
Abstract
Background:
Social cognition is the capacity to detect, comprehend, and evaluate environmentally relevant information and serves as a critical skill for effective interpersonal functioning. A significant clinical characteristic of depressive illness is the impairment in social and interpersonal functioning. Given the increasing prevalence of interpersonal difficulties among individuals with depression, it is crucial to get a greater insight into the underlying cognitive mechanisms leading to these social deficits. Alongside, early maladaptive schemas (EMS) also serve as proximal cognitive risk factors for depression. Altered socio-cognitive functioning in individuals with can help to draw a connection between impaired social cognition and EMS. In this context, the present study explores the role of social cognition in individuals with depression in relation to EMS.
Methods:
In this study, individuals of both genders (N = 60) were pooled based on the inclusion and exclusion criteria and screened for depression through the Beck Depression Inventory. Emotion Recognition and Theory of Mind (ToM) were assessed using the Reading Mind in the Eyes Test (RMET) and Theory of Mind Assessment Scale (TH.O.M.A.S), respectively. EMS was assessed using the Young Schema Questionnaire-Short Form.
Results:
Results indicate individuals with depression were found to be impaired in both domains of social cognition-emotion recognition and ToM. Individuals with depression also exhibited a greater number of EMS. A significant association was found between EMS and social cognition in depression. Moreover, few of the EMS emerged as significant predictors for social cognition in depression.
Conclusion:
Individuals with depression exhibit impairment in “reading” social interactions. Moreover, they exhibit specific EMS that emerges as significant predictors of social cognition. Implications of the study focus on recognizing EMS as a tool for addressing the socio-cognitive impairment in depression.
The role of social cognition is particularly relevant in depression owing to prominent social and interpersonal difficulties. It is important to understand the underlying cognitive mechanisms leading to these social deficits. The study helps in understanding the association between impaired social cognition and EMS in the context of depression.Key Message:
Depression is one of the most common mental disorders, marked by persistent low mood and/or loss of enjoyment and interest, and is linked with considerable impairment in daily functioning. 1 Individuals with depression retreat from social connections and express less satisfaction in interaction with others. There are several possible contributors to functional impairment in depression, including the degree of severity, comorbidity, treatment response, personality, motivation, dysfunctional thought processes, and the intensity of symptoms and neurocognitive difficulties. Neuropsychological studies in different mental health conditions have revealed deficits in social cognition in a variety of these disorders, including bipolar disorder, autism, and schizophrenia.2–4 Difficulties with social cognition, particularly emotion detection and theory of mind (ToM), can play an essential role in functional impairments in these psychiatric conditions.5–7
Social Cognition in Depression
Socio-cognitive impairment in depression 8 if found to be consistently related with depression, might be especially significant to social difficulties in depression, since social cognition is required for effective and adaptive interpersonal functioning and communication. Facial emotion recognition has been the most extensively researched domain of social cognition in Major Depressive Disorder. Depression was found to have a substantial influence on facial emotion recognition skills. 9 Depression may also be associated with impairments in more complex and demanding components of social cognition, such as ToM. ToM is a crucial facet of social cognition and can be defined as the ability to attribute mental states, such as desires, intentions, and beliefs, to other people in order to explain and predict their behavior. 10 ToM is an important skill for adjusting to our complex social environment. Depression is centered on the concept of dysfunctional cognition.
Early Maladaptive Schemas (EMS) in Depression
Distortions of thought content, also known as cognitive distortions, and EMS are two types of abnormal cognitive processes linked to depression. 11 Cognitive schemas, according to Alford and Beck, 12 bias the processing of information from the environment in a way that causes cognitive distortions. According to Beck’s cognitive theory, schemas are crucial in deciding how an individual processes and assigns meaning to environmental stimuli, the information that the person attends to and remembers, and in general societal adaptation and functioning. Young recently revised the schema concept, emphasizing EMS as a key structure in psychopathology development. 13 EMSs are convictions about oneself and the world that are stable, trait-like, and lasting, and are based on early childhood experiences. 12 EMS are relatively stable throughout childhood. Once triggered, they have the potential to distort reality representations. There are 18 EMSs, which are divided into five schema domains: disconnection and rejection, impaired autonomy and performance, impaired limits, other-directedness, and over-vigilance and inhibition. 13
EMSs have been related to depression in previous studies: they may be a risk factor for depression and an indication of vulnerability for depression. 14 EMSs are proposed as proximal cognitive risk factors in the schema model for persistent depression, mediating the impact of personality pathology and adverse life experiences on the persistence of depression and remaining stable without adequate intervention. 15 Specific, relatively stable EMSs distinguish individuals with depression from healthy counterparts.16–19 The EMSs from the domains of disconnection and rejection, as well as impaired autonomy schema, have been linked to depression.18, 16
Research studies that describe altered socio-cognitive capacity in individuals with depression can help to draw a connection between impaired socio-cognitive ability and EMS. Studies reveal that in depression, emotion recognition is either deficient or more accurate with respect to healthy controls in defining a negative emotional state, with little distinction between neutral and positive states. This may be due to the abstraction and negative filtering that is common in depression, that is, a bias for negative emotions over positive or neutral emotions. EMS leads to biased information processing, with selective filtering of corroborating information and dismissal of contradictory.20–23 Scanning for evidence and dismissing contradictory facts serve to maintain the schemas throughout one’s adult life and relationships.
Studies also show that individuals with depression tend to be deficient in the primary cognitive ToM tasks of interpreting both first- and second-order questions relating to social experiences. They often have less emotional understanding of what others are thinking, but good insight into their own emotional state. As a consequence, they can find it difficult to empathize with other people’s feelings.
As a result, both impaired and enhanced ToM can have negative consequences in terms of social functioning. An impaired ToM makes it difficult to correctly interpret what another individual is experiencing, resulting in selective abstraction and mental filtering errors that prevent the person from making adaptive adjustments to other people’s behavior, which can lead to conflicts, anxiety, withdrawal from social interactions, and other issues. Hypersensitivity to others’ mental states, on the other hand, provides further opportunities to use the negative biases of catastrophizing and overgeneralization in understanding others’ behavior and can be the source of the very interpersonal stressors that lead to severity in depressive symptoms.
The existence of rigid representations of interpersonal relationships, as defined in several clinical theories of personality, has been investigated in studies concerning cognitive schema–driven biases and ToM.14, 24, 25 However, few studies have looked at the connection between EMS and different aspects of social cognition particularly in the context of depression to date. Hence, the present study aims to study the role of social cognition in depression and the different facets of social cognition relating to the EMS. The study further aims to investigate the role of EMS if any in the socio-cognitive ability of individuals with depression.
Method
The current study used a cross-sectional design and was carried out in compliance with the Helsinki Declaration principles. Following Ethics Committee approval (Ref No: DRC-AIBHAS/ETHICS/A95210919007 dated 21.05.2021), 60 participants of both genders, 30 diagnosed with depression and 30 healthy controls in the age group of 18–55 were recruited through purposive sampling from private clinics, government and private hospitals, and communities in and around Kolkata. Individuals with depression for a minimum of two weeks were recruited from clinics and hospitals, were primarily diagnosed by a consultant psychiatrist using International Classification of Diseases (ICD-10) guidelines, and were taking psychiatric medications. The Beck Depression Inventory-II 26 was then administered to the participants in order to assess the severity of their depression. The healthy control group was age and gender-matched, biologically unrelated, and included individuals without a history of any psychiatric disorders in themselves and in their first-degree relatives (participant’s report and clinical assessment).
Participants in both groups had to be literate in English and able to give written, informed consent. Participants in the study had completed at least 12 years of formal education. Those having a history of any chronic medical or psychiatric condition, as reported, were excluded from the research. Participants provided written informed permission and were assured that their identities would be kept confidential. Participants completed a semi-structured socio-demographic and clinical datasheet that included information on age, gender, education, employment, physical and mental disease (if any), type of interpersonal interactions, and particular stressors in their lives.
The Reading Mind in Eyes Test (RMET) 27 is a brief test of social cognition, primarily mental state perception. Participants were shown 36 grayscale images of eye regions on various faces that express a variety of mental states in this exercise. Four words or phrases were shown around a single photo at the same time, each describing a potential mental state. Participants picked one of four terms that best defined what the person in the photograph was thinking or feeling. The items are presented in a predetermined order, and the test is graded on the number of correct answers. Each correct answer is given one point, with a minimum of 0 and a maximum of 36 possible. Responses that are incomplete are marked as incorrect. The test has moderate internal consistency (Cronbach’s alpha = 0.6) and test-retest reliability (intraclass correlation coefficient = 0.64, p < .001). Positive correlations have also been found between RMET and Wechsler picture arrangement (r = 0.60, p < .001), picture completion (r = 0.54, p < .001), and comprehension subtests (r = 0.48, p < .001). 28
The Theory of Mind Assessment Scale (TH.O.M.A.S) 29 consists of 37 open-ended questions that require the interviewee to present and clarify his or her thoughts on the functioning of ToM in everyday life, as well as examples that he or she can provide spontaneously or in response to a specific request from the interviewer. The structure of the interview splits the questions into four scales, each concentrating on a different internal or social domain where ToM is involved: Scale A (I–Me), Scale B (Other–Self), Scale C (I–Other), Scale D (Other–Me). Each of the four scales is subdivided into three subscales that investigate how the interviewee perceives different types of mental states, how he recognizes the causal relationships that exist between these mental states and an agent’s visible behaviors, and how he perceives the possibility of influencing the mental states of his peers. Internal consistency has been rated to be good. 29
The Young Schema Questionnaire-Short Form 30 is a 75-item self-report psychometric instrument for evaluating the manifestations of 15 EMS. The items are graded on a Likert scale ranging from 1 (completely false about me) to 6 (completely true about me) (describes me perfectly). Stronger manifestations of the measured EMS are indicated by high scores on a specific subscale index. The total scale’s internal consistency reliability was found to be 0.96, while the variables’ internal consistency reliability ranged from 0.65 to 0.86. 31
Complete administration of the tools was done in a single session. Unpaired t‑test, Levene’s test, and Pearson’s correlation were used to analyze the data. Confidence interval 95% and p ≤ .05 indicated a statistically significant difference between the groups.
Results
Sample Characteristics
The sample of the present study consisted of a total of 60 individuals (depression group = 30; healthy controls = 30). The mean age of individuals with depression and healthy controls was 26.64 (standard deviation [S.D.] = 8.17) and 31.07 (S.D. = 10.11) years, respectively, and the difference was not statistically significant. The mean years of education of individuals with depression and healthy controls were 16.27 (S.D. = 2.88) and 16.87 (S.D. = 2.61) years, respectively, and the difference was not statistically significant. Both groups had a significantly higher percentage of females. (Depression group = 76.66%; healthy controls = 53.33%; χ 2 = 3.59; p = .05) both groups were matched on socio-demographic variables suggesting no significant differences between the groups. Also, the majority of participants in the mild depression as compared to severe and moderate levels of depression (mild = 53.33%; moderate = 20%; severe = 26.67%).
On RMET measuring emotion recognition, the mean score of individuals with depression was 22.70, and the mean score of the healthy controls was 25.06 indicating a statistically significant difference between both groups.
On TH.O.M.A.S measuring ToM, on Scale A (I–Me) the mean scores of individuals with depression and healthy controls are 18.33 (S.D. = 6.81) and 25.10 (S.D. = 4.70); on Scale B (Other–Self) the mean scores of individuals with depression and healthy controls are 16.76 (S.D. = 5.62) and 24.00 (S.D. = 4.00); on Scale C (I–Other) the mean scores of individuals with depression and healthy controls are 13.47 (S.D. = 4.38) and 20.40 (S.D. = 2.66); and on Scale D (Other—me) the mean scores of individuals with depression and healthy controls are 13.20 (S.D. = 3.99) and 18.76 (S.D. = 2.49). The healthy controls have significantly higher means in comparison to individuals with depression on Scale A (I–Me), Scale C (I–Other), and Scale D (Other–Me) (Table 1).
Table Showing the Comparison of Means on the Emotion Recognition and ToM Between Both Groups.
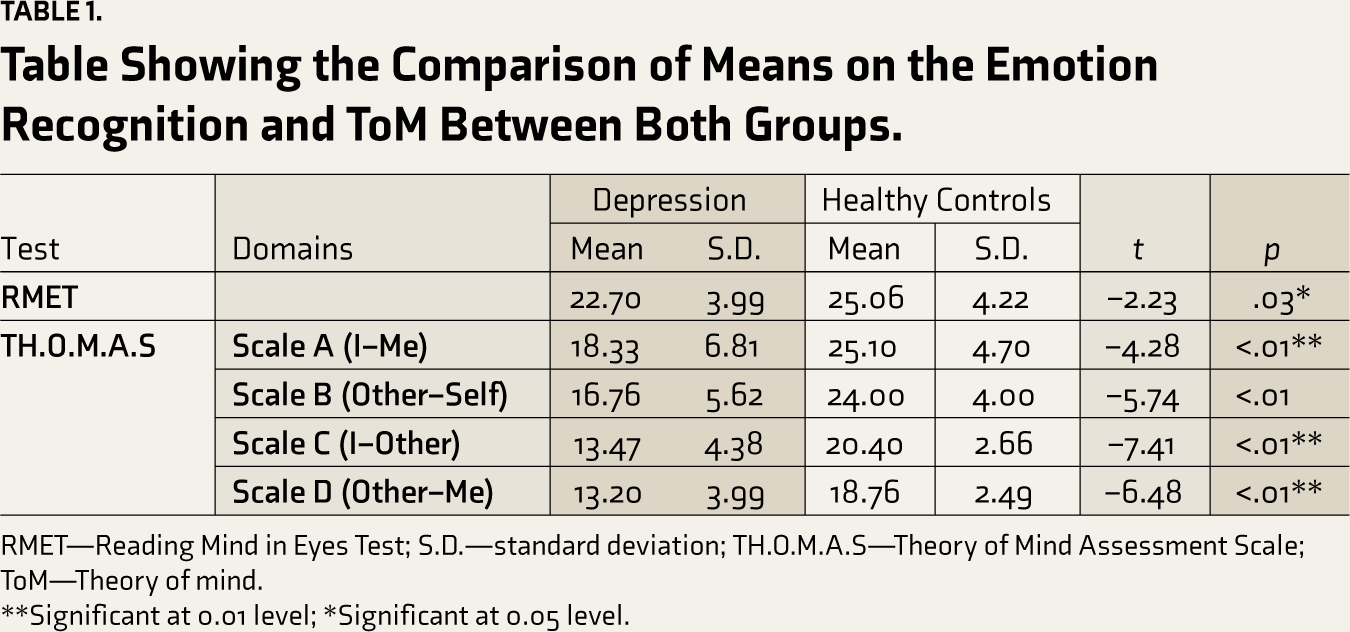
RMET—Reading Mind in Eyes Test; S.D.—standard deviation; TH.O.M.A.S—Theory of Mind Assessment Scale; ToM—Theory of mind.
**Significant at 0.01 level; *Significant at 0.05 level.
The above table shows that the following EMS: mistrust/abuse, social isolation, and defectiveness/shame have been found to be significantly correlated to emotion recognition (Table 2).
Table Showing the Relationship Between EMS and Social Cognition “(Emotion Recognition)” Based On RMET.
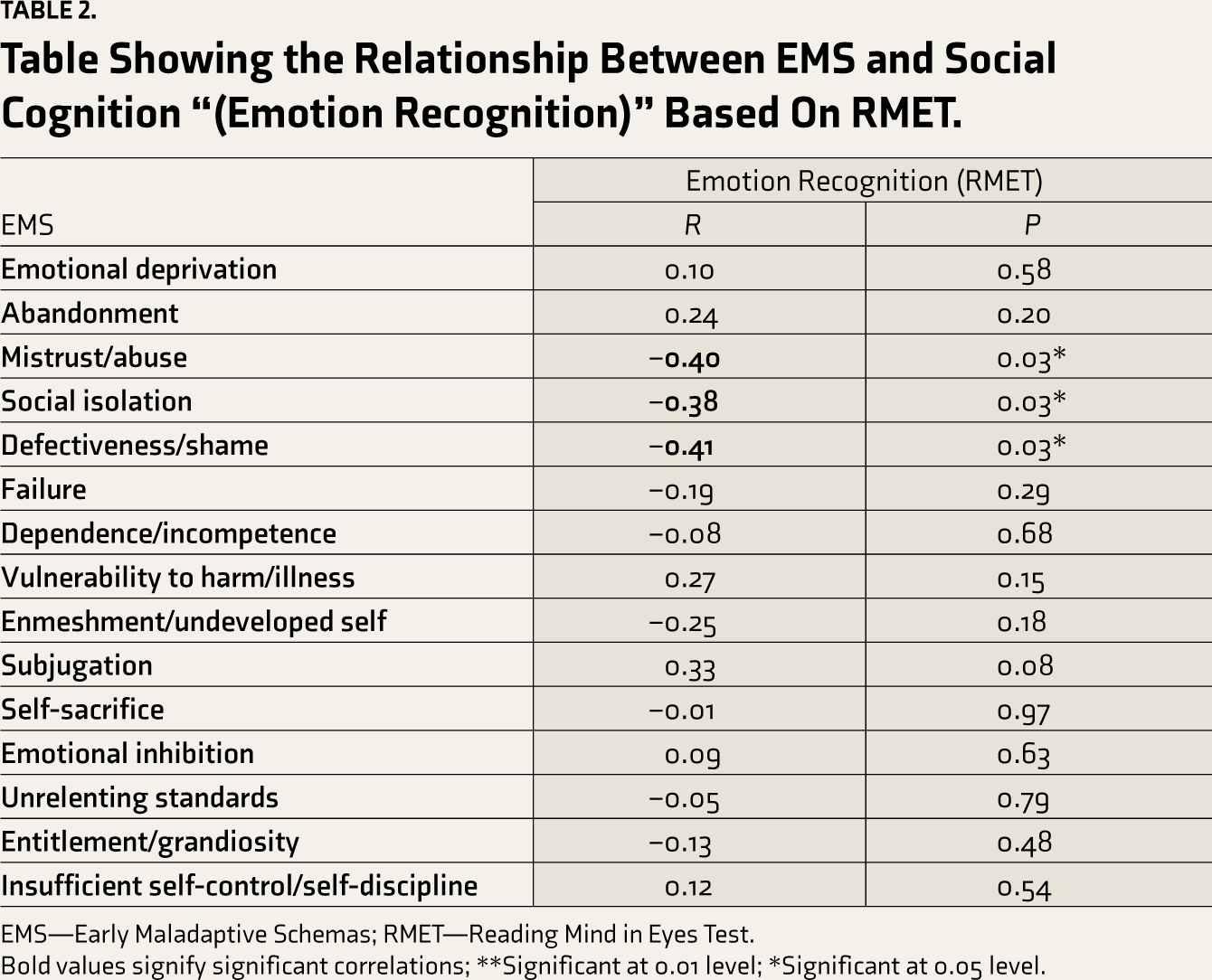
EMS—Early Maladaptive Schemas; RMET—Reading Mind in Eyes Test.
Bold values signify significant correlations; **Significant at 0.01 level; *Significant at 0.05 level.
Table Showing the Relationship Between EMS and Theory of Mind Based on THOMAS.
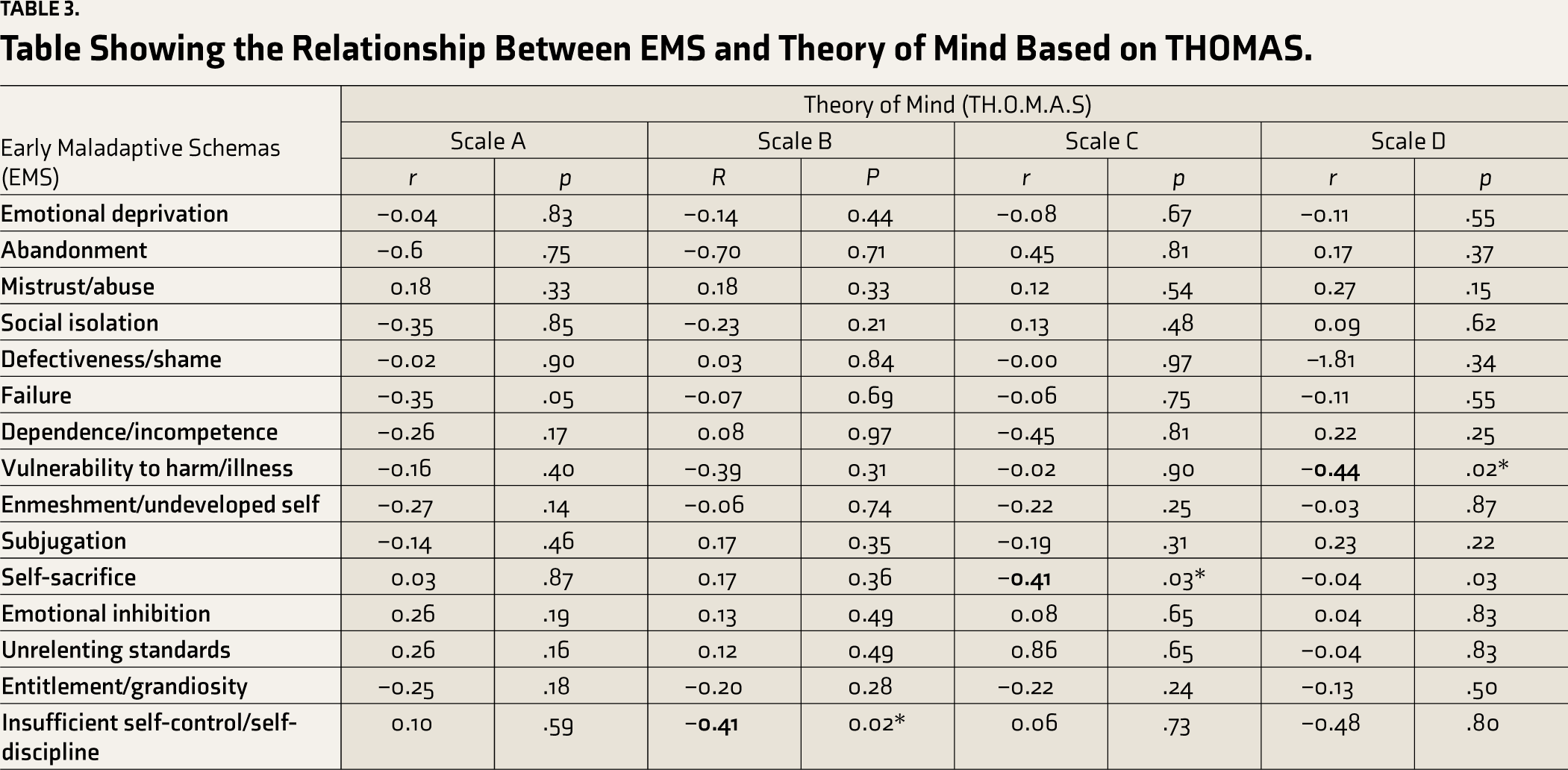
The above table shows that the following EMS: Insufficient self-control, self-sacrifice, and vulnerability to harm/illness have been found to be significantly correlated to the ToM (Table 3).
The above table shows that 41% variance is explained by self-sacrifice on ToM. It contributes negatively to I–Other domain of ToM. The above table shows that 41% variance is explained by insufficient self-control on ToM. It contributes negatively to Other–Self domain of ToM (Table 4).
Table Showing Simple Linear Regression Coefficients (Predictor: EMS; Criterion: Emotion Recognition; ToM).
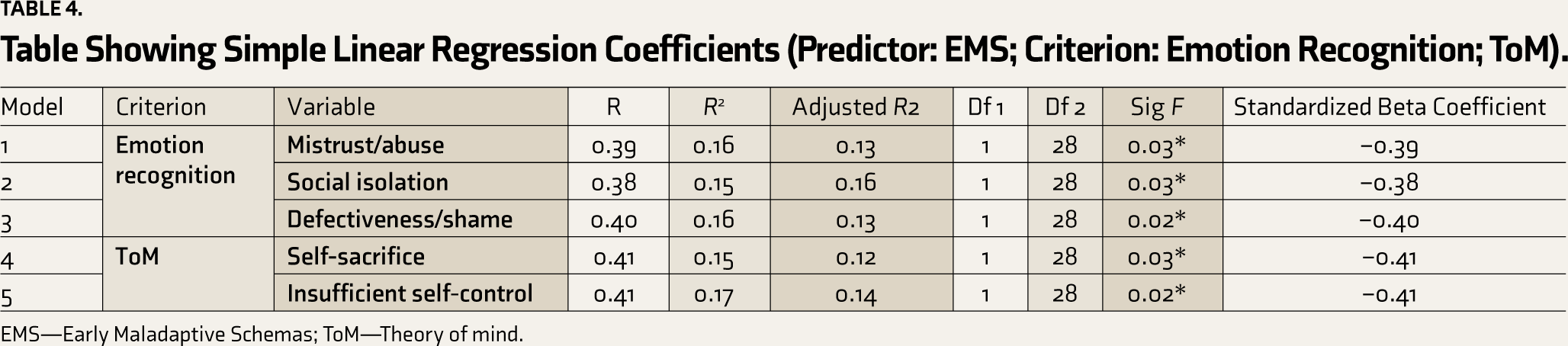
EMS—Early Maladaptive Schemas; ToM—Theory of mind.
Discussion
In recent years, depression has ceased to be regarded as a singular phenomenon. In accordance to the cognitive conceptualization of depression, 32 it is not the negative experience itself that causes depressive symptoms, but how the person interprets the event. 33 Depression is based on a concept known as dysfunctional cognition. EMS is a set of faulty cognitive mechanisms linked to depression. Environmental stressors trigger the underlying EMS, which helps organize the environment and give way to a distorted representation of reality. 34
As a result, EMS tends to have a significant effect on a person’s social and interpersonal functioning. In this regard, social cognition serves as a necessary component of interpersonal relationships and social functioning. Social cognitive deficits are believed to increase the risk of depression and the psychosocial dysfunction that comes with it. EMS can be an essential determinant of socio-cognitive abilities in depression, mediating how individuals interpret and make sense of their world, and significant others in the environment, in terms of their intentions, desires, beliefs, and other mental states.
In the present study, the association between EMS and emotion recognition has been significant with respect to schemas of mistrust/abuse, social isolation, and defectiveness/shame. Schema-level representations of human relationships are one of the central cognitive mechanisms that influence social knowledge processes regarding others’ mental states. EMS is formed during the adaptation process to a maltreating social environment, where it is necessary to observe, reflect on, and automatically identify negative social cues, as well as to learn to be alert and suspicious of neutral and positive social cues and to ignore them. With regard to Young’s theory of Schemas, 14 it is possible to hypothesize that the schemas of mistrust/abuse, social isolation, and defectiveness/shame are part of the schema domain of disconnection and rejection. Many of the core thoughts, emotions, and behaviors of depression are a part of the disconnection and rejection domain. Therefore, individuals with depression find difficulties in establishing stable and fulfilling relationships with others. All three schemas share an overarching conviction that their basic needs for security, protection, nourishment, affection, and belonging will not be met. They are more likely to misunderstand others’ motives and lack the ability to anticipate others’ state of mind, and thus their behavior. This, in reciprocal causation, may contribute to and can be, at least in part, stemming from the EMS observed in depression. The results of the study are consistent with previous research, which shows that EMS resulting from disconnection and rejection are especially linked to depression.16, 18 Linear regression analysis has shown that three domains of EMS: mistrust/abuse, social isolation, and defectiveness/shame have emerged as significant predictors of ToM: emotion recognition in depression. The prominent predictors also find major importance in social interaction as well as interpersonal relationships as they affect the processing of information of individuals. Individuals experiencing depression selectively filter corroborating information while dismissing contradictory data.20–23 The process of looking for evidence and dismissing contradictory facts helps to maintain these schemas in adulthood and relationships.
With regard to the domain of ToM the schemas of Insufficient self-control, self-sacrifice, and vulnerability to harm/illness, have been found to be significantly correlated in the current study. The schema of vulnerability to harm/illness is seen to have a significant correlation with the (Other—Me) scale, that is, the second person ToM. Individuals with depression harbor an exaggerated fear that any vulnerability of theirs might unfold at any moment and that one would not be able to cope. They in turn tend to misinterpret the intentions of others and exercise biases in that regard relating to their own well-being.
The third-person ToM refers to one’s understanding of other people’s perceptions of themselves, which is independent of the individual’s own. Third-person ToM has been found to be significantly correlated with the schema of insufficient self-control and self-sacrifice. Moreover, linear regression analysis has shown that insufficient self-control and self-sacrifice have emerged as predictors of third-person ToM (Other–Self and I other). In depression, a lack of self-control is linked to an inability to regulate their emotional expression. The use of maladaptive emotion control techniques to cope with environmental demands results in a lack of understanding of feelings, difficulties understanding them, and a reduced capacity to tolerate negative emotions, leading to increased depressive symptoms such as low mood and motivation. 35 Overall, this is how a lack of self-control will lead to a lack of comprehension of others’ perspectives. Similarly, the schema of self-sacrifice describes depression in individuals who voluntarily withhold their own needs in favor of those of others. Over-attending to other people’s needs is a strategy for projecting one’s own emotional state onto them. Due to this underlying egocentrism, other people’s perspectives are interpreted in an incorrect manner.
The findings from the present study are of much significance in understanding the dimensions of social cognition as it is still a comparatively unexplored concept with respect to depression. However, the study sample consisted of participants mostly from hailing urban, educated, and middle socio-economic backgrounds thereby restricting the generalizability of the findings. Future studies can focus on a longitudinal probe in order to see the trajectory of EMS from childhood and how it relates to the development of social cognition with age. Moreover, future research can also bring to light EMS in relation to other facets of social cognition across several clinical conditions.
Conclusion
Social cognitive deficits are believed to increase the risk of depression and the psychosocial dysfunction that comes with it. The present study findings are of much significance in understanding the different aspects of social cognition in relation to depression which is still a comparatively unexplored area of research. Moreover, previous studies have also seen the role of EMS in depression. In this regard, the present study focuses on how specific EMS can affect specific domains of social cognition in depression. The potential link between these EMS, social cognition, and depressive symptoms further suggests that the maladaptive schemas pertinent to socio-cognitive abilities may also be useful targets for early prevention and intervention efforts in depression.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.