
Abstract
Background:
Cognitive control (CC), including shifting, updating, and inhibiting functions, may play an integral role in various aspects of psychotherapy; however, research on this is limited. This review aims to link the disparate lines of evidence on CC as they relate to psychotherapy processes, techniques, and outcomes.
Methods:
A systematic search of the literature on neuropsychological domains relating to psychotherapy in adults with anxiety/depression yielded 18 eligible studies. The review also uses a narrative format to explore other potential links between CC and psychotherapy that are underinvestigated, and highlights the need for research and application to evidence-based practice of psychotherapy.
Results and conclusions:
Findings suggest that CC may predict psychotherapy outcomes and also improve as a function of psychotherapy. Analog sample studies suggest a possible link between CC and techniques for regulation of cognition and emotion, such as reappraisal, mindfulness, and cognitive restructuring. CC may also play an integral role in the regulation of behavior. Study of CC in the context of psychotherapy may potentially explain individual differences in psychotherapy outcomes and mechanisms of action of various psychotherapy techniques and processes. Such an understanding may have possible implications for “best fit” matching clients to therapies and modifying psychological interventions to account for poorer CC abilities. CC may be enhanced through training and further research is warranted on the impact of such training in facilitating better long-term psychotherapy outcomes.
Cognitive control (CC; also termed executive functions) is the effortful deployment of cognitive resources for flexible, adaptive responses to changing contingencies. It includes three core processes—shifting (or cognitive flexibility, the ability to flexibly adjust to new demands, rules, or priorities), updating (or working memory, the ability to hold and manipulate information in mind), and inhibiting (or inhibitory control, the ability to override prepotent responses). 1 CC is linked to the activity of a superordinate system involving the dorsolateral, medial, and anterior cingulate prefrontal cortices (PFC), parietal cortex, basal ganglia, and cerebellum. 2 With its significance to psychopathology, 3 goal-pursuit, and flexible coping, 1 CC is highlighted as a Research Domain Criteria (RDoC) transdiagnostic construct, 4 and may also play an important role in psychotherapy.
Psychotherapy is an intensive, time-limited intervention with well-established effectiveness for a range of psychiatric disorders. 5 Nevertheless, answers are still elusive to the questions raised half a century ago—“What treatment, by whom, is most effective for this individual with that specific problem, under which set of circumstances?” 6 (p. 62). The critical tasks of psychotherapy include managing maladaptive emotions through tolerance, reappraisal or reflection, acquisition of new skills, and the “homework” practice of new techniques and strategies in extratherapeutic settings. In addition, client variables and processes critical to psychotherapy 7 include attendance and punctuality; persisting with therapy despite encountering maladaptive emotions; negotiating and collaborating with the therapist rather than displaying resistance; and learning and practicing new skills in the face of environmental pressures rather than falling back on usual dysfunctional coping techniques. The above appears to require an individual’s modulation of thought, affect, behavior, or attention, also referred to as “self-regulation,” subserved by the deliberate or automated use of CC mechanisms. 8
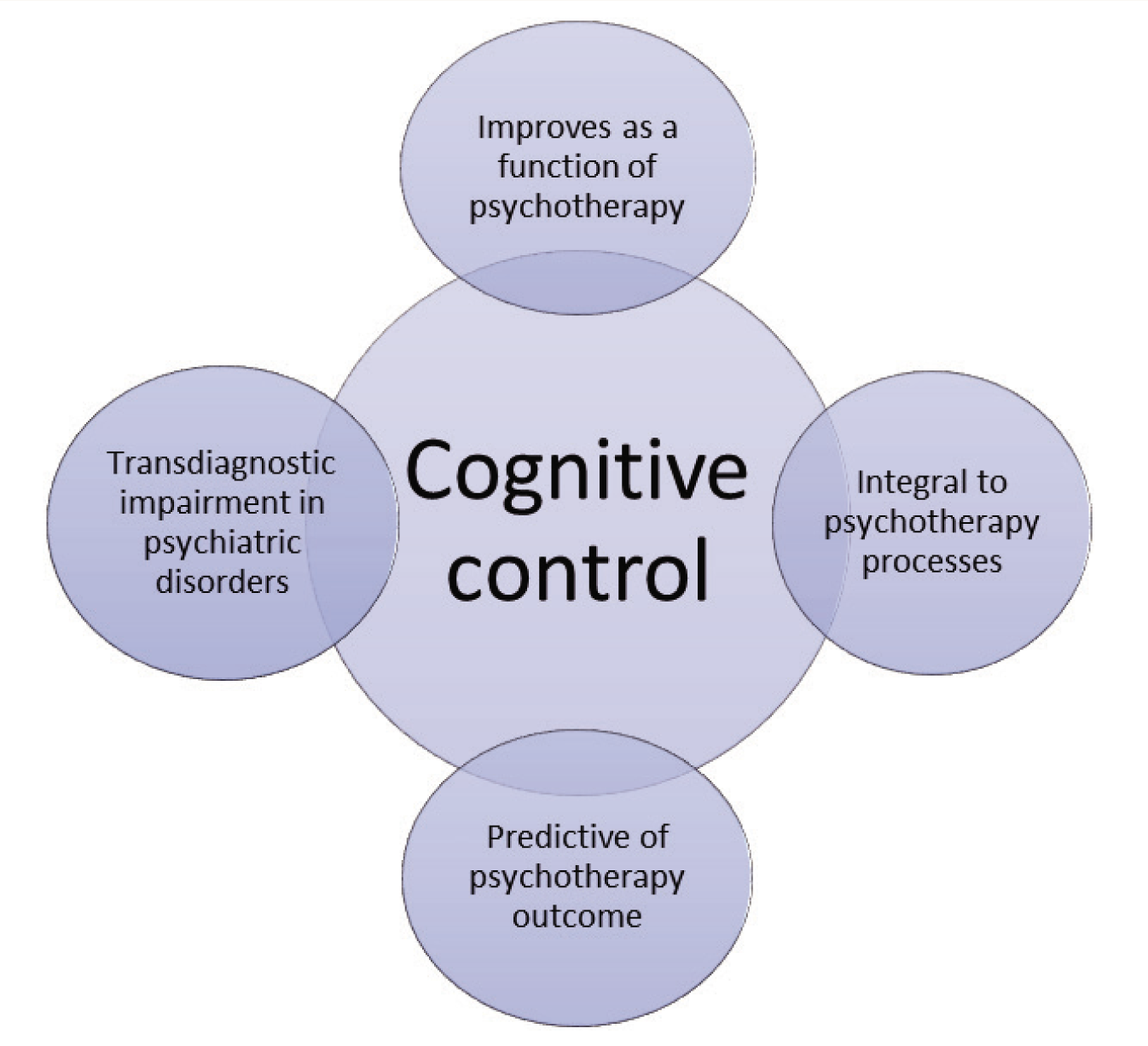
Despite receiving attention in the context of developmental processes,1, 9 psychopathology, 3 physical activity, 10 and eating behaviors, 11 CC has not been studied in relation to the self-regulatory processes required in psychotherapy. This appears to be part of a broader and oft-bemoaned difficulty in the marriage of ideas. Other researchers have pointed to the “parallel play” between clinical psychology/psychiatry and cognitive psychology/cognitive neuroscience, leading to failures in applying theoretical and methodological advances in one field to the other. 3 The postulation of CC as important to psychotherapy outcomes is borne out by some evidence. A few studies with geriatric and adolescent samples have examined the relationship of baseline cognitive functions with psychotherapy outcomes and compared different types of psychotherapy.12–14 Some evidence, predominantly from analog studies (e.g., non-clinical participants instructed to regulate emotion after watching a movie clip), demonstrates the link between CC processes and emotion regulation techniques.15–18 Research in adult clinical samples undergoing psychotherapy is limited, and evidence is mixed. While some studies suggest a role of CC in psychotherapy,19, 20 other studies show no significant relationships.21, 22 Neuroimaging studies largely show increased activation in CC brain circuits following psychotherapy. 23 Studies using standardized neuropsychological measures are few. It has been suggested that assessment of cognition could form another level of psychotherapy outcome measurement, allowing investigation of underpinning mechanisms that are not easily noticed clinically. 24 Nevertheless, these lines of evidence have remained largely disparate; there are considerable gaps in research on the mechanisms of change involved in psychotherapy and in translating this knowledge to clinical practice. This review attempts to draw together evidence of possible associations between CC and psychotherapy techniques, processes, and outcomes, in adult anxiety/depression samples and thus bridge existing knowledge gaps (Figure 1). The potential of CC training to enhance outcomes in psychotherapy is also discussed. Given the scant literature in the area, an integrated review was deemed appropriate.
Hypothesized Role of Cognitive Control in Psychotherapy.
Method
Eligibility Criteria
The review followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 25 guidelines. The integrated review consisted of, firstly, a systematic review with a clearly defined focus, as described below, followed by a narrative review with a broader focus. For the systematic review, studies on psychotherapy in anxiety and depressive disorders, reporting pre-post neuropsychological assessment data, on adult samples, were included. Anxiety and depression were selected since psychotherapy is an established first-line treatment in these disorders. Studies on psychotherapy in other psychiatric disorders (psychotic and bipolar disorders, substance use disorders, developmental disorders) or neurological conditions (epilepsy, stroke, degenerative disorders, tumors/lesions, traumatic brain injury) were excluded due to the variable extent of biological etiological factors, comorbidities, disability, and other treatments used in these disorders, which could confound the variable of CC. Studies primarily investigating other interventions (pharmacotherapy, brain stimulation, music/art therapy, journaling, self-help resources, cognitive remediation, physical exercise, herbal therapies) or on pediatric/geriatric/non-clinical samples were excluded. Neuroimaging studies were not included as several recent and comprehensive reviews exist.23, 26
Further, due to the small number of studies in this area, and in order to not overlook potentially important variables and relationships which may bear further exploration in future empirical studies, the systematic review was followed by a narrative integration of novel findings or theories from studies on nonclinical populations or children/adolescents/older adults, neuroimaging research, and theoretical articles.
Sources and Search Strategy
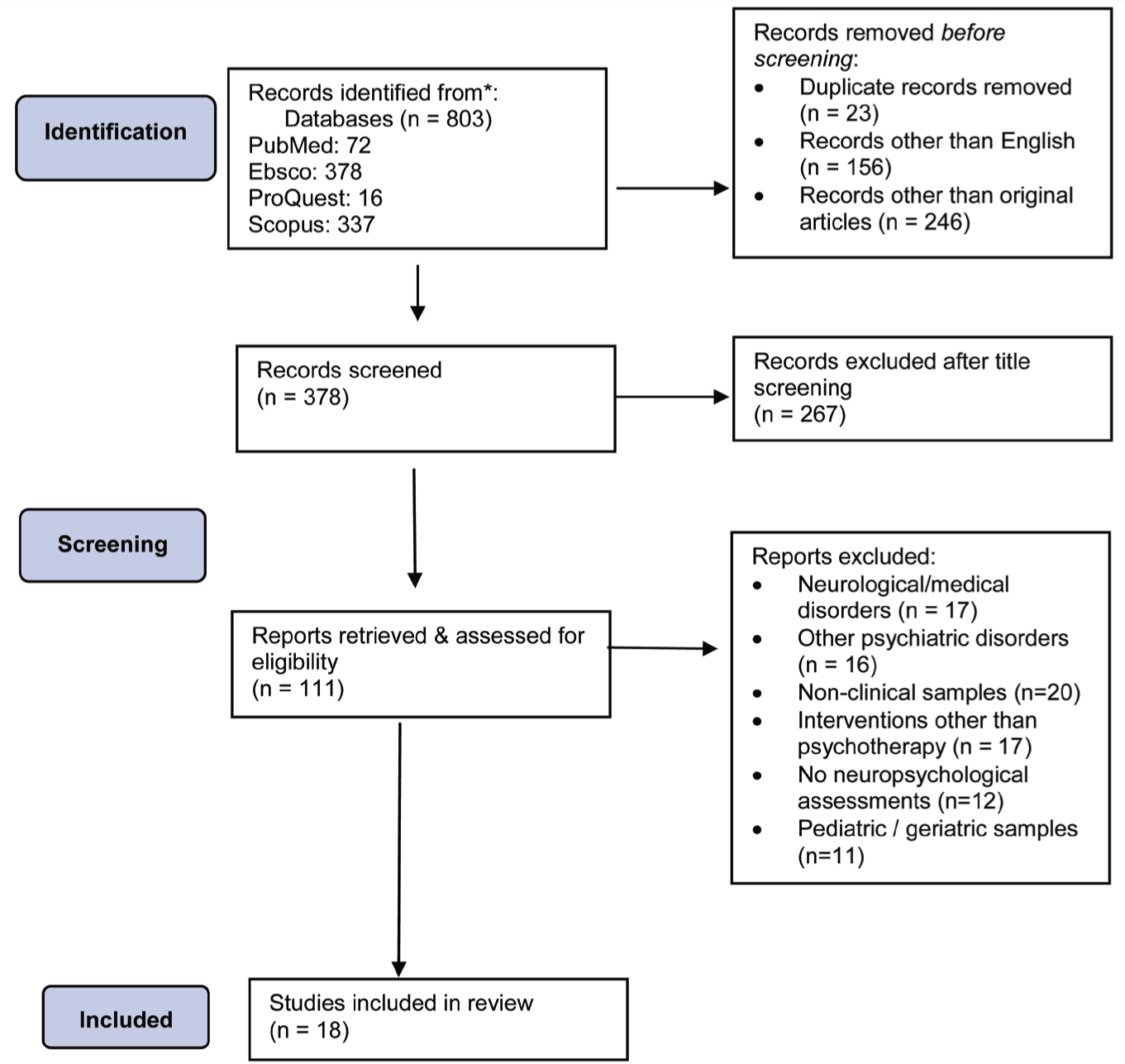
Electronic databases (PubMed, EBSCO, ProQuest, and Scopus) were searched. The search was executed within title/abstract, using the keywords “cognitive control”, “executive function”, “neurocognitive,” “neuropsychological”, “working memory”, “inhibitory control”, “cognitive flexibility” combined with “psychotherapy”, “therapy”, as well as combinations with “cognitive-behavioral”, “CBT”, “psychoanalytic”, “psychodynamic” “emotion regulation” with appropriate Boolean operators, and truncation and wildcard symbols. Filters were applied for language (English), article type (original article), subject headings/classifications as appropriate to each database (psychology/psychiatry/medicine/neuroscience/affective disorders/anxiety and depression/psychotherapy). After excluding duplicates, studies were assessed for eligibility through manual screening, filtering, and review of titles, abstracts, and full texts. Selected studies were searched for eligible cross-references. The first author executed the search between 2020 and 2022, with the most recent search retrieved on June 24, 2022. Decisions on inclusion/exclusion, when unclear, were resolved by consensus amongst the authors. The PRISMA flow chart for study selection is presented in Figure 2.
PRISMA Flow Chart for Study Selection.
Data Extraction, Charting, and Summarizing
Data extracted and charted from the selected studies comprised age, gender, diagnosis, sample size, details of psychotherapy (type, duration, and frequency), and pre-post neuropsychological domains assessed. The relationship of demo- graphic characteristics with CC or psychotherapy outcome was also extracted. While some studies examined CC as a predictor of psychotherapy outcome, others postulated improvement in CC over the course of psychotherapy, and a few examined measures that distinguished good versus poor response to psychotherapy. All such studies were included, regardless of the hypothesis tested, as long as pre-post data on at least one neuropsychological measure was reported. Pre-post data from 18 studies have been included (Table S1).
Since the review focuses on possible relationships between CC and psychotherapy processes, techniques, and outcomes, the relationships are operationalized and examined as follows—firstly, does psychotherapy contribute to improved CC, or conversely, does CC contribute to psychotherapy outcomes? Is CC part of existing psychotherapy techniques and processes? And finally, would enhancing CC improve psychotherapy outcomes?
Results and Discussion
Does Psychotherapy Improve Cognitive Control?
There are few published neuropsycho- logical studies of psychotherapy in anxiety and depression (Table S1). Studies of psychoanalytic/psychodynamic therapy in depression demonstrated improvements in CC (attention, processing speed, working memory, mental flexibility), and abstract reasoning.20, 27, 28 A comparison of metacognitive therapy (MCT) and cognitive-behavior therapy (CBT) for depression showed improvements in spatial working memory with MCT and verbal fluency with CBT 29 ; however, these were unrelated to clinical changes. Similarly, a comparison of schema therapy and CBT showed different predictors of response for each. 30 In a study on post-traumatic stress disorder (PTSD), improvements in CC and verbal memory were found in both arms, eye movement desensitization and reprocessing, and brief eclectic psychotherapy.31, 32 CC functions of flexibility, working memory, and inhibitory control have demonstrated improvements with psychotherapy across several studies.20, 29, 31–34 No post-therapy improvements or predictors of treatment were identified in some studies,21, 22 and the significance of persisting neuropsychological impairments has been highlighted.
Regarding demographic characteristics, most studies were comparable (Table S1). The relationship of demographic characteristics (age, gender, education) with CC and/or psychotherapy outcome was reported in eight studies only,21, 30, 34–39 with no significant relationships reported at baseline37–39 or over the course of treatment.21, 30, 34–36
Furthermore, a significant body of neuroimaging studies has demonstrated evidence of neuroplastic changes following psychotherapy for common mental disorders, which are common across styles of therapy, including cognitive-behavioral, psychoanalytic, and mindfulness-based therapies.40–43 The most consistently reported findings are of increased activation in dorsolateral PFC and anterior cingulate and reduced activation in medial PFC, orbitofrontal cortex, and amygdala. 26 It has been suggested that the increase in activation in prefrontal areas, particularly dorsolateral and anterior cingulate, indicates the recruitment of attentional systems and CC processes. Coupled with the reduced activation of “emotional” limbic areas, this suggests increased use of CC processes to regulate emotional arousal and reactivity (see Messina et al., 23 Santos et al., 26 and Brooks and Stein 43 for recent reviews).
It is worth noting that neuroimaging studies of psychotherapy far outnumber neuropsychological studies and provide more categorical evidence of improved CC functions following psychotherapy. The lack of neuropsychological studies and the observed inconsistencies across studies may perhaps relate to the sensitivity of tests and choice of outcome measures. 44
Is CC Predictive of Better Psychotherapy Outcomes?
It has been posited that well-functioning CC could be a prerequisite for effective psychotherapy. 12 Relatedly, executive dysfunction appears to predict a poorer outcome for CBT in pediatric obsessive–compulsive disorder (OCD). 19 In a study on older adults receiving CBT for generalized anxiety, those whose executive functions were intact at baseline, or improved during treatment, demonstrated better outcome measures from pre- to post-treatment, while stable executive dysfunction throughout treatment was linked to poorer response. 12 In empirical adult studies, predictors of psychotherapy outcome (Table S1) identified include CC variables and others—attention, 36 verbal fluency, 39 and verbal learning and memory.30, 32, 34, 37
CC has been posited as an antecedent to effective regulation of health behaviors (physical activity and eating), 45 through the ability to disengage from affective reactions towards temptations and inhibiting or overriding impulsive behavior responses; however, this has not been investigated in the context of psychotherapy.
CC may also be an important factor in decisions relating to the “best fit” of therapy for successful outcomes. For instance, older adults with depression and executive dysfunction demonstrated better outcomes with problem-solving therapy rather than supportive therapy (greater improvements in symptoms, executive functions, and disability scores). 46 One study in OCD showed that adolescents with poorer executive functions at baseline showed greater symptom reduction from CBT, 13 and attributed to gains from the highly structured approach of CBT, such as agenda setting, role modelling, in-session exercises, clear alternative plans, etc. These postulations merit further testing in adult psychotherapy samples.
Do Psychotherapy Techniques Recruit CC Processes?
It has been hypothesized that several adaptive strategies for managing thoughts, emotions, and behaviors may be underpinned by CC processes; however, much of the evidence comes from nonclinical samples.15, 47, 48 CC appears to be recruited by healthy individuals to regulate emotion but may be impaired in individuals with mood disorders. 49 It has been suggested that inhibitory control may be necessary for inhibiting prolonged rumination and negative affect, flexibility may be necessary for shifting attention away from emotional stimuli and towards the task at hand, while working memory may be necessary for updating task-relevant information (both emotional and nonemotional) and activating and maintaining an alternate representation of a situation in order to regulate emotion.15, 50, 51 Furthermore, effective regulation of health behaviors appears to be underpinned by executive attention, inhibitory control, and affect regulation; individuals who are stronger in all three of these factors may have particular advantages in challenging situations (e.g., when temptations are stronger or conditions are stressful). 11
CC has been shown to have significant links to specific regulatory techniques common to many kinds of psychotherapy. Mindfulness, with its known benefits on emotion regulation, appears to enhance CC; experienced meditators show lower brain activity during a Stroop task, as the conflict-monitoring process becomes less effortful. 52 Reviews of mindfulness, with a preponderance of nonclinical samples, also indicate improvements in CC—sustained, selective, executive, and switching attention and working memory.53, 54 Evidence suggests that reappraisal (construing an emotion-eliciting situation in a way that alters emotional trajectory) consistently activates CC regions, including dorsolateral, dorsomedial, and ventrolateral PFC and posterior parietal lobe. 55 Reappraisal is linked to working memory and inhibition through the selection, inhibition, and manipulation of appraisals and ability to override dysfunctional automatic attention and interpretation biases; and to flexibility through the replacement of automatic appraisals with alternative adaptive evaluations.15, 17 It has also been found in nonclinical samples that set-shifting abilities are linked to reappraisal and, hence, regulation of affect. 17 In healthy participants, after watching an emotion-arousing film clip, working memory capacity was seen to be linked to better expressive suppression (e.g., instructions to “suppress all expressions of emotion”) and cognitive reappraisal (“think about the film unemotionally and objectively”). 47 Working memory capacity and set-shifting ability (but not verbal ability, reasoning ability, or inhibitory control) have been linked to better cognitive reappraisal. 56 It appears that emotion regulation and CC have two processes in common: (a) a (conflict) monitoring process, comparing the current state with a goal state; and (b) an operating system/effortful regulatory process/response implementation process that works to reduce discrepancies between the current and goal states.57, 58
In clinical samples of older adults, it has been suggested that cognitive restructuring processes integral to CBT recruit CC 59 and also that CBT exercises require allocation of attention, inhibitory control, and self-monitoring. 12 Behavior regulation integral to psychotherapy may also link to CC. For instance, it has been suggested that positive effects of behavioral activation approaches (techniques for increasing “approach behavior” in the presence of strong cues for avoidance and aversive emotion) could be partially mediated by improved goal maintenance, putatively subserved by CC. 3 Conversely, inhibitory control difficulties are linked to procrastination and goal management failures. 60 Improvements in CC are noted following behavioral activation for depression—for instance, the lower magnitude of prefrontal activation required to successfully respond to CC stimuli in sad contexts versus neutral contexts. 61
In general, the evidence supports the role of CC in adaptively regulating cognition, emotion, and behavior—the primary tasks in psychotherapy. However, any form of explicit and controlled strategy (including effortful regulation and reappraisal) is resource-intensive and may be difficult to sustain over the long term. Hence it is economical for regulation to become implicit and/or automatic—i.e., acquiring skills for effortful regulation of cognition, affect, or behavior is important, but there is a further need to facilitate lasting changes in self-schemas and habitual behaviors, for implicit “dispositional” regulation. Such “self” changes may be based on the semantic memory areas and appear to be reflected in neuroimaging findings of the inferior parietal lobe, the temporoparietal junction, and the anterior/middle temporal lobes, found in studies of psychotherapy outcomes. 42 It may therefore be posited that regulation is best understood as a dynamic and cyclical dual process 42 —explicit control may need to be recruited when usual methods of coping become dysfunctional or inflexible; once effortful regulation is achieved, it may need to become internalized and implicit— until such regulation once again appears entrenched or mismatched to situational demands.
Specific techniques have been studied predominantly in nonclinical populations; however, findings remain to be tested in the clinical practice of psychotherapy. Reappraisal/restructuring is the most commonly used and studied technique15, 17, 55, 56; focusing on an individual’s CC abilities as they relate to reappraisal in psychotherapy may be critical to understanding and enhancing clinical outcomes. It may also be hypothesized that CC may be necessary for other psychotherapy tasks of shifting perspective, tolerating distress, and adopting a reflective stance to experience. To illustrate, successful reflection may require an individual to hold a specific instance in working memory, abstract the key features of the experience as a concept, and flexibly examine and apply the concept to other aspects of one’s experience while inhibiting distractors and maladaptive emotions during the entire process. Furthermore, CC may be implicated in psychotherapy processes such as regular attendance; punctuality in starting and ending sessions; managing time, content, and structure in sessions (e.g., avoid running out of time to address important issues due to overelaboration of minor details); homework compliance, and reducing experiential avoidance and automatic/reckless/impulsive behaviors. Inhibitory control may be critical to effective regulation of behavior in psychotherapy. Inhibition encompasses both “stopping” oneself from behaviors that are pleasurable/habitual but inappropriate/unhealthy (e.g., reducing substance use, anger outbursts, risky driving, rumination), as well as “persisting” with behaviors that may be unpleasant/aversive but appropriate/healthy over the long term (e.g., sticking to an exercise plan, working steadily at a job or assignment, engaging in exposure exercises despite significant anxiety). In addition, set-shifting difficulties may potentially interfere with the ability to implement newly learned techniques. CC may therefore be important for generalizing in-session learning to everyday life and problem-solving.
Based on the existing literature, it may be posited that CC abilities may underlie emotional, cognitive, and behavioral regulation in psychotherapy and hence be linked to clinical and functional outcomes of psychotherapy. This may have significant implications as CC functions may be trainable and may potentially be utilized for better behavioral and emotional regulation.
Does Improving CC Lead to Better Psychotherapy Outcomes?
If CC is integral to psychotherapy techniques, processes, and outcomes, then enhancing CC may potentially improve psychotherapy outcomes—highlighting the promising role of cognitive training. 62 Cognitive training methods harness neuroplasticity mechanisms for normalization of impaired neural systems through specifically defined, neuroscience-based, and controlled learning events. The premise of cognitive training is that targeting established neural mechanisms of impairment will produce clinical change and it is promising as an evidence-based intervention in psychiatry. 63 In anorexia nervosa, for instance, a cognitive training program to enhance cognitive flexibility and holistic attention has been useful as a precursor to psychotherapy. 64 Cognitive training may also enhance the recovery of socio-occupational roles beyond clinical remission. 65
CC may be particularly suited as a target of training——studies with combined strategy training have demonstrated transfer of training to other domains.1, 65–67 Better self-regulation of physical activity has been linked to improvement in CC, 10 and modulation of attention appears to improve self-regulation through enhancing the salience of goal-related representations and reducing activation of competing, goal-irrelevant neural representations. 68 These findings are yet to be tested in relation to the regulatory processes required in psychotherapy.
Preliminary data suggest that adding CC training (for working memory and attention) to treatment-as-usual results in greater improvements in depressive symptoms and normalization of activation in dorsolateral PFC and amygdala in depressed individuals. 69 Other studies on training in specific aspects of CC have shown limited improvement of depressed mood—e.g., active suppression for forgetting and inhibition of aversive stimuli. 70 Reviews of cognitive training interventions for depression71, 72 have concluded that CC training may complement treatment-as-usual and produce benefits on working memory, symptom severity, and daily functioning, albeit with small to moderate effect sizes and important considerations relating to duration and intensity of treatments and nature of samples (at-risk/major depression /recurrent depression). The impact of CC training on enhancing psychotherapy outcomes has, however, not received specific attention.
Summary and Implications
The present review examined the relationships between CC and psychotherapy techniques, processes, and outcomes. Neuroimaging studies have been comprehensively reviewed recently23, 26, 43 and provide strong evidence for the role of CC in psychotherapy; however, neuropsychological studies are few. Hence, the current review focused on neuropsychological studies on adults diagnosed with anxiety and depressive disorders undergoing psychotherapy, along with a narrative exploration of other potentially novel findings and hypotheses.
CC appears to improve over the course of psychotherapy. Baseline CC abilities also appear to predict response to psychotherapy. Techniques central to psychotherapy, such as the use of reappraisal, mindfulness, acceptance of emotions, exposure and habituation, homework exercises, diaries, and schedules, implicate CC through effortful regulation processes. Successful psychotherapy is also associated with client variables such as attendance and engagement, motivation for change, self-agency, and collaboration—which implicate the use of CC processes. In this sense, CC may be an “active ingredient” of psychotherapy. Nonclinical studies have contributed significantly to our understanding through a dissection of the processes involved in regulating cognition, emotion, and behavior in controlled experimental studies. However, despite strong evidence implicating CC in psychopathology, treatment outcomes, and processes and techniques central to psychotherapy, CC has received only cursory attention in the adult psychotherapy literature. Bridging this gap between cognitive and clinical sciences, research, and practice may be a crucial step in enhancing outcomes for psychiatric disorders.
Understanding the role of CC in psychotherapy may have important implications through an understanding of individual differences in psychotherapy response, mechanisms of action, and potential for enhancing clinical and functional outcomes in psychotherapy. Further, training designed to improve CC may enhance clinical outcomes beyond treatment-as-usual. Mounting evidence suggests that interventions to improve cognitive regulatory processes before the start of psychotherapy may help to enhance outcomes, and such approaches have been heralded as the most promising direction for future translational research. 3
Future Directions
It has been emphasized that in order to be efficient, economical, and informed by research advancements, psychological interventions may need to be process-specific and transdiagnostic in nature (i.e., target basic dysfunctional processes such as impulsivity, reduced CC, working memory impairments, autobiographical memory specificity, etc.). 73 Such an approach is in line with the RDoC matrix and may assist in identifying common vulnerability factors, integrating disparate theoretical models, facilitating translational research, and formulating broader evidence-based interventions that can be adapted to many disorders.73, 74
Several possibilities may be envisaged for psychological interventions with such an approach (Figure 3).
Cognitive Control and Psychotherapy: Possible Research Questions, Suggested Methods, and Implications.
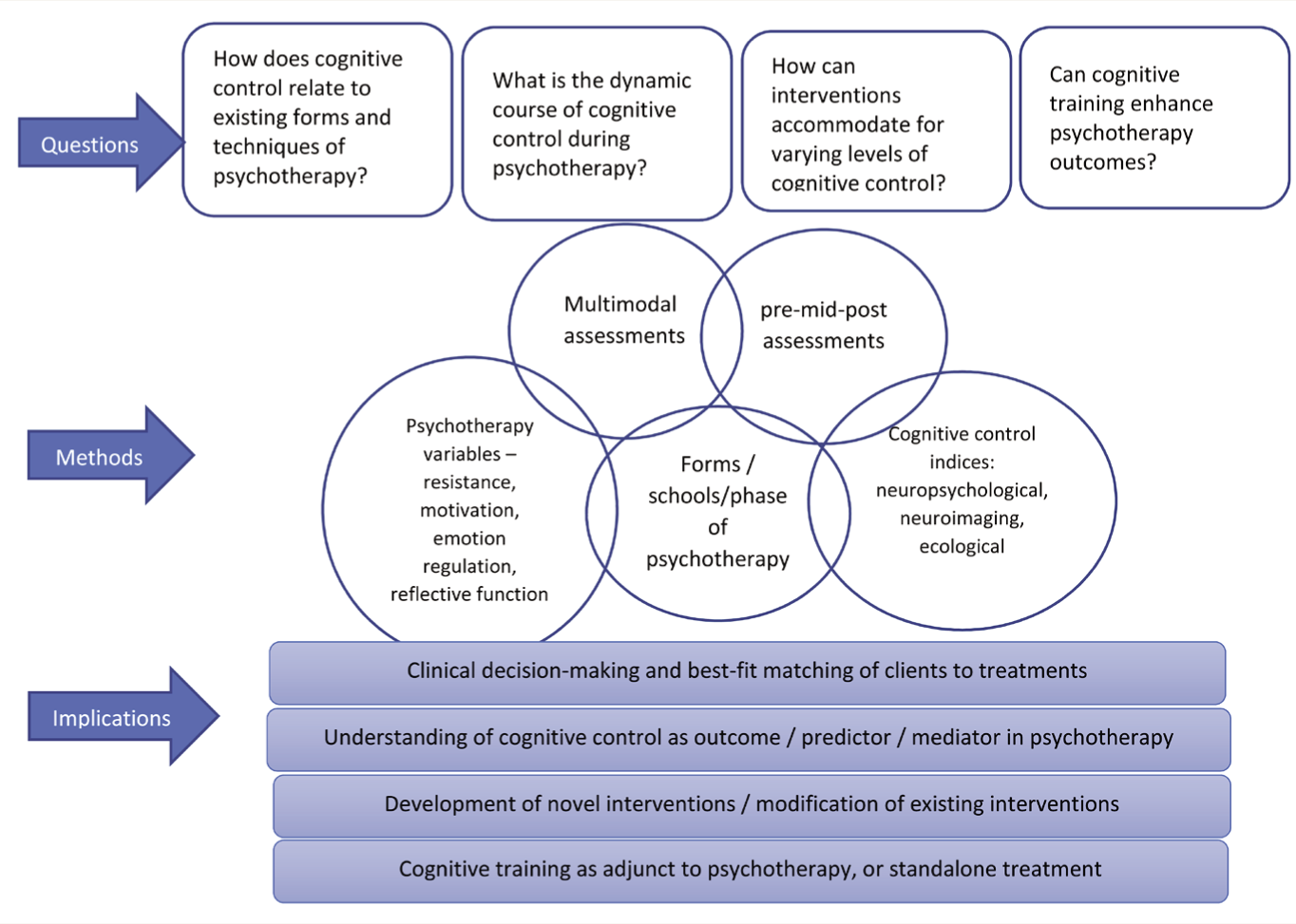
An understanding of CC processes as they relate to existing forms, techniques, and processes of psychotherapy could assist in better clinical decision-making. Research along such lines [e.g., Alexopoulos] 46 may facilitate matching clients to specific treatments based on individual strengths or vulnerabilities. Some possible questions to examine include—What is the role of CC in different kinds of therapies, e.g., cognitive and/or behavioral, acceptance-based, experiential, metacognitive, mentalization-based, or psychoanalytic therapies? Would CC be a necessary component, a sufficient one, or both in various forms of therapies? In particular, does the ability to benefit from self-help resources depend partly on CC processes? It is also important to consider the recruitment of CC in specific aspects of psychotherapy, for instance, in relation to other variables such as motivation, therapeutic alliance, and reflective function, and to the phase of psychotherapy (initial, middle, or late). Such understanding may represent a way forward in the scalability of psychotherapeutic interventions and streamlining interventions based on client variables to improve outcomes.
Developing/modifying techniques or interventions for individuals lower in CC may contribute to better outcomes. Psychotherapy has a long tradition of innovation and adaptability. For instance, CBT, originally intended for depression and anxiety disorders, has been adapted to several other conditions such as psychosis, substance abuse, and eating disorders. Novel interventions address metacognitive deficits in anxiety, depression, and schizophrenia75, 76; as well as mentalization deficits in borderline personality. 77 It is likely that the development/modification of psychological interventions, accounting for low levels of CC, may have some prospects for enhancing outcomes. For instance, enhancing the structure of psychotherapy to buffer inhibitory control difficulties, or scaffolding the working memory requirements of common psychotherapy techniques, may potentially benefit individuals with CC difficulties. This has been explored in relation to children with cognitive dysfunction who may derive limited benefit from verbally oriented psychotherapy. 9 In support of this, research has demonstrated significant improvements in psychotherapy attendance with simple techniques such as using self-statements to manage negative affect at the start of therapy (i.e., cognitive regulation of emotion). 78
Cognitive training interventions may bear the potential to enhance CC as a prelude or adjunct to other psychotherapies. CC training may enhance individuals’ abilities to modulate emotion and implement behavior change. This, in turn, may increase client engagement and, hence, psychotherapy outcomes. Evidence for the state/trait nature of deficits in different disorders may help select a focus for training.
Limitations
Limitations of the Review
For the purpose of systematic review, only studies with pre-post neuropsychological data on anxiety and depression were selected. Findings from other age groups (pediatric/geriatric) and analog samples have been examined in a narrative review and, therefore, not subjected to the same stringent standards as a systematic review. However, given the limited research in this area, this was deemed useful as pointers for future research directions. The psychotherapy literature on other disorders is worth examining in the future. The study has also not used meta-analytic methods, which may be considered in future studies.
Limitations of the Reviewed Studies
Current research is characterized by inconsistent terms and definitions, contributing to the knowledge gap. For instance, some research suggests that CC may not always be adaptive for emotion regulation. 42 The evidence in this regard comes from findings that the neural bases for reappraisal are not very different from inhibition, avoidance, or suppression (although it is acknowledged that reappraisal may indicate an earlier modulation of emotion than suppression and may additionally rely on semantic brain structures to access alternative representations/explanations for an experience). Reappraisal is often confused with suppression by clients in the early phases of therapy, and lab-based studies demonstrate that instructed reappraisal is not very successful. 79 Further, several gaps remain to be bridged. Research has been restricted to certain schools and techniques. Studies on nonclinical populations predominate; although these have value in dissecting specific components of a technique, research on clinical diagnoses is necessary. Neuroimaging studies have contributed to an understanding of psychopathology but must be extended to the clinical practice of psychotherapy and the underlying regulatory mechanisms—both maladaptive and adaptive.
Conclusions
Existing studies in the field have advanced our understanding of the mechanisms of psychotherapy by giant strides. CC, an RDoC construct, may be an “active ingredient” of psychotherapy through its role in change processes and outcomes of psychotherapy, and merits further empirical investigation.
It cannot be denied that, in psychotherapy, lasting change in self-structures must be triggered by a series of smaller domino effects, including regularity and punctuality in attendance; acquiring new skills and perspectives and remembering to use them; self-agency, planning, and implementation of change; and persistence in effortful control of thought, affect and behavior—which may be rooted in CC.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors thank Dr Hannah R Snyder for insightful comments on the draft manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.