
Abstract
Background:
Neurotrophins have been implicated in multiple psychiatric disorders. Nerve Growth Factor (NGF) is one of the major neurotrophins that has attracted much research interest. Therefore, we undertook, to the best of our knowledge, the first scoping review encompassing all major psychiatric disorders and their relation to NGF. This review aimed to identify the current position of NGF in psychiatric research and to outline present gaps in knowledge, which can be answered with a more detailed systematic review in the future.
Methods:
Suitable studies were identified using PubMed. A total of 20 studies were included in the review: two on bipolar affective disorder (BPAD), three on schizophrenia, seven on depression, and eight on alcohol use disorder.
Results:
NGF levels are definitively reduced in BPAD and depression, while NGF levels in schizophrenia decreased further after treatment than in the drug-naïve state. The effect of treatment on NGF levels in depression varied based on treatment modalities and severity of depression. In patients with depression, raised NGF was a predictor of conversion to bipolar disorder (BD). NGF levels were raised in acute alcohol intoxication and withdrawal but normalized slowly as abstinence was maintained. NGF may play a protective role in preventing the toxic ill effect of acute alcohol intoxication on the central nervous system.
Conclusion:
Based on current knowledge, NGF levels may be a useful biomarker of a chronic mental stress condition. However, further research is needed before it can be used to identify a specific psychiatric illness or predict treatment response.
Neurotrophins are critically involved in neuronal and synaptic plasticity and regulation of brain development. They play key roles in differentiation and survival of neurons, as well as cell death associated with inflammation, ischemia, and seizure.1, 2 Nerve Growth Factor (NGF) was the first neurotrophin discovered in 1951 by R. Levi-Montalcini and is one of the best-characterized members of the group. Alterations in circulating NGF levels have been described in many neuropsychiatric disorders, including Alzheimer’s Disease, schizophrenia, schizophreniform disorder, and psychological stress conditions.3–5
Animal model studies have shown that NGF and other neurotrophins may be implicated in the light-dependent regulation of suprachiasmatic pacemaker and other functions implicated in the acquisition of long-term memory during sleep.6–8 Hippocampal formation and the frontal cortex have the highest expression and protein levels of NGF and Brain-Derived Neurotrophic Factor (BDNF) in CNS, and both are implicated in neuronal growth, development, and plasticity.9, 10 Specific alterations in the neuronal cytoarchitecture in those two regions have been implicated in schizophrenia,11, 12 which suggests that neurotrophins might have a role in schizophrenia. Adequate neurotrophic support is essential for normal brain development, suggesting that a deficit in neurotrophins in cortical neurons is an important factor in the pathophysiology of schizophrenia.13, 14
A growing body of evidence indicates that impaired neuroplasticity 15 and immunologic processes 16 may underlie the pathology of Bipolar Affective Disorder (BPAD), which points towards a role of neurotrophins in its pathophysiology. Despite evidence suggesting that neurotrophin levels are altered in BPAD, it remains unclear whether they can be considered a biomarker of the illness.
The neurotrophic factor hypothesis of depression postulates that the depressive state is associated with decreased neuroplasticity, neuronal atrophy, and aberrant neurogenesis in brain areas associated with memory and mood.17, 18 This theory is corroborated by findings that levels of some neurotrophins, notably BDNF, are lower in acute depressive episodes and tend to increase after treatment. 19 It is hypothesized that a reduction in neurotrophins in depression impairs the neural networks’ pruning and negatively impacts the structural and functional processes, particularly involving the limbic system. 20 Maximum research concerning neurotrophins in depression has been done involving BDNF. However, recent studies have been focusing on NGF too. Animal model studies have demonstrated decreasing NGF levels in various mice models, including models of anxiety vulnerability, stress-induced illness, and learned helplessness. Further, as NGF [along with Neurotrophin-3 (NT-3) and Neurotrophin-4 (NT-4)] binds to both TrK and p75 neurotrophin receptors, which also binds to BDNF, it also may play a role in the neurotrophic hypothesis. 20 Despite the recent surge in interest in the role of NGF in depression, the research is still not conclusive.
To the best of our knowledge, no previous reviews have examined the role of NGF in major psychiatric disorders. This review aims to identify the position of NGF in psychiatric research at present and to outline present gaps in knowledge that can be answered with a more detailed systematic review in the future.
Materials and Methods
The scoping review was conducted according to the PRISMA-ScR guidelines.
Search Strategy
A search was conducted on the PubMed database, without any year limitation. The initial search was conducted in July 2021 and updated in September 2022. The review aimed to study the role of NGF in schizophrenia, BPAD, depression, obsessive-compulsive disorder, schizoaffective disorder, and alcohol use disorders. Searches were conducted separately for studies on NGF in different diseases using the MeSH terms: Nerve Growth Factor AND depression; NGF AND depression; Nerve Growth Factor AND Major Depressive Disorder; Nerve Growth Factor AND MDD (Major Depressive Disorder); NGF AND MDD; Nerve Growth Factor AND bipolar disorder; NGF AND bipolar disorder; NGF AND BPAD; Nerve Growth Factor AND BPAD; Nerve Growth Factor AND mania; NGF AND mania; Nerve Growth Factor AND schizophrenia; NGF AND schizophrenia; Nerve Growth Factor AND alcohol; NGF AND alcohol; Nerve Growth Factor AND schizoaffective disorder; NGF AND schizoaffective disorder; Nerve Growth Factor AND obsessive compulsive disorder; Nerve Growth Factor AND OCD; NGF AND OCD.
Screening and Selection Criteria
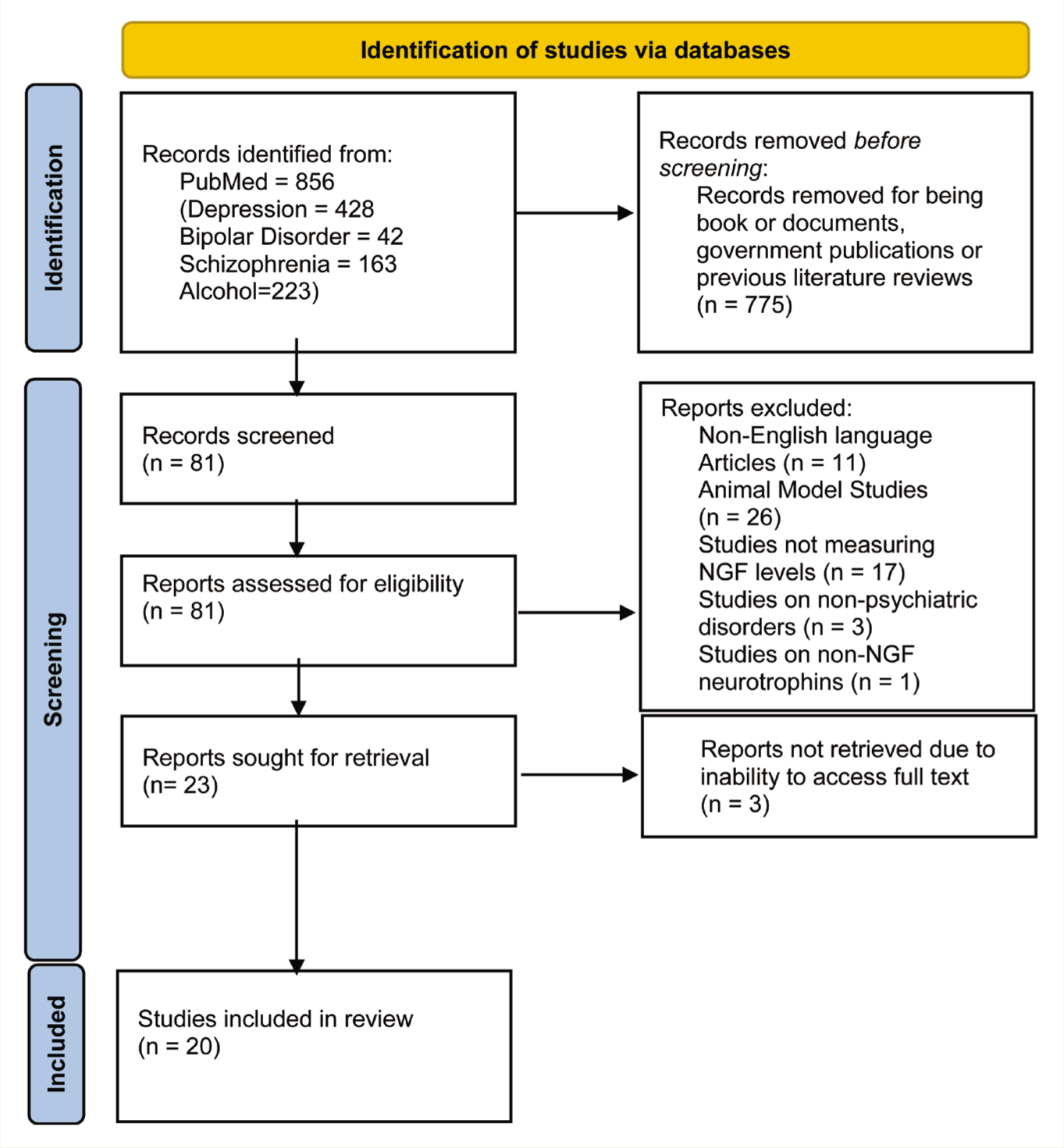
The first author conducted the screening. After conducting an initial search, the studies were filtered to include case reports, classical articles, clinical conference papers, clinical studies/trials, controlled clinical trials, multicenter studies, observational studies, and Randomized Controlled Trial (RCT). Books, previous reviews, animal model studies, and studies that did not measure NGF levels were excluded. Only studies that were reported in the English language were included. A total of 23 studies were found to be eligible for the review. Finally, 20 studies were included in the review after removing those for which full text could not be accessed or those found to not pertain to the subject matter after reading the full text (Figure 1). The final decision on which studies to include was made by all three authors. The selected studies are detailed in Table 1.
Identification of Studies via Databases.
Details of Studies Selected for Review.
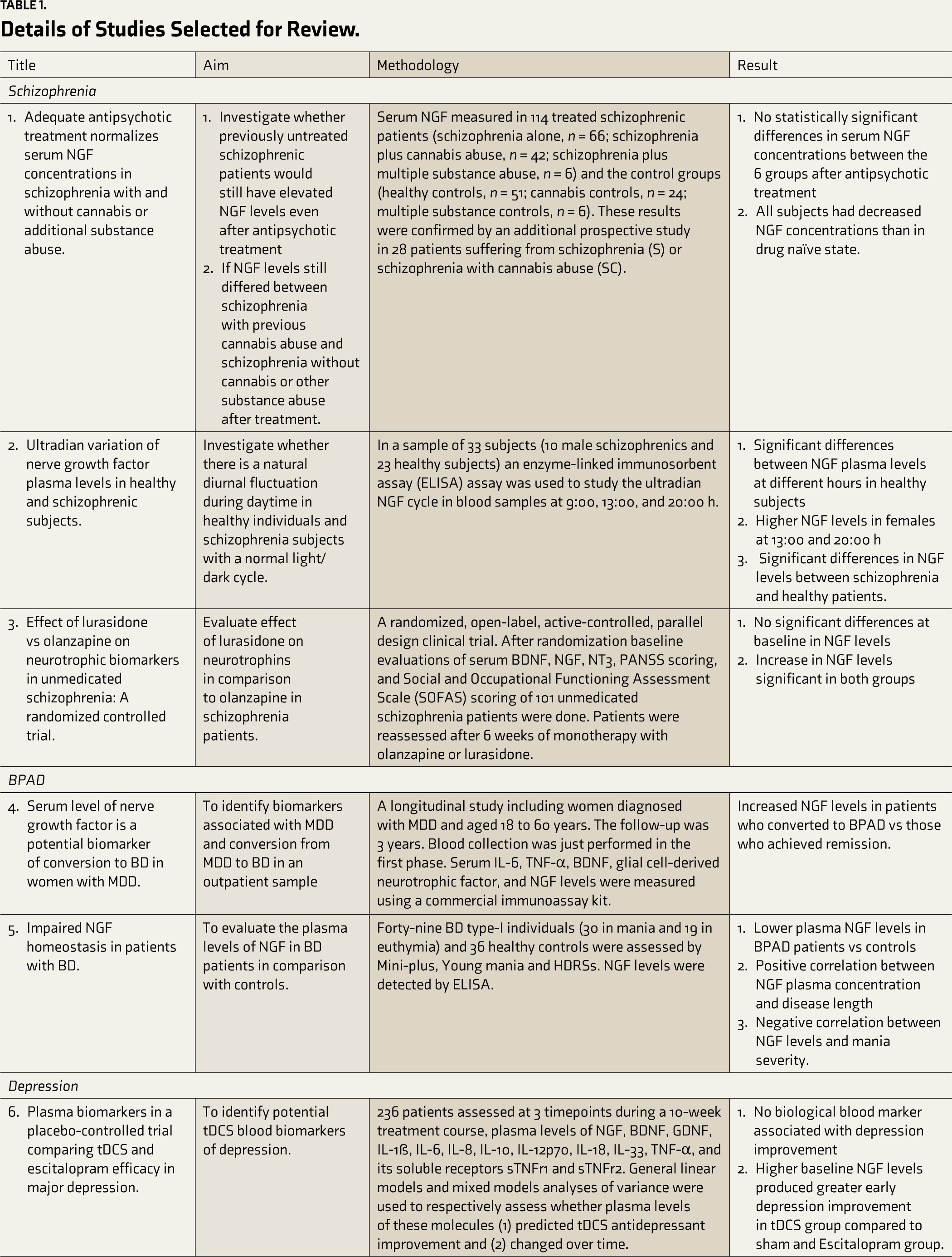
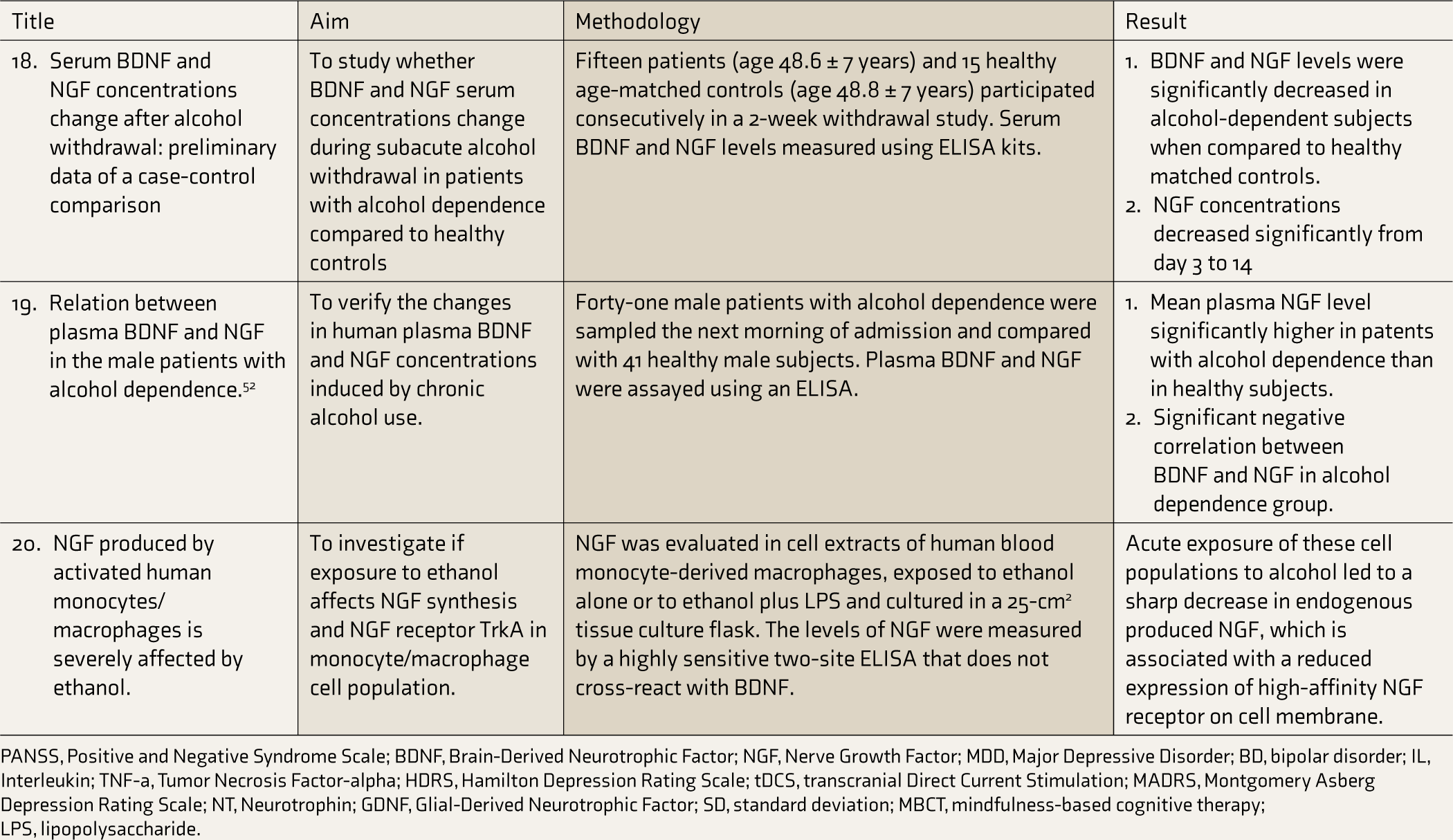
PANSS, Positive and Negative Syndrome Scale; BDNF, Brain-Derived Neurotrophic Factor; NGF, Nerve Growth Factor; MDD, Major Depressive Disorder; BD, bipolar disorder; IL, Interleukin; TNF-a, Tumor Necrosis Factor-alpha; HDRS, Hamilton Depression Rating Scale; tDCS, transcranial Direct Current Stimulation; MADRS, Montgomery Asberg Depression Rating Scale; NT, Neurotrophin; GDNF, Glial-Derived Neurotrophic Factor; SD, standard deviation; MBCT, mindfulness-based cognitive therapy; LPS, lipopolysaccharide.
Results
NGF and Schizophrenia
Three studies about schizophrenia were included in the review. The first study had six groups (schizophrenia patients without cannabis use, with cannabis abuse, with multiple substance use, and their respective healthy controls). No significant differences in the serum NGF concentrations were found between the six groups. After antipsychotic treatment, all the patients had lower NGF concentrations than in the drug naïve state, irrespective of the previous drug use status, though the degree of decrease varied. 21 Those patients who consumed cannabis regularly in the past showed significantly elevated NGF serum concentrations (412.9 ± 288.4 pg/ml; median, 286.7 pg/ml) compared to schizophrenia patients without a history of cannabis abuse (p < 0.0001), healthy controls (p < 0.0001), and otherwise-healthy persons with cannabis abuse (p < 0.0001). The group of patients with schizophrenia and multiple substance abuse in the past showed even greater elevation of their NGF serum concentrations with a mean (±SD) value of 2336.2 ± 1711.4 pg/ml (median, 2005.1 pg/ml), which differed significantly from all other groups (p < 0.001 for every group comparison). 22
In the second study, significant differences were found in the NGF levels of healthy subjects at different hours of the day in both males and females, with females displaying significantly higher levels and larger diurnal differences. Significant differences were also seen in the NGF levels between healthy males and schizophrenia patients at 09:00 and 20:00 h. 23
The third study compared the effect of olanzapine and lurasidone on changes in serum neurotrophins. No differences in NGF levels were found at baseline. A significant increase in NGF levels was found in both groups after six weeks of treatment, though no statistically significant difference could be seen when the mean change of the individual groups was compared. No correlation was found between the positive/negative/total Positive And Negtive Syndrome Scale (PANSS) scores and NGF levels at baseline or after treatment. 24
NGF and BPAD
Two articles were included. The first found a 15.4% rate of conversion from MDD to BPAD in their exclusively female sample. Increased NGF levels were seen in those who converted to BPAD vs those who achieved remission from MDD. Only NGF, out of the five different cytokines studied [Interleukin-6 (IL-6), Tumor Necrosis Factor-α (TNF-α), Glial-Derived Neurotrophic Factor (GDNF), BDNF, and NGF] was found to be associated with conversion to BPAD. 25
The second found significantly lower plasma levels of NGF in BPAD patients than in healthy controls and a positive correlation between the levels of NGF and total disease duration. NGF levels were also negatively correlated with mania severity, as assessed using Young’s Mania Rating Scale (YMRS). However, no correlation was found with the severity of depressive symptoms. NGF levels did not differ in BPAD categorized according to the presence of psychiatric comorbidities (i.e., generalized anxiety disorder, panic disorder, obsessive-compulsive disorder) or dependence on substances or nicotine. No significant differences were found in patients receiving or not receiving different medication, either (lithium, sodium valproate, carbamazepine, antidepressants, or antipsychotics). 26
NGF and Depression
Seven studies were found. The main aim of the first study was to identify potential transcranial Direct Current Stimulation (tDCS) blood biomarkers of depression. Secondary goals were to assess whether plasma levels of various cytokines predict tDCS antidepressant response and verify if those molecules’ plasma levels changed over time and according to the treatment group and clinical response. The study did not find any blood biological markers to be associated with improvement in depression. Higher NGF levels predicted early improvement in the tDCS group compared to the sham and Escitalopram groups. NGF was the only one of the 13 cytokines analyzed to predict response to tDCS vs Escitalopram. 27
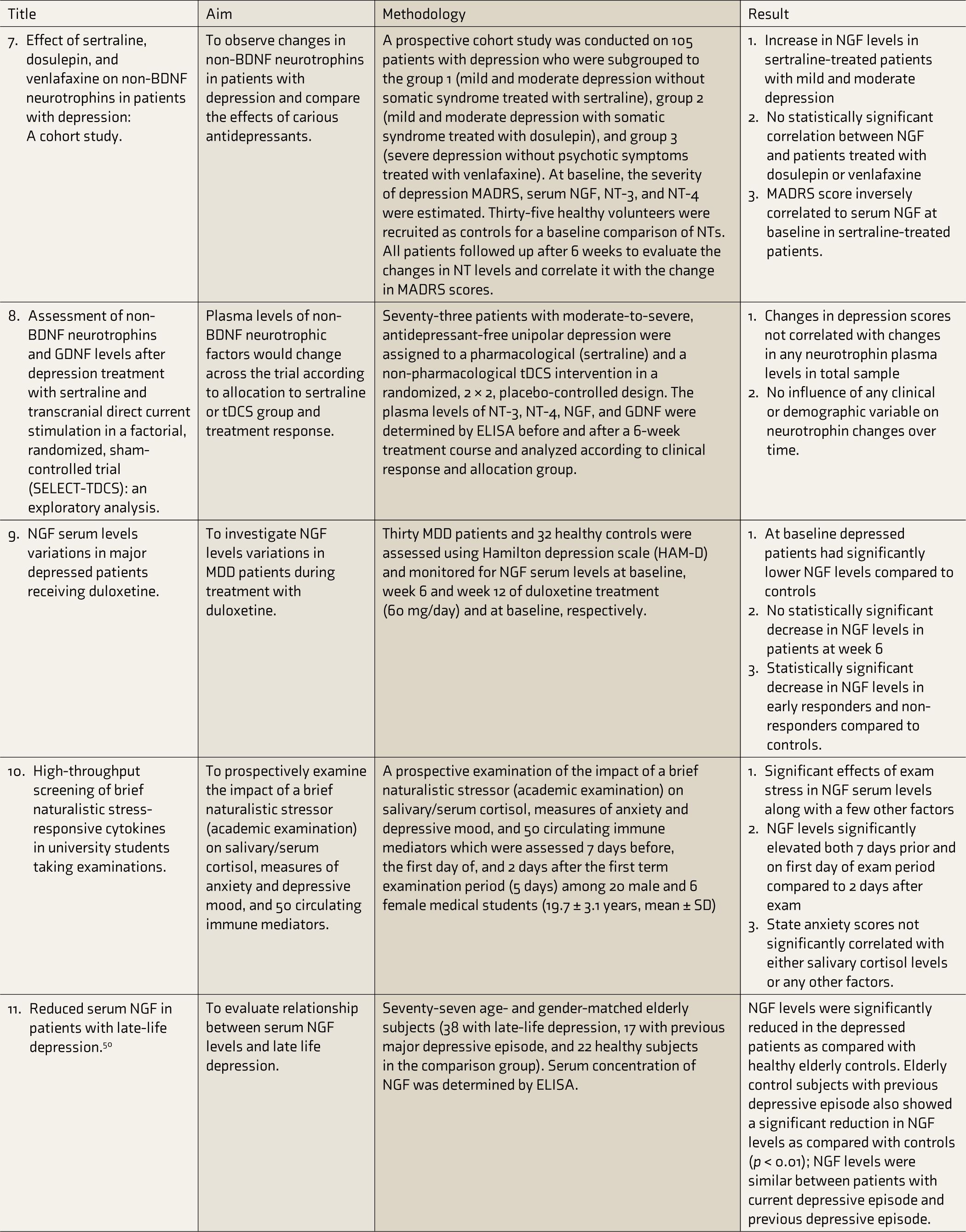
The second study divided the patients into three groups based on the severity of depression and the treatment received. The patients with mild/moderate depression without somatic syndrome were treated with sertraline and placed into group 1. Those with mild/moderate depression with somatic syndrome were treated with dosulepin in group 2. The third group comprised patients with severe depression without psychotic symptoms treated with venlafaxine. A statistically significant increase in NGF levels was found only in group 1. In group 1, NGF levels were also inversely correlated to Montgomery Asberg Depression Rating Scale (MADRS) scores at baseline. No associations were found between the other neurotrophins and the MADRS rating. 28
The third study evaluated serum levels of different neurotrophins to see whether they changed according to allocation to sertraline or tDCS groups and treatment response at various time points. It was seen that the changes in depression scores on Hamilton Depression Rating Scale (HDRS) did not correlate with changes in plasma levels of any neurotrophin. Neither an effect of time nor an interaction of time with group, clinical response, or group and clinical response could be observed. No influence of any clinical or demographic variable on neurotrophic changes over time was seen either. Plasma levels at baseline were not found to be associated with depression improvement either, using regression models. 29
The next article studied variations in NGF serum levels in MDD patients receiving duloxetine. It grouped the participants whose week 6 HDRS scores were reduced by 50% compared to baseline on Duloxetine treatment as Early Responders (ER) and the others as Early Non-Responders (ENR). At baseline, the patients had significantly lower NGF levels than controls, with statistically significant lower values in ENR and no difference between ER and controls. At week 6, no statistically significant change in NGF levels was found in any of the groups compared to baseline, but both ER and ENR groups had a statistically significant decrease in NGF compared to controls. Week 12 showed significantly lower levels of NGF, compared to the week 6 values, in ENR compared to ER. 30
Another article measured the serum concentrations of 50 factors, using cytokine panels, in individuals undergoing a brief naturalistic stressor: term-end exams. Significant effects of exam stress were observed in serum levels of βNGF along with a few other factors [Interleukin-4 (IL-4), Interferon-γ (IFN-γ), Monocyte Chemotactic Protein-3 (MCP-3), Interleukin-16 (IL-16), and Macrophage Migration Inhibitory Factor (MIF)]. Serum levels of βNGF on both seven days prior and on the first day of the exam period were significantly elevated compared to two days after the examination. 31
Diniz et al. evaluated the relationship between serum NGF levels and late-life depression. They recruited age- and gender-matched elderly subjects with late-life and previous depressive episodes. NGF levels were significantly reduced in both groups (p < 0.01), but no difference in NGF levels was found between the groups.
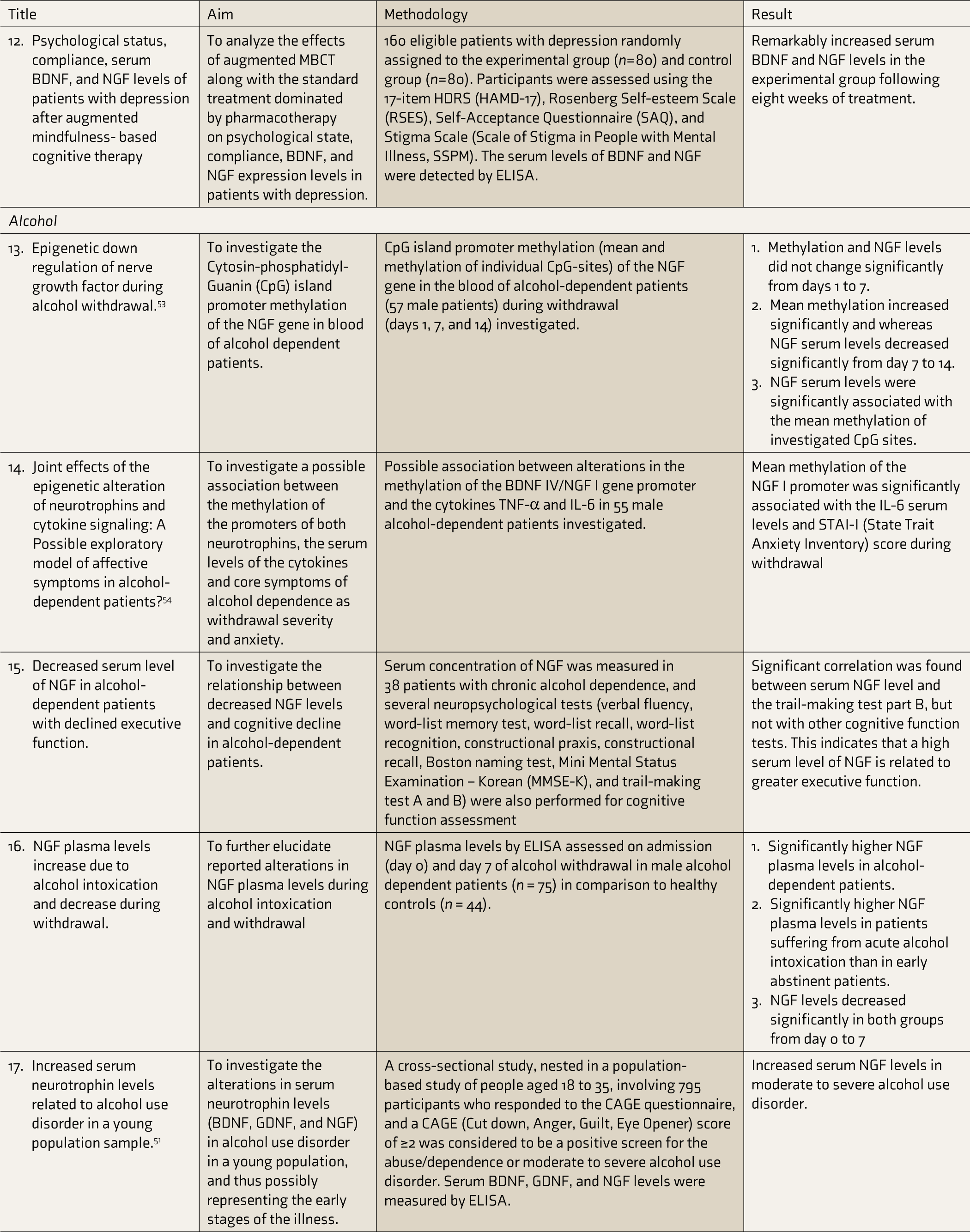
The last article studied the effects of mindfulness-based cognitive therapy (MBCT) on depression, BDNF, and NGF levels and found that MBCT caused a remarkable increase in NGF levels following eight weeks of treatment and also lowered the patients’ HDRS scores significantly. BDNF levels also decreased significantly. 32
NGF and Alcohol
Seven studies were included. Lhullier et al. studied young patients with alcohol use disorder (AUD) and found higher serum levels of NGF than controls. 51 Lee et al. compared 41 male inpatients with AUD with 41 healthy male subjects; plasma NGF concentration was elevated in the patients within 24 h of abstinence. Another study on alcohol withdrawal examined 15 patients with alcohol dependence according to the DSM-IV criteria and 15 healthy subjects. In the patients, the mean NGF concentrations increased initially and then decreased significantly from days 3 to 14. 33 These findings agree with the NGF gene’s epigenetic down-regulation during alcohol withdrawal, as demonstrated by Heberlein et al. They had investigated the correlations between alterations in NGF serum concentrations and changes in the methylation of the NGF promoter during alcohol withdrawal by studying 57 patients with alcohol dependence, who showed a significant decrease in the NGF serum levels from day 7 to day 14 of withdrawal and a significant increase in the methylation of the CpG-sites within the NGF gene promoter. 53 Heberlein et al. also demonstrated that the mean methylation of NGF promoter is significantly associated with IL-6 serum levels and State Trait Anxiety Inventory scores during withdrawal. 54 Another study investigated the relationship between NGF plasma concentration and cognitive dysfunction of alcohol-dependent patients during abstinence. The NGF levels were higher in patients with lower completion times in trail-making test B, which includes motor components and visual scanning, indicating better executive function. 34 Another study found that, in patients with alcohol dependence, acute alcohol intoxication was related to an increase in NGF plasma levels, which decreased after withdrawal, indicating that NGF plasma levels may increase to block the toxic effects of alcohol during acute intoxication. 35 Caroleo et al. studied the effects of acute ethanol exposure in blood-monocyte-derived macrophages cultured in vitro. These cells were isolated from the peripheral blood of healthy donors in basal conditions and produce a little NGF, which increases if they are activated in vitro by treatment with lipopolysaccharide (LPS). The acute exposure of LPS-activated cultures to ethanol was found to alter NGF synthesis, reduce the expression of Tyrosine kinase A (TrkA), as well as decrease the production of TNF-α.
The search strings Nerve Growth Factor AND schizoaffective disorder; NGF AND schizoaffective disorder; Nerve Growth Factor AND obsessive compulsive disorder; Nerve Growth Factor AND OCD; NGF AND OCD did not yield any results, neither did any searches involving the term “AND mania”.
Discussion
NGF is essential in tropism and structural changes of specific neuronal populations, including basal forebrain cholinergic neurons and homeostasis of neuro-endocrine immune system. 36 Hypothalamo–pituitary–adrenal axis hyper-activity and glucocorticoids seem to inhibit basal forebrain cholinergic neurons and increase NGF. However, a chronic high dose of glucocorticoids can also cause the downregulation of NGF.3, 36, 37 Therefore, acute stress increases NGF serum levels, while repeated stress paradigm might result in long-term downregulation. 38
NGF is a neuroplasticity marker. Thus, a decrease in NGF may indicate a neural adaptation process that might be ongoing due to a chronically stressed state. It can also be inferred that NGF is more likely a state-dependent variable than a trait-dependent one.
The three studies reviewed about NGF and schizophrenia brought up complementary results. One study reported raised levels of NGF in drug naïve schizophrenia compared to that after treatment, which the researchers attributed to a “normalization of NGF”, on treatment, in patients with a history of substance abuse. 21 The other two reported a lower level of NGF in patients than healthy controls. All but one of the studies had a good sample size (195 and 92). One study used Lurasidone and Olanzapine as treatment options while the treatment provided in the other study was not reported. A meta-analysis of peripheral blood NGF levels in schizophrenia, conducted in 2017, totally comprising 1693 individuals, quite conclusively reported that schizophrenia patients had lower NGF levels than healthy controls in both drug-free and medicated states, which also complements the findings of the studies reviewed. 39 Altogether, it might be hypothesized that increased NGF levels in cannabis users with schizophrenia might be an indicator of the regenerative and neuroprotective properties of cannabis on cognitive functioning,40, 41 functioning via NGF upregulation. An increase in NGF levels seen on treatment using antipsychotics (Olanzapine and Lurasidone) might point to the same direction and throws up interesting questions regarding the role of cannabis in schizophrenia and the possibility of a self-medicatory nature of cannabis abuse in schizophrenia. Schizophrenia has been reported to cause specific alterations of neuronal cytoarchitecture in the hippocampal formation and the frontal cortex.11, 12 The central cannabinoid receptor CB1 has its highest expression in the hippocampus and frontal cortex, 42 hinting at a possible connection between the two. The study on ultradian variations in NGF levels would also support the hypothesis that bio-rhythm alterations affect NGF plasma levels, making cross-study comparisons and even individual comparisons quite difficult to reliably comment upon unless stricter control measures are applied.
As mentioned previously, it has often been thought that immune system abnormalities and an increased inflammatory response may contribute to the pathology of BPAD.16, 43 A corollary to this would be that BPAD would result in elevated levels of all, or many, neuroinflammatory markers. Previous studies supported this hypothesis by demonstrating increased levels of TNF-α and IL-6 in BPAD patients than in healthy controls.44, 45 These findings were not replicated in another study included in the review, with only NGF shown to be associated with neuroconversion to BPAD in females with MDD. NGF levels were correlated positively with disease duration and negatively with mania severity as assessed using YMRS. These findings support the potential role of NGF as a biomarker for BPAD, though a sample size of two studies may be too small for a definite comment.
It has been quite conclusively reported that NGF levels in depressed patients at baseline are significantly lower than in healthy controls. A 2015 meta-analysis reported the same but also concluded that NGF levels did not change significantly even after treatment. 46 The studies reviewed here largely support those findings, with no significant change in NGF levels seen in patients treated with Duloxetine, Dosulepin, or Venlafaxine. Patients receiving tDCS also did not show an increase in NGF levels despite improvement in HDRS scores. One study did report an increase in NGF blood levels of patients with mild depression without somatic syndrome being treated with Sertraline. But the same study reported no NGF changes in patients with more severe depression being treated with other molecules. One study did, however, report that higher baseline NGF levels were associated with better response to tDCS than Escitalopram. In contrast, another study on the effect of MBCT in depression showed a remarkable rise in NGF levels after eight weeks of treatment, leading the researchers to speculate that higher NGF levels may be associated with more resilience and/or more responsiveness to treatment, with an early response and later compensatory changes. 27 However, as an article reviewed in this study reported, in MDD patients, neuroconversion to BPAD is associated with higher baseline NGF levels. 25 Thus, early treatment response to tDCS may be a sign of underlying bipolarity and an indicator of the switch-inducing potential of tDCS compared to Escitalopram.
Acute stress increases NGF levels, while repeated stress leads to long-term NGF downregulation. 38 This is corroborated by the study on exam-going students included in this review, which showed raised NGF levels, along with higher State Anxiety Scores, even up to seven days in advance. In contrast, the understanding of depression as a chronic stress condition helps explain the commonplace finding of low baseline NGF levels in the disease.
Several studies have been conducted in acute alcohol intoxication as well as alcohol-dependent patients to determine the correlation between plasma NGF concentration and alcohol dependence. All the studies seem to confirm that NGF plasma levels increase during acute intoxication and in the initial withdrawal phase and slowly decrease as abstinence is maintained. Studies by Heberlein et al. on the epigenetic regulation of NGF also suggest the same.53, 54 It has been hypothesized that NGF levels increase during acute intoxication to protect against the acute toxic effects of alcohol. Some studies also suggest a protective role of NGF in preventing neuronal damage in patients with alcohol dependence. 47 Studies have also implicated NGF in newer mechanisms of alcohol-induced compromise in the efficiency of the mononuclear phagocyte system.48, 49
The review highlights the dearth of literature about NGF levels in psychiatric disorders other than depression and alcohol dependence. The existing literature on NGF in schizophrenia and BPAD only throws up more questions regarding:
The role of cannabis and the nature of cannabis use in schizophrenia. The differences in the pathophysiology of BPAD in men and women. The role played by NGF and other neurotrophins in unipolar vs bipolar illness. Differences in mechanism of actions of different therapeutic modalities in depression and the possible neuroprotective roles of Sertraline and tDCS over other modalities. Neuroprotective effects of NGF in alcohol intoxication and schizophrenia.
Hopefully, this scoping review will pave the way for future research targeting these specific areas.
Conclusion
Most research about the role of NGF in psychiatry so far has been done in depression and alcohol. This is indicated by the maximum number of search results obtained for “NGF and Depression” or “NGF and Alcohol” and also the number of studies included in this review being the highest for depression and alcoholism. NGF levels are less in both depression and schizophrenia compared to healthy controls, while the research on the role of NGF in BPAD is not conclusive enough for comment as of yet. Further studies are needed on the effect of various treatment protocols on serum NGF levels for both depression and schizophrenia before it can serve as a biomarker, not just for the depressed or schizophrenic state, but also for treatment response and disease severity. NGF and other growth factors may also be considered crucial elements for disclosing innovative information on AUD. In particular, important findings show increased NGF plasma concentrations during alcohol intoxication and a possible protective role against neuronal degeneration.
One limitation of this review is the use of only one online database for the identification of suitable studies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.