
Abstract
Background:
Older adults with serious mental illness (OASMI) have to manage the twin challenges of old age and mental illness. Understanding their characteristics will help policymakers and researchers plan tailored interventions. The profile of OASMI is not described in any publication from India, and this paper addresses that gap. The information from this study will serve as a baseline for the planned periodic follow-up of the study participants.
Methods:
This study employed a cross- sectional design among a sample of OASMI identified through multistage cluster sampling from three districts in Kerala. We interviewed them in their households and collected sociodemographic data using a pretested tool.
Results:
Among the 917 OASMI participants, 66% were females, 18% were the ‘oldest-old’ (≥80 years), 94.1% were unemployed, 51.7% were socially backward, 68.5% were financially weak, 10.1% were living alone, 59.4% were living without partners, and 63.7% had caregivers.
Conclusion:
Compared to the general population of older adults in Kerala, the OASMI have poorer socioeconomic status and higher rates of social isolation, and males are dying earlier. The profile of the OASMI depicts their multiple vulnerabilities and the need to address those.
Keywords
Older adults with serious mental illness in Kerala have poorer socioeconomic status and higher rates of social isolation, and males are dying earlier compared to the general population of older adults in the state. Their profile depicts multiple vulnerabilities and stresses the need to address those.Key Messages:
With increased life expectancy, the proportion of older adults is growing in India. 1 A person aged ≥60 years is considered a “senior citizen” or “elderly” in the country. 2 The National Statistical Office (NSO) predicted India’s older adult population would increase by 41% over this decade (2021–2031), from 138 million to 194 million. 3 The proportion of older adults was expected to rise from 8.6% in 2011 to 10.1% in 2021 and 13.1% in 2031. Kerala has the highest proportion of older adults (16.5%) among the states, and an estimated increase to 20.9% is predicted by 2031. 3 The Census of 2011 showed the overall old-age dependency ratio in Kerala to be 19.6%, 4 and the NSO has projected it to ascend to 34.3% in 2031. Compared to males, the female old-age dependency ratio is also high in Kerala.
Aging is associated with physical frailty, reduced mobility, chronic conditions requiring long-term care, solitude, drop in socioeconomic status, etc. 5 Spouses of older adults who may have been caregivers might have passed away, maybe disabled themselves, or perhaps be dealing with age-related problems. Children may have migrated in search of better prospects, alienating and isolating the aged persons. Serious mental illnesses (SMI) are “mental, behavioural, or emotional disorders resulting in serious functional impairment, which substantially interferes with or limits one or more major life activities.” 6 A modest 1% estimated prevalence of SMI among older adults translates to nearly 2 million older adults with SMI in the country by 2031. Patients with SMI suffer functional disabilities almost throughout their life. The challenges of old age further compound the problems faced by SMI.
Sociodemographics refers to social and demographic factors that define people in a specific group or population. 7 The framework for measuring health information by the Health Metrics Network, cited by the WHO Mental Health Gap Action Programme (mhGAP) categorizes essential information required for planning a health intervention into three categories. Sociodemographics is one of the two items listed under ‘The Determinants of Health’. 8 Although some studies and government reports have described the sociodemographics of Indian older adults, 9 the profile of the Older Adults with Serious Mental Illness (OASMI), who forms a subsection, has not been described previously. Understanding this component is vital for planning and delivering healthcare interventions.
The SENIOR (Support Systems Evaluation of Neuropsychiatric Illness in Old age) research project evaluated the problems OASMI in Kerala faced in obtaining mental healthcare. The sociodemographic characteristics of the participants of the SENIOR project described in this paper could be helpful for policymakers and researchers planning interventions for OASMI.
Methods
The detailed methodology of the SENIOR project has been published as a protocol article. 10
Study Design
This study conducted among OASMI was cross-sectional in design. Our participants were those aged ≥60 years who had been identified with SMI and/or moderate to severe dementia by Accredited Social Health Activist (ASHA) workers using a screening tool and confirmed through interviews by the project research fellows. Schizophrenia-spectrum disorders, bipolar disorder, and severe depression were the SMIs captured. Although the focus of our study was SMI, dementia was also considered, as it is prevalent in old age and its symptoms often overlap with those of mental illness. Participants with dementia alone (without SMI) formed only a minor share (3.5%) of the participants in our study.
Based on 20% service access, a 95% confidence level, 20% relative allowable error, a design effect of 2.0 for cluster sampling, and the formula Z2pq/d,2 the final minimum sample size requirement of 768 was computed. We used multistage cluster sampling to select the participants from community-dwelling OASMI in 60 panchayats in three districts of Kerala – Thiruvananthapuram, Malappuram, and Kannur. Thiruvananthapuram, the southernmost district in Kerala, is the state capital and has a better health infrastructure than the other two study districts. Malappuram is the most populous district of Kerala and is home to about 13% of the state’s total population. Kannur, situated toward the northern end of Kerala, has the second-largest urban population in the state. Data collection was completed between August 2019 and March 2020.
Sampling
The minimum sample size required was 768, and the final number of participants included in our study was 917. Through a screening exercise, specially trained ASHA workers identified and listed the OASMI. From this list, 15 ± 2 participants were selected from each panchayat through random sampling. The caregivers were the first choice as respondents to provide information about the OASMI participants. The OASMI were chosen as responders if they were considered more competent than the caregiver or if there was no caregiver.
Data Collection
A pretested sociodemographic data tool captured relevant details like age, sex, religion, social group, marital status, education, occupation, income, type of family, family size, and housing standards of the participants. The relevant components of the National Family Health Survey 4 (NFHS-4) 11 and the Census of India 2011 12 helped develop this sociodemographic data tool. The interviews were conducted in the participant households by trained research fellows using Open Data Kit (ODK) digital forms.
Data Analysis
We conducted univariate and bivariate analyses of the data using the SPSS version 25.0. Quantitative variables were expressed as mean and standard deviation, and qualitative variables were expressed as frequencies and percentages. The chi-square test for count outcomes was used to perform exploratory analyses of the association of different variables with the sex of the OASMI and also their various age categories. The significance level was estimated with 95% confidence intervals and a p-value <0.05. We compared our findings with the Longitudinal Ageing Study in India – Wave 1 (LASI) 13 – a survey across all states and union territories of India to assess the health, economic, and social determinants and consequences of population aging in India, and the 2011 census data. 14
Ethical Considerations
The study was approved by the Institutional Ethics Committee of Government Medical College Manjeri (IEC/GMCM/10/17). Written informed consent was obtained from all the caregivers and competent OASMI participants.
Results
Through the screening exercise involving ASHA workers, 2685 OASMI were listed. From this list, 930 OASMI were randomly sampled and contacted for interviews at their households. Three participants did not provide consent, six did not meet the screening criteria (in the research fellows’ interview), and the information from four participants was considered unreliable. Thus, the data from 917 OASMI participants were included in the study (response rate of 99.2%).
Among the respondents, 6.2% were OASMI themselves. The other respondents included son/daughter (29.4%), spouse (27.6%), son-in-law/daughter-in-law (19.4%), siblings (11.5%), etc. Among the OASMI, 63.7% had caregivers. According to the respondents, 32.3% did not have caregivers because they were independent, and 37 (4%) did not have caregivers despite their need.
The characteristics and sex-wise comparison of OASMI are provided in Table 1.
Characteristics and Sex Differences of Older Adults with Serious Mental Illness.
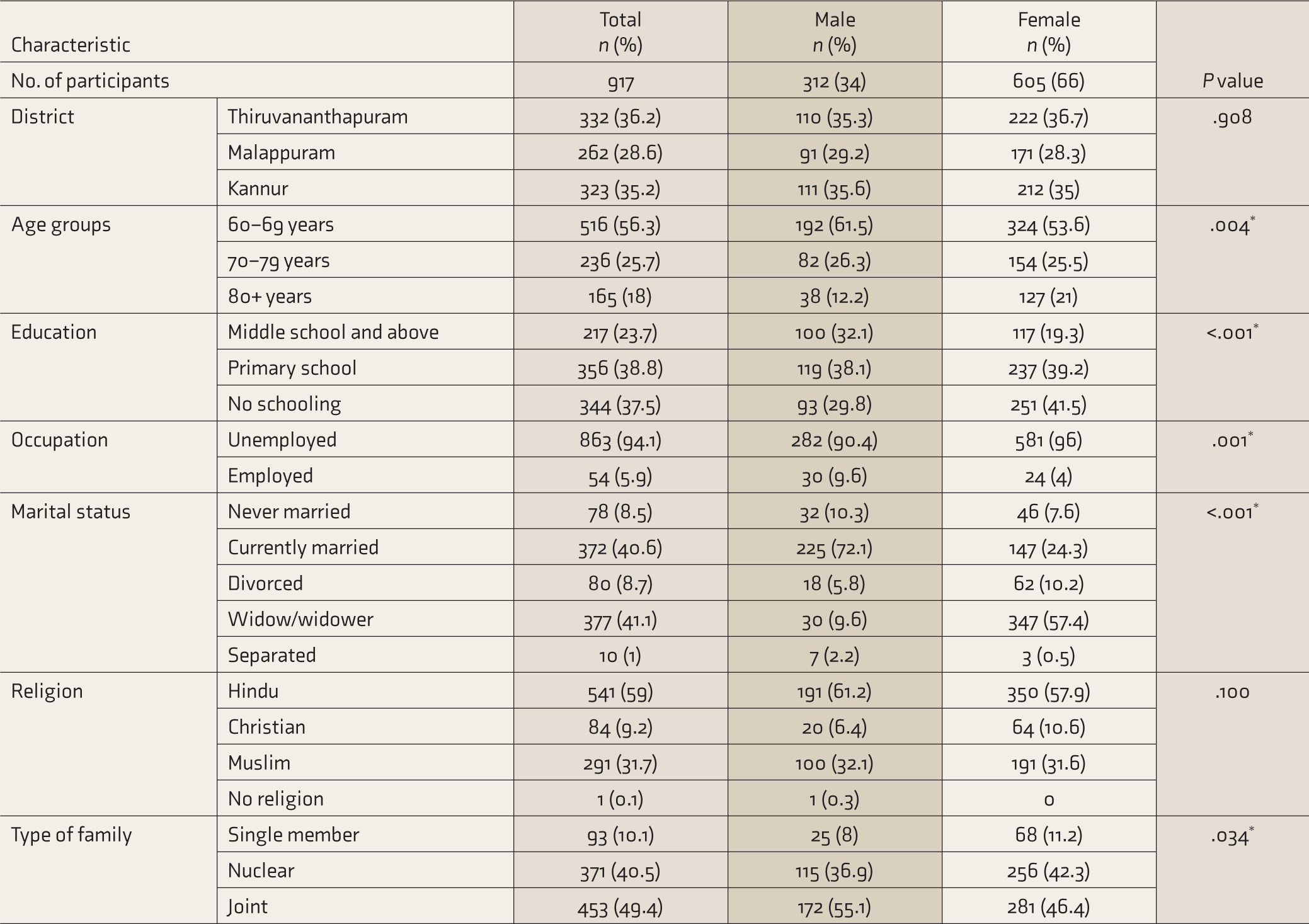
*Significant.
Sex
Two-thirds of the participants were female. The sex ratio was almost the same in all three districts. There was no significant difference in religion, social group, type of house, or ration card status between the sexes. But they differed in age groups, education levels, current employment status, marital status, and type of family (Table 1).
Age
The age of the participants ranged from 60 to 97 years. The mean age was 69.91 (SD 8.8), and the median was 67. As expected, the percentage share of participants showed a reducing trend with increasing age (Table 1).
Type of Family
Most participants (49.4%) lived in joint families, and 10.1% lived alone. The mean family size was 3.3. The never-married participants were more likely to live alone than others (OR 4.24, 95% CI: 2.45–7.36, p < 0.001). This difference was significant for both males (OR 6.46, 95% CI: 2.50–16.22, p < 0.001) and females (OR 3.61, 95% CI: 1.79–7.27, p < 0.001), with the odds being higher for males.
Education
The lower age groups had a comparatively better education than the older age groups.
Occupation and Income
Most of the participants were unemployed (94.1%). Females were more likely to be unemployed than males (p = 0.001). Although 81.6% reported having a regular income, a meager government social pension (Rs. 1,600/month) was its source for most. A total of 490 (53.4%) participant households had ‘Pink’ (Below Poverty Line) ration cards and 120 (13.1%) had ‘Yellow’ (Andhyodaya Anna Yojana) ration cards. A total of 180 (19.6%) had ‘Blue’ (Above Poverty Line) and 100 (10.9%) had ‘White’ (Nonpriority) ration cards. A total of 27 (2.9%) participants did not have ration cards. Thus, 66.6% of families had ration cards issued for the poor or priority groups.
Religion and Caste
The social composition of the participants was as follows: general castes (48.2%), other backward castes (41.9%), scheduled caste (8.9%), scheduled tribe (1.0%), and caste not declared (0.3%).
Housing
The vast majority (90.5%) lived in pucca houses. Only about 2.5% lived in kutcha houses (houses made of mud, thatch, or low-quality materials). 15
Discussion
Almost all published studies on OASMI in India are among institutionalized patients, hospital outpatients,16,17 or beneficiaries of welfare activities like outreach clinics. 18 This paper describes the sociodemographic characteristics of OASMI participants in the SENIOR research project in Kerala. SENIOR is the first study in India to assess the community-dwelling OASMI. Computer-assisted data collection using ODK in our study improved data quality and helped avoid missing data. Our sampling strategy, a highly representative sample, and a high response rate reduced the probability of selection bias. Personal interviews of participants in their households by trained researchers using a standard tool reduced the likelihood of information bias. We discuss our findings under four key themes.
1. Risk of Social Isolation
The proportion of currently married adults among the OASMI (40.6%) was around 20% points lower compared to the older adults in India (61.6%) 19 and Kerala (60.8%). 13 Male OASMIs (72.1%) were likelier to be currently married than female OASMIs (24.3%), by a massive 47.8 percentage points difference (Table 1). The sex disparity was starker in the ≥ 80-year age group, with only 5.5% of women having spouses compared to 63.2% among men. This study found that among OASMI, the proportion of those living alone (10.1%) is double that of the general population of older adults (5.1%) in Kerala (Figure 1). 13
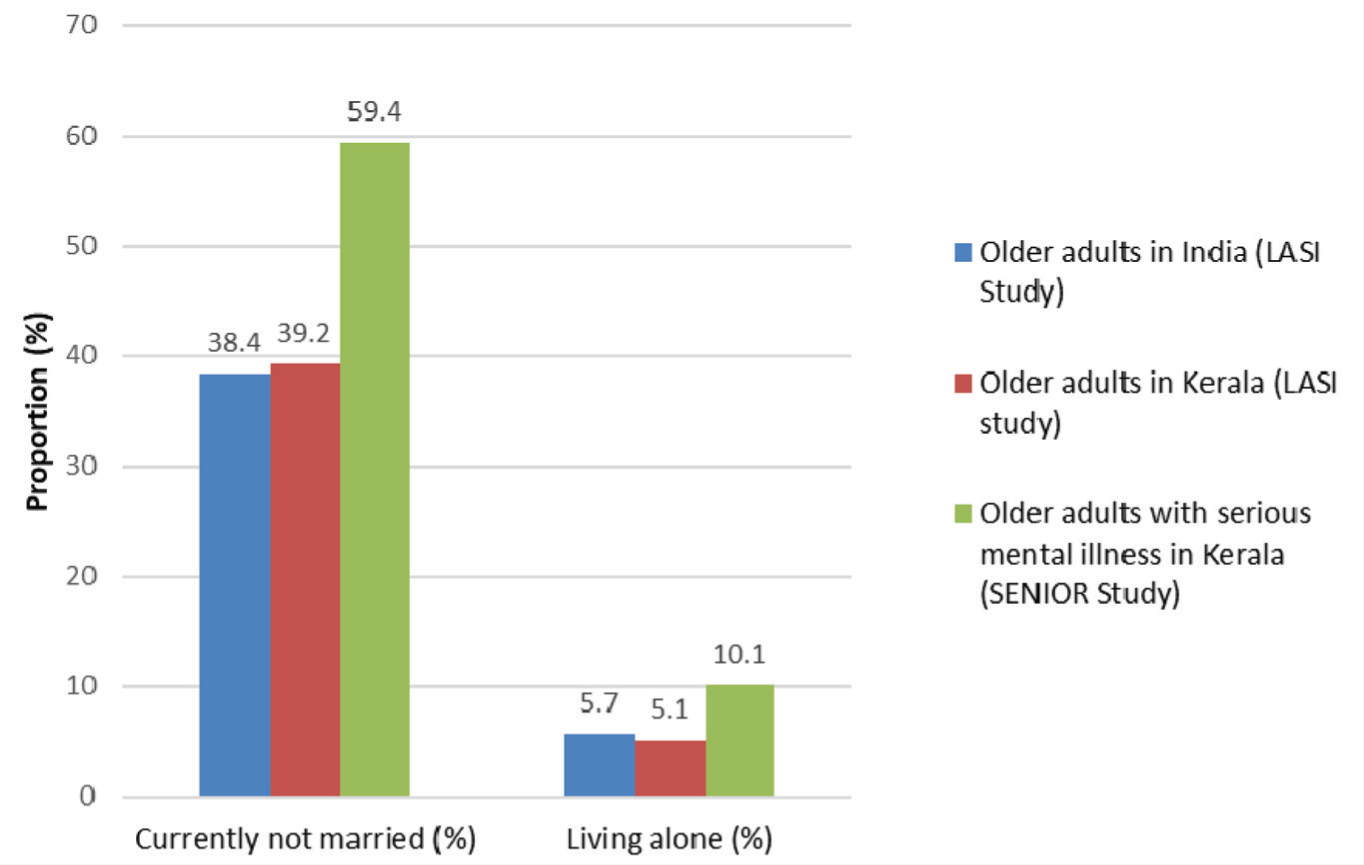
* Longitudinal Ageing Study in India - Wave.
Social isolation is the absence or near- absence of meaningful social relationships and interactions among individuals and exists in all countries across the life course. 20 Older adults who have lost their spouses/partners lack companionship, which is crucial for humans. Social isolation in older adults is associated with an increased risk for poor mental and physical health and increased mortality. 21 A meta-analysis of 3,08,849 individuals indicated a 50% increased likelihood of survival for participants with stronger social relationships than those with poor connections. 22 When adult children move out to start their families, many OASMI are forced to live alone. Some prefer to live independently as a choice, and some because of their mental illness.
2. Feminization
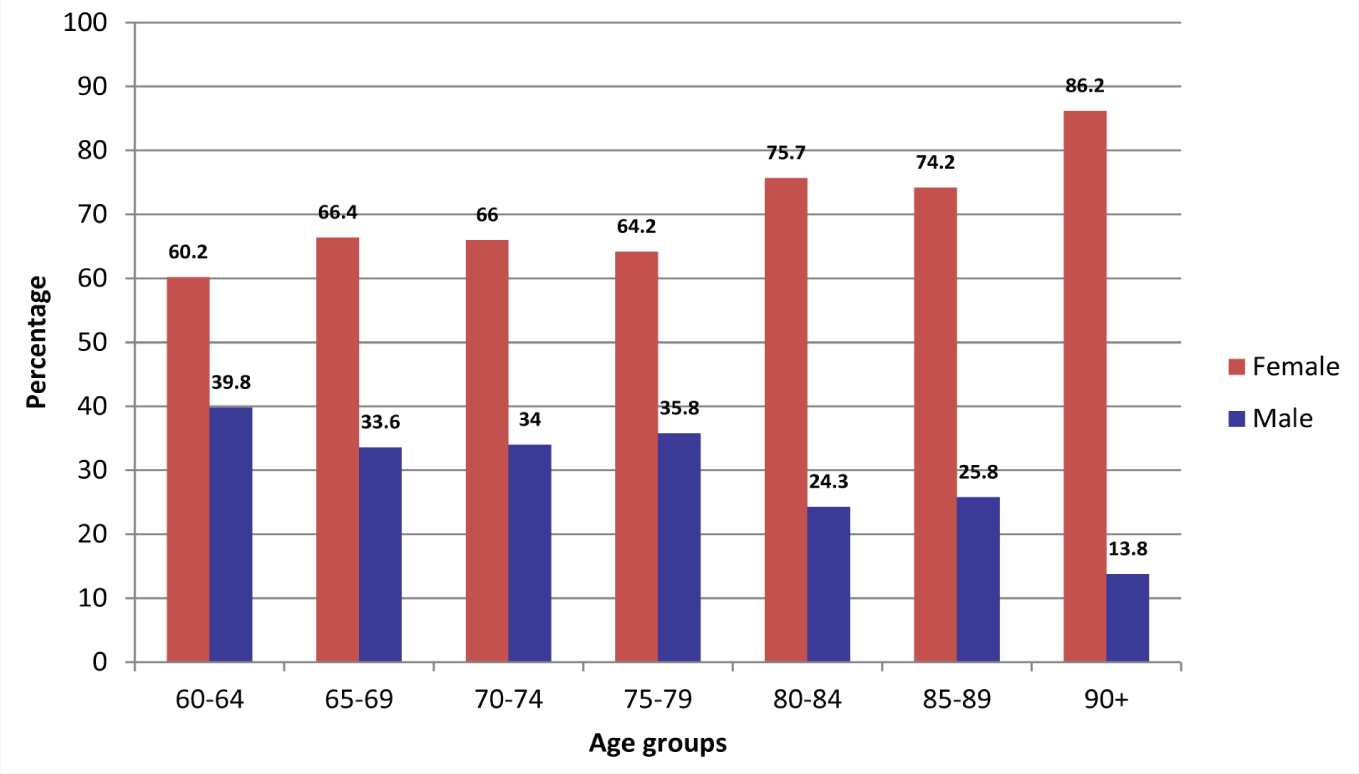
Our study found that the proportion of males decreased progressively in the higher age groups (Figure 2). The proportion of males among the OASMI (34%) was 10.5% points lower than the proportion of males among the general population of older adults in Kerala in LASI Wave 1 (44.5%). 13 The progressive reduction in the ratio of males in the higher age groups among the general population is a global phenomenon. 23 Still, the decline was starker among the OASMI in our study. With the limitation of a cross-sectional study, this finding indicates that older men with SMI die earlier than those without SMI. Identifying the reasons for this disparity can help prevent early deaths among males with SMI. The increased proportion of women among OASMI highlights the need for gender considerations in any future intervention program for OASMI.
Comparison of the Proportion of male and female older adults with serious mental illness in different age groups.
3. Socioeconomic Vulnerability
Kerala has the highest overall literacy rate (96.2% in 2020) 24 and literacy rate among older adults (79.2% in 2011) 14 in India. But our study found the rate among the OASMI to be much lower (62.5%). The unemployment rate among the OASMI was also higher (94.1%) than that of older adults in Kerala (74.6%). 24 A total of 27 (2.9%) participant households who did not have ration cards were excluded from the Public Distribution System (PDS) and some government welfare schemes. Financial backwardness was also higher among the OASMI than in the general population. 13 Education and occupation are two factors that influence income and economic status. The disadvantage for OASMI in these two areas possibly compounds the financial backwardness. On the brighter side, the younger age group OASMI were more educated than the higher age groups. Hence, the educational status of OASMI is expected to increase in the future in parallel with the general population as the younger groups replace the current oldest-old age group.
4. Oldest-Old
Of the OASMI, 18% belonged to the oldest-old age group (≥80 years) (Table 2). According to the World Health Organization, people with SMI have a 10–25-year reduction in life expectancy. 8 The mortality rates for those with schizophrenia are 2–2.5 times that of the general population, and for those with depression, it is 1.8 times higher. For bipolar disorder, the rates are 35–50% higher 8 . Although life expectancy cannot be gauged using cross-sectional study design, we found that many OASMI survive beyond the age of 80 years. Their requirement for assistance in everyday activities and medical care is high, and India’s existing mental health programs must consider the oldest-old persons with SMI.
We recommend that the government develop policies and programs to address the problems of the older adults with SMI identified in this study – social isolation, poorer socioeconomic status, and sex difference. Such interventions are crucial for the country to achieve the United Nation’s Sustainable Development Goals (SDGs) and the central promise of the 2030 Agenda for Sustainable Development – “Leave no one behind.” 25
Age-wise Difference in Characteristics of Older Adults with Serious Mental Illness.
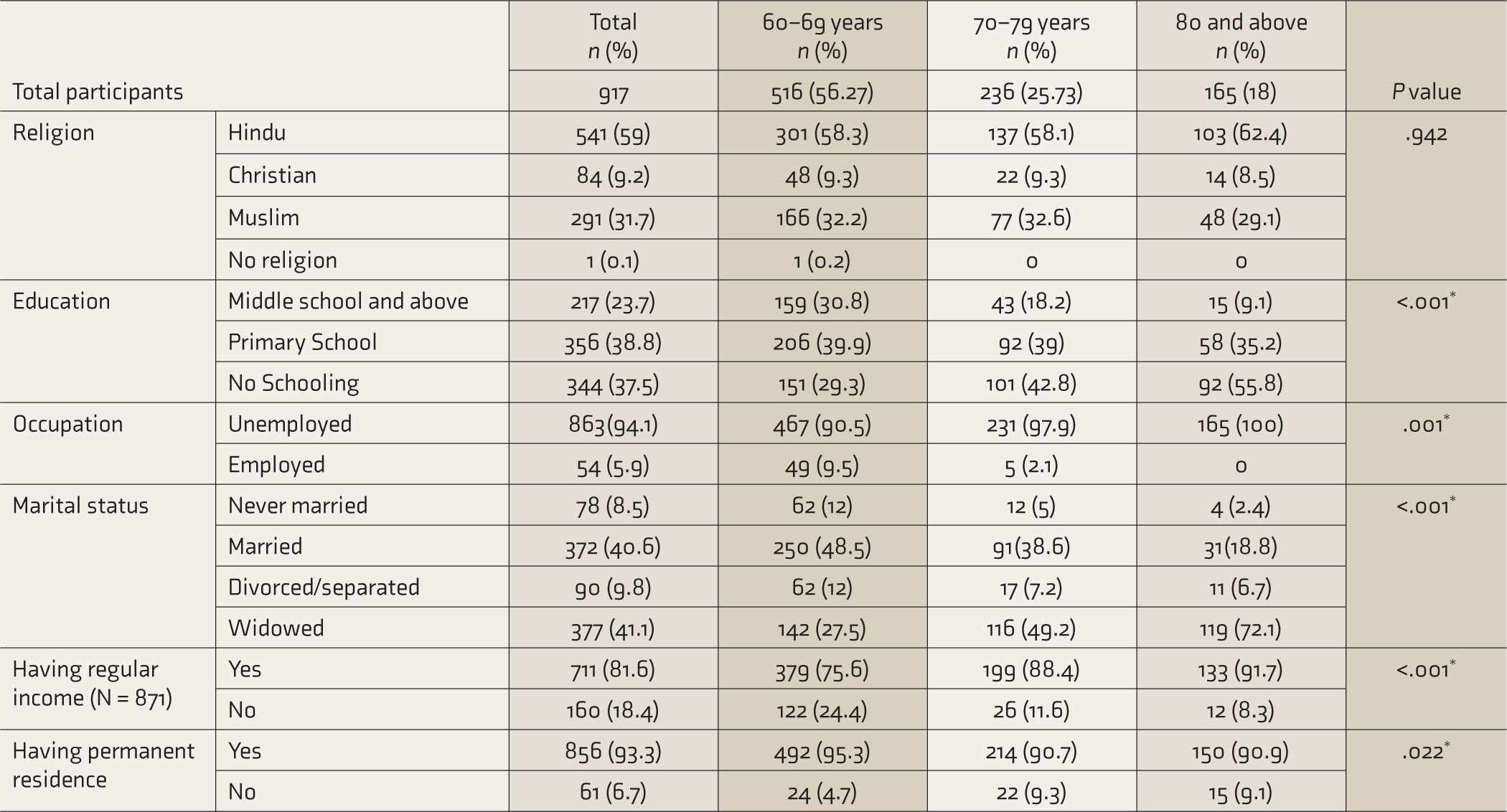
*Significant.
Limitations
Kerala has the best human development indicators in India, and the generalizability of the findings to the remaining Indian states could be limited. But it can be understood that if the OASMI in Kerala shows so much vulnerability, their situation in other states could only be worse.
Conclusion
India lacks evidence on the sociodemographic profile of OASMI. This study captured their profile in Kerala state and highlighted their multiple vulnerabilities. They have poorer socioeconomic status and have higher rates of social isolation. Male OASMI are dying earlier compared to the general population of older adults in Kerala. Considering these findings from a state with the best health and social indicators in the country, the situation of OASMI in India demands more attention.
Footnotes
Acknowledgements
We thank Dr. Smita N. Deshpande, Dr. Triptish Bhatia, Dr. Asma Rahim, Dr. K. S. Shaji, Dr. Ravinder Singh, Dr. Balram Bhargava, Dr. R. S. Dhaliwal, Dr. Margaret C. McDonald, Dr. Mary Hawk, Dr. Vishwajit L. Nimgaonkar, Dr. James E. Egan, Dr. Robert W. S. Coulter, Dr. Kiran P. S., ASHA workers, and the Department of Health Services, Kerala, for their support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Indian Council of Medical Research under the ‘Capacity Building Projects for National Mental Health Programme, ICMR-NMHP’ vide file number 5/4-4/151/M/2017/NCD-1. International mentors were funded by the training program ‘Cross Fertilized Research Training for New Investigators in India and Egypt’ funded by FIC, NIH (No. D43 TW009114).