
Abstract
Background:
Antenatal depression is associated with several adverse maternal outcomes, perinatal outcomes, lower academic achievements in adolescence, and future mental health problems for the mothers. Early identification and effective treatment of depression in antenatal women can also improve perinatal outcomes.
Aim:
This study aims to understand the prevalence of antenatal depression and anxiety disorder, along with associated factors, among antenatal women attending the outpatient clinic of the obstetrics department in a tertiary care hospital.
Methods:
A cross-sectional design was employed for determining the prevalence, while a case-control framework was used for analysis of the associated factors. Semi-structured sociodemographic pro forma, Patient Health Questionnaire (PHQ-9) Tamil version, and Generalised Anxiety Disorder (GAD-7) Tamil version were administered to antenatal women after obtaining informed consent. Those who scored above 10 points on the PHQ-9 or above 9 points on the GAD-7 were interviewed using the Mini-International Neuropsychiatric Interview (MINI) diagnostic interview schedule, by a psychiatrist, for confirming the diagnosis.
Results:
In our sample, 22% of the participants were diagnosed with depression, and 23% with generalized anxiety disorder (GAD). Twenty-eight participants (13.4%) had both depression and GAD. Antenatal depression was associated with alcohol use in the spouse (P < 0.015), physical violence (P < 0.026), low perceived social support from the in-laws (P < 0.039), and pressure to have a male child (0.001). Antenatal GAD was associated with low perceived social support from the in-laws (P < 0.039) and pressure to have a male child (P < 0.041).
Conclusion:
The occurrence of depression and generalized anxiety disorder is high in antenatal women. Our study identified relevant psychosocial factors that may be potential targets to develop effective interventions.
Depression and anxiety disorders do exist in a significant proportion of antenatal women attending an obstetric clinic. Regular screening will enable early identification and effective treatment of depressive and anxiety disorders in antenatal women.Key Messages:
Multiple factors, which vary depending on the local and cultural factors, have been shown to be associated with maternal depression. Financial difficulties, non-arranged marriage, marital conflict, preference for a male child, previous miscarriage, stillbirth, child with special needs, domestic violence, and a partner with alcohol dependence4–7 were some of the common factors identified in studies conducted in India. Good social support, high satisfaction with pregnancy, and multiparity were protective factors.6, 7
Depression in pregnant women is associated with poor quality of life, 8 an increase in suicidal behavior, 9 preterm birth, 10 low birth weight, 11 and poor nutrition in the child.12, 13 Further, antenatal depression can contribute to postnatal depression, which is associated with an increase in diarrheal diseases and an early cessation of breastfeeding and increases the chances of antisocial behavior, Attention Deficit Hyperactivity Disorder (ADHD )symptoms, emotional difficulties, and cognitive impairment in the child. 14 Maternal depression is associated with poor academic achievement in the adolescence. 15
Studies in low- and middle-income countries have shown that it is possible to successfully target maternal depression through lay workers trained in psychosocial interventions 16 and some such workers have been integrated in existing maternal and child health programs.17–19 Successful treatment of maternal depression has correlated with improvement in mother–child interaction and better rates for breastfeeding and vaccination.17–19 World Health Organization (WHO) has called for integration of mental health in maternal and child health programs, with a focus on recognition, prevention, early intervention, and treatment of maternal depression. 8
Yet, services for screening and treatment of depression in pregnant women are not available even in most tertiary care settings in India. There are few studies on antenatal depression and anxiety from India. This study aimed to evaluate the prevalence of antenatal depression, anxiety, and the associated factors in a tertiary care maternity hospital, as a first step towards implementing culturally sensitive evidence-based interventions.
Materials and Methods
The Setting
This study was conducted in the antenatal clinic in the department of Obstetrics and Gynecology in a tertiary care teaching hospital. The antenatal clinic is a busy unit, with an average of about 60 outpatient visits per day. This study was approved by the Institutional Ethics Committee and was conducted from January 2019 to March 2019.
Design
A cross-sectional design was employed for determining the prevalence, while a case-control framework was used for analysis of the associated factors.
Recruitment of Subjects
All women attending the antenatal clinic who were above the age of 18 and able to provide informed consent were recruited. Patients with mental subnormality and those who refused consent were excluded.
Procedure
The participants were screened for depression and generalized anxiety and evaluated for associated factors. Those who screened positive were interviewed by a psychiatrist for further diagnostic evaluation using the MINI diagnostic interview schedule. 20 Patients who qualified for a diagnosis of depression or anxiety were referred to the psychiatry department for further management.
Assessment and Diagnosis of Depression and Generalized Anxiety Disorder
The following instruments were used in the assessment:
Statistical Analysis
Statistical analysis was done using SPSS (Statistical Package for Social Sciences) version 20. The demographic and clinical data are presented in frequencies and mean and standard deviation. The chi-square and Fisher’s exact tests were used to assess the significance of associations between categorical variables. Multivariate analysis was performed using stepwise backward logistic regression models. The sample size calculated was 207 using Epi Info (version 6.1), using the following assumptions: prevalence of antenatal depression to be 16%, 4 precision of 5%, with an alpha error of 5%.
Results
All the women were married and living with their spouse. The majority of them were homemakers (179, 81.8%). Thirty-nine (18.7%) were in the first trimester, 83 (39.7%) in the second trimester, and 87 (41.6%) in the third trimester. Fifty-nine (28.2%) women had scores of 10 or more on PHQ-9, indicating possible depression.
Distribution of Sociodemographic and Clinical Variables
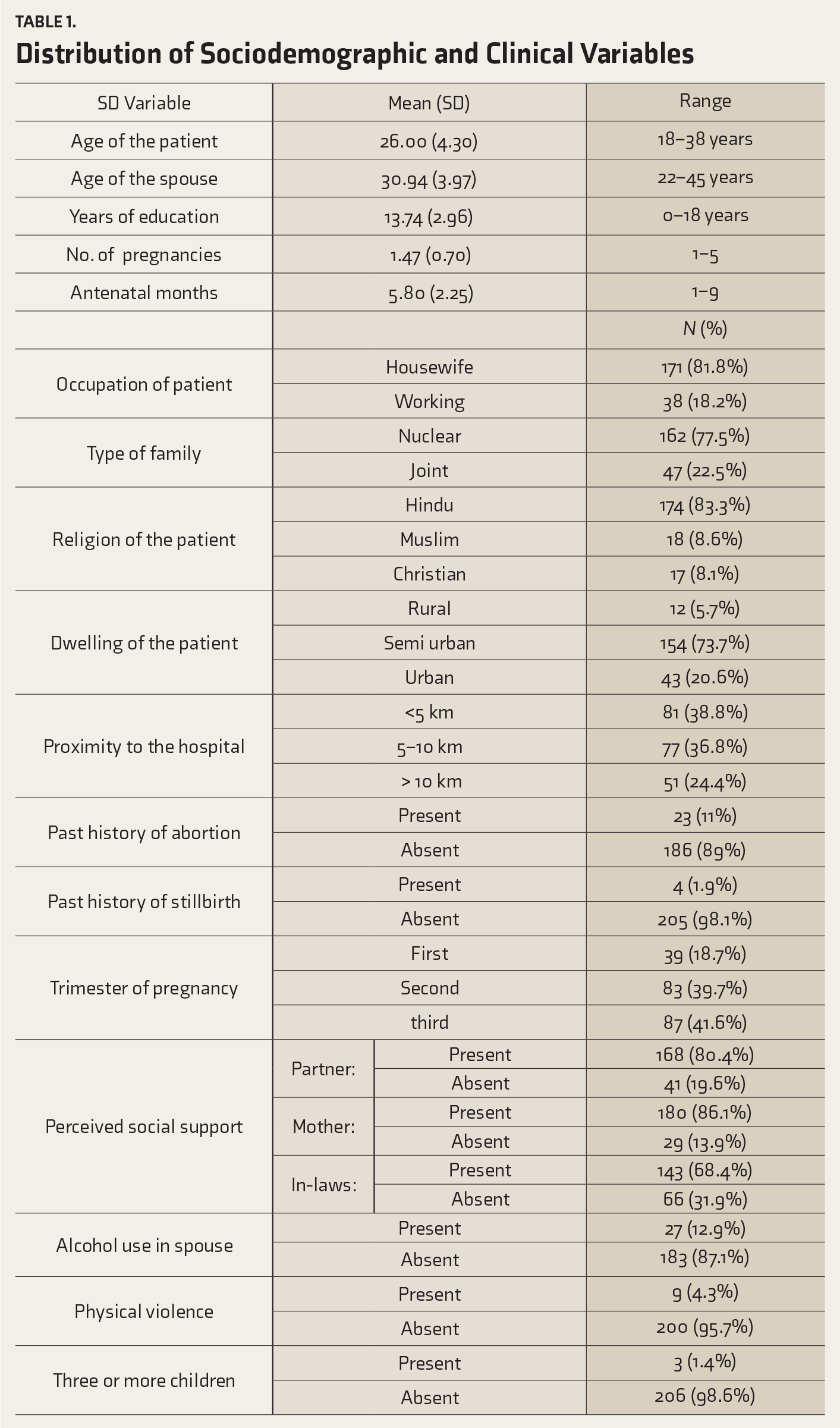
Of the 209 subjects, 59 (28.2%) were screened positive for depression with PHQ-9, and subsequently, the diagnosis was confirmed in 46 (22%) of them with MINI. Also, 49 (23.4%) were screened positive with GAD-7, and the diagnosis of GAD was confirmed in 48 (23%) with MINI. Twenty-eight subjects (13.4%) were diagnosed with both depression and GAD. Thirty-eight subjects (18.2%) had either depression or GAD and 143 subjects (68.4%) had neither.
Examining the association of the above sociodemographic and clinical characteristics with the diagnosis of depression and GAD revealed statistical significance for alcohol use in the spouse, physical violence, perceived poor support from in-laws, and pressure for a male child.
Factors Associated with Depression in Antenatal Women
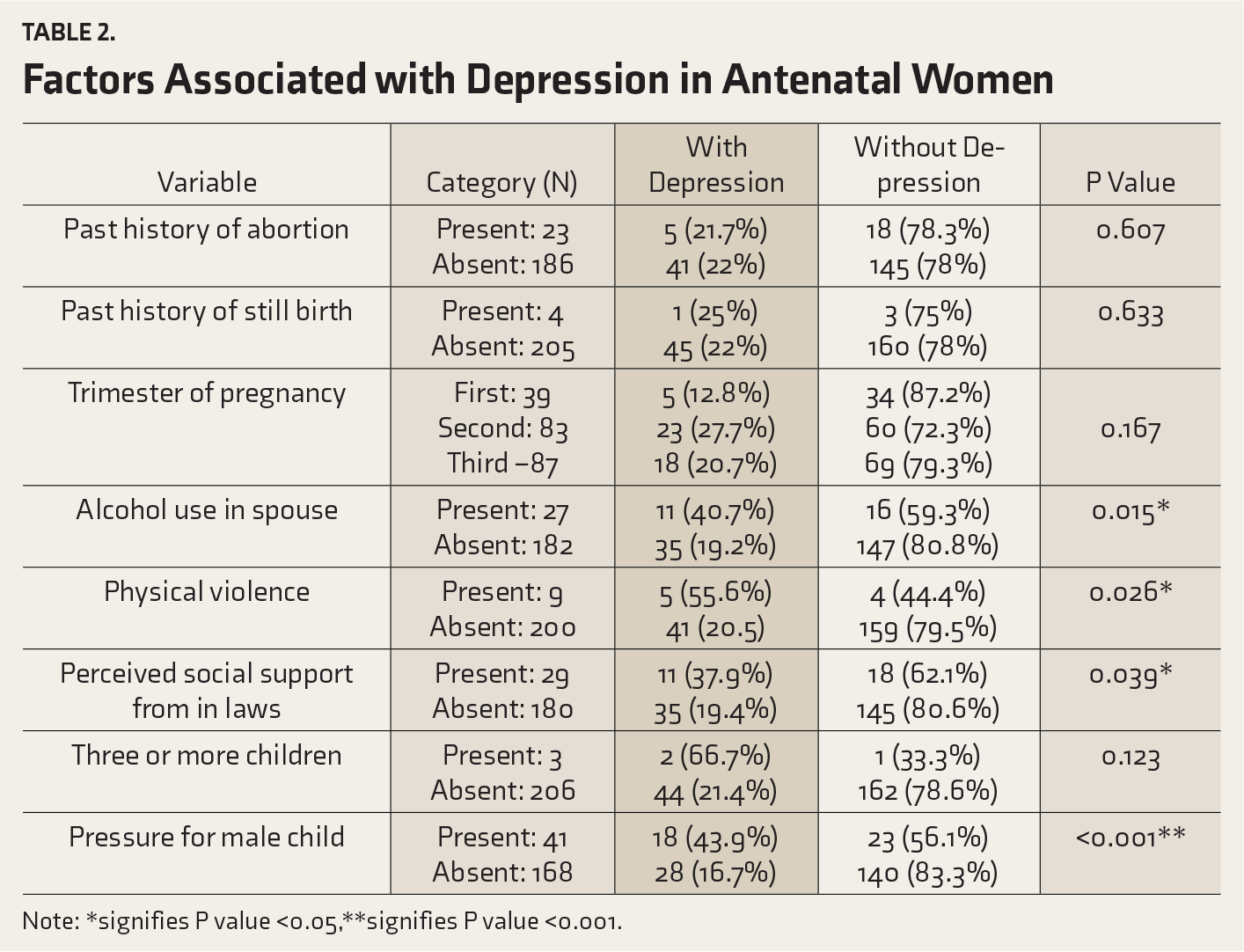
Note: *signifies P value <0.05,**signifies P value <0.001.
Factors Associated with Generalized Anxiety Disorder in Antenatal Women
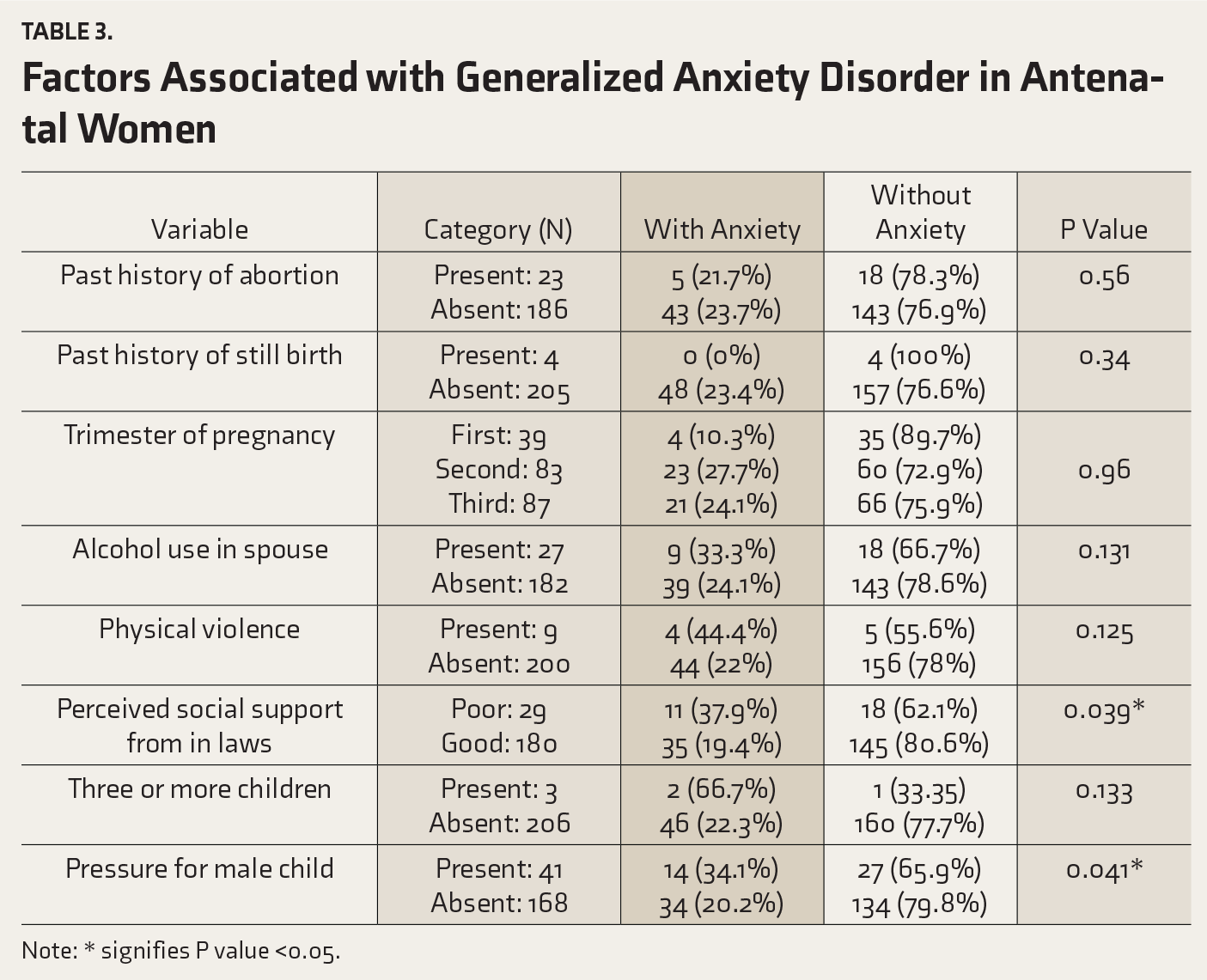
Note: * signifies P value <0.05.
A multivariate analysis was conducted entering variables with significance (P < 0.05) into stepwise logistic regression model.
Multivariate Analysis of Factors Associated with the Occurrence of Depression in Antenatal Women
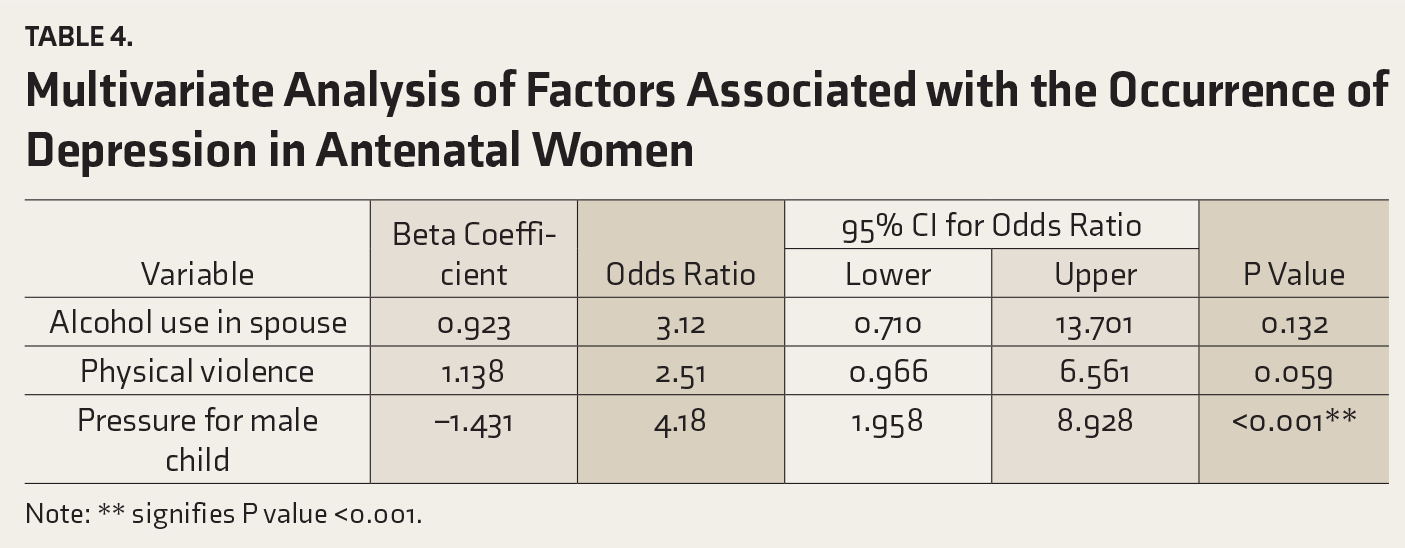
Note: ** signifies P value <0.001.
Discussion
Antenatal depression can lead to significant adverse outcomes for both the mother and the infant.3, 19, 23 According to studies from India, the prevalence of antenatal depression varies from 1.9% to 21.6%.24, 25 In our study, the prevalence of antenatal depression was 49 (22%). Like other studies from Low- and middle-income countries (LAMIC), this was much higher compared to the average prevalence (of about 10%) in developed countries. 3 The variability in the rates across the studies could be attributed to the difference in settings, tools used, and whether the diagnosis was based on only self-report measures or standardized diagnostic interview schedules.
The prevalence of depression we detected was also higher than the average of 16% reported from LAMIC. 3 The reason for this higher prevalence is unclear. Given that the sample was selected from a tertiary care hospital, one possibility is that those with obstetric complications are more likely to approach tertiary care centers, which might have contributed to the increased prevalence of depression. However, the rates of obstetric morbidity were not high in our sample and did not correlate with the prevalence of depression. The sample characteristics were comparable to those of other Indian studies from tertiary care centers in Bengaluru and Delhi, which reported a prevalence of 19% and 17%, respectively.24, 26 Two studies from Tamil Nadu had reported a lower prevalence of depression, around 14% 27 and 16.3%. 4 The first study 27 was conducted in three sites of rural Tamil Nadu, using Edinburgh Postnatal Depression Scale (EPDS), with a cutoff score of 13 for diagnosis. George et al. 4 conducted a community-level screening followed by a diagnostic interview and found that 16.3% of antenatal mothers had depression. Generally, obstetric centers in India are very busy, crowded, and with no privacy for conversation. In our study, care was taken to provide a private and confidential atmosphere for the participants to be screened and later interviewed. It could have led to a more open discussion about their mental state and hence, a better recognition of depressive symptoms.
The rate of alcohol use in spouses of our sample was 27 (12.9%), which was well below the prevalence of 34% 28 reported in the literature. It is likely that the participants under-reported the use of alcohol in their spouses, due to stigma.
Fewer studies on perinatal mental health have assessed the prevalence of anxiety. The prevalence of GAD was 48 (23%) in our sample, which is similar to Heyningen et al. 29 and Kang et al. 30
In our sample, diagnosis of depression was associated with alcohol use in the spouse, physical violence, reduced social support from the in-laws, and pressure for a male child. This is very similar to several other studies from LAMIC, 3 including India.4, 27 In the study by Kamali, 27 antenatal depression was associated with teenage pregnancies, spousal alcohol abuse, marital conflict, and perceived lack of social support. Further analysis in that study suggested that alcohol abuse could be contributing to depression by worsening marital discord and poor social support. This finding highlights how social determinants are inextricably linked to mental health issues in women. Unlike other studies,3, 13 in our study there was no significant association between the obstetric outcomes in the past or trimester of pregnancy.
There was a trend towards statistical significance of GAD, becoming worse in the second and third trimesters. Kang et al. 30 found that anemia, pregnancy-induced hypertension, and family discord were related to antenatal anxiety. In a study from South Africa, 29 history of mental health problems, multi-gravidity, food insecurity, unwanted pregnancies, life-threatening events, and pregnancy loss was associated with antenatal anxiety. They also found that better social support mitigated the impact of other factors. In this study, we found that anxiety was related to pressure for a male child and perceived social support but not past obstetric history.
The screening process in our study helped identify 66 women out of 207, who were offered psychological interventions, which highlighted the importance of screening antenatal women for mental health conditions.
Limitations
We relied on a self-report instrument, and it is possible that the patients under-reported their symptoms. This also raises some concerns about the accuracy of the self-reported symptoms due to a lack of collateral information. The study design was cross-sectional, and we do not have a sense of the longitudinal course. Though we asked the subjects if they had any co-morbid medical conditions at the time of screening, no formal medical tests were conducted.
Conclusion
Antenatal depression and anxiety are common and often not diagnosed. Screening for perinatal depression and culturally sensitive evidence-based treatment are likely to positively impact on the maternal well-being and child development. Both depression and GAD
in antenatal women seem related closely to social factors. Hence, prevention and treatment approaches should include culturally appropriate psycho-social interventions integrated with existing evidence-based mental health treatments.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.