
Abstract
Background:
Only a few studies have explored the relationship between psychosocial factors and medication adherence in Indian patients with noncommunicable diseases (NCDs). We aimed to examine the association of psychosocial variables with medication adherence in people with NCDs and comorbid common mental disorders (CMDs) from primary care in rural southern India.
Methods:
We performed a secondary analysis using baseline data from a randomized controlled trial in 49 primary care health centers in rural southern India (HOPE study). Participants were adults (≥30 years) with NCDs that included hypertension, diabetes, and/or ischemic heart disease, and comorbid depression or anxiety disorders. Medication adherence was assessed by asking participants if they had missed any prescribed NCD medication in the past month. Data were collected between May 2015 and November 2018. The association between psychosocial and demographic variables and medication nonadherence were assessed via logistic regression analyses.
Results:
Of the 2486 participants enrolled, almost one-fifth (18.06%) reported missing medication. Male sex (OR = 1.74, 95% CI 1.37–2.22) and higher internalized mental illness stigma (OR = 1.46, 95% CI 1.07–2.00) were associated with higher odds of missing medication. Older age (OR = 0.40, 95% CI 0.26–0.60, for participants aged 64–75 years vs 30–44 years), reporting more social support (OR = 0.65, 95% CI 0.49–0.86), and higher satisfaction with health (OR = 0.74, 95% CI 0.61–0.89) were associated with lower odds of missing medication.
Conclusions:
Greater internalized mental illness stigma and less social support are significantly associated with lower rates of medication adherence in patients with NCDs and comorbid CMDs in rural India.
Keywords
In patients from rural primary care settings with comorbid common mental disorders, male sex, younger age, and higher internalized stigma are associated with higher odds of missing medication for noncommunicable diseases. Those who reported more social support and higher satisfaction with health had lower odds of missing medication.Key Messages:
The burden of noncommunicable diseases (NCDs) is escalating in India. 1 The Global Burden of Disease (GBD) Study estimated 23.8 million prevalent cases of Ischemic Heart Disease (IHD) in India in 2016, a 2.3 times increase from 1990, and overall, cardiovascular diseases (IHD and stroke) contributed 28.1% of the total deaths and 14.1% of the total disability-adjusted life years (DALYs). 2 The GBD also estimated that the number of people with diabetes in India increased from 26.0 million in 1990 to 65.0 million in 2016, with higher prevalence in Southern states. Besides, the age-standardized DALY rate for diabetes increased in India by 39.6% from 1990 to 2016, which was the highest increase among major NCDs. 3
Treatment adherence is a key component of NCD management. The World Health Organization (WHO) defines “adherence” as the extent to which a person’s behavior—taking medication, following a diet, and/or executing lifestyle changes—corresponds with agreed recommendations from a health-care provider. 4 The consequences of poor adherence to long-term therapies are poor health outcomes and increased health-care costs. 4 Poor medication adherence among NCD patients has been consistently associated with poor perceived overall quality of life (QOL) and poor satisfaction with health.5–8 The WHO framework on adherence to long-term therapies identifies several factors that can influence adherence, including social and economic factors, the health-care team/system, the characteristics of the disease and disease therapies, and patient-related factors. 4
There are various ways to measure medication adherence, including self-report methods (e.g., scales like the MORISKY Medication Adherence Scale and Visual Analogue Scale), electronic medication monitoring, pill count, electronic medical records, pharmacy claims, and prescription refill records. 9 Studies that employ self- report methods to measure adherence in people with multiple medical conditions typically define nonadherence as <80% to <100% of prescribed pills taken, depending on the regimen. 10 Studies from primary care settings in India have found that the proportion of NCD patients nonadherent to treatment ranges 32.7 to 75.9%.11–15
Psychosocial factors are important determinants of adherence to medications. 16 Depression has consistently been shown to be associated with poor medication adherence in patients with NCDs.17–19 There is also evidence that the treatment of depression enhances medication adherence in patients with chronic medical conditions.20,21 Social support, and more specifically functional or practical social support, was found to be positively associated with medication adherence among patients with NCDs.22–26
Studies from various settings in India have also considered the relationship between psychosocial variables and medication adherence in NCD patients. The Prevalence of Depression in Diabetes (DEPDIAB) study, a cross-sectional survey that included 1371 patients with diabetes, 27 found that those with poor medication adherence had five times higher odds of being depressed compared to patients with excellent adherence. A cross-sectional study of older adults with NCDs in primary care from rural Karnataka reported no significant association between depression and medication adherence. 11 Another cross-sectional study from rural Karnataka, which examined the association between social support and medication adherence among older adults (>60 years) suffering from chronic diseases like diabetes mellitus, hypertension, osteoarthritis, and chronic obstructive pulmonary disease, found that practical social support was significantly associated with good medication adherence. 28 A cross- sectional study conducted at a tertiary care hospital in Uttarakhand, India, reported that patients who were adherent to antidiabetic medications had significantly higher mean overall perception of QOL and overall perception of health, compared with nonadherent patients. 29
Several studies from India among people living with HIV have shown that depression and anxiety are significantly associated with nonadherence to antiretroviral therapy (ART).30–32 Studies from rural and urban settings in India among people living with HIV have found a significant positive relationship between ART adherence and social support and a negative association between ART adherence and internalized stigma.33–38
There is a paucity of studies from rural India that have studied the relationship between psychosocial factors and medication adherence in NCD patients.11,28 More specifically, there is a gap in the literature on the association between factors such as psychological distress, social support, stigma, QOL, and satisfaction with health, and medication adherence, in these patients. The objective of the present study was to examine the associations of these psychosocial variables with medication adherence in people with NCDs and comorbid common mental disorders (CMDs) from primary care in rural southern India.
Materials and Methods
Setting and Participants
The present study was part of HOPE study, a cluster-randomized controlled trial (cRCT) conducted in 49 primary health centres (PHCs), which were randomly selected, in the rural Ramnagara district of Karnataka state in southern India. 39 The trial evaluated the effects of using a collaborative care model to integrate screening and treatment of PHC patients in rural Karnataka with depression who were also diagnosed with chronic medical conditions. 40 The present study is a secondary analysis that used baseline data from the HOPE trial participants. Eligible participants were adults (≥30 years) with a diagnosis of major depressive disorder, dysthymia, generalized anxiety disorder (GAD), and/or panic disorder on the Mini- International Neuropsychiatric Interview (MINI) 41 that was untreated at the time of screening, plus comorbid medical condition(s) that included hypertension, diabetes, and IHD. No one screened had to be excluded for already being in treatment for their psychiatric condition. Data were collected between May 2015 and November 2018. Details of the trial protocol have been published previously. 39
Measures
CMD Diagnosis: MINI 41 was used to confirm the diagnosis of major depressive disorder, dysthymia, GAD, and/or panic disorder as per DSM-IV guidelines. It is a short structured diagnostic interview with an administration time of approximately 15 minutes.
Medical Treatment: Participants self- reported, due to a lack of medical charts at the PHCs, if they were taking medication for diabetes (tablets or insulin), hypertension/IHD, or dyslipidemia. Patients were not always sure about which condition they were being treated for while taking medications prescribed for hyper- tension and IHD. Additionally, several of these medications could be used to treat both conditions. Therefore, we combined these two conditions into one category. All responses were verified by having the participant present the corresponding medication container or the prescription. The number of comorbid medical conditions for which participants were on medication was constructed as the sum of being on medication (0 = no, 1 = yes) for diabetes, hypertension/IHD, and dyslipidemia, resulting in a range of 0–3.
Adherence to Medication Regimen: This was the outcome variable. It was assessed by asking the participant if they had missed any prescribed medication in the past month for diabetes, hypertension/IHD, and dyslipidemia separately. The responses were combined for all conditions for which the participant was being treated, into a dichotomous “missed medication” variable that was scored 0 if the participant took all medication as prescribed and was scored 1 if he/she missed at least one dose in the past month. We chose to capture adherence to medication in this manner as patients tend to overestimate adherence on self-reported recall of missed medications. 42
Psychological Distress: Depression was assessed using the Patient Health Questionnaire-9 (PHQ-9). 43 This widely used measure asks about the frequency of experiencing (0: “Not at all” to 3: “Nearly every day”) nine potential symptoms of depression (e.g., little interest or pleasure in doing things, thoughts that you would be better off dead or of hurting yourself in some way) in the past two weeks. Per standard scoring instructions, we used a cut-off sum score of ≥10 to classify participants as moderately to severely depressed vs not to mildly depressed. We used the 7-item GAD Scale (GAD-7) for anxiety. 44 It contains seven questions relating to potential symptoms of anxiety experienced in the past two weeks (e.g., feeling nervous, anxious, or on edge, worrying too much about different things). Response options are the same as for the PHQ-9. Again, we categorized participants as exhibiting moderate to severe anxiety (GAD sum score ≥10) vs lower anxiety levels. Cronbach’s alpha in this sample was 0.81 for the PHQ-9 and 0.84 for the GAD-7.
Social Support: This was assessed using the Social Support Questionnaire. 45 Participants responded to five questions about the amount (1: “Definitely not enough” to 4: “Definitely enough”) of instrumental social support (defined as social support which relates to assistance in problem-solving by tangible help or information) in their environment (e.g., “Do you feel there are enough people in your environment that would lend or give you something you need, like food, clothing, or money?”) and another five questions about emotional social support (defined as the communication of caring, empathy, and esteem. For example, “Do you feel there are enough people that can comfort you when you feel unhappy about your daily life?”). 46 In each subscale, a sixth question from the original measure that was applicable only to people with young children was deleted, as our sample contained mostly people with older or adult children, as well as childless participants. The two subscales were highly correlated (r = 0.77), so we combined all items and took their mean score so that higher scores represent more support. Reliability was good: Cronbach’s alpha = 0.91.
Mental Illness Stigma: The Internalized Stigma of Mental Illness (ISMI) scale was used to measure internalized mental illness stigma. 47 Participants indicated their level of agreement (1: “Strongly disagree” to 4: “Strongly agree”) with 29 items representing five subscales: alienation (six items, e.g., feeling inferior due to one’s mental health problems), discrimination experience (five items, e.g., feeling patronized), stereotype endorsement (seven items, e.g., agreeing that people with mental health problems shouldn’t get married), social withdrawal (six items, e.g., avoiding getting close to people to avoid rejection), and stigma resistance (five items, e.g., feeling that one can have a good, fulfilling life, despite one’s mental health problems). As found in other studies, 48 the stigma resistance subscale was found to have low internal reliability in our sample (Cronbach’s alpha = 0.47) and therefore omitted from the variable constructed for the analyses reported here. Since the other subscales correlated between 0.68 and 0.80, we combined them all into one variable (Cronbach’s alpha = 0.93) by taking the mean over their 24 items, with higher scores representing more stigma.
Quality of Life: We used the physical (seven items, e.g., need for medical treat- ment to function, mobility), psychological (six items, e.g. ability to concentrate, self- esteem), and environment (eight items, e.g., opportunity for leisure, financial resources) subscales from the WHOQOL-BREF to assess participants’ QOL in the past two weeks. 49 Response options are on a Likert-type scale ranging from 1 to 5, with exact wording varying for different questions, but (reverse) scored as needed so that higher scores always indicate better QOL. The subscale scores range from 4 to 20; reliability was 0.78, 0.67, and 0.72 for physical, psychological, and environment-related QOL, respectively. We did not use the social subscale, which we assessed separately in more detail (see above), and a sexual relationships question, for which we had a high number of missing data, largely from widowed/unmarried female participants who possibly viewed the question as inappropriate.
Satisfaction with Health: This variable was measured with one question from the WHOQOL-BREF: 49 “How satisfied are you with your health?” (1: “Very dissatisfied” to 5: “Very satisfied”).
Demographics: We assessed the participant’s age, gender, marital status, religion, education, and household income.
All measures were administered by trained research assistants.
Analyses
Descriptive statistics consisted of frequencies and percentages for categorical variables and either means plus standard deviations (SD) or medians plus range for continuous variables, depending on their distribution. The association between mental health, psychosocial and demographic variables and the missed medications outcome was assessed via logistic regression analyses. For mental health, a model with depression, anxiety, and their interaction as predictors was explored. The interaction was not significant and therefore abandoned for the analyses reported here. All variables associated at P < 0.10 in unadjusted analyses were subsequently entered in a multivariate logistic regression model. Robust standard errors were used to account for the clustering of participants in PHCs. Analyses were performed in Stata v16.
Ethics Approval
Ethics approval was obtained from the Institutional Ethical Review Board at St. John’s Medical College and Hospital and the Committee on Human Research, University of California, San Francisco. All participants provided written informed consent.
Results
The sociodemographic characteristics of the study participants are shown in Table 1.
Sociodemographic Characteristics (N = 2486).
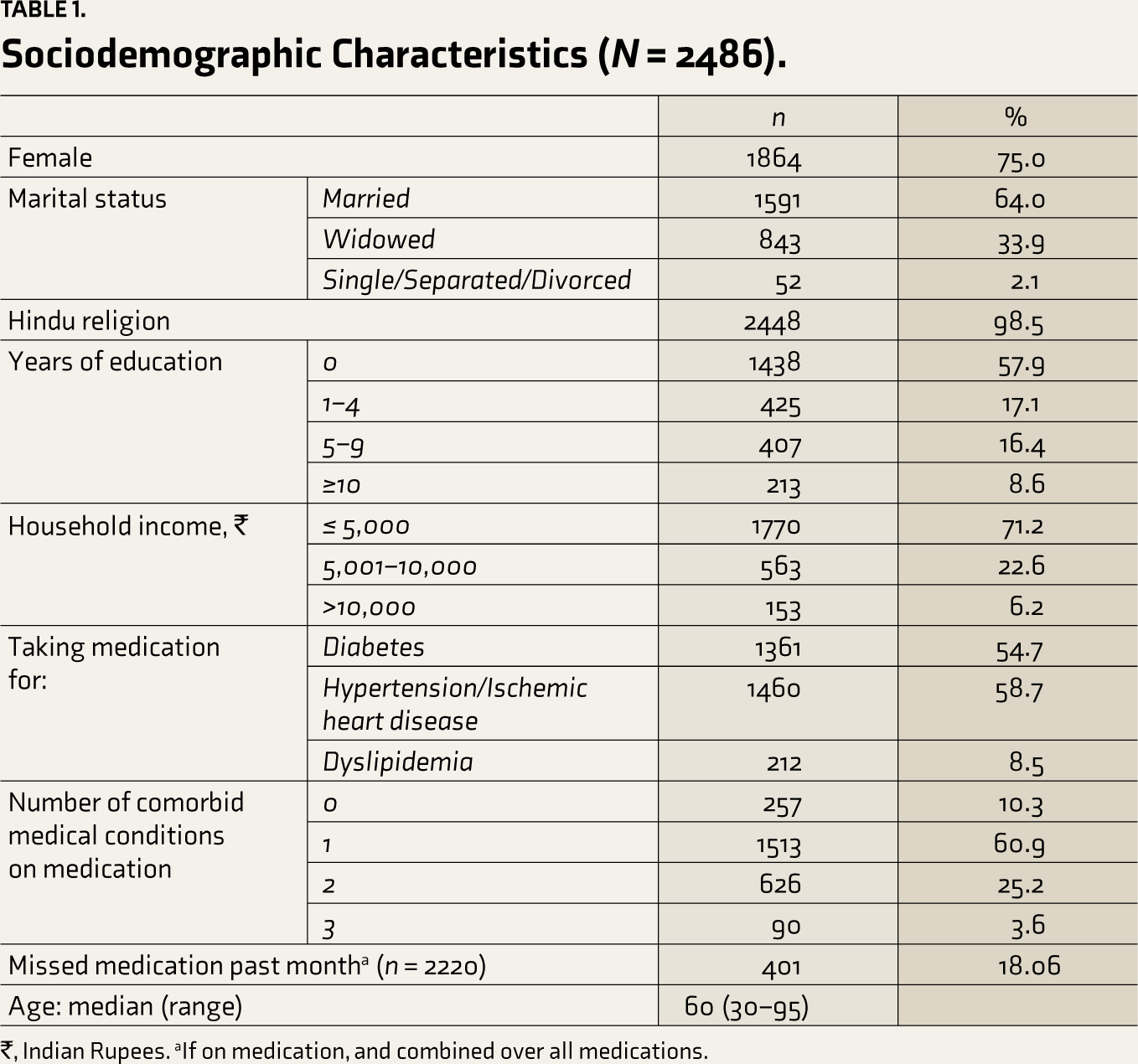
₹, Indian Rupees. aIf on medication, and combined over all medications.
Of the patients who met eligibility criteria, 2486 consented to participate in the study, while 192 declined. There were no significant differences between participants who did vs did not consent with respect to age or gender.
Most participants were female (n = 1864, 75%) and married (n = 1591, 64%). More than half had not received formal education (n = 1438, 57.9%), and more than two-thirds (n = 1770, 71.2%) had a monthly household income of ≤ 5000 Indian rupees. Slightly more than half the participants were on medication for diabetes (n = 1361, 54.7%) or hypertension/IHD (n = 1460, 58.7%). If participants were not on any medication for diabetes, hypertension/IHD, or dyslipidemia (n = 257), or adherence data were missing (n = 9), they were excluded from further analyses (n = 266). Of the participants on medication (n = 2220), almost one-fifth (n = 401, 18.06%) reported missing medication in the past month.
The psychosocial characteristics of participants who were on medication for diabetes, hypertension/IHD, and/or dyslipidemia are shown in Table 2.
Psychosocial Characteristics of Participants Who Were on Medication (N = 2220).
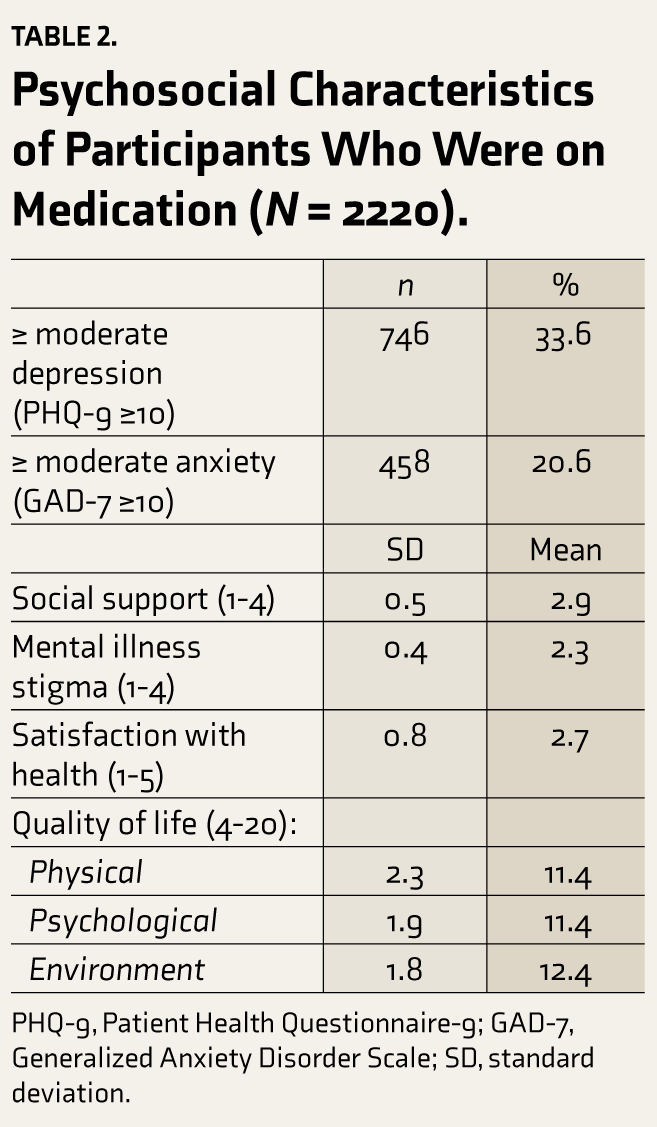
PHQ-9, Patient Health Questionnaire-9; GAD-7, Generalized Anxiety Disorder Scale; SD, standard deviation.
In the multivariate logistic regression model (Table 3), males (AOR = 1.74, 95% CI 1.37–2.22, P < 0.001) and participants with higher mental illness stigma (AOR = 1.46, 95% CI 1.07–2.00, P < 0.05) had higher odds of missing medication. In contrast, older participants, those with more social support (AOR = 0.65, 95% CI 0.49–0.86, P < 0.01) and those with higher satisfaction with their health (AOR = 0.74, 95% CI 0.61–0.89, P < 0.01) had lower odds of missing medication.
Unadjusted and Adjusted Logistic Regression Results for Missed Medication.
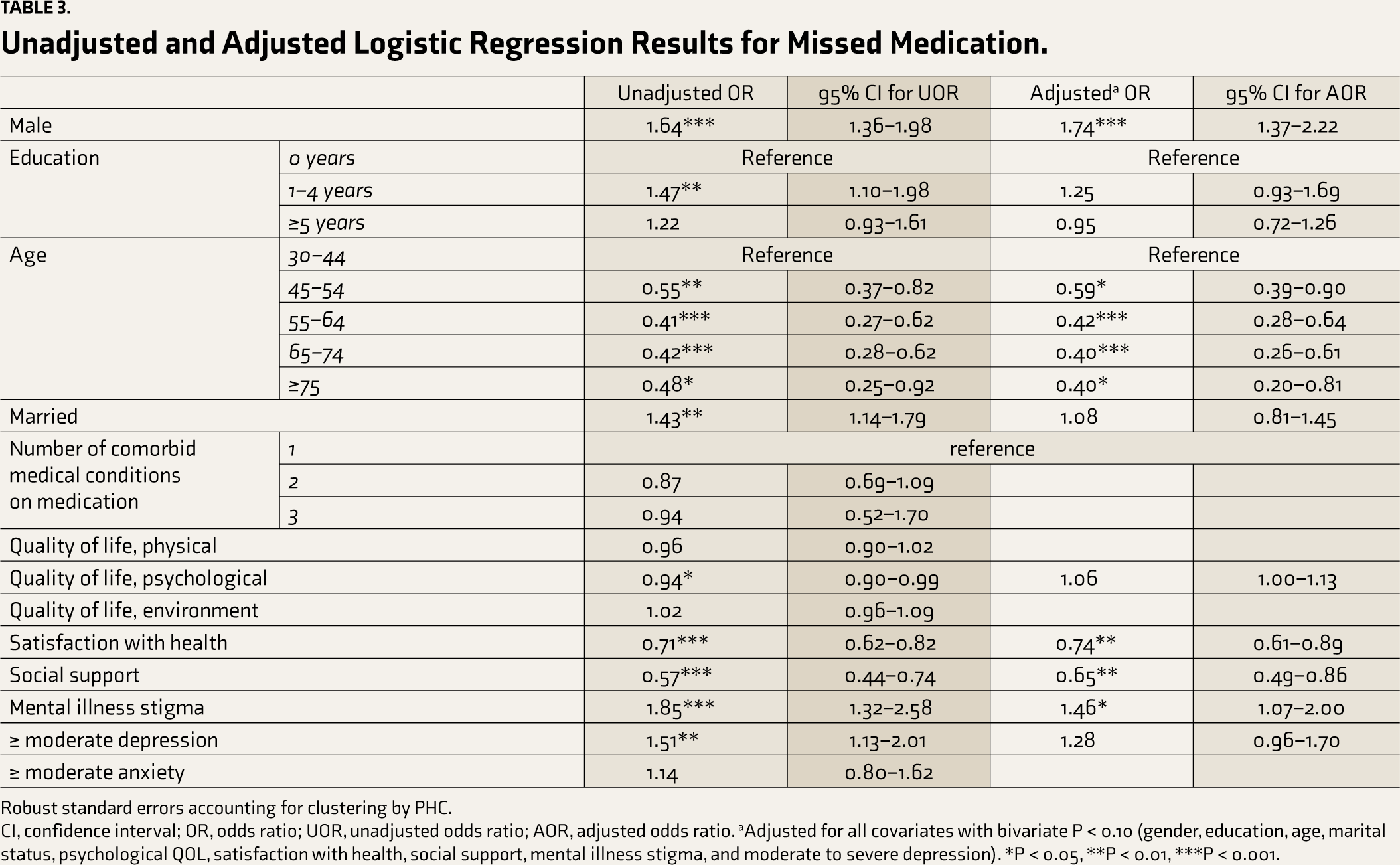
Robust standard errors accounting for clustering by PHC.
CI, confidence interval; OR, odds ratio; UOR, unadjusted odds ratio; AOR, adjusted odds ratio. aAdjusted for all covariates with bivariate P < 0.10 (gender, education, age, marital status, psychological QOL, satisfaction with health, social support, mental illness stigma, and moderate to severe depression). *P < 0.05, **P < 0.01, ***P < 0.001.
Discussion
This paper presents data on the association between psychosocial factors and adherence to medication for NCDs in a large sample of primary care patients with NCDs and comorbid CMDs from rural India. Although likely an underestimate, it is noteworthy that almost one-fifth of participants (18.06%) reported missing medication in the past month. Male participants and those reporting higher internalized mental illness stigma had higher odds of missing medication. Older participants and those reporting more social support and higher satisfaction with health had lower odds.
The proportion of participants who were nonadherent to their medication in our study (18.06%) was lower than the range (32.7–75.9%) reported by previous studies on patients with NCDs from primary care in India.11–15 This may be because our study used brief measures to capture medication adherence, which may have underestimated the number of patients missing medication. In contrast, prior studies have used longer, structured questionnaires like the MORISKY Medication Adherence Scale, Medication Compliance Questionnaire, or questionnaires specifically designed for the study, to capture medication adherence.11–15 Patients are known to overestimate adherence on self-reported recall of missed medications, 42 which may be more pronounced in response to a single question rather than multiple items on a scale. Social desirability bias may also have influenced the report of adherence to medication, resulting in underestimation of missed doses. 50
Depression has previously been shown to be an important determinant of medication adherence in NCD patients.17–19,27 One previous study of older adults with NCDs in primary care from India reported no significant association between depression and medication adherence. 11 As seen in the unadjusted model, moderate to severe depression was significantly associated with nonadherence to medication only in the bivariate analysis but not in the adjusted multivariate model. Moderate to severe anxiety was not significantly associated with missed medication. It should be noted that all our participants met the criteria for a diagnosis of major depressive disorder, dysthymia, GAD, and/or panic disorder on the MINI. Therefore the reference groups for these comparisons were participants with a diagnosis of a CMD with a lower severity score, unlike other studies that used participants without a psychiatric diagnosis.17,19,27 It is thus likely that not including patients without a diagnosis of CMD could have influenced the lack of associations with medication adherence in our analyses.
Stigma is a known barrier to implementing mental health programs in primary care in India. 51 We found that internalized mental illness stigma, characterized by cognitions similar to those seen among depressed individuals, negatively impacts medication adherence in patients with NCDs and comorbid CMDs. This is similar to the results of a study from India by Ansari et al., which showed that internalized mental illness stigma was negatively correlated with medication adherence in patients with obsessive-compulsive disorder. 52 Therefore, nonpharmacological intervention packages for improving patients’ medication adherence might benefit from including a module focussed on reducing internalized mental illness stigma. This could include psychoeducational interventions delivered in a group format, which are effective in reducing internalized stigma. 53 The number of sessions used in various psychoeducational approaches ranges from 1 to 12, but common strategies include providing information about mental health and mental disorders, the different forms of stigma, and the strategies to deal with it. 53 These strategies can be condensed into a module and delivered to patients with NCDs and comorbid CMDs, who, on assessment, are found to have higher internalized mental illness stigma.
We also found that participants who reported less social support had poorer medication adherence rates. This finding aligns with a prior study from rural Karnataka among older adults with NCD, which found that practical social support was significantly associated with good medication adherence. 28 Several studies, including those from primary care settings, have noted that social support interventions that employ family members or members of a peer group have efficacy in improving medication adherence in patients with hypertension.54–56 Such modules can be included in non-pharmacological intervention packages to improve medication adherence.
Future research could benefit from focusing on testing the efficacy of interventions to reduce internalized mental illness stigma and increase social support on medication adherence in patients with NCDs and comorbid CMDs. Future longitudinal studies could also examine the impact of the treatment of depression on medication adherence among NCD patients.
Our study included a large sample of primary care patients with NCDs and comorbid CMDs from rural India. Limitations include a cross-sectional design and the use of self-report to assess medication adherence. The generalizability of findings from the present study to other rural regions of the country is limited.
Conclusion
In rural India, greater internalized mental illness stigma and less social support are significantly associated with lower medication adherence rates in patients with NCDs and comorbid CMDs. Additional research is needed to examine the association between depression and adherence in samples that include participants who are not depressed. Interventions to reduce mental health stigma and improve social support should be empirically tested and integrated into the treatment of NCDs to improve adherence to medication regimens.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the US National Institute of Mental Health [R01MH100311].
Trial Registration
ClinicalTrials.gov NCT02310932 URL: