
Abstract
Background:
Areca nut (AN) is one of the world’s most widely used drugs, especially in Asia-Pacific, causing dependence and multiple adverse health impacts. The International Agency for Research on Cancer (IARC) has classified it as a type-1 carcinogen. Despite evidence of harms, its use is culturally ingrained in many regions worldwide; harm perception is low; and the availability of intervention strategies is limited.
Methods:
To identify the range and efficacy of interventional studies on AN use cessation, a narrative review of studies published between 1990 and 2021 was undertaken using selected electronic databases (PubMed, Embase, and Scopus).
Results:
Three types of interventions were identified: educational, psychological, and pharmacological. Overall, educational interventions significantly enhanced knowledge regarding harms related to AN use. Some psychological interventions reported enhancement of motivation to quit as well as helped in reduction/cessation of AN use. Two pharmacological studies on psychiatric patients with depressive disorders and AN use found that antidepressants helped in reducing/cessation of AN use.
Conclusion:
Overall, the number of interventional studies on AN cessation is limited, and most studies have measured the short-term effects of the intervention. The role of pharmacotherapeutic interventions needs to be evaluated for AN cessation, and evidence-based psychosocial interventions need to be developed for AN cessation. Furthermore, longitudinal research using adequate sample sizes and longer follow-up durations are needed to establish interventions in this important area.
Areca nut (AN) is a widely used psychoactive substance, with millions of people consuming it worldwide. A 2002 study estimated 600 million AN users globally, with most use concentrated in the Asia-Pacific region. 1 In 2009–2010, a study by the Asian Betel Quid Consortium found that the prevalence of AN chewing varied by countries, with the highest consumption reported in Indonesia among women (47.8%) and Nepal among men (43.6%), while the rates were 10.3% in Malaysia and 2.3% in mainland China. 2 Each of these countries has varied ways of consuming AN, wherein in many places, it is eaten on its own or in combination with other ingredients. When eaten on its own, it is used in fresh or dried form, boiled, soaked, or roasted, and it may also be consumed with other ingredients such as tobacco, slaked lime, betel leaf, traditional spices, sweeteners, and other flavorings (e.g., menthol and mint). The term areca nut is often used synonymously with betel nut (BN). However, betel nut is a misnomer, though it is still a widely used term. AN is the seed of the fruit of the oriental palm areca catechu, and betel quid (BQ) generally contains betel leaf, AN, and slaked lime, and it may contain tobacco.
Indians are among the world’s largest AN-consuming populations. 3 In certain parts of India, the use of AN represents a centuries-old tradition. AN can be found in various forms, with or without tobacco, such as gutka, sweet supari, chali, paan, paan masala, mainpuri, mawa, and khara. 1 It is considered a divine fruit of God in Hindu religious ceremonies, has a significant value as a token of respect and honor, and may be used as a gift or offering during marriage ceremonies in certain regions of the country. 4
International Agency for Research on Cancer (IARC) categorized both BQ and AN (with or without tobacco) as type-1 carcinogens. 5 In particular, the IARC concluded that there is sufficient evidence that using BQ and AN without tobacco causes oral cancer, whereas using BQ and AN with tobacco causes oral, pharyngeal, and oesophageal cancers. 5 In a meta-analysis, the relative risk for oral/oropharyngeal cancer in the Indian subcontinent was 2.56 (95% CI, 2.00–3.28) for those who use BQ without tobacco and 7.74 (95% CI, 5.38–11.13) for those who use BQ with tobacco. 6 AN contains arecoline, an alkaloid that stimulates various brain receptors, promoting physical dependence. Like tobacco, AN has been associated with both stimulant and anxiolytic effects, which have been linked to the escalation of use and dependency.7,8,9 Overall, research suggests that a substantial proportion of AN users show signs of dependence. However, dependence is greater among those who use BQ and AN products with tobacco than among those who use them without tobacco.
Additionally, a systematic review found that AN affects almost all the organs in the body and can cause or worsen conditions such as myocardial infarction, cardiac arrhythmias, hepatotoxicity, asthma, obesity, type 2 diabetes, the metabolic syndrome, hypothyroidism, infertility, and adverse reproductive outcomes. 10
Despite the multiple health risks, AN use (areca with or without tobacco) remains an orphan addiction, 11 with little research and understandings. There is now a growing appreciation for the global health impact of this form of drug addiction.12,13 As western societies have in recent decades been trying to deal with tobacco use, Asian countries are now beginning to enact new public policies to deal with the public health and individual costs of AN use.10,1,12 There is a growing appreciation of the need for education campaigns and oral-health screening in AN-using communities;14,12 however, as with smoking, the comorbid health issues are best addressed by prevention of AN addiction and cessation programs. Unfortunately, for those already using AN, individual awareness of a health risk is generally not a motivation for a person to quit the addiction.15,16 Furthermore, the availability of efficacious treatments is limited, thereby providing a reason for developing targeted cessation therapies. Only recently has AN addiction been approached using the same methodology and behavioral scales as tobacco addiction research.16–20 However, aside from the identification of nicotine-like activity in arecoline, little is known about the fundamentally addictive properties of AN. 21
Thus, despite evidence of the harms and health issues related to AN, limited research is available in this area. This narrative review has been undertaken to understand the effectiveness of prevention and treatment strategies for AN use and to understand the gaps in research.
Method
We searched for literature using terms for AN/BQ (areca nut/betal quid) and related synonyms, cessation, and intervention in three databases: PubMed, Embase, and Scopus. The inclusion criteria were articles that defined interventions specifically for AN/BQ use and were published in English between 1990 and 2021. We excluded articles that focused on interventions for AN use as a component of tobacco use. Interventions that focused primarily on disease outcomes, commentaries, and review articles were excluded. Authors K.D. and S.J. reviewed the abstracts for inclusion, and after a full-text review of articles, our search revealed 13 interventions targeting AN/BQ use that fit our inclusion and exclusion criteria. The interventions were categoriZed by strategy: educational and cessation interventions (both psychological and pharmacological).
Results and Discussion
Educational Interventions
These are largely aimed at informing the target groups about the harms of AN use and the prevention of betel nut chewing. Three of these studies were school-based, and one was in an adult, high-risk refugee population. Yang et al. tested the efficacy of an educational program focused on knowledge and behaviors and aimed to improve the oral health of junior high school students in Taiwan. 22 For BQ chewing habit, a significant association was observed with common diseases in the oral cavity (odds ratio [OR]: 1.44, 95% confidence interval [CI]: 1.10–1.90, p = .009). Post-intervention, though a statistically significant decrease in tobacco use and increase in tooth-brushing frequency were observed, no significant change was demonstrated in betel nut chewing. The authors concluded that the health education program led to significant increases in students’ oral health knowledge and certain improvements in their risk behaviors.
Wang et al. assessed the effect of a preventive health education intervention to improve knowledge about, attitude towards, and practice of betel nut chewing, and self-efficacy to stop it, for school-going adolescents, in an experimental and control group design, with assessments at pre-test, post-test (14 weeks), and post-post-test (28 weeks). 23 The program consisted of 14-week classes that focused on the knowledge related to AN, its harms, and the need to quit. Significant improvements were observed in the intervention group in the attitude, practice of betel chewing, and self-efficacy to not chew betel nut, at post-test and post-post-test assessments. The study concluded that health education enables students to better resist the use of betel nuts.
A cross-sectional study by Chen et al. investigated the effectiveness of education programs for primary and secondary school students in Papua New Guinea. 24 The study was planned due to the high incidence of oral cancer in the country and the rampant use of betel nut by all age groups. The intervention focused on the knowledge, attitude, and motivation to quit. Before the intervention, knowledge about the harmful effects of betel nut was low, and there was no motivation to quit. After the intervention, knowledge increased among both groups, but reached statistical significance for secondary school students only (mean difference: 0.7 ± 0.2, 95% CI: 0.16–1.24, p = .018).
Research among a high-risk refugee population suggested that a visually guided educational intervention could enhance knowledge about harms related to betel nut/AN. 25 The study investigated the impact of an educational brochure illustrating the health risks associated with chronic BN use and information on oropharyngeal cancer among two groups: familiar cohorts and unfamiliar cohorts, based on their reported familiarity with betel nut. At baseline, in the familiar cohort, 75% recognized the harmful effects of betel nut, and 52.3% knew that betel nut alone could be a cause of cancer, as compared to 8% and 4%, respectively, in the unfamiliar cohort (p < .0001). Encouraging results were found after the educational intervention, wherein both cohorts believed that betel nut use was harmful (100%; p < .01), and 85% recognized that betel nut alone could cause cancer (p < .001).
The results of the educational interventions are summarized in Table 1.
Educational Interventions.
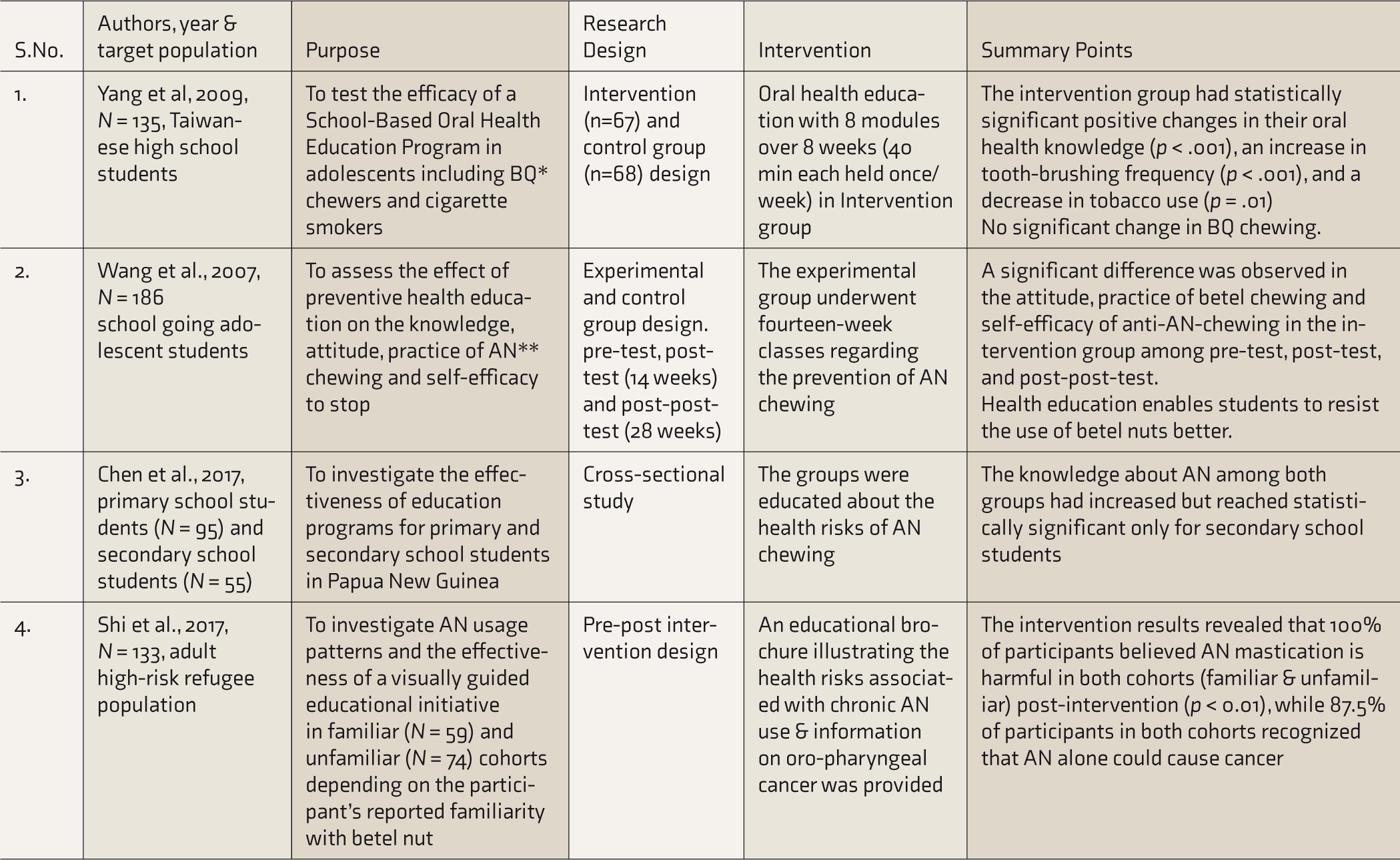
BQ, betel quid; AN, areca nut.
Psychological Interventions
Much of the research on psychological interventions for AN cessation has been modeled on the interventions that work for tobacco use disorders. In a study in Guam, betel nut chewers, like smokers, generally wanted and intended to quit but did not have specific plans of how or when they will quit. That study also suggested that betel nut chewers could benefit from cessation programs modeled after smoking cessation programs. 26 The authors tested the feasibility of a group-based cognitive behavioral program that consisted of an informational support to a group of 5–10 people who met for five 1-hour sessions over a period of 22 days. The behavioral program included identification of triggers, quit experiences and challenges faced, identifying high-risk situations for relapsing to chewing, and coping with withdrawal symptoms and urges to chew. Some suggestions that came up as a result of the study were that BQ cessation programs must be respectful of cultural contexts and also include family members in the intervention. Furthermore, public health educational material used to provide information regarding the carcinogenic effects of AN should be in the local language. This educational material may include photographs of chewers who suffer from oral cancer or dental problems. The study recommended that further research is needed with a larger sample and a control group to better establish the efficacy of the BQ cessation program it described.
Another study in Guam tested the efficacy of an intensive group-based betel nut cessation program (BENIT). The intervention comprised an intensive 22-day program covering five sessions and a 6-month follow-up session and provided social support groups, interactive discussions, and methods to quit chewing. This is an ongoing randomized controlled trial (RCT), and the results are still awaited. 27
In an RCT involving 2,140 adolescents from 26 private and public-sector schools in Karachi, Pakistan, 1,185 were placed in the intervention group and administered a behavior changing intervention (BCI), while 955 constituted the control group. 28 The components of BCI included identifying the harmful effects of SLT (smokeless tobacco) and BQ, setting a quit date, and managing craving and withdrawal symptoms. Efforts were made to culturally adapt the intervention, highlighting the harmful effects of BQ and SLT without stigmatizing its sociocultural use. Furthermore, the components of the BCI that assisted participants in changing their perceptions and/or cessation were also explored. The results indicated an increase in the intervention group’s knowledge regarding the harmful effects of SLT and BQ by 0.17 units (95% CI: 0.08–0.27, p < .001), the use perception score by 0.14 units (95% CI: 0.09–0.19, p < .001), and the quit perception by 0.07 units (95% CI: 0.006–0.129, p = .031). The BCI components that helped participants change their perceptions were identification of the product and ill effects of SLT and BQ and the preparation to quit (p = 0.024 and p = .005, respectively). The study demonstrated the efficacy of school-based interventions to curb the chewing habits of SLT and BQ in adolescents. The authors suggested that such tailored interventions may be made a part of school curricula to keep these schools free of SLT and BQ use.
In a 10-year prospective intervention study of 12,212 individuals in Ernakulam district, Kerala, India, 29 a behavioral intervention program comprising education through personal and mass media messages and an oral examination program with feedback showed that the intervention group stopped or reduced the chewing habit significantly and with a substantially higher percentage (13% vs. 4%), compared with control groups, during the first five years of the study. The decrease in the incidence of oral submucous fibrosis in the intervention group was not statistically significant, probably due to the small number of cases who developed oral submucous fibrosis.
A study in a dental clinic assessed the 3A3R educational intervention program for its effectiveness in betel nut users. 30 The 3A3R technique consisted of Ask, Advice (educating and encouraging quitting), Assess (strengthening motivation and evaluating willingness to quit), Risk (educating about the dangers of using betel nut), Relevance (making the situation personal), and Reward (educating about the benefits of quitting). Effectiveness was measured on improvements in awareness of risks of betel nut use, perceived susceptibility and severity to oral health issues including cancer, and changes in the behavior and frequency of betel nut use. Results indicated an increase in awareness of the risks, perceived susceptibility, and perceived severity of betel nut use. Around one-third (more than 32%) of the patients moved one stage forward in quitting betel nut use in one week. BN use was reduced by an average of 7.77 nuts. The study recommended the standardization and implementation of the 3A3R intervention in hospitals to help betel nut users quit.
A prospective quasi-experimental study on 827 students in Mumbai, India, aimed to understand the impact of a school-based tobacco and AN (supari) cessation intervention among adolescent students. 31 The intervention was conducted for 7th, 8th, and 9th grade students using LifeFirst, a standardized tobacco and supari cessation program conceived and implemented by the Narotam Sekhsaria Foundation, India, since 2012, which includes the delivery of six group-based education and counseling sessions by trained counselors. The program aimed at providing educational intervention to corporation-funded/managed (local government) schools in Mumbai. Intervention sessions focused on understanding the types of tobacco and supari products, associated health harms, ways of quitting, understanding craving and withdrawal, and relapse prevention and refusal skills, including activities that used role play of refusal skills for tobacco and supari products. A pre-post interventional assessment was carried out by administering a baseline questionnaire before intervention and end-line questionnaire in the last session after intervention. These questionnaires were similar, except for a section in the end-line questionnaire that assessed the students’ feedback on the LifeFirst program. A statistically significant reduction in the intervention group for tobacco and AN use (17.7% and 38.1% points, respectively) was found through the difference-in-difference estimates, as compared to an increase in tobacco use in the control group.
In another study using the LifeFirst program, a 20-week pre- and post-test quasi-experimental trial was conducted on school-going adolescents from 12 schools in Mumbai. 32 The school-based psychosocial cessation intervention program had six group sessions consisting of counseling to address barriers to quit and ways to overcome them. This intervention was added to an already existing life skills and tobacco prevention program (the components of which were awareness of harms, refusal skills, and becoming advocates for change). Six schools were randomly assigned to the intervention and the remaining to the comparison condition. The LifeFirst program aimed to assess self-reported tobacco and/or AN (supari) use and the likelihood of quitting after the provision of this add-on intervention. A 19.1% and 18.7% decrease in the intervention and comparison group, respectively, was noted for all users. While this reduction in use was significant (p < .001) within both groups, it was not significant between the intervention and comparison schools. Further results, based on the type of product used, showed a 1.7% increase for the tobacco-only users in the intervention group, which was not significant, and a significant increase of 26.2% in the comparison group (p < .001). Tobacco plus AN use showed a decline in both groups; however, AN-only use declined by 14.8% in the intervention schools and 32.7% in the comparison schools, and this difference was significant (p < .01). Thus, in the intervention group, the addition of a cessation intervention along with the life skills program appeared to have stopped tobacco-only use and not AN-only use. The main focus of a psychological intervention is to bring about behavioral change through the use of various therapies and programs. The above studies also depict different intervention plans that aim at behavior change. Table 2 summarizes the psychological interventions.
Psychological Interventions.
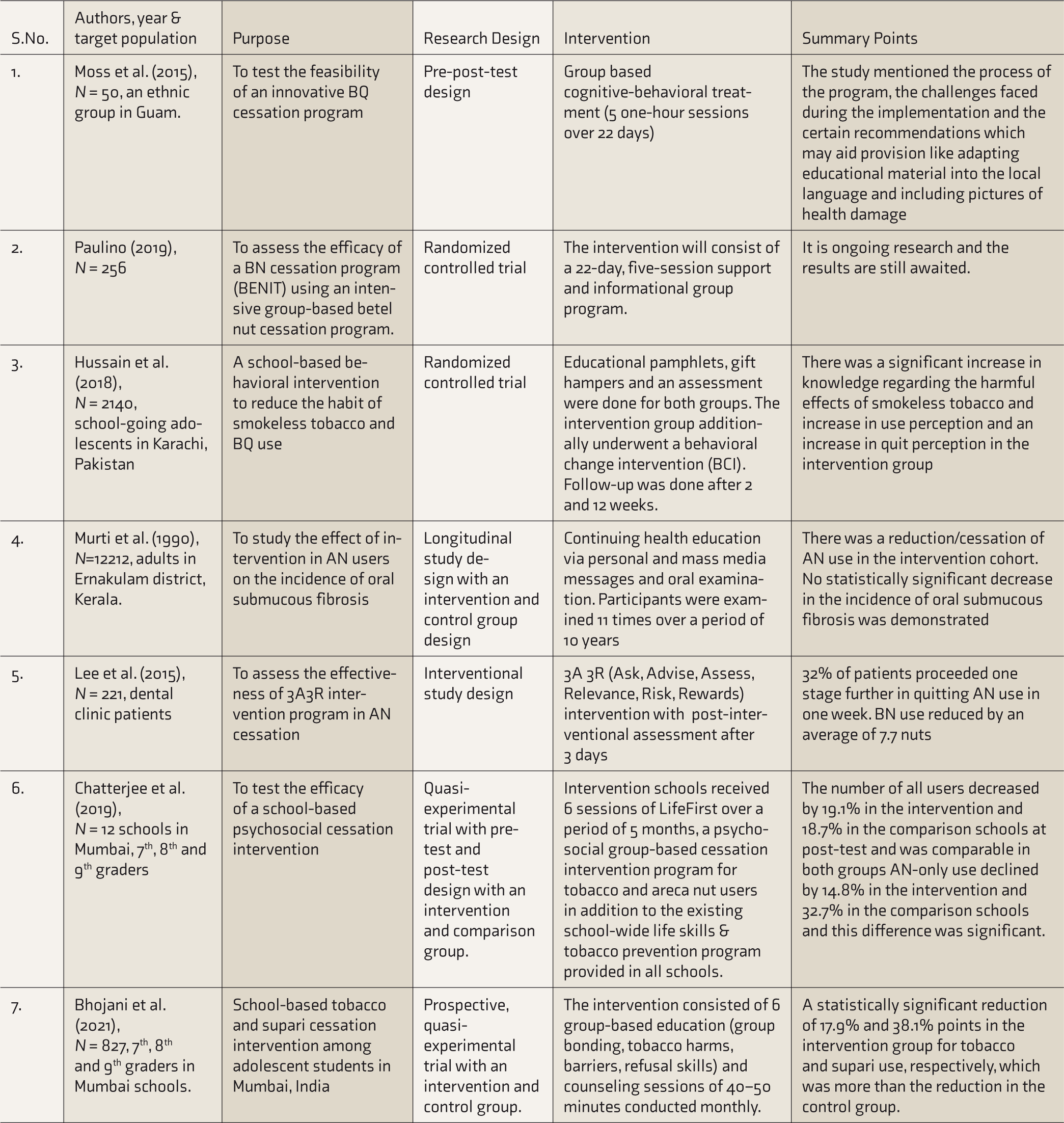
BQ, betel quid; BN, betel nut; AN, areca nut.
Pharmacological Interventions
Currently, no approved pharmacological treatments are available to help AN users quit. Two studies had evaluated the role of antidepressants in the cessation of AN. Hung et al. (2020) enrolled 204 patients with depressive disorders. Patients with depression had a higher prevalence (26%) of BQ chewing and reciprocally, patients who used BQ showed more severe depressive symptoms. 33 After antidepressant therapy, the addictiveness of BQ was significantly reduced by four times. This study provided preliminary evidence of the usefulness of antidepressants for BQ cessation. Another study by Hung et al. (2020) assessed the effects of escitalopram and moclobemide as cessation therapy in BQ disorder. 34 It was a randomized, double-blind, placebo- controlled trial undertaken in male BQ users (n = 111) to determine the efficacy of these antidepressants to help quit/reduce BQ use. Subjects were randomized into three arms: escitalopram 10 mg/tab daily, moclobemide 150 mg/tab daily, and placebo for eight weeks. The primary outcome was BQ cessation, defined as subjects who continuously stopped BQ use for ≥6 weeks. 2 (5.4%), 13 (34.2%), and 12 (33.3%) of BQ use disorder patients continuously quit BQ chewing for six weeks among the placebo, escitalopram, and moclobemide groups, respectively. Furthermore, subjects on escitalopram and moclobemide treatments exhibited a significantly lower level of BQ intake at the 8th week compared to those on placebo.
Table 3 provides a summary of these two studies. No other pharmacological interventional studies for AN were identified, although a researcher postulates the potential role of nicotine gum with pilocarpine for the treatment of AN disorders. The rationale given for nicotine gum was that AN’s active ingredient, arecoline, acts on the same receptor proteins in the brain as nicotine, and hence nicotine gum would help reduce cravings for tobacco while the pilocarpine potentially would recreate the BQ’s salivation experience. 35
Pharmacological Interventions.
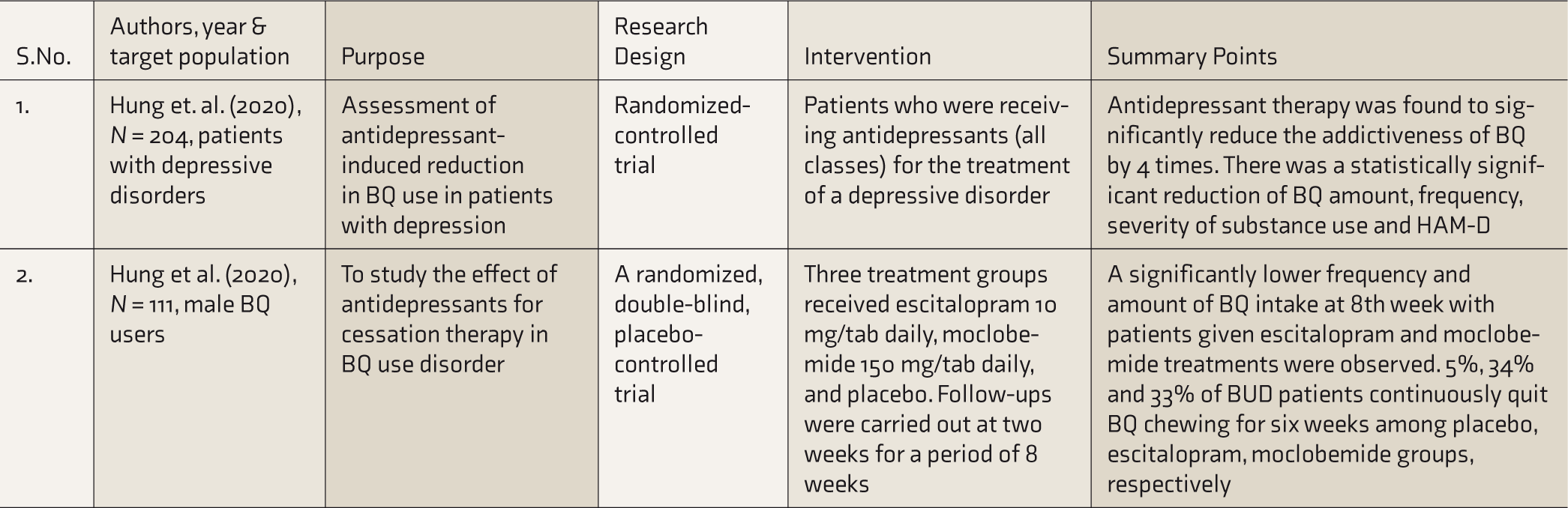
BQ, betel quid; BUD, betel quid use disorder.
Conclusion
A number of articles were reviewed to understand the current status of the effectiveness of the intervention plans related to AN/BQ cessation. Educational interventions focused on prevention and provided knowledge related to the harms and effects of betel nuts/ANs, aimed at enhancing awareness related to them and motivating participants to quit. These educational interventions seemed to have a positive impact in increasing awareness of the people regarding the health effects of AN use, showing statistically significant increase in the knowledge and harm perception related to AN use. One study also showed that health education enables students to better resist the use of ANs. 23
Psychological interventions included were mainly group-based, using techniques like cognitive behavior intervention, culturally tailored behavior change interventions (BCI), 28 and 3A3Rs intervention, 30 and many of these techniques were adapted from smoking cessation programs. One study also evaluated the feasibility of providing psychological intervention. 26 Two Indian studies31,32 developed a school-based psychosocial cessation intervention plan to reduce AN intake among school children. Most studies demonstrated an increase in awareness related to the harms of AN, motivation to quit, and a reduction in AN use.
There were only two studies33,34 pertaining to pharmacological intervention. Both were RCTs where antidepressants were used in patients with depressive disorders who were also using AN. A statistically significant reduction in the frequency and amount of AN consumed by the patients was demonstrated in the intervention arm. Since both these studies were RCTs, they provide initial evidence of efficacy of pharmacological treatment in AN use disorders in patients with depressive disorders.
In conclusion, limited interventional research has been carried out for AN use cessation. Most studies evaluated end-of-treatment or short-term treatment outcomes. All studies used self- report measures to assess the reduction/cessation of AN use. No biochemical confirmation of abstinence was done. Paulino et al. 27 propose to measure cotinine and AN biomarkers in saliva samples, but this study’s results are awaited. Pharmacological intervention was done using antidepressants in patients with depressive disorders who were also using ANs. Hence, the results of these studies have limited generalizability.
Nevertheless, the findings of these studies are encouraging and pave the way for further studies. The components of psychological intervention that work for AN cessation need to be evaluated. Longitudinal studies with adequate sample sizes and longer term follow-up periods with biochemical measures of abstinence need to be carried out. The role of pharmacotherapeutic interventions needs to be evaluated for AN cessation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.