
Abstract
Background:
Internalized stigma experienced by individuals with schizophrenia and bipolar affective disorder dramatically affects their overall quality of life. While several studies have explored this topic, there remains a scarcity of research comparing internalized stigma across both these illnesses. We investigated and compared how internalized stigma is associated with different socio-demographic factors among individuals diagnosed with schizophrenia and bipolar affective disorder in remission. This was a comparative study of the internalized stigma experienced by patients with schizophrenia and bipolar affective disorder in remission.
Methods:
A total of 106 patients with schizophrenia and 53 with bipolar affective disorder (BPAD) in remission underwent assessment using the Internalized Stigma of Mental Illness Scale (ISMIS), Positive and Negative Syndrome Scale (PANSS), and Young Mania Rating Scale (YMRS).
Results:
The study revealed that internalized stigma was significantly more (p value = .0001) in patients with schizophrenia (84.84 ± 6.02) compared to those with BPAD (78.55 ± 6.07). Further analysis of the ISMIS domains revealed significant correlations between internalized stigma and stereotype endorsement (p value = .005), stigma resistance (p value = .009), social withdrawal (p value = .0001), and alienation (p value = .0001).
Conclusion:
The study suggests that individuals with schizophrenia experience higher levels of internalized stigma in comparison to those with BPAD.
Internalized stigma was more common in patients with schizophrenia as compared to those with bipolar affective disorder. This study emphasizes the importance of stigma reduction strategies in comprehensive care.Key Messages:
Schizophrenia is a chronic mental disorder that substantially interferes with various aspects of individuals’ social, educational, and professional functioning. This condition typically emerges during adolescence or early adulthood, affecting a considerable portion of the global population, with an annual incidence ranging from 1% to 7.5%. 1
The pervasive stigmatization of individuals grappling with mental illnesses, including schizophrenia, is a distressing reality. 2 Those with schizophrenia frequently bear the brunt of public prejudices, leading them to internalize disparaging beliefs about their group, which often culminates in self-stigmatization. 3 Since stigma is closely linked to a diminished quality of life, it can be broadly categorized into personal and public stigma.4,5
Personal stigma, characterized by low self-esteem, reduced self-efficacy, and diminished self-confidence, hampers the recovery process for individuals with schizophrenia. Furthermore, it constrains their societal roles, exacerbates social exclusion, and impedes social integration. 6 Individuals grappling with mental health issues face various dimensions of stigma, impacting their self-worth and restricting their access to social opportunities. This may manifest in employment or housing rejections due to their mental health condition. 7 Stigma gives rise to discrimination, segregation, and a perceived erosion of autonomy and self-efficacy.8–10
When an individual experiences or anticipates adverse reactions due to potentially stigmatizing characteristics, it indicates an internalized stigma. This can lead to maladaptive behaviors and a shift in self-perception. 3 Patients often express apprehension about encountering prejudice and exclusion due to their mental illness. 11 Moreover, bipolar affective disorder (BPAD) patients during manic episodes are also confronted with significant stigma. 12 Discrimination against individuals with BPAD is prevalent in workplaces and healthcare settings, impeding their ability to pursue education, manage finances, and cultivate meaningful interpersonal relationships.
The objectives of our study were: (a) to assess and compare the levels of internalized stigma in patients diagnosed with schizophrenia and BPAD in remission and (b) to explore the correlation between internalized stigma in individuals with sand BPAD and a range of socio-demographic and clinical factors.
Methods
This was a hospital-based, observational, descriptive, cross-sectional study conducted at the psychiatry outpatient department in a tertiary healthcare facility in rural central India. Convenient sampling methods were utilized after receiving approval from the institutional ethics committee, and written informed consent was acquired from all participants. The study was conducted between January 2021 and June 2022.
The study included patients who were in the remission phase, as per the Andreasen criteria for schizophrenia, symptomatic remission, and maintenance over six months of simultaneous rating of a score less than 3 on items of delusions, unusual thought content, hallucinatory behavior, conceptual disorganization, mannerism, blunted affect, social withdrawal, and lack of spontaneity in the Positive and Negative Syndrome Scale (PANSS) 13 and had Young Mania Rating Scale (YMRS) scores below 12 for BPAD. Participants were aged between 18 and 60 years. Those with co-existing psychiatric or physical conditions and those unwilling to provide consent were excluded from the study. The study included patients who had comorbid tobacco use.
Tools
Young Mania Rating Scale 14
The YMRS is a widely used 11-item scale designed to evaluate manic symptoms that was developed by Young et al. in 1978. It relies on the patient’s subjective-reported assessment of their clinical condition over the preceding 48 hours. Four items (irritability, speech, thought content, and disruptive/aggressive behavior) are rated on a scale from 0 to 8, while the remaining seven are rated from 0 to 4. The total score ranges from 0 to 60. The scale has a reliability of 0.93 and a validity of 0.88.
Positive and Negative Syndrome Scale 15
The PANSS is a 30-item questionnaire created by Kay, Fiszbein, and Opler in 1987, aimed at evaluating positive, negative (7 questions each), and general psychopathology symptoms (16 questions) in individuals diagnosed with schizophrenia. Symptoms are assessed based on severity, ranging from 1 (absent) to 7 (severe). Administering the scale typically takes around 35 minutes. The reliability of the scale is reported to be 0.80.
Internalized Stigma Mental Illness Scale 16
The ISMIS was developed in 2004 by Ritsher and Phelan and is designed to measure internalized stigma experienced by individuals with a mental illness. It consists of 29 items, each rated on a scale of 1 to 4, with higher scores reflecting greater stigma. The scale assesses various aspects of internalized stigma, including alienation, stereotype endorsement, perceived discrimination, social withdrawal, and stigma resistance. Scores below 2 indicate no stigma, scores between 2 and 2.5 suggest low stigma, scores between 2.5 and 3 indicate moderate stigma, and scores above 3 indicate a high level of stigma.
The statistical analysis involved descriptive and inferential methods, including the chi-square test, Student’s unpaired t-test, Pearson’s correlation coefficient, and regression analysis. The analysis of data was done using SPSS version 27.0.
Results
The study found that a significant proportion of patients diagnosed with schizophrenia were in the age range of 40–49 years, whereas individuals with BPAD were predominantly aged between 30 and 39 years. The gender distribution in the schizophrenia group consisted of 51% females and 49% males, whereas in the BPAD group, 60.38% were males and 39.62% were females. In the schizophrenia group, 20.75% had no formal education, and 28.30% had completed primary school, whereas in the BPAD group, the majority had completed secondary school (28.30%), followed by higher secondary education (22.64%). More patients in the schizophrenia group were unemployed (31.13%) compared to the BPAD group (13.21%). Regarding religion, the schizophrenia group had 58.45% of patients belonging to the Hindu religion, compared to 54.72% in the BPAD group. The married population represented 43.40% of schizophrenia patients and 49.06% of those with BPAD. A positive family history of psychiatric illness was found in 15.9% of schizophrenia cases and 9.48% of BPAD cases, as indicated in Table 1.
Socio-demographic Variables of the Study Population.
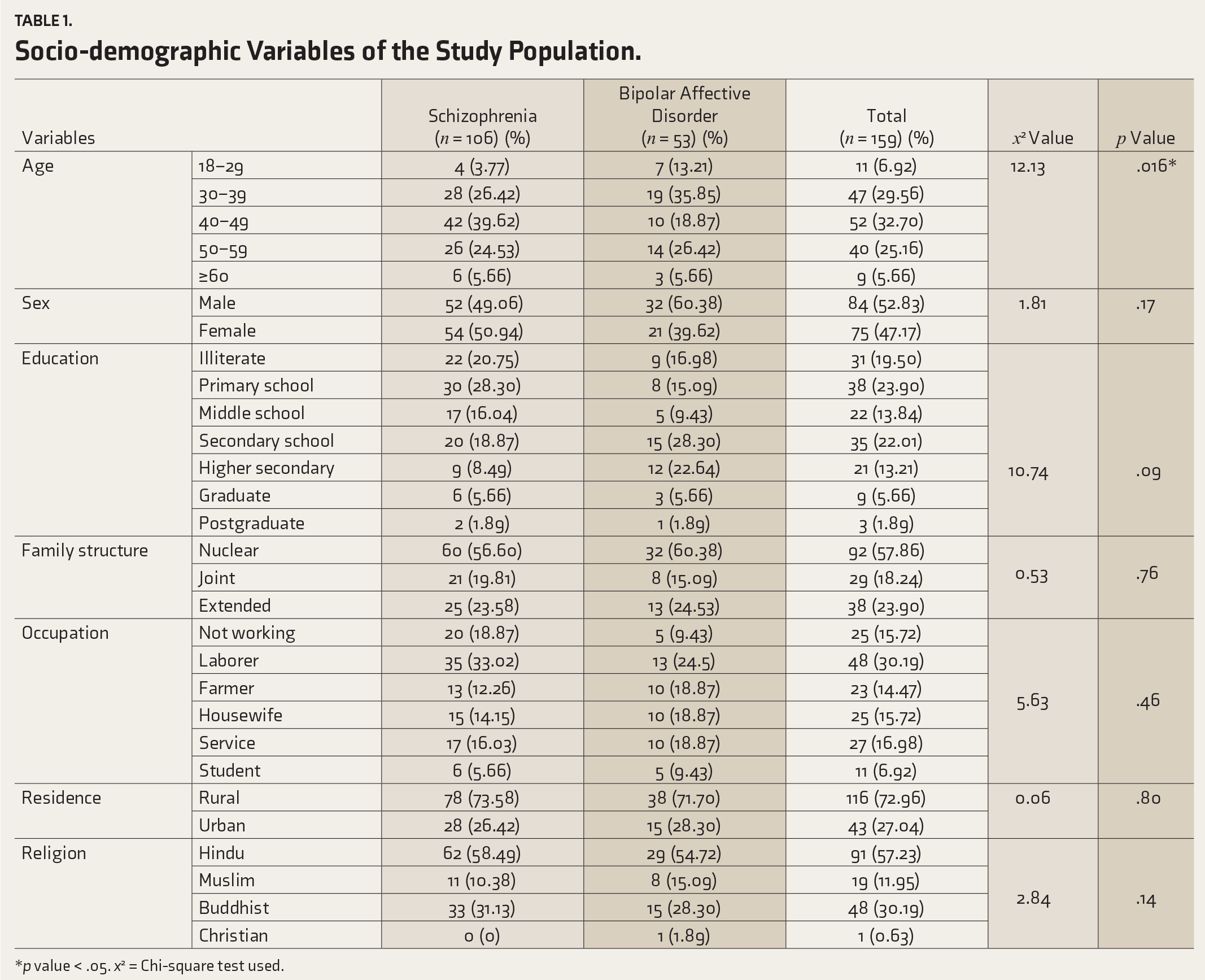
*p value < .05. x2 = Chi-square test used.
Regarding the ISMIS scores, schizophrenia patients had an average score of 84.84 ± 6.02, whereas for BPAD patients, the score was 78.55 ± 7.59. This discrepancy was statistically significant in both groups (p value = .0001). Table 2 presents the comparison of ISMIS scores between schizophrenia and BPAD patients, demonstrating a notably higher mean score in the schizophrenia group (p value = .0001).
Comparison of Internalized Stigma Mental Illness Scale Score in Schizophrenia and Bipolar Affective Disorder Groups.
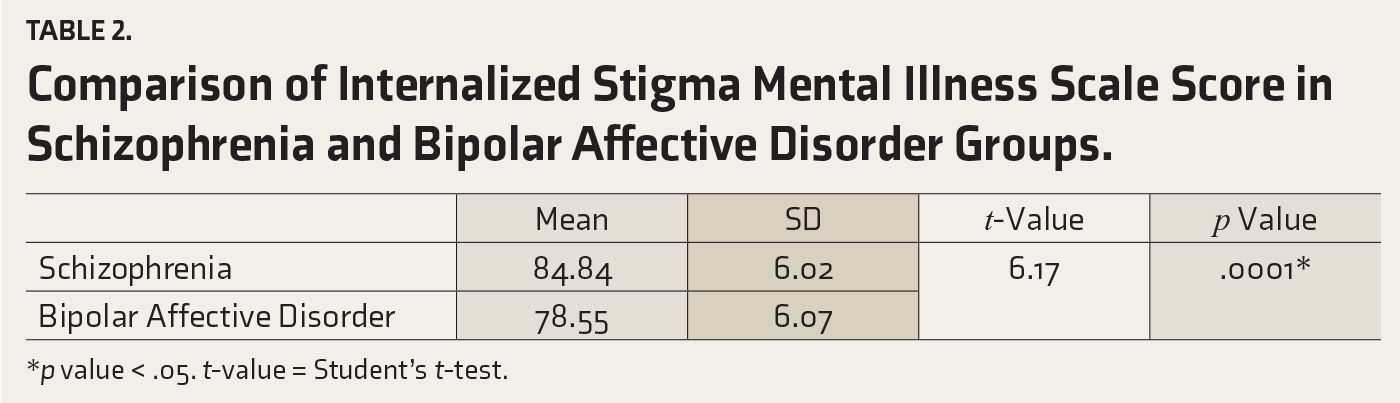
*p value < .05. t-value = Student’s t-test.
The average scores for stigma among individuals with schizophrenia, as assessed across the five subcategories of the ISMIS, were as follows: stigma resistance (9.66 ± 1.72), social withdrawal (14.60 ± 2), discrimination experience (15.35 ± 1.8), stereotype endorsement (23.07 ± 1.68), and alienation (22.56 ± 2.85). In contrast, the mean scores for the BPAD group were 8.89 ± 1.80, 11.80 ± 2.59, 14.94 ± 1.79, 22.05 ± 2.32, and 20.47 ± 3.19, respectively. These scores were significantly higher in the schizophrenia group, with a p value < .05 in all categories.
Further examination of the ISMI subscale scores in the schizophrenia and BPAD groups revealed a statistically significant difference in stigma resistance (r = 2.65, p value = .009) between the two cohorts. However, no significant correlation was found for discrimination endorsement (r = 1.35, p value = .17) between these groups. Conversely, the other four subscale scores demonstrated significant correlations: social withdrawal (r = 6.64, p value = .0001), social resistance (r = 2.60, p value = .005), stereotype endorsement (r = 2.83, p value = .005), and alienation (r = 4.03, p value = .0001). Table 3 outlines the statistically significant disparities in ISMI subscale scores between schizophrenia and BPAD patients for stigma resistance (p value = .009), social withdrawal (p value = .0001), stereotype endorsement (p value = .005), and alienation (p value = .0001).
Comparison of Subscales of Internalized Stigma Mental Illness Scale score in Schizophrenia and Bipolar Affective Disorder.
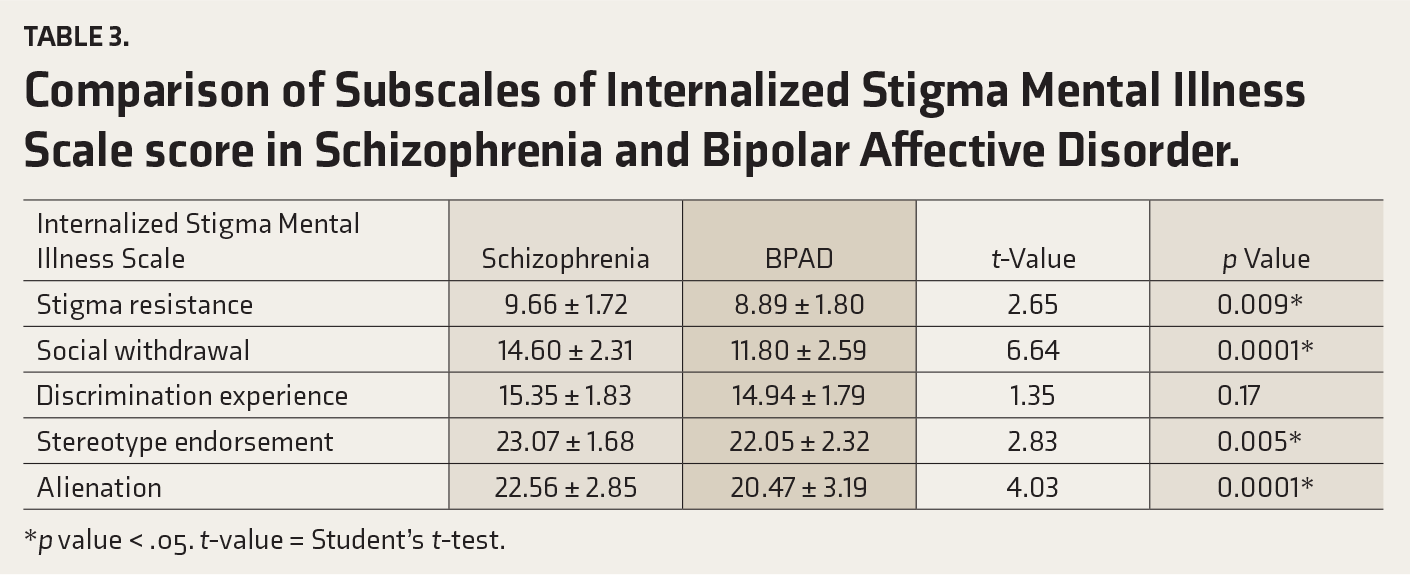
*p value < .05. t-value = Student’s t-test.
Table 4 illustrates the relationship between ISMIS scores and demographic factors among patients diagnosed with schizophrenia and BPAD in remission. Notably, individuals with BPAD displayed a statistically significant correlation between their level of education and ISMIS score (p value = .0001).
Correlation Between Internalized Stigma Mental Illness Scale and Demographic Variables in Schizophrenia and Bipolar Affective Disorder Patients.
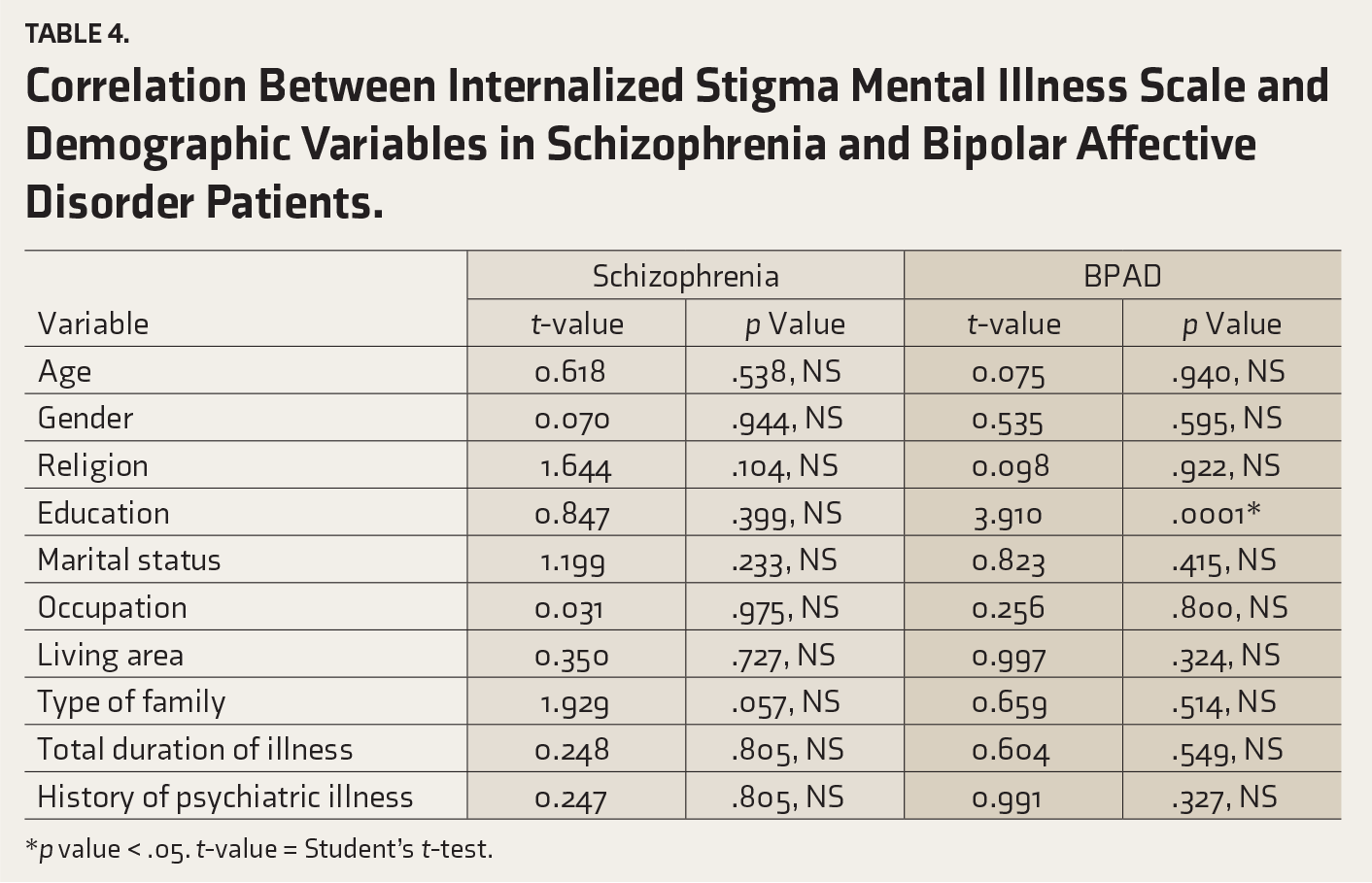
*p value < .05. t-value = Student’s t-test.
Discussion
In this article, we delved into the key findings of our study on internalized stigma in patients with schizophrenia and BPAD in remission while drawing comparisons with previous research.
In the current study, out of a total sample size of 159 individuals, 53 patients (33.33%) had BPAD and 106 patients (66.67%) had schizophrenia. Other studies had more participants as their study was multicenter, which could be the reason for this difference. Other epidemiological studies have consistently used larger sample sizes but do not directly compare the two disorders.
Age Distribution
Our research findings indicate that a significant portion of schizophrenia patients were between the ages of 40 and 49 years, while BPAD tended to affect individuals aged 30–39 years. These age patterns correspond to the expected onset periods for these disorders, as observed in prior studies conducted by Ramachandran et al. and Karidi et al.17,18
The BPAD patients who were in symptomatic remission were also taken into consideration in the study. Our schizophrenia patients were in remission with long-term regular follow-up.
Gender Difference
In the schizophrenia group, there was a nearly equal distribution between genders, with 51% female patients and 49% male patients. Conversely, the BPAD group showed a higher prevalence of males (60.38%) than females (39.62%). This gender imbalance aligns with findings reported in earlier studies conducted by Aakanksha Singh et al. and Kumar et al., suggesting potential differences in prevalence rates across genders in various psychiatric disorders.19,20
Education
The educational levels varied, with 20.75% of schizophrenia patients being illiterate and 28.30% having completed primary school. Conversely, most BPAD patients had attained secondary education (28.30%), followed by higher secondary (22.64%). These results are in line with the findings of Karambelkar et al., which also highlighted disparities in educational backgrounds between the two groups of patients. 20 Education has a significant impact on psychiatric disorders. Increased levels of literacy are linked to lower probabilities of affective disorder occurrence.
Increased education has a higher likelihood of receiving psychoeducation, psychotherapy, and a reduced risk for mandatory IPD care were all connected with affective illness.
Stigma Scores
The mean ISMIS score in the schizophrenia group was 84.84 ± 6.02, significantly higher than that of BPAD patients, who scored 78.55 ± 7.59 (p value = .0001). These results concur with Grover et al. and Kumar et al., indicating that schizophrenia patients tend to experience more severe internalized stigma compared to BPAD patients.21,22
Subscales of ISMIS
Examining the subscales of the ISMIS, we observed significant differences between the two groups. Stigma resistance, social withdrawal, discrimination experience, stereotype endorsement, and alienation were notably elevated in the schizophrenia group compared to the BPAD group (p value < .05). These findings corroborate a study by Grover et al., which reported similar trends in the mean scores of various ISMI subscales among schizophrenia patients. 23
Comparison with Other Studies
Our results were consistent with research by Prasko et al. and Picco et al., highlighting the variation in self-stigma levels between BPAD and schizophrenia patients.24,25 Additionally, we found that discrimination experience appeared to be a distinct construct, as it did not significantly correlate with other ISMIS domains, in agreement with Grover et al. 26
Significant Correlation with Demographic Variables
Education was the only demographic variable that was significantly correlated with the ISMIS in the BPAD group (p value = .0001).
These results are consistent with the conclusions drawn by Chen et al., who linked lower rates of manic disorders with higher levels of education. 29 Nonetheless, in the schizophrenia group, only age demonstrated a notable correlation (p value = .012).
In summary, our study highlights that individuals diagnosed with schizophrenia typically encounter more significant levels of internalized stigma compared to those with BPAD. This emphasizes implementing targeted interventions to address stigma within both patient cohorts. Specifically, among individuals diagnosed with schizophrenia, our research identifies notably heightened stigma across certain domains, including alienation, social withdrawal, stereotype endorsement, and stigma resistance. Notably, discrimination experience does not exhibit a similar association with schizophrenia diagnosis. This insight emphasizes the importance of targeted stigma reduction interventions for individuals with schizophrenia and BPAD. Internalized stigma is closely linked to higher disability levels and poorer functioning among individuals with mental health conditions. Therefore, incorporating stigma reduction interventions as an integral part of the management of schizophrenia and BPAD is paramount. By addressing stigma, we can potentially mitigate the impact of these conditions on individuals’ lives, fostering improved functioning and overall well-being.
Strengths
This research is the first of its kind in central India, focusing on understanding the stigma faced by patients with schizophrenia and BPAD. Unlike previous studies, we looked closely at how factors such as age, gender, education, and the nature of the illness related to the stigma these patients experience. By doing this, we better understand what contributes to stigma among these individuals, which can help improve support and treatment for them in the future.
Limitations
The sample size was small, and the study was conducted in a hospital setting with a cross-sectional design, which limits the generalizability of the findings.
Conclusion
The study reaffirms the observation that individuals diagnosed with schizophrenia typically encounter elevated levels of internalized stigma in comparison to those with BPAD. These findings add to our comprehension of the variations in stigma experiences among different psychiatric disorders, emphasizing the importance of tailored interventions to address these unique challenges. Our study underscores the urgency of implementing stigma reduction strategies as part of comprehensive care for individuals with schizophrenia and BPAD. By understanding and addressing the unique challenges posed by stigma in individuals with these mental health conditions, we can improve their quality of life and functioning, leading to better overall mental health outcomes. Further research and targeted interventions in this area are essential to advance our understanding and treatment of internalized stigma in psychiatric disorders.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The Institutional Ethics Committee approved the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was acquired from all participants.