
Abstract
Background:
Among working people with serious mental illness (WPSMI), return to work (RTW) is controlled by several factors. Identifying these factors can help prevent long-term sick leave absence and work disability. We aimed to identify facilitators and barriers of RTW in WPSMI admitted to a psychiatric hospital and clinic affiliated with the Hamadan University of Medical Sciences, Iran.
Methods:
This qualitative study was conducted in 2020 on 27 participants with SMI and their families, supervisors, coworkers, managers, and mental health professionals (MHPs). The participants were selected through purposive sampling and subjected to semi-structured interviews. Forty interviews were conducted and analyzed using conventional content analysis.
Results:
Nine hundred initial codes were extracted and categorized into 34 subcategories and eight categories. Categories that emerged as facilitators of RTW include emotional availability, information availability and use, practical assistance of others, employment facilitation by the society, and supervisor’s flexibility. Categories identified as barriers are imposed effects of mental illness, poor self-concept, and social obstacles.
Conclusion:
WPSMI experience some facilitators and barriers in RTW. Therefore, MHPs and politicians are recommended to consider these factors in vocational rehabilitation plans.
Keywords
According to WPSMI, emotional availability, information availability and use, practical assistance of others, employment facilitation by society, and the supervisor’s flexibility are facilitators of the RTW. In contrast, imposed effect of mental illness, poor self-concept, and social obstacles may hinder or delay the RTW; family members, friends, coworkers, supervisors, managers, MHPs, and the government are essential facilitators of RTW; and empowering support sources helps improve the RTW.Key Messages:
Some working people suffer from mental illnesses. 1 Working people with serious mental illness (WPSMI) are highly susceptible to adverse effects of sick leave, work disability, loss of purpose, and a higher risk of social isolation.2, 3 Return to work (RTW) in a competitive market is difficult for people with SMI, such that only 10% to 25% of them can return to their job. 4 In a meta-synthesis, Suijkerbuijk et al. reported that supporting people with SMI through RTW programs may increase the RTW rate by 20% to 60%. 5 In Iran, the unemployment rate of people with SMI is above 70%. 6 However, the Disability Protection Act of Iran passed in 2003 has provided some sections related to employment and inclusion of persons with disabilities in the workforce. 7 In another effort, the bill to protect the rights of people with mental illness was passed in 2020. 8 Despite these programs, Iranians with disabilities still face barriers to accessing vocational rehabilitation services. 9 Findings from other studies in Iran also show a knowledge gap about working people with mental illness in this country.10, 11
According to some reports, RTW in people with SMI is a function of some individual and environmental factors that facilitate or hinder their decision to RTW. Sometimes, barriers to RTW cause dissatisfaction in people with mental illness, mainly because of insufficient support or recurrence of the illness, especially in the context of work.12, 13
There is limited information about facilitators and barriers to RTW for designing interventions related to the RTW of WPSMI, especially in low-income countries. Among the limited studies conducted in this regard, some RTW interventions have not been successful.14, 15
Cameron et al. noticed a difference between people with SMI who are looking for a job and employment and those who want to RTW after recovery. The latter have previous work experience and may confront different challenges from the former. 16 Thus, the difference in the RTW of WPSMI and the need to design appropriate interventions with low-middle-income countries’ structures are strong motivators to identify the facilitators and barriers to RTW. Qualitative studies are context-based, 17 and because the subject of this study is context-based, the present qualitative investigation was performed to identify factors facilitating or acting as a barrier to RTW in WPSMI admitted to a psychiatric hospital affiliated with the Hamadan University of Medical Sciences, Iran.
Methods
Design
This study was performed in a qualitative paradigm using the content analysis approach. The content analysis approach is a research method for the subjective interpretation of the content of text data through systematic coding and identifying themes or patterns. Content analysis has roots in social science that can be used to study social phenomena such as RTW.18–20
Study Setting
The study was conducted in Sina (Farchian) Educational and Therapeutic Center affiliated with the Hamadan University of Medical Sciences in Hamadan, west of Iran.
Participants
Being a qualitative study, the participants were recruited through purposive sampling with maximum variety. In purposive sampling, the researcher looks for participants with rich experiences about the phenomenon under study who are willing to share their experiences. 17 The study subjects included WPSMI willing to participate in the study. The major inclusion criterion was having a definite diagnosis of SMI based on Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition in medical history. According to a definition, SMI refers to mental, behavioral, or emotional disorders creating severe functional disorders that mainly intervene with one or many major life activities. Most cases in this category are schizophrenia, bipolar I disorder, schizoaffective disorder, and major depressive disorder.21, 22
Other inclusion criteria were being over 18 years old, having a job before developing SMI, being discharged from the hospital, being in the recovery phase, currently having a job at least 28 days continuously, and having the ability to communicate and express experiences, feelings, and reactions. According to the International Labor Organization regulations accepted in Iran, one has a job if they work for at least 1 h per week in return for cash or noncash salary. 23 Individuals with alcohol or drug addiction problems or other mental and developmental disorders were excluded.
WPSMI (n = 15), family members (n = 3), organizational manager (n = 1), supervisors (n = 1), coworkers (n = 1), and health care team members (n = 6) were included. In this way, it was likely to capture a wide range of experiences, views, and maximum variance in data. Data saturation was achieved after 24 interviews, and the last three interviews yielded no new data.
Data Collection
The study was conducted from February 9, 2020, to December 20, 2020. Participants’ medical documents were checked by the first author (MM), who had the experience of working in the psychiatric department. Next, the documents were confirmed by the third author (AG), as an experienced psychiatrist. The first author (MM) called the participants and conducted the interviews.
The interviews were semi-structured to explore both perceived barriers and facilitators of RTW for WPSMI. After establishing a relationship with the participants, the interviews were conducted face-to-face with an opening question: “Can you describe anyone or anything that has helped you to RTW?” The interview was continued as a conversation between the interviewer and the participant around the interview matters, such as experiences hindering the RTW. Probes were used to encourage participants to describe more experience: “Can you please tell me more about it?” “Can you give me an example?” Each interview lasted 30 to 45 min. All interviews were performed in the Persian language. Each interview was translated to English by an expert translator and again back-translated to Persian. The researcher team checked the accuracy of the translation. Two pilot interviews were not included in the study. To ensure the validity of the interview guideline questions, the fellow researchers read the transcripts of the interviews performed by the first researcher. We conducted at least two interviews with some participants. The second interview was conducted to complete the first interview. Overall, 40 interviews were conducted with 27 participants.
Data Analysis
The verbatim interviews were transcribed and transferred to MAXQDA 10 to facilitate data management. The analysis was conducted alongside the data collection using a qualitative conventional content analysis method described by Hsieh and Shannon, 24 and Erlingsson and Brysiewicz’s 25 qualitative conventional content analysis involves coding categories extracted directly and inductively from the raw data. In the conventional content analysis, data are summarized to a higher level, that is, from coding to category level.19, 25 In the first stage of this study, the transcriptions were read carefully to obtain a general impression of the whole, and the text was divided into smaller parts (i.e., semantic units). In the next step (i.e., open coding), semantic units were shortened and compacted without affecting the text content. Each semantic unit was abstracted and labeled with a code (live or interpretive). After open coding, the codes were sorted into subcategories by comparing their differences and similarities. Afterward, subcategories were abstracted and grouped into categories with the same issue.
Ensuring Qualitative Rigor
Four criteria of confirmability, dependability, trustworthiness, and credibility were used to determine data’s validity and reliability. 26 In this study, the researchers’ long-term engagement, maximum diversity in sample selection, appropriate interaction with participants, integration of information, and checking the participants’ data helped increase credibility. The reliability or consistency of the findings was assured by writing memos as soon as possible, using peer reviews, and rereading the entire data. Confirmability was obtained by documenting the procedures for checking and rechecking the data and using the audit trial strategy during the research process. To enhance the data transferability, we carried out the entire research process and wrote the work along the study path clearly and precisely. As a result, others are allowed to follow the research path and the characteristics of the study population. Transferability was also assured by providing direct quotes and examples, rich explanations of data, and scientific consultations with expert university professors.
Ethics Considerations
This study is a part of a psychiatric nursing PhD dissertation approved by the Ethics Committee and Research Council of Technology, the Hamadan University of Medical Sciences (IR.UMSHA.REC.1399.504). All the participants were informed about the study’s objectives and stages. Their participation was voluntary, and they could leave it at any stage. After each interview, participants received a gift as a token of gratitude for participating in the research.
Results
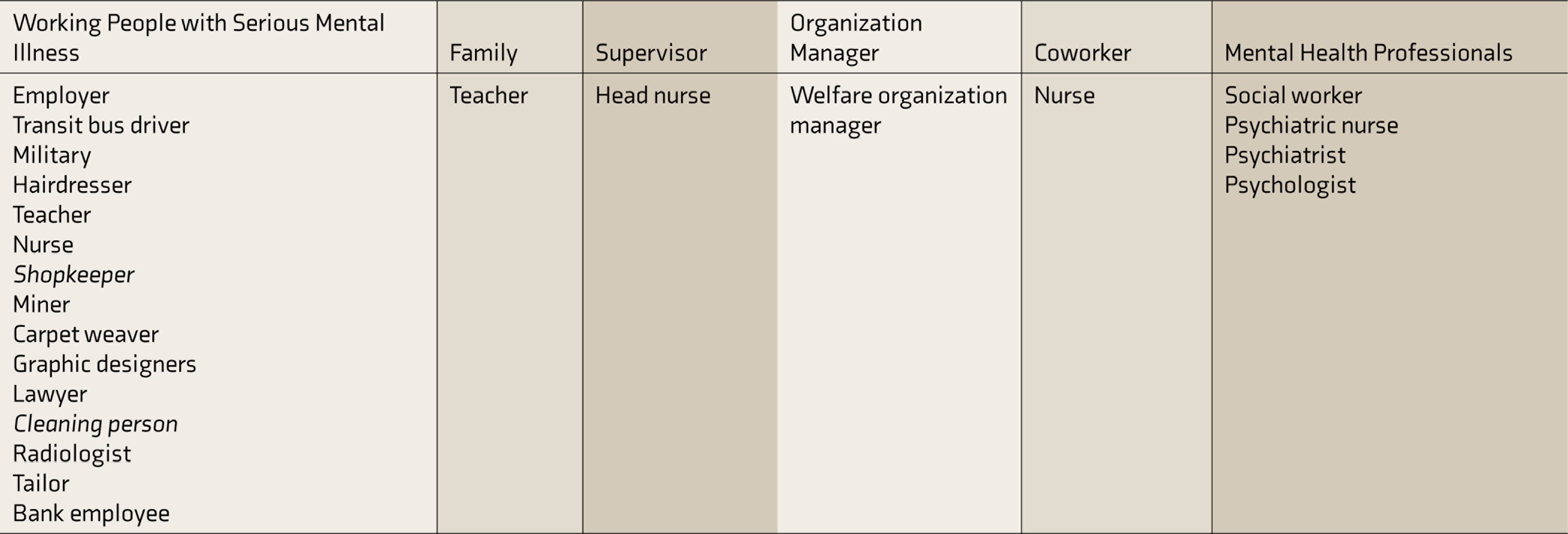
The 27 participants included 15 men and 12 women with a mean age of 39.2 ± 8.5 years. They were single (n = 4), married (n = 19), or divorced (n = 4) and had primary education (n = 4), diploma (n = 7), or university education (n = 16). Among the patient participants, diagnoses were major depression (n = 5), schizophrenia (n = 2), bipolar I disorder (n = 7), and schizoaffective disorder (n = 1). They had a mean RTW of 7 ± 5 months. The occupations of participants include WPSMI, family members, organizational managers, supervisors, coworkers, and MHPs listed in Table 1.
List of Job Title of Participants
A total of 900 codes were extracted and categorized into 34 subcategories and eight categories (Table 2). The participants described facilitators of RTW, including emotional availability, information availability and use, practical assistance of others, employment facilitation by the society, and supervisor’s flexibility. Imposed effects of mental illness, poor self-concept, and social obstacles were identified as barriers.
Illustration of Subcategories and Categories
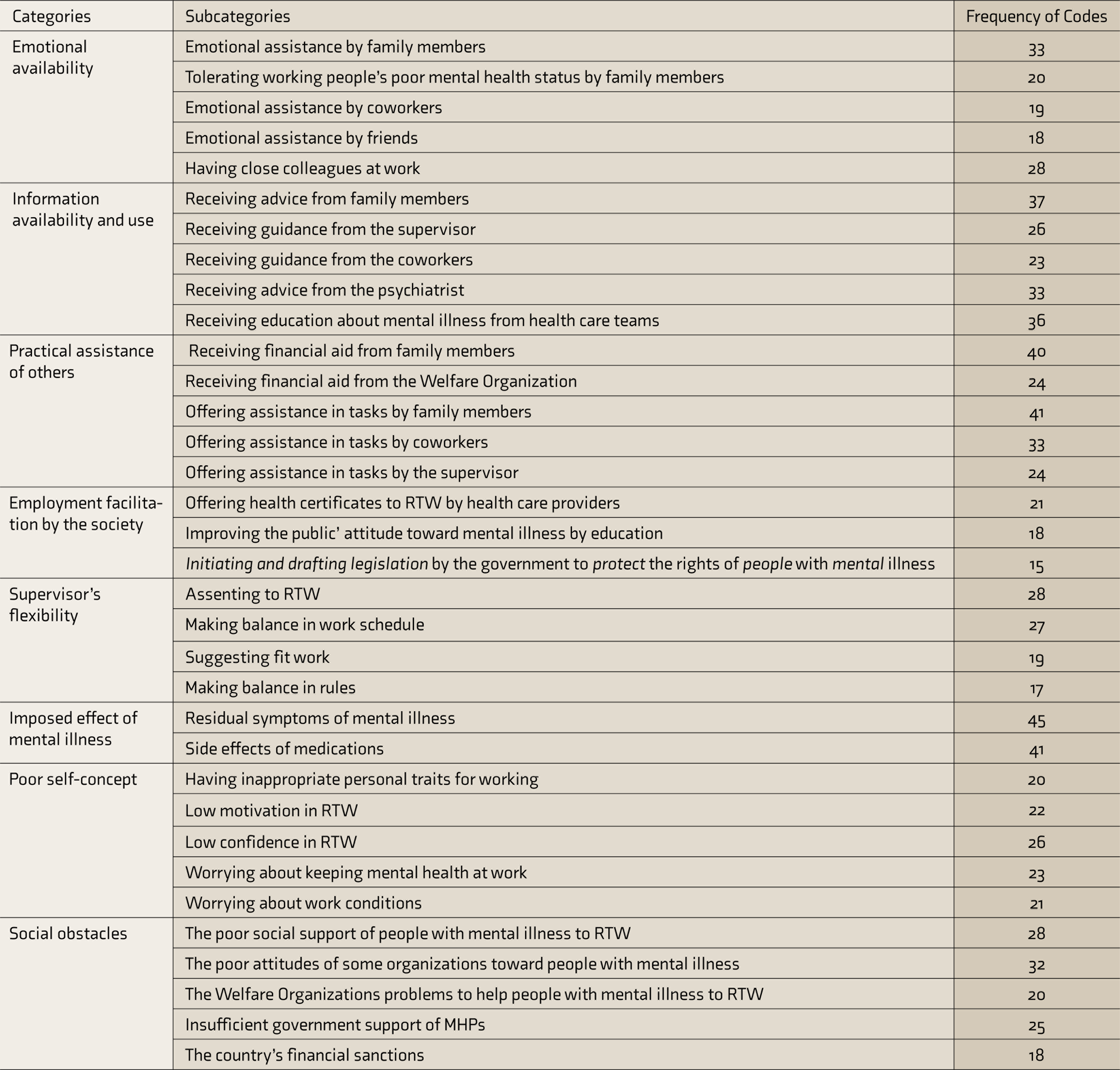
RTW: return to work, MHPs: mental health professionals.
Facilitators of RTW
Participants believed that emotional availability, information availability and use, practical assistance of others, employment facilitation by the society, and supervisor’s flexibility facilitated the RTW.
Category 1: Emotional Availability
One of the facilitators of RTW is emotional availability. In this study, emotional availability included five subcategories: providing emotional assistance by family members, coworkers, and friends; family members tolerating working people’s poor mental health status for helping RTW; and having close colleagues at work. Emotional assistance by family members (e.g., parents, spouses, or other family members) offers encouragement, hope, and reassurance or creates a more peaceful environment. The spouse of a participant who is a teacher with major depression disorder explained, “I constantly encourage my husband to RTW because working may help to improve mental health status. The man should go to work. I support him a lot…” (P17). Also, family members tolerate inappropriate behaviors of participants that result from poor mental health status. Emotional assistance offered by family members helps to proceed with RTW. For instance, the above-mentioned participant’s spouse explains that major depression disorder slowed down her husband’s behaviors and she tolerated him. In addition to the families, coworkers and friends provide emotional assistance for helping RTW. Emotional assistance by coworkers may help them maintain the RTW because coworkers understand WPSMI and try to deal with their mental health problems. Similarly, friends support working people by sympathizing with and respecting their feelings. One of the working participants, who is an employer with bipolar disorder, explained: “My coworkers knew about my mental illness and would try to help me by telling me to control myself, forget about the troubles, and things like that…” (P1). Some participants mentioned having close colleagues in the workplace. Close colleagues understand working people with mental problems, listen to their problems, and make their RTW easy. Typically, close colleagues ask supervisors to re-engage WPSMI. According to the supervisor of a participant, “His psychiatrist of P6 (nurse) strongly supported him, taking advantage of his power in the organization. He used to call me frequently and ask me to have him back to work. I could not say no…” (P20).
Category 2: Information Availability and Use
This includes five subcategories: providing advice, guidance, education, or helpful information by family members, supervisors, coworkers, and MHPs.
Although our participants were not supported with vocational rehabilitation services, they were seeking information and guidance from other sources. Family members are a key information resource. Family member participants described that their close relationships with WPSMI allowed them to give their opinion, suggestion, and useful information. For instance, a participant’s spouse advises her husband to talk to his supervisor, to convince him to RTW. At work, supervisors and coworkers offer emotional support for helping RTW. A coworker of a participant, who is a nurse with bipolar disorder working in the psychiatric ward, explains how he has supported him: “At work, we help him (P6, nurse), guide him, and answer his questions…” (P20). Also, the supervisor of a participant mentioned her recommendations, “Nurse (P6) called me (supervisor) after his recovery and said that he did not want to come to work … but he wanted to keep his work. I said if you do not have a shift, the nurse manager will consider absenteeism. He asked me to help. I told him to send me his sick leave documents and that I will show them to the nurse manager…” (P19). In addition to participants receiving information from the sources mentioned above, psychiatrists also have a role in serving information to them. The participants described that they consult their psychiatrist about RTW, and the psychiatrist usually talks about RTW stresses and decreasing the workload.
One of the subcategories of information availability and use is receiving mental illness training from treatment teams. In a bill on protecting the rights of persons with mental disorders (2020), the President of Iran mandated the Ministry of Health and Medical Education to work with other organizations to educate all people about mental illness. One participant, who is a psychiatrist, explained: “The requests of WPSMI to RTW are reasonable and should be taken seriously … Education at various levels of society helps RTW…” (P25).
Category 3: Practical Assistance of Others
Participants believed that family members, friends, colleagues, supervisors, and psychiatrists help them by providing emotional and information assistance and support them in other more tangible ways. This category has six subcategories: receiving financial help from family and Welfare Organizations (WOs) and receiving support from family members, coworkers, and the supervisor for performing work-related tasks.
Family members assist participants in response to an RTW request. RTW of SMI is important for family members, as they want to see them financially independent of the family to pay for their treatment. To this end, they may help WPSMI by offering financial aid. For instance, a participant, who is an employer with bipolar disorder, explained: “In time of sickness, when I didn’t have enough money in the account to cover the check, my brother cashed my checks. I had family support…” (P1). Sometimes, family members assist patients in performing work-related tasks or their responsibilities. In one case, the spouse of a participant (a radiologist with bipolar disorder) contacted the supervisor and requested a leave of absence to save him from losing his job. In another case, the sister of a male participant (a miner with schizophrenia) requested her boss to employ his brother in a limestone mine. Also, the spouse of an employer with bipolar disorder knows that mental illness influenced her husband’s work function, she assisted him at work, for instance, by paying the salary of the workers or managing the purchase of raw materials for the workplace. Coworkers and supervisors help practically facilitate the RTW of WPSMI. In this respect, one of the participants, a cleaning staff with schizophrenia, explained, “My body-functions are slow. I cannot perform my tasks faster, and hence my coworker helps me…” (P12). In the same way, supervisors provided paid time off to participants, used replacement staff, kept in regular contact with the participants about their position, negotiated with high managers to RTW, and gave participants the opportunity to RTW.
WOs provide financial or other aid to individuals or groups who need support at the society level. The WOs are aimed to help promote independence in people with SMI and reduce the unemployment rate. In this study, SMI patients talked about receiving loans from WOs. The State Welfare Organization of Iran and Imam Khomeini Relief Foundation are two governmental supporting entities that allocate a general state budget for supporting people with disabilities and deprived persons. The division for rehabilitation of the State Welfare Organization is the main state institution concerned with providing support and assistance to disabled people in Iran. The State Welfare Organization and Imam Khomeini Relief Foundation offer a loan to WPSMI who want to work and earn their living from any independent type of economic activity. Loans often come with lower interest rates, and WOs offer them to WPSMI if they are qualified on medical documents. For instance, the mother of a participant who had a supermarket noted, “My son used to work with his father. After his mental illness, we helped him to open a new store. He obtained a loan of Rial 100,000,000 from Imam Khomeini Relief Foundation …” (P18).
Category 4: Employment Facilitation by the Society
This category shows the importance of support received from mental health professionals (MHPs) and the government to employ people with SMI and their RTW. This category includes three subcategories about sickness certification, mental health awareness, and mental health legislation. We found that mental health caregivers help WPSMI by offering health or sick leave certificates. Providing these certificates to the supervisors may affect the supervisor’s assent and facilitate RTW. MHPs, organizations, and the government support the RTW of people with SMI by improving the public perception about mental illness and alleviating the stigma. For example, a psychiatrist explained the need to develop educational programs to change the attitudes of family members, especially spouses, toward people with SMI to reduce the stigma of mental illness. MHPs and organizations should provide such education. Also, the government has passed regulations for supporting people with SMI that extend premium exceptions for employers who recruit people with SMI. About SMI employees, an organization manager describes that: “An order has come from the ministry, asking to support SMI employees …. Therefore, I have recruited a psychologist to help these employees…” (P22).
Category 5: Supervisor’s Flexibility
This category includes four subcategories about agreeing to RTW, making balance in work schedule, suggesting fit work, and making balance in rules. The supervisor’s flexibility refers to all the plans and actions arranged by the supervisors to change the workplace condition because of the RTW of WPSMI. For example, some participants have a sick leave in an acute stage of SMI. In the recovery stage, they need to take supervisors’ assent for RTW. Some characteristics of participants (e.g., long work experience, good work experience, and awareness about the participants’ poor living conditions and financial problems) convinced the supervisors to assent with RTW requests. In this respect, one of the participants narrated:
After recovery, I asked the supervisor for RTW… Given my long and positive experience, my request was accepted, and I came back to work as a substitution teacher to fill the places of those who miss a class. I also received the full salary, despite less work and a better work condition… I spent the time mostly at home…. (P5)
Moreover, supervisors may reduce the work hours, create a flexible work schedule, and assign simpler tasks to WPSMI.
Barriers to RTW
Participants believed that imposed effects of mental illness, poor self-concept, and social obstacles impede the RTW.
Category 1: The Imposed Effects of Mental Illness
Consequences of mental illness are among the barriers in the pass of RTW. These imposed effects may restrict or delay the RTW. WPSMI has to suffer many unwelcomed and unpleasant effects of their mental illness. This category includes two subcategories: (a) residual symptoms of mental illness and (b) the side effects of medications.
The majority of the participants reported that residual symptoms of mental illness are a major problem for RTW. Possible loss of previous job position, demands from the supervisor for RTW, and the chronic nature of SMI cause them to RTW before full recovery. Thus, RTW becomes difficult when they still experience residual symptoms of the illness. One participant explained that he was still feeling the symptoms of the mental illness while preparing for RTW. “ As military personnel, I have to RTW after sick leave period; however, I do not feel that I like it…, it is really boring and depressing” (P4).
Also, undesirable effects of psychiatric medications such as drowsiness, depression, stress, and anxiety may affect the work performance of WPSMI. Therefore, they hesitated whether they were really ready to RTW. One participant stated, “I have to tolerate the side effects of medications to go to work. I try to take less medicine…” (P4).
Category 2: Poor Self-Concept
This category emphasizes how participants thought about their personality, motivation, confidence, and mental illness that may affect RTW. A poor self-concept often impairs the ability to RTW. This category has five subcategories: poor personality traits, low confidence, low motivation, and worrying about the relapse of mental illness at work and work conditions. Some participants noted that they had particular characteristics that were unsuitable for work. For instance, they preferred isolation, were not mind-sharp at work, and were shy. These characteristics affected their chance of RTW and delayed it. A miner who has schizophrenia stated, “I got used to isolation, and maybe, the mental illness made me isolated. I was always at home and asleep. This lifestyle made me tired all the time. Well, all this delayed RTW…” (P9). WPSMI were continuously worried that the supervisors or employers might find out about their mental problems. Also, they may feel worried about whether they are capable enough to do their tasks at work and that their employers might blame them if they did not have enough ability. As a result, such concerns lowered their self- confidence. The same participant mentioned, “I thought that back to work, I might make an error at the workplace, coworkers or the supervisor may tell me I could do nothing, or I may make a mistake. This made me upset and worried for RTW…” They were also worried about maintaining their mental health at work. Their concerns included the fear of recurrence of the mental illness at work, the inability to control the residual symptoms of the disease, and the medication side effects. All these experiences and many other factors created a dark image of RTW in their mind, lowering their motivation to RTW.
Category 3: Social Obstacles
One of the problems encountered in the pass of RTW is social obstacles. Like other society members, the participants had public or social problems. As a result, they may become hesitant to RTW and postpone it. This category includes five subcategories: poor social support, poor attitudes of some organizations toward mental illness, the WO’s problems, insufficient government support of mental health care teams, and financial sanctions. Poor social support means that the WPSMI did not receive adequate social support from family members, supervisors, coworkers, government, or society. For instance, some participants complained that they cannot find a suitable job because of bureaucratic structures, the country’s poor economic condition caused by sanctions, and the COVID-19 pandemic. A few employers were employing them, or only some supervisors agreed with changing the work conditions. Consequently, they were forced to accept some high-risk jobs such as that of transit bus drivers though the psychiatrists had prohibited them from employing in these jobs. Sometimes, WPSMI were sick or had financial problems, but they could not receive any help from their family members.
Also, some participants described they wanted to RTW but have no close colleagues who can influence the supervisors’ assent for RTW or have no one who answers their questions or guides them at work. One of the participants, a carpenter who experienced major depressive disorder, explained: “Welfare Organization bought me a carpet loom, but there is no one in the workshop of the Welfare Organization to help me. Well, I forget details …” (P10).
Some participants were worried about the organization’s poor attitude about mental illness, such as stigma, fear of supervisor or coworker about mental illness, or inappropriate organization insight into mental illness. Poor attitude of organizations can affect their ability to perform their work well. Besides, stress at work can cause the recurrence of SMI.
Insufficient government support of mental health professions is an issue that affects the RTW of WPSMI. Some issues in this regard include high workload in the public mental health services, insufficient government attention to the private services, inappropriate referral system, and inadequate payment of health care team costs. These issues create poor coordination in mental health care systems. Besides, WPSMI could not easily access rehabilitation services, especially occupational rehabilitation.
In addition, the WO had its limitations and complained about the lack of adequate public funding or many applicants. The organization claimed that they could not cover all applicants, which dissatisfied them. There were also extensive bureaucratic structures like bank regulations that prevented an easy and smooth RTW. One of the participants added:
After recovery, I went to a center affiliated to Welfare Organization, but they closed their workshop because of COVID-19, and there was no job for me. I applied for a loan to buy a small carpet workshop. They referred me to a bank, which told me that I needed an officially employed public worker as the guarantor. I have nobody for this, and I do not know what to do…. (P10)
Furthermore, the country’s poor economic condition because of sanctions and the COVID-19 pandemic influenced RTW and intensified participants’ financial problems. The spouse of a working participant explained: “My husband can handle the work, but financial problems do not allow him to work full-time. When the USA dollar price surges suddenly, he cannot supply the materials he needs for work. Therefore, he cannot accept orders as much because he cannot supply the material….” (P16).
Discussion
This study showed that receiving emotional, informational, and practical assistance from various sources, including family members, friends, coworkers, supervisors, managers, MHPs, and the government, is a major facilitator of the RTW of WPSMI. In line with our findings, Dunn et al., Hall et al., and Cameron et al. highlighted the importance and the role of facilitating support in RTW of WPSMI. In these studies, support means assistance or help that people with SMI receive from others. Availability of different support sources enables people with SMI to RTW.13, 27, 28 Dunn et al. showed that workers with SMI needed at least one supporter to RTW, as mental illness lowered their performance at work. Employers, coworkers, families, and mental health team members are not the same for all WPSMI. Nevertheless, receiving support creates hope and motivation to improve their skills, self-confidence, and capabilities to find jobs suitable for them. 13 Furthermore, Hall et al. explained support in people with mental illness as “social inclusion.” Experiencing social inclusion in the family and community promoted unity and acceptance among people with mental illness. 28 Similarly, Hatchard et al. and Smeets et al. explained a supportive environment and good cooperation between family members, coworkers, managers, and community as key facilitators for RTW of workers with mental illness.29, 30
However, Joosen et al. explained that the RTW is complicated and that there is no specific standard for support. The reason was that the RTW is affected by multiple factors related to the work environment and work content, relationships at work and in private life, and professional guidance and intrapersonal factors. 31 According to Johanson et al., the most facilitating factor of the RTW is the close and continuous support with a respectful and equal relationship between the people with SMI and the other people related to them. Such support enabled them to overcome their low self-confidence and increase their self-efficacy regarding RTW. 32 In addition to the positive effect of support on the RTW, other studies showed that participating in vocational rehabilitation programs is an important factor that facilitates RTW of WPSMI.27, 33, 34 However, participants of our study explained they did not enroll in rehabilitation vocational programs before RTW. A recent study conducted in Iran showed that many people with SMI could not participate in vocational rehabilitation programs because of financial problems. 35 According to our study, WPSMI received assistance from others for RTW rather than participating in vocational rehabilitation programs. The results also showed that practical assistance is more commonly used in the RTW of WPSMI than other types of assistance.
Our participants experienced barriers in the RTW, including the imposed effects of mental illness, poor self-concept, and social obstacles. In line with our findings, Ebueny et al. explained that people with mental illnesses confronted RTW challenges such as poor health, psychiatric illness, social stigma and discrimination, negative attitudes among employers, and the lack of social support and government welfare. 36 At the same, Samuel et al. addressed individual factors such as possible recurrence of illness, decreased concentration, fatigue, sensitivity to criticisms, and family issues affecting the competency of WPSMI at work. 37 Evidence has shown that people with SMI, especially in countries with low- and moderate-income levels, deal with a large number of multiaspect political, economic, social, and cultural limitations. Negative reactions and exaggerated fears about mental illnesses in families, supervisors, coworkers, and society create discomfort for people with mental illness. Because society is forced to give up on the benefits of these workforces, it is necessary to apply different forms of support for people with SMI at different levels, including individual, family, work, and society.28, 38–40
A few limitations are notable in this study. Men’s participation level was higher than women’s because, according to traditional Iranian culture, bringing money to family is mainly a masculine job, and women with mental illness usually stay at home. Future studies may need to focus on working women with mental illness. Also, our sample did not include WPSMI without a successful RTW. However, our results represent different perspectives, including that of the WPSMI, family members, coworkers, supervisors, WO managers, and MHPs.
Another noteworthy issue in this study is that, although WPSMI could not tolerate extended interviews, we conducted at least two interviews with some participants. Some participants were worried about disclosing experiencing SMI, stigma, and possible job loss. Therefore, they were ensured about the interviews’ confidentiality. Also, the interviews were conducted away from their workplace (at the office of the first researcher).
Despite the above limitations, the study prepared the background for interventions to improve the RTW in people with SMI. In low-middle-income countries such as Iran, access to rehabilitation programs is difficult for people with SMI. Hence, we recommend that MHPs provide sufficient education to family members, especially spouses, supervisors, employers, and managers of the WO, for addressing the challenges WPSMI face with regard to RTW. MHPs can promote understanding of policymakers and employers about WPSMI’s ability to work with SMI. Also, introducing social support from various sources can help the success of RTW. Lastly, MHPs can guide WPSMI on what they can do when they want RTW.
Conclusion
This study underlined some facilitators and barriers that WPSMI experience in the RTW. Facilitators may be offered in the form of emotional support, sharing of information, and practical assistance. On the other hand, imposed effects of mental illness, poor self-concept, and social obstacles may hinder or delay the RTW. Overall, family members, friends, coworkers, supervisors, managers, MHPs, and the government are important sources in providing facilitators. However, sometimes, they may not cooperate with the RTW of WPSMI. Hence, MHPs and politicians are recommended to consider the facilitators and barriers of the RTW and sources that assist WPSMI in the RTW. Further studies may focus on empowering sources that provide the facilitators of the RTW.
Footnotes
Acknowledgements
We would like to extend our gratitude and appreciation to Vice-Chancellor for Research and Technology and all the people with SMI, their families, coworkers, employers, supervisors, managers, mental health care professionals, the Welfare Organization, and the Imam Khomeini Relief Committee. This manuscript was published by Research Square as preprint with DOI: 10.21203/rs.3.rs-382274/v1.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project has received funding from the Vice-Chancellor for Research of Hamadan University of Medical Sciences 2020 research (Grant agreement: No. 9906254144).