAMD, Hamilton Depression Rating Scale.
Among psycho-social stressors, alcohol use in husband (P: 0.049, OR—2.01, CI—1.1-4.11), history of medical/surgical illness (P: 0.031, OR—2.25, CI—1.07-4.74), stressful life events (P: 0.005, O—3.16, CI—1.3-7.23), history of depressive episodes (P: 0.049, OR—2.09, CI—1.1-4.46), and history of any physical abuse (P: 0.029, OR—9.76, CI—1.06-89.94) were significant (Table 3).
Association between Risk Factors and Presence of Depression (Postpartum Period).
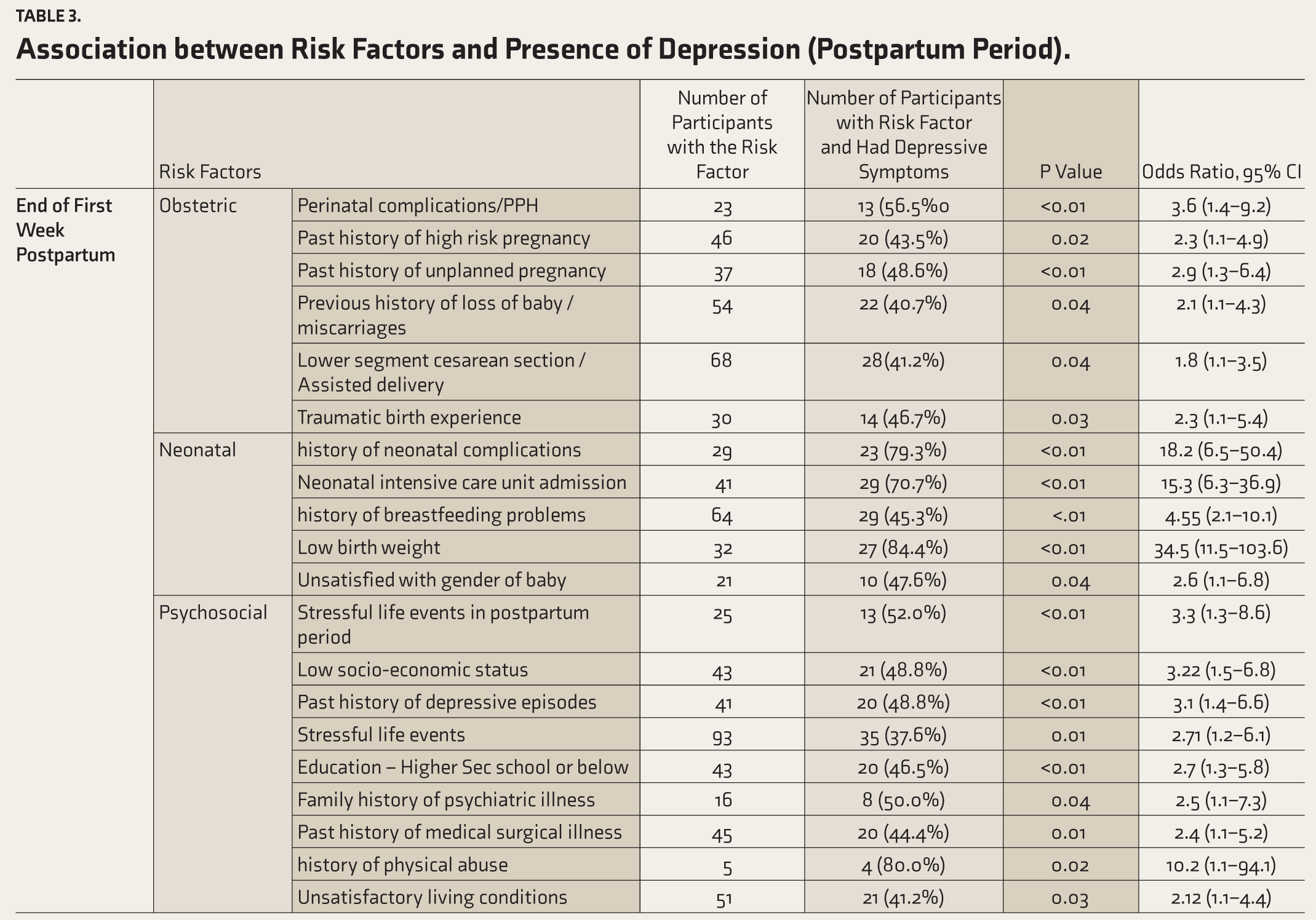
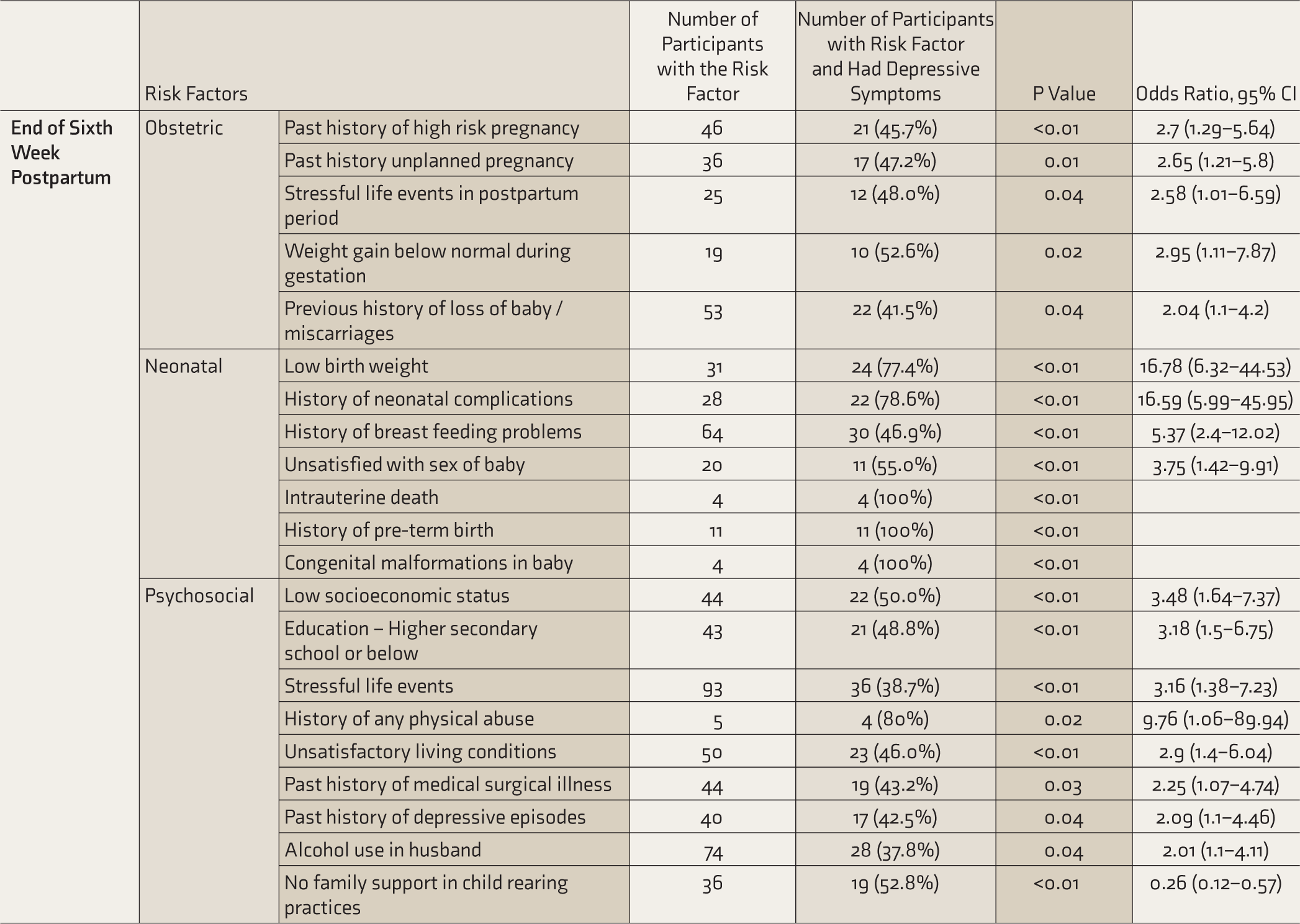
Among obstetric factors, below-normal weight gain (P: 0.026, OR—2.95, CI—1.11-7.87), history of high-risk pregnancy (P: 0.008, OR—2.7, CI—1.29-5.64), history of miscarriages (P: 0.049, OR—2.04, CI—1.1-4.2), stressful events in the postpartum period (P: 0.043, OR—2.58, CI—1.01-6.59), and Lower segment cesarean section/assisted delivery (P: 0.041, OR—1.87, CI—1.1-3.5) were significantly associated with depression at sixth week postpartum.
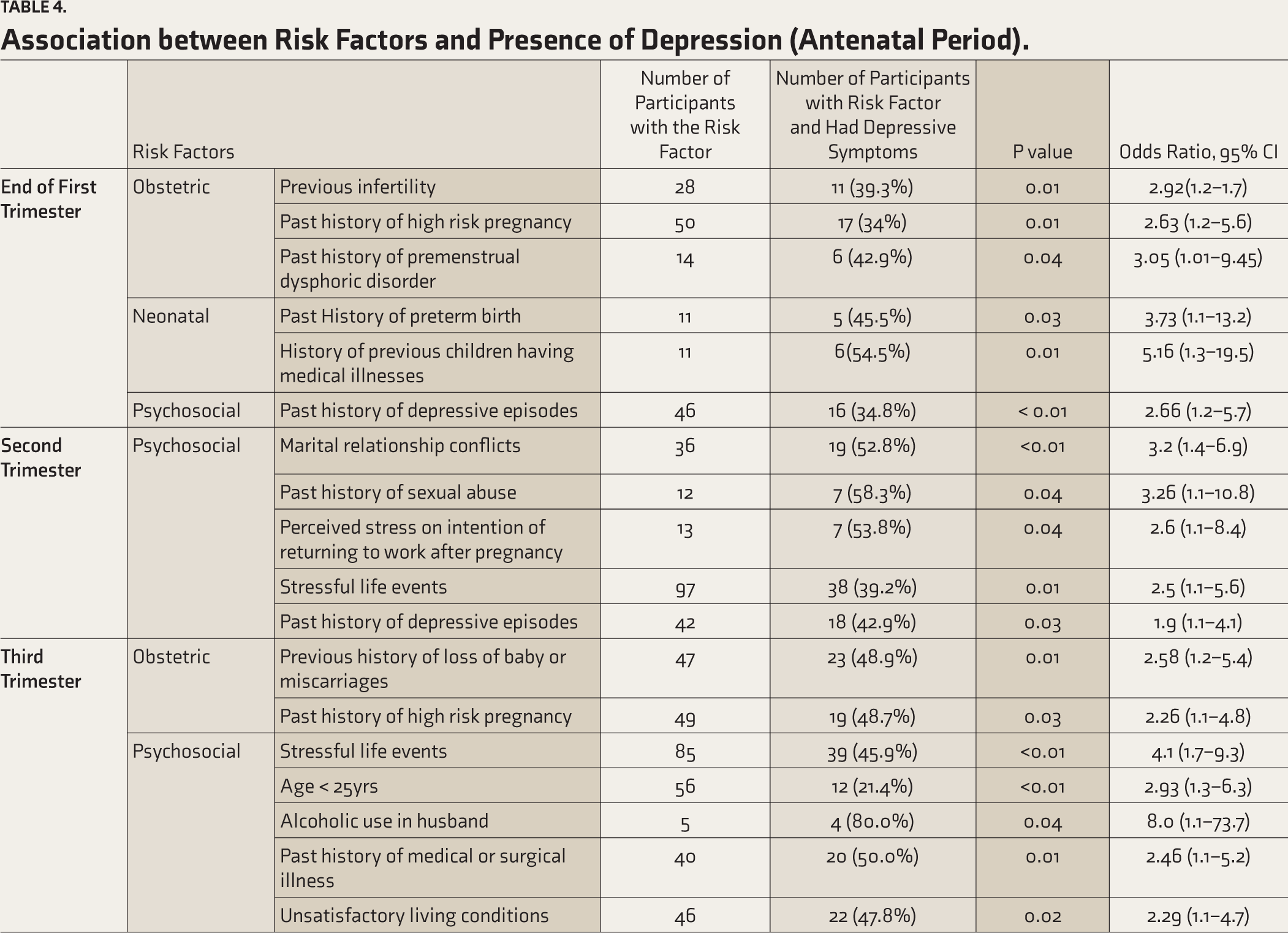
Among neonatal factors, IUD (P: 0.001), preterm birth (P: 0.001), congenital malformations (P: 0.001), NICU admissions (P: 0.001, OR—13.84, CI—5.8-33.04), history of breast feeding difficulties (P: 0.001, OR—5.37, CI—2.4-12.02), dissatisfaction with the sex of the child (P: 0.005, OR—3.75, CI—1.42-9.91), poor family support in child rearing (P: 0.001), and low birth weight (P: 0.001, OR—16.78, CI—6.32-44.53) were significantly associated with depression at sixth week postpartum (Table 3). Having a child with medical illness and a history of preterm birth seems to be the major risk factor for PND with OR of 5.16 and 3.73, respectively (Table 4). These analyses are purely exploratory.
Association between Risk Factors and Presence of Depression (Antenatal Period).
Discussion
This study estimated the periodic prevalence of PND at various time points from the early antenatal period onwards, which is the first of its kind. The prevalence ranged 21.7%–35%; a similar range was seen in the pooled prevalence of one study. 17
Assessing the association between various factors and depression in the different phases of pregnancy gives us some idea regarding the role played by these factors in the development and maintenance of depression in a given individual, and knowledge about these factors can help the treating clinicians in deciding the more individualized treatment plan.
In this study, we preferred HAMD over other self-rated scales like Beck’s depression inventory and Edinburgh postnatal depression scale because the learning effect is less with the HAMD than with self-rated scales, when applied repeatedly during follow-ups, as shown by Ji et al. 23 The first visit versus follow-up visit cut points for the HAMD only varied by 0–1 points, but the BDI and EPDS first versus follow-up visit cut points differed by 6 and 4 points, respectively. This apparent post-first visit learning effect has significant implications for the use of these self-report depression rating scales in longitudinal studies across the perinatal period, suggesting that the HAMD may be preferred for longitudinal investigations and BDI and EPDS may be preferred for cross-sectional studies. 23
The prevalence of perinatal depressive symptoms increased till third trimester; later, there was a slight decline. Similar to previous studies, among various factors past history of depression was a moderate–strong predictor of PND.21,24
In a study, 19 stressful life event was significantly associated with developing PPD. Our study replicated this finding from second trimester onwards.
Receiving social support (informational, instrumental, and emotional) through friends and relatives during stressful times is thought to be a protective factor against developing depression. In our study, lack of family support in child rearing was significant during the postpartum period.
A meta-analysis showed that neonatal factors like LBW and preterm delivery are consistently associated with PND. 24 Vigod et al. found that mothers of premature infants are 40% more likely to develop PPD than the general population. 25 Literature examining psychological maladjustment in mothers of infants admitted to the NICU reports that these women have consistently higher rates of PPD, ranging 28%–70%, compared with mothers of healthy term infants not in the NICU. 26 The present study also showed the presence of feed-ing difficulties and neonatal intensive care unit admissions are strongly associated with depressive symptoms in the first and sixth week of postpartum, which is similar to earlier studies. 18 Mothers of babies with neonatal complications should be considered vulnerable and must be evaluated for depression.
Past depressive episodes, sexual abuse, and physical abuse were consistently associated with depression during pregnancy; these are independent risk factors for depression in any individual. Hence the presence of these factors in pregnant women should caution us about the possibility of underlying depression.
It is possible that in an otherwise normal nonvulnerable pregnant woman, socio-economic difficulties at the beginning can make one apprehensive about the difficulty they might face by an additional member entering into the family, and worries about raising the child and its future may predispose one to develop depression in the early phase. During the pregnancy, obstetric complications and anxiety about labor and delivery outcome might add to the above factors, thereby increasing the risk of developing depression, especially during the later stages of pregnancy. During the postpartum period, probably, neonatal risk factors and lack of family support in rearing the child may play a major role in predisposing the mother to develop depressive symptoms.
Altogether, only eight patients among those diagnosed to have depressive symptoms were willing for psychiatric treatment, including medications. Most of them who had depression avoided psychiatric consultations due to various reasons like social stigma. In India, very often, during pregnancy, the decisions are not taken by the pregnant woman or her husband; it is her in-laws and extended family members who take decisions; this might prevent pregnant women from seeking psychiatric help. The other possible reasons are lack of awareness and poor insight; people ignore the psychosocial stressors and difficulties these individuals face as part and parcel of life that do not need a psychiatric evaluation.
Though evidence exists for the negative effects of maternal depression on the emotional, behavioral, cognitive, and interpersonal development of young children, such effects appear to be time-limited; however, prolonged or recurrent episodes of maternal depression appear to be more likely to cause long-term effects on children. 27 The potential adverse effects of PND on the maternal–infant relationship and child development reinforce the need for early identification and effective treatment models.
Although there is no archetypal model for a woman at risk, identifying the risk factors helps to prevent and manage PND. The long-term consequences of PND suggest a need for preventive approaches. However, translating risk factor research into predictive screening protocols and preventive interventions has limited success, as complex interactions of bio-psycho-social risk factors with individual variations must be contemplated. This recommends the need for multi-centered cohort study with large representative samples to determine the causal factors and to compare different treatment modalities and their effectiveness.
A multidisciplinary approach involving obstetricians and pediatricians is needed to create awareness and clear misconceptions about PND. Steps need to be taken in the policy and practice of maternal and child health care programs related to prevention, early detection, optimal treatment, and amelioration of the effects of PND.
Given the magnitude of mental health issues in pregnant women and their impact on developing children, it is imperative to include mental health screening as part of the obstetric evaluation. Establishing a Perinatal Psychiatric Unit within the OG outpatient department where mental health profess-ionals can work as a team along with obstetricians, providing handouts about depression and mental health issues, and including supervised psychiatric training for OG students as a part of their postgraduate curriculum are steps that can be initiated to improve mental health in pregnant women.
The strengths of our study are we were able to recruit a decent number of pregnant women and evaluate them for depression and other possible risk factors from the first trimester onwards, and the prospective follow-up of these participants in different stages of their pregnancy until six weeks postpartum, with only a minimal attrition rate. This study attempted to find the possible risk factors, the pattern of change of risk factors throughout pregnancy and postpartum, and their impact on maternal well-being. The present study has some limitations: it was conducted in a single, tertiary care center, and hence, the findings cannot be generalized to the community. It was conducted in a private hospital setup; the sociodemographic profile of pregnant women described here could differ from that of a government hospital setup. One could imagine that those consulting in government setups can have varying psychosocial stressors and the prevalence of those stressors, and the impact of those factors on their mental health, could be different. We adopted a convenient sampling method purely due to practical constraints; it was not possible to visit OG OPD daily to recruit participants, but random or consecutive sampling could have been better. We did not use objective measures or standardized and validated instruments to rate the quality of relationships with significant others or to elicit adverse life events. Using a self-report method to assess some of the risk factors is not as reliable as other methods. Using HAMD to assess depression could have overestimated the prevalence of depression due to its potential overlap with normal physical complaints related to pregnancy and childbirth. However, it is noteworthy that the specificities of the other scales, including BDI and EPDS, were uniformly lower during pregnancy and the early postpartum period than during the preconception period. The earlier-mentioned study on the validity of different scales for PND had found that the pregnancy cut-off points are the same or lower than the preconception cut-off points, suggesting that women incorporate their own opinions regarding the etiology of the symptoms during both interviews and completion of self-rated scales. 23 We only assessed the presence or absence of depressive symptoms. We did not specifically analyze how many had mild, moderate, or severe depression in each assessment. The possibility of bias while rating on the depression scale could not be ruled out. A longer follow-up study including one year post-partum would be more creditable. Establishing a causal association was not done.
To conclude, the prevalence of depressive symptoms is high right from the early antenatal period. Antenatal mothers with various obstetric factors, including bad obstetric history, neonatal factors including neonatal complications, psychosocial factors including stressful life events or marital conflicts, with significant past history, warrant an evaluation of PND for early intervention and appropriate management, to improve the mental health of mother and child.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.