
Abstract
Background:
Impulsivity is a multifaceted construct that plays a prominent role in substance use disorder (SUD). The UPPS-P model distinguishes five impulsivity components (positive urgency, negative urgency, lack of perseverance, lack of premeditation, and sensation seeking). This study aimed to explore the structure of the UPPS-P in patients hospitalized for SUDs and to investigate the relationship between the dimensions of impulsivity and clinical variables.
Method:
Inpatients of a residential detoxification service (n = 125) were recruited. A confirmatory factor analysis was performed, and associations were assessed between the components of impulsivity and clinical indexes.
Results:
The factor analysis supported a model of impulsivity with five interrelated latent variables. Good internal consistency was found. External validity was supported by relationships with psychological difficulties. Multiple correlations (Kendall) suggested that, except for its sensation-seeking component, impulsivity is a significant risk factor for both the severity of addictive problems and their comorbidities.
Conclusion:
This study provides further evidence in favor of the 5-dimensional model of impulsivity. It highlights impulsivity as a transdiagnostic risk factor that should be considered in the management of SUD.
The validity of the five-dimensional model of impulsivity (UPPS-P) has been confirmed in a sample of substance use disorder (SUD) patients in treatment. Lack of perseverance and premeditation emerged as quite critical impulsivity dimensions to consider in the treatment of SUD patients. Role of the lack of persistence and premeditation suggests that the ability to stay focused on one’s goal of sobriety and the ability to anticipate adaptive responses to cravings would be key challenges in the treatment of patients with SUD. All dimensions of impulsivity except sensation seeking appear to be involved in the comorbid difficulties observed in patients with SUD.Key Messages:
There is increasing evidence for a model of impulsivity consisting of five interrelated dimensions: (1) negative urgency (tendency to overreact in situations that induce unpleasant emotions), (2) positive urgency (expressing overreactions to emotions that are experienced as pleasant), (3) lack of perseverance (difficulty in staying focused on a task when it is perceived as difficult or boring), (4) lack of premeditation (difficulty anticipating the consequences of one’s actions before undertaking them), and (5) sensation seeking (tendency to seek out stimulating or exciting activities and new and unconventional experiences).1–7 The development of this model was accompanied by the construction of a 20-item questionnaire, the Urgency, Premeditation, Perseverance, Sensation Seeking–Positive Urgency (UPPS-P) Impulsive Behavior Scale. 8 This tool has been validated multiple times in various languages.1–3,5,6,8–11 In addition to this five-factor model, some authors argued for a hierarchical representation that identifies three interrelated higher-order constructs of impulsivity.8–10 According to them, positive and negative urgency could be grouped in a higher-order construct of general urgency, lack of premeditation and perseverance could fall under a higher-order construct called “consciousness”, and sensation seeking would be a separate dimension.
Several studies showed that the five dimensions of the UPPS-P predict the presence of substance use disorders (SUDs) and various psychological disorders such as depression, anxiety, or borderline personality,12–14 which are often regarded as comorbid conditions making SUDs more severe and more difficult to overcome.15–19 High impulsivity scores, particularly in lack of premeditation and negative urgency, were also associated with poorer outcomes to SUD treatment.13, 20 Furthermore, low motivation to abstain, low self-efficacy, and high levels of craving tend to predict relapse to addiction. 21 Some aspects of impulsivity are associated with craving 22 and, therefore, a greater likelihood of relapse. However, no or few studies 12 had specifically examined the relationship between UPPS-P scores, difficulties comorbid with SUD, and factors involved in the relapse process, such as motivation, self-efficacy, or craving, which would provide insight into the interrelations between UPPS-P dimensions and the clinical aspects of SUDs from a transdiagnostic perspective.
This study had two purposes. The first was to assess impulsivity in an inpatient population treated for severe SUDs, in an attempt to replicate the correlated five-dimensional structure of the UPPS-P found in other populations. The second was to determine whether the different dimensions of impulsivity are correlated, on the one hand, with motivation to abstain, the feeling of self-efficacy for abstinence, and the intensity and frequency of craving experienced during detoxification and, on the other hand, with a set of comorbid psychological difficulties generally reported in SUDs. We thus assessed anxiety and depressive symptoms, as well as the level of perceived stress, tendency to ruminate, heightened emotional reactivity, and lack of emotional awareness and low self-esteem, which are risk factors for various psychological disorders.
Method
Sample Size Calculation
Determination of sample size was based on an a priori power analysis, considering the expected effect size for the confirmatory factor analysis (RMSEA <0.05), a minimum number of degrees of freedom of 160, an alpha level of 0.05, and statistical power of 0.80. The analysis revealed that the minimum sample size for the model is 125 participants. This sample allowed us to detect at least moderate size correlation r = 0.26 (corrected α = 0.035, 1 – β = 0.80.).
Sample
The sample comprised 125 patients admitted to a residential detoxification service attached to a hospital specializing in psychiatric problems. Admissions were exclusively voluntary, and, for each patient, hospital stays and care were financed for more than 80% of the costs by the public welfare system, with possible participation of the patients’ private insurance. After a possible short period of withdrawal from the substance, the patients entered a 4-week treatment program aiming to help them develop a set of behaviors and knowledge that promote abstinence. Regardless of the substances used, patients were invited to participate in psycho-education sessions, group discussions, individual interviews, therapeutic physical activities, and occupational therapy to promote abstinence, mental and physical well-being, and self-reflection. If required, the patient could be given psychotropic medication to secure or facilitate withdrawal (e.g., benzodiazepines) or for comorbid psychiatric symptoms (e.g., antidepressants). Substitution products (e.g., methadone) were not used. Patients were excluded if they used any unprescribed substances during the treatment. Recruitment took place from December 2019 to June 2021, with a break from March 2020 to April 2021 due to the COVID-19 pandemic. The survey was proposed to all persons newly admitted in the unit, provided that they had a sufficient understanding of French, that their cognitive and emotional situation allowed taking it, and that they signed an agreement to participate.
Questionnaires
Sociodemographic Information
Data on sex, age, education, and income are reported in the first part of Table 1.
Descriptive Statistics.
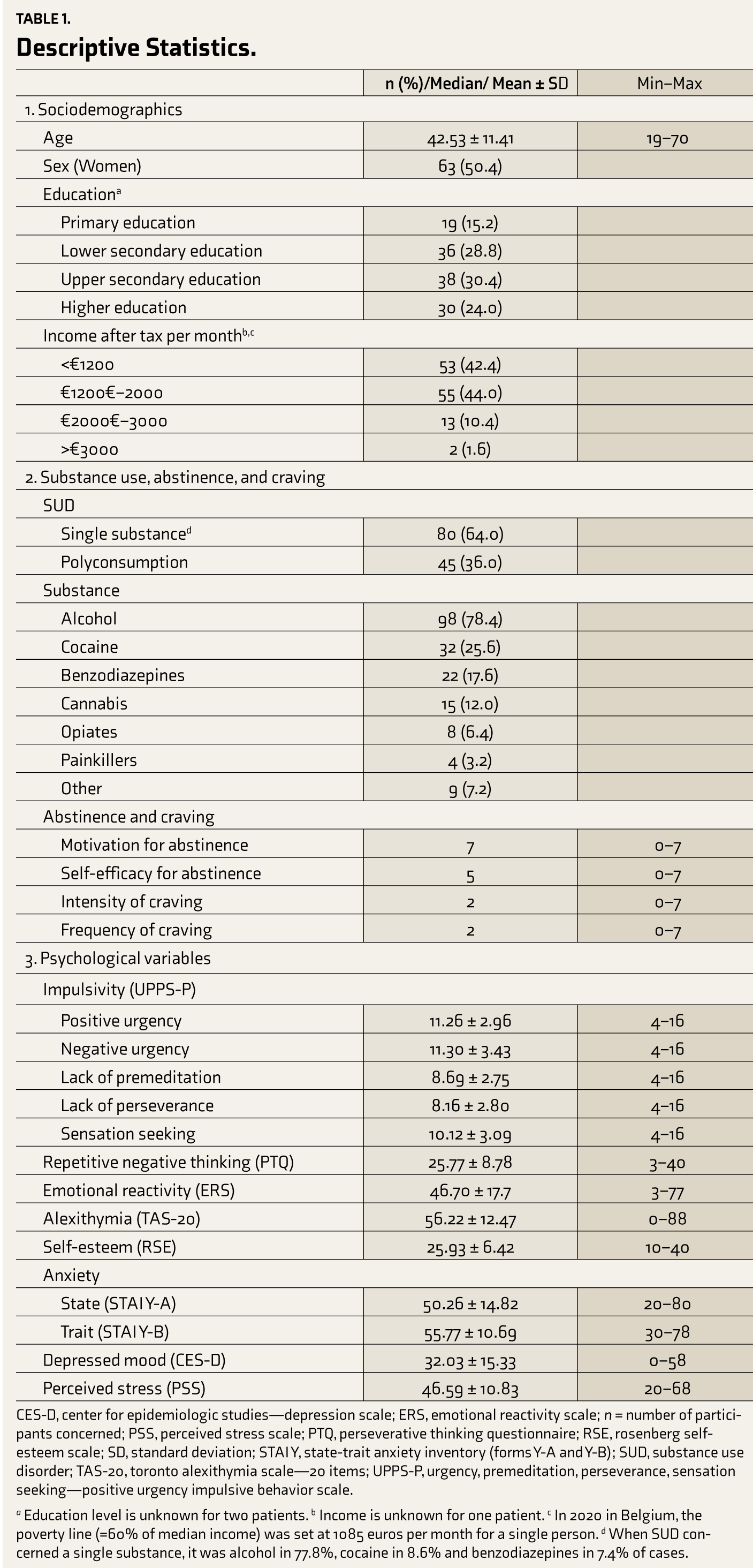
CES-D, center for epidemiologic studies—depression scale; ERS, emotional reactivity scale; n = number of participants concerned; PSS, perceived stress scale; PTQ, perseverative thinking questionnaire; RSE, rosenberg self- esteem scale; SD, standard deviation; STAI Y, state-trait anxiety inventory (forms Y-A and Y-B); SUD, substance use disorder; TAS-20, toronto alexithymia scale—20 items; UPPS-P, urgency, premeditation, perseverance, sensation seeking—positive urgency impulsive behavior scale.
a Education level is unknown for two patients. b Income is unknown for one patient. c In 2020 in Belgium, the poverty line (=60% of median income) was set at 1085 euros per month for a single person. d When SUD concerned a single substance, it was alcohol in 77.8%, cocaine in 8.6% and benzodiazepines in 7.4% of cases.
Abstinence and Craving
Patients were interviewed about the number and the nature of substances used. In the case of poly-consumption, the substances were prioritized according to their severity of use. The levels of motivation to abstain, self-efficacy to abstain, and intensity and frequency of craving were considered in relation to the substance described as the most problematic.
Motivation for abstinence. Motivation to stop using (i.e., “Currently, how much do you want to be abstinent from this substance?”) was measured using a 7-point Likert scale (ranging from 1 = “I do not wish to become abstinent” to 7 = “I wish to maintain total and definitive abstinence”).
Abstinence self-efficacy. The feeling of self- efficacy in abstinence (i.e., “How well do you feel you are currently able to live without this substance?”) was measured using a 7-point Likert scale (ranging from 1 = “I feel absolutely incapable of living without this substance” to 7 = “I feel perfectly capable of living without this substance”).
Craving. The intensity and frequency of craving experienced during the first 2 weeks of treatment (i.e., “During the past two weeks, what was the average intensity/frequency of your craving for this substance?”) were evaluated using a 7-point Likert scale (ranging from 1 = “I had no craving” to 7 = “The craving was extremely intense/frequent”).
Psychological Variables
Impulsivity: Impulsivity was assessed using the short French version 8 of the UPPS-P Impulsive Behavior Scale, 7 which consists of 20 items, related to the five dimensions, in the form of a 4-point Likert scale (ranging from 1 = “strongly disagree” to 4 = “strongly agree”). High values characterize impulsive tendencies.
Repetitive negative thinking: The propensity to experience excessive and repetitive thinking about negative topics 23 was assessed by the French version 24 of the Perseverative Thinking Questionnaire (PTQ). 25 This 10-item questionnaire, rated on a 5-point Likert scale (ranging from 0 = “never” to 4 = “almost always”), assesses the extent to which the individual usually experiences negative, repetitive, and intrusive thoughts that affect their mental resources. The scale produces a total score between 0 and 40. High scores characterize a high propensity for mental ruminations.
Emotional reactivity: Emotionality was measured by the French version 26 of the Emotional Reactivity Scale (ERS). 27 This 21-item questionnaire, which uses a 5-point Likert scale (ranging from 0 = “not at all like me” to 4 = “completely like me”), produces a total score between 0 and 84. The more emotionally reactive the person is, the higher the score.
Alexithymia: The difficulty in identifying, describing, and expressing emotions was assessed by the French version 28 of 20-item Toronto Alexithymia Scale (TAS-20). 29 This consists of 20 items assessed on a 5-point Likert scale (ranging from 1 = “strongly disagree” to 5 = “strongly agree”). It produces a score between 20 and 80. A score ≤51 suggests non- alexithymia; 52–60 possible alexithymia, and >60, alexithymia disorder.
Self-esteem: This was measured by the French version 30 of the Rosenberg Self-Esteem Scale (RSE). 31 It consists of 10 items assessed by a 4-point Likert scale (ranging from 1= “strongly disagree” to 4 = “strongly agree”). Values <25 indicate low, 26–35 indicate normal, and >35 indicate high self-esteem.
Anxiety: The French version 32 of the State-Trait Anxiety Inventory (STAI, forms Y-A and Y-B) was used to assess state anxiety (form Y-A) and trait anxiety (form Y-B). Each of the two 33 forms includes 20 items assessing anxiety with a 4-point Likert scale (state anxiety: ranging from 1 = “no” to 4 = “yes”; trait anxiety: ranging from 1 = “almost never” to 4 = “almost always”). For both scales, scores can range from 20 to 80. A higher score indicates greater anxiety. According to Ercan et al., 34 a score above 44 for the trait subscale suggests an anxiety disorder. For both state and anxiety scales, Bruchon-Schweitzer and Paulhan 32 propose a transformation of the raw scores into standard scores of a mean of 50 and standard deviation of 10; scores >55 were regarded to indicate high levels and >65, very high levels of anxiety.
Depressed mood: The frequency of depressive symptoms experienced during the last 7 days was assessed with the French version 35 of the Center for Epidemiologic Studies – Depression Scale (CES-D). 36 It consists of 20 items rated on a 4-point Likert scale (ranging from 0 = “never or very rarely” to 3 = “frequently, all the time”). The total score ranges from 0 to 60, with higher scores indicating higher symptom severity. Scores ≥16 and ≥20 indicate a depressive state in men and women, respectively. 37
Perceived stress: The extent to which life situations were perceived as threatening during the last 2 weeks (i.e., unpredictable, uncontrollable, and distressing) was assessed using the French version 38 of the Perceived Stress Scale (PSS). 39 It consists of 14 items rated on a 5-point Likert scale (ranging from 1= “never” to 5 = “often”) and produces scores that range from 14 to 70. The higher the score, the greater the perceived stress.
Procedure
Within a week of admission to detoxification, the patients were invited to complete the following questionnaires: sociodemographic questionnaire, identification and prioritization of substances according to the severity of use, assessment of motivation and abstinence self-efficacy for each substance, UPPS-P, ERS, TAS, CES-D, STAI Y A-B, PSS, PTQ, and RSE. Fourteen days later, the craving experienced since substance cessation was assessed.
Statistical Analysis
We performed a confirmatory factor analysis using weighted least squares estimation with robust standard errors and a mean- and variance-adjusted test statistic (WLSMV) with the Lavaan package in R, version 0.6–8. This method produces accurate parameter estimates in case of small sample size and categorical non-normal data.40, 41 Three different models were tested. The first model identifies a unitary impulsivity construct (Model 1). The second model identifies a factorial structure with five correlated dimensions (Model 2):1–3,5,6,9 positive urgency (items 2, 10, 15, 20), negative urgency (items 4, 7, 12, 17), lack of premeditation (item 1, 6, 13, 19), lack of perseverance (items 5, 8, 11, 16), and sensation seeking (item 3, 9, 14, 18). The third hierarchical model identifies three interrelated impulsivity constructs (Model 3):8–10 positive and negative urgency represent a higher-order construct of general urgency, lack of premeditation and lack of perseverance loads on a higher-order construct called “conscientiousness”, and sensation seeking is a separate dimension. A non-significant χ² indicates a good model fit. If the χ² is significant, a χ²/degree of freedom ratio of <2 indicates a good fit, while a result of <3 is acceptable. 42 We also computed several other fit statistics, including the Root Mean Square Error of Approximation (RMSEA), the Standardized Root Mean square Residual (SRMR), the Tucker-Lewis Index (TLI), and the Comparative Fit Index (CFI).42–44 RMSEA between 0.05 and 0.08, SRMR <0.10, TLI >0.90, and CFI >0.90 are generally interpreted as indicating an acceptable fit.43, 45 We also explored the internal consistency of each UPPS-P subscale using the McDonald’s omega. 46 Values ≥0.70 are considered acceptable.
Second, we determined whether the dimensions of impulsivity were correlated with abstinence motivation, abstinence self-efficacy, intensity and frequency of craving, as well as with repetitive negative thoughts, emotional reactivity, self-esteem, state anxiety, depressive symptoms, and perceived stress. We performed bilateral Kendall’s correlations to take into account violations of normality in our data. The Benjamini–Hochberg procedure for correction for multiple testing was applied in order to identify significant correlations.
Results
Description of the Sample
The sample consisted of 125 participants. All had severe SUD according to DSM-5 criteria. Nearly 100% of those offered the opportunity to participate in the study accepted, and the actual participation rate is estimated at over 90%. Losses in numbers were mainly due to people who very quickly ended their hospitalization for personal reasons. The women were slightly older (mean ± SD, 44.7 ± 11.5 years) than men (40.4 ± 11.0 years) (t123 = 2.13, p = 0.036, Cohen’s d = 0.38) and also less involved in cocaine use, with 15.9% of them using it compared to 35.5 % of men (Fisher’s exact test: p = 0.014, φ = 0.23, Table 1).
Of the 125 patients, 49 discontinued their treatment before its expected end. For five of them, this choice was due to the disruption caused by the COVID-19 pandemic. For 18, the healthcare team indicated that the treatment was not appropriate to their current expectations or capacities (e.g., they did not want or were unable to remain abstinent during treatment). For the other 26, we do not have explicit information about the reasons.
Confirmatory Factor Analysis
The one-factor model had a poor fit [χ²(170) = 408.36, p < 0.001, RMSEA = 0.11, SRMR = 0.14, TLI = 0.54, CFI = 0.59]. The five correlated dimensions had an acceptable fit [χ²(160) = 185.11, p = 0.086, RMSEA = 0.036, SRMR = 0.065, TLI = 0.95, CFI = 0.96]. In comparison, the hierarchical model had a slightly worse fit [χ²(163) = 206.54, p = 0.012, RMSEA = 0.047, SRMR = 0.075, TLI = 0.91, CFI = 0.93]. The χ² difference testing confirmed that the five correlated dimensions model had a significantly better fit than the hierarchical model [χ²(3) = 21.43, p > 0.001]. Item loading and intercorrelations for the retained model are reported in Figure 1. Excellent internal consistency was found for all subdimensions [ωNegative urgency = 0.82, ωPositive urgency = 0.74, ωLack of premeditation = 0.81, ωLack of perseverance = 0.84, ωSensation seeking = 0.79].
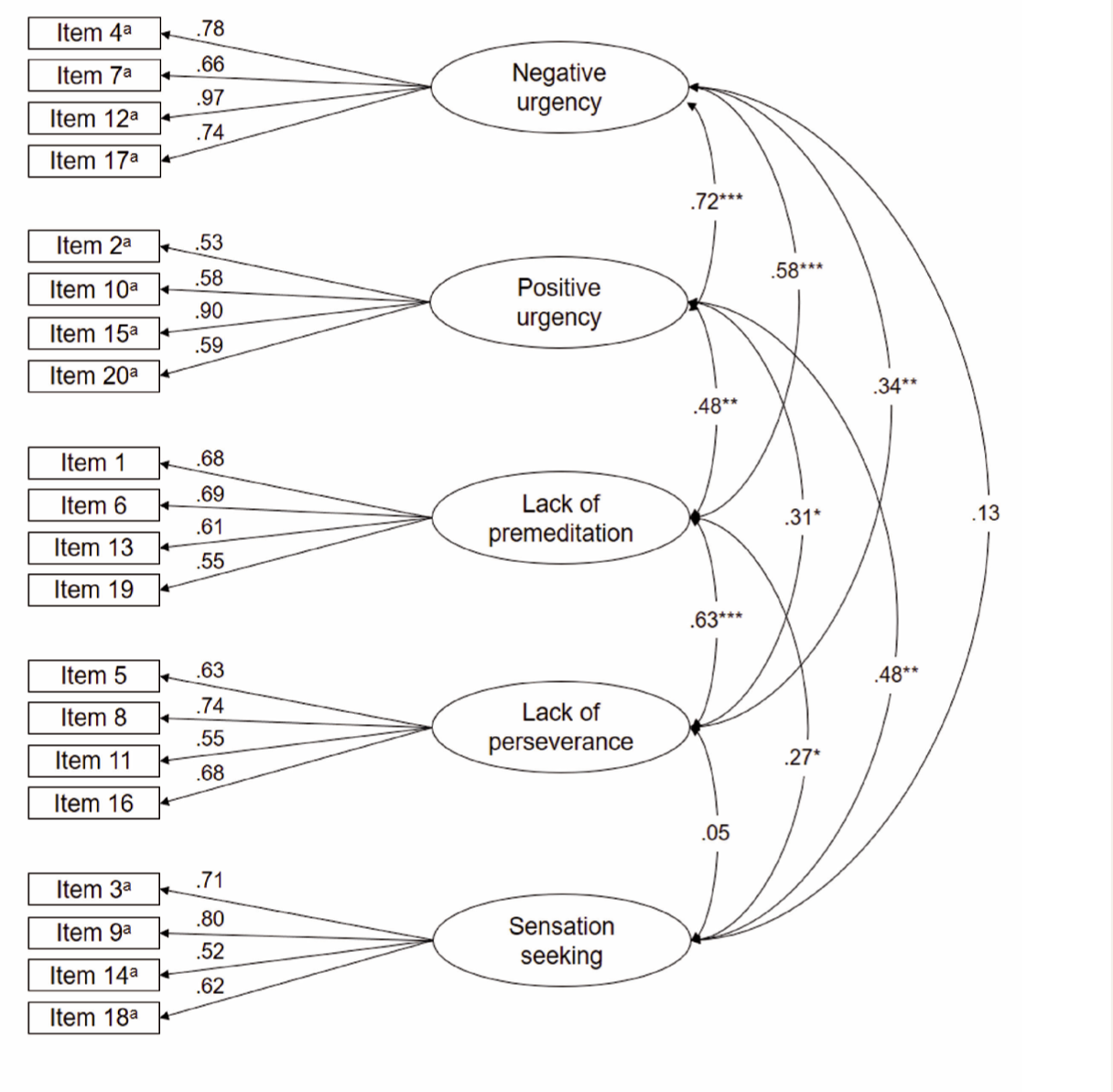
Standardized factor loading and correlations between factors. a opposite items. * p < 0.05, ** p < 0.01, *** p < 0.001. UPPS-P, urgency, premeditation, perseverance, sensation seeking—positive urgency impulsive behavior scale.
Correlations Between UPPS-P Scores and Clinical Variables
Among the patients, 77.4% could be considered as having a depressive state, 73% had a high to very high (50.4%) level of state anxiety, 83.1% could be regarded as having a probable anxiety disorder, 43% had probable alexithymia, and 40% had low self-esteem (Table 1).
Kendall’s correlations between UPPS-P subdimensions and clinical variables were performed (Table 2). After correcting for multiple testing (Benjamini-Hochberg correction: p ≤ 0.035), results revealed negative correlations between motivation to abstain, on the one hand, and positive urgency and lack of perseverance on the other. Self-efficacy for abstinence was negatively correlated with lack of perseverance. The intensity and frequency of perceived craving were positively correlated with lack of premeditation and perseverance. Negative urgency, positive urgency, lack of premeditation, and perseverance were positively correlated with repetitive negative thinking, emotional reactivity, state anxiety, depressed mood, perceived stress, and alexithymia (except for lack of perseverance). Conversely, these four dimensions of the UPPS-P were negatively correlated with self-esteem. Finally, only the sensation-seeking dimension was positively correlated with emotional reactivity. Considering the criterion of the strength (≥0.30) of the correlations, it appears that, overall, the clinical variables covary the most with lack of premeditation.
Kendall’s Correlations (τ) between Dimensions of Impulsivity and Clinical Variables.
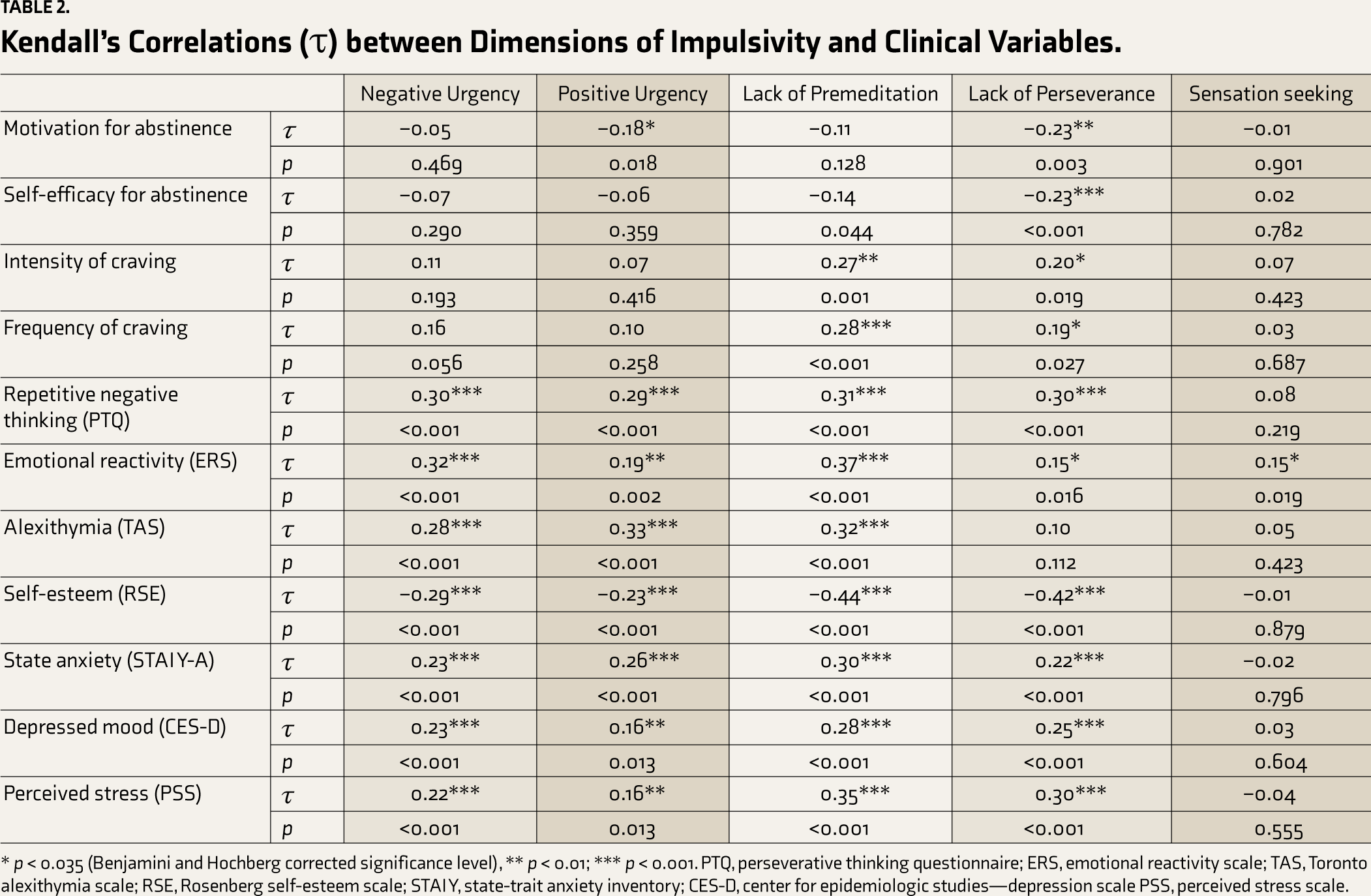
* p < 0.035 (Benjamini and Hochberg corrected significance level), ** p < 0.01; *** p < 0.001. PTQ, perseverative thinking questionnaire; ERS, emotional reactivity scale; TAS, Toronto alexithymia scale; RSE, Rosenberg self-esteem scale; STAI Y, state-trait anxiety inventory; CES-D, center for epidemiologic studies—depression scale PSS, perceived stress scale.
The 49 people who discontinued their treatment before its expected end had higher average scores than the others in lack of perseverance (Mann-Whitney U-test = 1037.50; df = 112; p < 0.003; d = 0.64) and premeditation (U = 1214.50; df = 113; p < 0.03; d = 0.49).
Discussion
We examined the psychometric properties of the short French version of the UPPS-P in a sample of detoxification patients. Confirmatory factor analysis revealed that the five latent variables cross-correlated models showed the best fit rather than unitary or hierarchical models.1–3,5 These results are quite similar to those reported by another French-speaking team 9 on patients also hospitalized for SUD but more widely involved with opiates. Second, the internal consistency of the subscales was good. Third, construct validity was confirmed by specific relationships with clinical variables.
While many studies have focused on the relationship between dimensions of impulsivity and substance (ab)use,47–49 our data suggested that certain dimensions of impulsivity are specifically related to the abstinence process. In particular, the motivation to abstain was negatively correlated with positive urgency and lack of persistence, whereas feelings of self- efficacy were negatively correlated with lack of persistence. We also observed that the intensity and frequency of craving positively correlated with lack of premeditation and persistence. These results may highlight the impact of difficulty in staying focused on one’s goal despite the troubles of the abstinence process. Self-reported craving appears to be more closely related to the difficulty in staying focused on one’s goals and the ability to anticipate and identify appropriate reactions when confronted with the substance. Thus, high levels of impulsivity may increase the likelihood of relapse. This echoes the results of Hershberger et al.’s meta-analysis, 13 which suggested that lack of premeditation and negative urgency are related to poorer psychotherapy outcomes.
Contrary to a series of studies suggesting that urgency is the dimension of impulsivity most likely to predict the severity of addictive behaviors,12, 50 our data rather draw attention to the role of lack of perseverance and premeditation. This might be related to the particularities of our sample, which was composed of patients in treatment. Their voluntary commitment to a detoxification process indicates a certain aspiration on their part to reduce consumption behaviors perceived as undesirable. This might be much less the case for participants in other studies on addictive behavior, who were not specifically treated, who were possibly less convinced of the problematic aspect of their behavior and, therefore, less strongly motivated to abstain than our patients claimed. As a result, the fairly strong and consistent motivation to abstain found in this sample may have mitigated disparities in urgency as they would be revealed in individuals less explicitly committed to a change process. In this regard, lack of perseverance and premeditation would likely be particularly critical variables for people who do complain of SUD and wish to overcome this difficulty. These factors may reveal a vulnerability consisting of low resistance to psychological discomfort and a low ability to project adaptive behaviors in situations where there is a chance of a lapse to substance use, which therefore represent points of focus for treatment strategies.
The high prevalence of depressive symptoms, anxiety, and alexithymic difficulties among our participants is consistent with frequent observations of an over-representation of psychopathology in people with SUD.15, 19,51,52 Unfortunately, therapeutic action becomes more complex and hazardous as the severity of the disorder and comorbid difficulties increase. 16 We also observed small to moderate correlations of positive urgency, negative urgency, lack of persistence, and lack of premeditation with psychological suffering. Similar correlations have been at least partially reported in the literature for other samples. For example, depressive symptoms have been explained by positive urgency, 3 negative urgency, lack of perseverance, and lack of premeditation.3, 12 Anxiety appears to be more correlated with positive urgency and negative urgency,3, 12 while perceived stress seems to be correlated with positive urgency, negative urgency, and sensation seeking. 3 Impulsivity clearly does not usurp its reputation as an overall risk factor for many clinical difficulties. Some even consider impulsivity a proximal transdiagnostic risk factor (i.e., within-person variables related more directly to disorders via specific mechanisms). 53
Finally, the explanatory role of sensation-seeking seems to be totally marginal. This is probably not unrelated to the essentially hedonistic dimension of this aspect of impulsivity, a search for pleasure that certainly explains risky behavior but fails to characterize SUDs or psychological difficulties.8, 54
The scope of our observations is limited by the specificity of our sample, which was composed of patients in treatment, who were, therefore, quite motivated to abstain and mostly willing to limit their substance use. On the other hand, the question of whether or not they had the means to achieve their desire to abstain (i.e., the criterion of self-efficacy) became central. These results certainly invite us to consider the dynamics involved in addiction, but we should be wary of generalizing to the entire population of people with SUDs. Furthermore, it should be borne in mind that some consider self-assessments, both in terms of craving and the ability to become abstinent, to be rather unreliable indicators of the severity of the disorder.55, 56 Finally, the relatively small sample size also limits the scope of the conclusions. It should be noted that as originally planned, notably in terms of duration, the study should have resulted in a sample size of 250 to 350 participants. However, disruptions due to the COVID-19 pandemic altered the original plans and reduced the sample size to 125. As noted in the Methods section, this proved sufficient for validating moderate to large effects, but the fact that most of the observed effects were precisely in the moderate range at most invites great caution in interpretation.
Conclusion
This study provides additional evidence in favor of the five-dimensional model of impulsivity as well as the high psychometric properties of the UPPS-P scale in a sample of inpatients in detoxification. Patients’ clinical status is correlated with the different dimensions of impulsivity, except for sensation seeking. Overall, it appears that impulsivity should be considered a necessary clinical management focus to improve clinical outcomes in SUDs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the University of Liège.