
Abstract
Background:
Tobacco use contributes to almost 40% of the cancers in India. Considering the potential threat, many preventive measures have been instigated in the country. However, tobacco cessation for hospitalized cancer patients is an unexplored territory in India. This study aims to understand the quit status and to explore the reasons to quit or continue the use of tobacco after the diagnosis of head and neck cancer (HNC).
Methods:
HNC patients admitted between February and April 2016 were assessed for their tobacco use status. A DT was used to assess the psychological distress. Users were assessed for their readiness to quit and dependence on tobacco. An in-depth interview was conducted among 25 patients (seven current users and 18 recent quitters), and themes that emerged were discussed.
Results:
Of the 119 HNC patients, 71 were tobacco users and 48 had quit tobacco after the diagnosis. The reasons to quit were the perceived benefits of quitting, advice from the physicians, and awareness about cancer and its association with tobacco. In contrast, the reasons to continue the use of tobacco were attributed to coping mechanisms, nihilistic perception about the outcome of the cancer, and a lack of understanding about cancer and its association with tobacco.
Conclusion:
The recent quitters comprehended the benefits of quitting and were able to prioritize their needs after the diagnosis. However, one-third of the HNC patients continued to use tobacco even after the diagnosis of cancer. Hence, tobacco cessation services need to be integrated into oncology services for achieving better treatment outcomes.
A better understanding of the current users’ and recent quitters’ attitudes, behavior, and perception about tobacco and its association with cancer would help in designing effective tobacco cessation interventions for hospitalized cancer patients.Key Message:
Continued use of tobacco after cancer diagnosis reduces the overall treatment efficacy, quality of life, and survival period. It also increases the risk of surgical complications, weight loss, and aggravation of chemo-induced side effects, including skin and oral mucosites.9–11 Cancer patients who continue to use tobacco also experience depression, severe fatigue, and decreased pulmonary and immune functions.12,13 Hence, assisting tobacco users to quit after a cancer diagnosis is of paramount importance in enhancing the quality of their lives.
The need for tobacco cessation in the primary prevention of cancer is well established. However, there is a dearth of research in the area of the tobacco users’ perception, knowledge, behavior, and attitude about the association of tobacco and cancer in the Indian context. 14 This mixed-method sequential explanatory study assessed the quit rate of tobacco users and explored the reasons for quitting and continuing tobacco usage among HNC patients after the diagnosis. Exploring the reasons for quitting or continuing the use of tobacco would help in designing tailor-made tobacco cessation interventions among cancer patients in India.
Materials and Methods
Participants’ Recruitment
The study included HNC inpatients who had a history of tobacco usage and were admitted in a tertiary cancer center in South India for treatment with curative intent, between February 2016 and April 2016. Patients who were above 25 years of age and could converse in Tamil or English were included, irrespective of their education, gender, socioeconomic status, and occupation. Purposive sampling was used, and participant recruitment for the qualitative study was not based on data saturation. This study was approved by the ethics committee of the center. Prior written informed consent was obtained from all participants.
A list of patients with history of tobacco use was prepared based on the hospital records. The patients were then approached and asked about their current tobacco use. For patients who confirmed having quit tobacco, the quit status was confirmed from caregivers and hospital staff. The patients were then categorized as current users (who continued tobacco use after diagnosis and during treatment) and recent quitters (who quit tobacco use immediately after the cancer diagnosis and continued the quit status until the time of the interview).
Tools Used
All patients were initially screened to measure their psychological distress using a Distress Thermometer (DT) developed by the National Comprehensive Cancer Network (NCCN). 15 The DT is a self-report tool where cancer patients are asked to rate their overall distress on a scale of zero (no distress) to 10 (extreme distress). Additionally, the current tobacco users were assessed using the Fagerstrom Test for nicotine dependence 16 (smoking and smokeless), which is a questionnaire used to assess the level of nicotine dependence, and Readiness to Quit Scale, 17 which is a questionnaire to measure the “stages of change” in a tobacco user.
To explore the reasons to quit or continue tobacco use, a semi-structured interview was conducted by the principal investigator who is an MPhil scholar with a master’s degree in psychology and is trained in qualitative research methods. For semi-structured interviews, participants were enrolled based on in-person interactions. The researcher did not have a prior relationship with the study participants, and no one besides the researcher and the participant was present during data collection. The questions to guide the semi-structured interview were generated based on informal discussions with tobacco-related cancer patients admitted to the ward by the first author before the study. The questions were identified and pretested for their relevance, appropriateness of wording, and clarity. The questions were translated into the regional language (Tamil). The following lead questions were asked, and further probing was done based on the responses, to have an in-depth understanding about the reasons.
What are the reasons to continue or quit tobacco use after the cancer diagnosis?
Can you briefly tell me about your understanding of tobacco and its association with cancer?
Data Analysis
The quantitative data for the Fagerstrom Test for nicotine dependence (smoking and smokeless), the Readiness to Quit Scale, and the NCCN DT were summarized using descriptive statistics. Field notes were made after the semi-structured interviews were conducted by the researcher. Each interview lasted 15–20 min. The audios recorded in the semi-structured interviews were transcribed in Tamil and then translated to English by experts. Themes were identified based on thematic analysis developed by Braun and Clarke. 18 To gain systematic and meaningful data, two experts were asked to code the raw data independently. After the coding process, differences in interpretations were resolved through discussions with two other experts, who then sorted the code into potential themes. All the themes were made up of different subcodes, of which some initial codes were generated to form the main themes, and others were generated to form the subcategories. Codes with similar meanings were grouped together. The researchers and qualitative experts refined the themes that emerged for coherency and examined the relationship between them. A psychologist and a psycho-oncologist with prior experience in qualitative research and no other involvement in the study performed an independent review of the analysis, critically read the transcripts, explored the themes, and analyzed subsets of the raw data for further validation of the findings. The study findings are reported based on the recommendation of the 32-item checklist of the consolidated criteria for reporting qualitative research (COREQ) 19 for conducting interviews.
Results
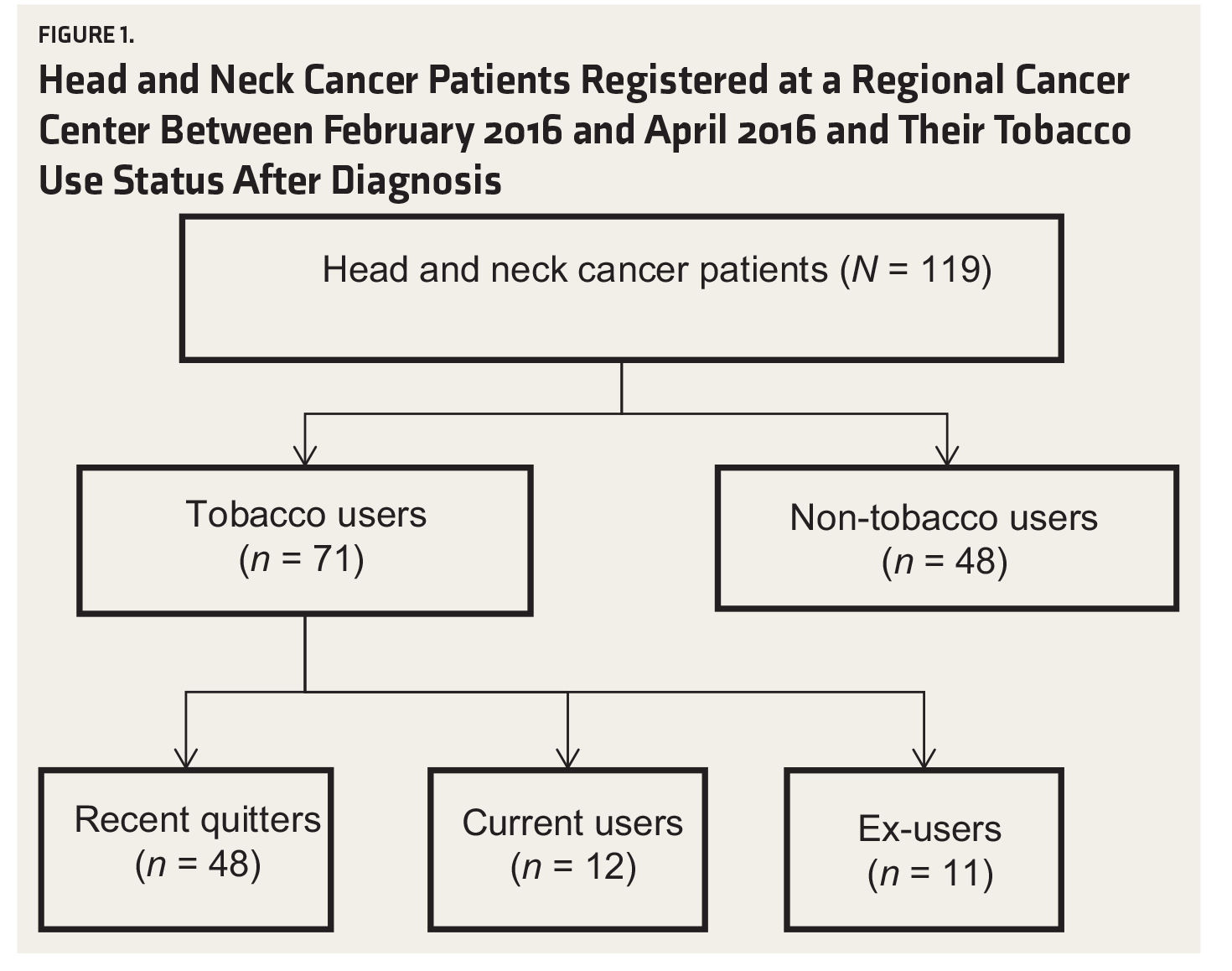
A total of 119 HNC patients registered during the study period, out of which 71 were tobacco users as found in the medical records (Figure 1). Out of the 71 patients, 48 (68%) were recent quitters (quit immediately after diagnosis), 12 were current users, and 11 reported that they had quit tobacco prior to the diagnosis of cancer.
Head and Neck Cancer Patients Registered at a Regional Cancer Center Between February 2016 and April 2016 and Their Tobacco Use Status After Diagnosis
Among the 48 recent quitters, 28 could not be included in the study due to the following reasons: difficulty in speaking (n = 5), palliative treatment (n = 6), language barriers (n = 7), Ryle’s tube insertion and longer stabilization time (n = 2), unwillingness to participate (n = 2), and administrative reasons (n = 6). Eventually, 20 recent quitters (age range, 29–65 years) consented to give an in-depth interview. As two of the audio recordings of patient interviews lacked audio clarity, only 18 interview transcriptions were included for analysis.
Among the 12 current users, only seven consented to participate in the study, whereas the other five refused to participate due to lack of motivation and fear of exposing their continued tobacco use to the family members.
Demographic, Clinical Characteristics, and Distress Level of Head and Neck Cancer Patients Using Tobacco
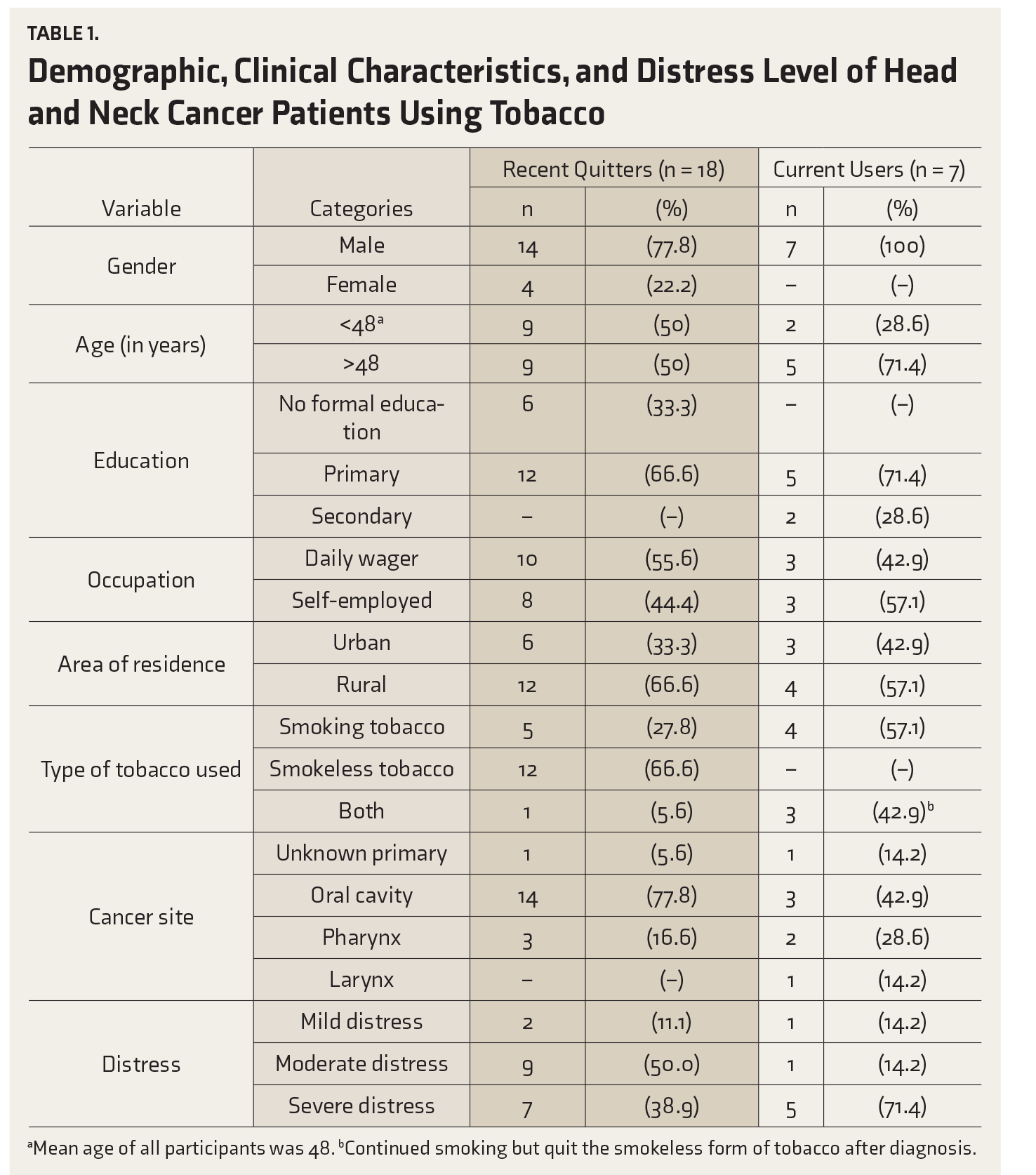
aMean age of all participants was 48.
bContinued smoking but quit the smokeless form of tobacco after diagnosis.
With Fagerstrom Test for nicotine dependence, the severity of the nicotine dependence was found to be very low in five of the current users, while the remaining two had medium severity. All the seven of them were in the precontemplation stage (readiness to quit). Five of the current users were severely distressed (NCCN DT), whereas the 16 (89%) of the recent quitters were moderately or severely distressed.
Themes That Emerged Among Current Users
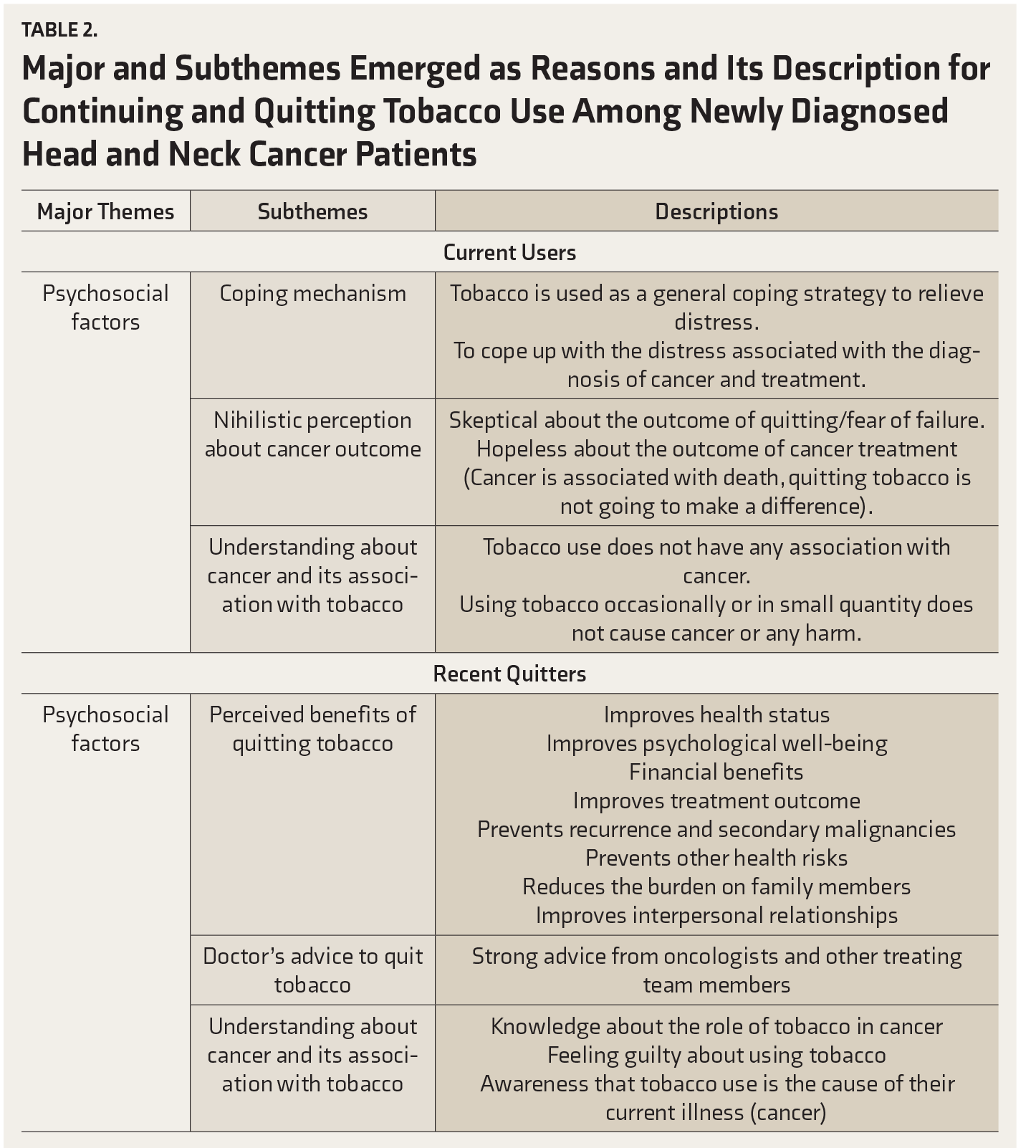
The themes that emerged among current users (Table 2) were using tobacco as a coping mechanism to relieve the psychological distress associated with cancer and treatment, hopelessness about the outcome of cancer and its treatment, and a lack of understanding about cancer and its association with tobacco.
Major and Subthemes Emerged as Reasons and Its Description for Continuing and Quitting Tobacco Use Among Newly Diagnosed Head and Neck Cancer Patients
1. Coping mechanism
Current users reported that they use tobacco as a coping strategy in general to relieve stress and that they continue to use tobacco to cope with the current distress associated with cancer diagnosis and treatment.
“It’s all because of stress…for getting relief from stress and to feel good…. Yes, I do have difficulties and family problems, and to get rid of those thoughts, I smoke….”
(Current User Participant No: 01).
2. Nihilistic perception about cancer outcome
Some patients did not perceive any added benefit in quitting at this stage, as they thought that the damage was already done. Despite the assurance of the treating oncologists about a possibility of cure, they were skeptical about the outcome of cancer and its treatment. They strongly believed that quitting tobacco at this stage cannot improve one’s health and that death is inevitable after being diagnosed with cancer. This sense of hopelessness was a major deterrent in the case of current users’ decision to continue with tobacco use.
“What I think is that I have got cancer, and nothing can be done at this stage. I am in this condition. So I do not know what to do…. I am continuing because everything is over anyway….”
(Current User Participant No: 04)
3. Understanding about cancer and its association with tobacco
Current users disputed the fact that “tobacco causes cancer.” They brought up real-life examples of those people who had cancer despite having clean habits and those who never had cancer despite heavy and prolonged tobacco usage. Current users raised these real-life examples in their defense to continue with the use of tobacco even after cancer diagnosis. They believed that the current illness was not associated with tobacco and, therefore, continued to use it.
“There are so many people who smoke, and they don’t get any disease. I smoke only occasionally, but I got cancer. I don’t know which one is to blame: the cigarettes or the disease….”
(Current User Participant No: 02).
Current users believed that smoking one or two cigarettes a day might not be harmful.
“When I started, I was thinking what big deal is going to happen…. Now it has become a habit, and smoking one or two cigarettes in a day is not a big deal….”
(Current User Participant No: 05)
Themes that Emerged Among Recent Quitters
The themes that emerged among recent quitters (Table 2) were perceived benefits of quitting tobacco, doctor’s advice to quit tobacco, and understanding about cancer and its association with tobacco.
Perceived benefits of quitting tobacco use after diagnosis
Recent quitters believed that quitting tobacco might improve their health status. Tobacco use further caused pain and irritability in the affected site and prevented them from using tobacco.
“I have quit only after experiencing pain. I have pain in my tongue. Whenever I eat spicy food or I put pan, I experience a burning sensation and due to that, I have quit….”
(Recent Quitter Participant No: 06)
The recent quitters felt an improvement in their psychological well-being after quitting.
“Now I am healthy. Feeling good and strong…. Initially, it was difficult even to walk…. Now I can walk better….”
(Recent Quitter Participant No: 03)
Recent quitters believed that the price of tobacco products was too high and that they should rather save money for their treatment instead of spending it on tobacco.
“First, to begin with money, 2000 rupees per month can be saved…. I can use it for my treatment….”
(Recent Quitter Participant No: 03)
Recent quitters were concerned about the outcome of the cancer treatment and recurrence, and they associated the current illness with tobacco. They believed that continuing tobacco use might lead to poor prognosis and recurrence.
“I have to stop…. After being diagnosed with cancer, I should stop…. If I continue to use, I think my disease will come back…. I don’t want to suffer any more…. By merely thinking about the disease, I’m scared…. When I came to know about the diagnosis itself, I was shocked…. If I don’t quit, the disease might spread further and endanger my life….”
(Recent Quitter Participant No: 08)
Recent quitters associated tobacco not only with cancer but also with other noncommunicable diseases, and the knowledge was attributed to media campaigns.
“Didn’t see any risk, might get cancer, might get some problem in the lungs or heart because of tobacco…. The juice from tobacco gets deposited in the lungs. They show on TV also…. They trap it in bottles and show…. There is a fear that something like that might come….”
(Recent Quitter Participant No: 01)
Commitment to the family too was a motivating factor to quit.
“If I were alone, then fine. But I must take care of five people. I know that I have got the disease. I have got two kids, my wife, and my parents. Hereafter (pause), if I continue again, it’s over….”
(Recent Quitter Participant No: 10)
“My wife suffers a lot. She doesn’t tell me. But I feel guilty. I am not even able to face her. Why have I got cancer? It is because of this.”
(Recent Quitter Participant No: 05)
Recent quitters believed that quitting tobacco would bring in happiness among their family members.
“My relatives had always asked me to stop this habit, but I never listened to them. Whenever they say anything related to smoking, I tried to avoid them. This had created a lot of indifference amongst us. Now they are happy because I have stopped this habit….”
(Recent Quitter Participant No: 17)
Doctor's advice to quit tobacco
Some of the recent quitters had quit because of repeated and consistent advice received during their hospitalization from oncologists and other health care professionals.
“Yes…Doctors have advised me…. They said that only after quitting this habit will they be able to cure the disease or else it will be growing and lead to bigger issues…. That’s why I decided to stop the habit….”
(Recent Quitter Participant No: 13)
Half of the HCN patients who quit after cancer diagnosis experienced withdrawal symptoms in the first week following cessation. The common withdrawal symptoms were craving, irritability, anger, and headache. But these patients adopted several coping strategies that they had learned from the doctors to abstain from the habit.
“I used clove whenever I had craving…. But gradually, I have reduced, and I quit the habit…. Now I feel relieved….”
(Recent Quitter Participant No: 03)
“Whenever I have such thoughts, I use cinnamon or dry grapes…. Then such thoughts won’t recur immediately…. Even sweets are effective.”
(Recent Quitter Participant No: 02)
“That’s what, it would be slightly difficult. It is irritating, I have felt like I have lost something. Still, when we think about our family, we get the confidence…. When I have such thoughts, I would drink water, iced water, or juice. In the evenings, I would take tea or milk with some biscuits.”
(Recent Quitter Participant No:10)
3. Understanding about cancer and its association with tobacco
Prior to the cancer diagnosis, the recent quitters were well aware about the strong association of cancer with tobacco usage. The diagnosis further strengthened their credence and made them feel guilty of their behavior, leading to quitting the use of tobacco.
“I quit the habit only after the cancer was diagnosed on my tongue…not before that….”
(Recent Quitter Participant No: 07)
“Our sins will not leave us alone. What we sow, so shall we reap. I have got cancer. I got it because of the mistake I made. I have reformed. But, I do have to pay for the sins I have already committed. So, God has given me cancer. That is how I feel. It was difficult, but I was not angry. I generally don’t feel much anger….”
(Recent Quitter Participant No: 05)
“Whatever is bad for health, I have used it all my life and it has been the cause of my cancer…. So, I feel very angry looking at my own self…. I have spoilt my own health….”
(Recent Quitter Participant No: 13)
No patient in the study group received any special intervention from professionals to quit tobacco, apart from simple advice from oncologists and nurses.
Discussion
This study added new knowledge in understanding the tobacco cessation status among newly diagnosed HNC patients and the reasons associated with it. The quit rate was observed to be 67.6%. The self-reported quit rates among cancer patients were reported as 83% 20 and 65% 21 in earlier literature, in line with the current study. Previous studies22–24 have reported that demographic variables such as gender (male), socioeconomic status (low), and education (low) play a vital role in continuing tobacco usage after a cancer diagnosis. Because of the small sample size, we were unable to perform further analysis to see if our sample had findings similar to those of the previous literature.
All smokeless tobacco (SLT) users in our sample had quit their habit. This could be due to the treatment-related side effects and the inability to use SLT. While undergoing radiation therapy, patients often experience symptoms such as mucositis and pain. Patients who quit because of side effects might resume tobacco usage once the symptoms disappear. 21 However, in a previous study, the quit rate was found to be low among SLT users due to the high level of nicotine dependency. 25 During in-depth interviews, our patients reported having a burning sensation at the cancer site. This had also prevented them from taking their regular diet during such times. Further exploring this might give a better understanding of whether their quitting is temporary due to the side effects or is it because of the correct understanding of the ill effects of tobacco usage.
In this study, 71.4% of the current users experienced severe psychological distress after cancer diagnosis, as compared to 38% of the recent quitters. Although the current users experienced severe distress, none of them were clinically depressed in this study. It has been established that cancer patients experience severe psychological distress from the time of diagnosis to the completion of treatment.26–28 As supported by the qualitative findings of this study, distress could be the reason for not being able to quit this habit. A majority of our patients reported a lower level of nicotine dependence and still found it difficult to quit. A systematic review had concluded that stress is one of the factors that lead to continued tobacco use. 14
All current users were in the precontemplation stage and, hence, they had low awareness, whereas the recent quitters were well-aware of its association with cancer. A low quit rate among tobacco users who were in the precontemplation stage has also been found in other studies. 29
Reasons to Quit or Continue to Use Tobacco
Users who continued to use tobacco after cancer diagnosis did so because of higher psychological distress and this outweighed the benefits of quitting. The current users were unconvinced that even moderate smoking posed health risks. There are similar studies attributing low awareness on the health risks associated with tobacco use as the reason for cancer patients’ lower motivation to quit the habit.30–34 Although advancement in treatment resulted in improved quality of life, the current users perceived that cancer has no cure and that death is inevitable even though they were under treatment with curative intent.
Furthermore, many current users believed that tobacco consumption did not cause cancer. In order to support their claims, they cited examples of people around them who smoked tobacco for their entire lifetime and were still cancer-free. On the other side, they also cited examples of many nontobacco users who were diagnosed with cancer. In fact, some current tobacco users were of the opinion that continuing tobacco use would improve their overall physical condition and that quitting would damage their psychological well-being. Consistent with previous studies,35 heightened psychological distress and constant worry about the future of their families detracted the patients from their frail aim to stop tobacco use. Hence, many of the current users continued to use tobacco after the diagnosis as a coping strategy.
The recent quitters experienced feelings of guilt and censure, which led to tobacco cessation. This finding is consistent with other studies where recent quitters claimed that their cancer was a result of God’s anger and punishment for their bad habit of using tobacco. Family support had also played a strong predictor of tobacco cessation.36–38
A majority (n = 13) of the quitters perceived that continued use of tobacco would aggravate the pain at the cancer site and increase the chances of secondary cancers. They also feared the stigma of death by cancer and were willing to take any measures to avoid it. The recent quitters were convinced that the benefits of quitting outweighed the potential threat of tobacco use at this stage. They perceived that quitting would improve the treatment outcome and cancer prognosis, and enhance their psychological well-being.
No patients received specialized tobacco cessation intervention to quit tobacco, although some recent quitters reported that their physician’s advice was a motivating factor. Advice and tips provided by doctors and other health care professionals on managing withdrawal symptoms have been found to be effective in helping patients to quit tobacco usage. 39 Hence, it is essential to offer cessation support to all tobacco users who are diagnosed with cancer, as it is difficult for them to quit on their own. 40
Strengths and Limitations
This study was conducted in a single tertiary cancer center, because of which its findings cannot be generalized. The small sample size limited the ability to perform inferential statistics to determine the association of tobacco quitting with the stage of change, level of nicotine dependence, stress, and demographic characteristics. While the recent quitters had reached data saturation, the current user group was not able to meet the same, which is another limitation of this study. Further studies can be conducted to explore these aspects. The quit rate was based on the self-report. Although the author took efforts to confirm the quit rate through surrogate measures, there are chances that the patients might have used tobacco without the knowledge of caregivers and hospital staffs. The quit status was not confirmed using any biomedical assessments such as urine cotinine. Moreover, all study participants were admitted to the hospital and were under treatment. The hospital has a tobacco-free policy, and patients and visitors were not able to use tobacco within the campus. Also, the patients might have had side effects associated with treatment. This would have restricted them from using tobacco apart from the reasons reported by them. These aspects were not explored in the study.
The strengths of the study are as follows: firstly, it is a mixed-method sequential explanatory study, and, secondly, it adds new knowledge to the field of oncology in the Indian context as no study has been conducted in this area so far and to best of our knowledge.
Conclusions
“Cancer cures smoking,” the often-said statement, was disproved in this study, as a substantial proportion of patients continued tobacco use after the cancer diagnosis, indicating the need for tobacco cessation services at oncology settings.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.