
Abstract
Background:
Mental health issues are common among college students, and structured services have been proven to enhance outcomes. Despite increased enrolment for higher education in India, college mental health services remain sparse. JEEVANI is the first structured state-wide college mental health service in India. This paper describes its framework and provides an overview of its functioning during the initial five months.
Methods:
In 2019–2020, the Directorate of Collegiate Education, Government of Kerala, implemented the program in 66 colleges catering to approximately 60,000 students. Qualified counsellors were trained to identify issues and provide interventions and early referrals, using a stepped-care approach. They conducted awareness programs to promote mental health and reduce stigma.
Results:
The services were accessed by 2,315 students during the assessment period (October 2019 to February 2020). The beneficiaries were predominantly females (54.1%). Over a third (38.8%) belonged to the lower socio-economic strata, and 2.5% had significant vulnerabilities. Although no syndromal diagnoses were made, anxiety and depression were the most common presentations. The counsellors provided 3,758 individual sessions and facilitated support for students who reported academic difficulties or interpersonal issues. Severe mental illness was detected in 54 students, and referrals for specialist mental health input were initiated in 68.
Conclusion:
Describing the framework, sharing the technical material, and providing an overview of its functioning from a resource-constrained setting in India may encourage higher education institutions in low- and middle-income countries to consider similar projects.
JEEVANI is the first structured state-wide college mental health service in India. Trained counsellors identified mental health issues and provided interventions. Program effectiveness is reflected in the service utilization in the initial few months.Key messages:
Mental health issues are common among college students. The World Mental Health Survey, involving 21 countries, found that 20.3% of college students fulfilled the criteria for a psychiatric disorder in the preceding year. 1 Findings from various Indian states also reflect a similar trend.2, 3 Late adolescence, which translates to the college-going period, is neurodevelopmentally the period of highest risk for development of severe mental illness (SMI), with 75% reporting symptom onset by 25 years of age. 4 Mental illness also correlates with suicidality, and international surveys show that 16%, 3%, and 1.2% of college students report suicidal ideations, plans, and attempts, respectively. 5 India in 2018 witnessed approximately 10,000 completed student suicides. 6
Among college students, mental health issues are increasing both in number and severity.7–9 Mental health issues have profound negative impacts; there are consistent reports of poor academic achievement and college dropouts in the short term, and lower employment, social isolation, and poor overall health over the long term.1, 10 Young people with mental health issues often make poor lifestyle choices. Physical underactivity, unhealthy diet, substance use, and high-risk sexual behaviors increase the risk of noncommunicable diseases.11, 12
Despite these, this period also presents a window of opportunity for mental health interventions.1, 10 Structured college mental health programs have shown clear benefits for both students and the larger society. 13 A range of interventions has been reported to reduce mental health difficulties among college students effectively. 13 Therapies, especially brief therapies with a cognitive behavioural template, have been effective in reducing mild–moderate depressive and anxiety symptoms. 14 Additional academic supports, especially for students with difficulties, significantly improve mental health. 15 Gatekeeper training has an impact on suicidal behavior in the short term; however, professional assessment of suicidal students has a lasting impact. 13 Among the universal mental health prevention programs, relaxation-based interventions have been amongst the most effective. 16 Recreational interventions like exercise, art, and plays were also helpful in reducing both anxiety and depression. 14 Inconsistent evidence suggests that psychoeducational approaches reduce stress, anxiety, and general distress. 17
In India, the last decade has witnessed increased student enrolment in higher educational institutions, after the Government prioritized access to college education. 18 Provision of a structured mental health program for colleges in India and low- and middle-income (LAMI) countries is a significant challenge due to the scarcity of mental health resources.19, 20 In India, such programs have largely been restricted to elite institutions such as the Indian Institutes of Technology, Indian Institute of Management, etc.21, 22 Hence, the Department of Collegiate Education of the Government of Kerala launched “JEEVANI,” a structured, state-wide, comprehensive college mental health program for students in all government arts and science colleges of the state. The project aimed to improve awareness, promote mental health, and ensure early identification and intervention for mental health issues among college students. This paper describes the framework of this program and provides an overview of its functioning during the initial five months. In addition, the supplementary material includes the training manual for college counsellors, which is being made available as a free technical resource.
Methods
The study is an observational study, exploratory in nature. Kerala is the 13th largest state in India. It has a commendable educational system and was the first state in India to achieve 100% literacy rates. 23 There are three streams of higher education in Kerala, each under a directorate: collegiate education for arts and science streams, technical education for engineering and other technical courses, and health education, pertaining to medical, nursing, and paramedical courses.
Planning and Approval for the Project
The project was initially proposed to the Department of Higher Education, Government of Kerala, after published data indicated a high prevalence of mental health issues, with negative correlates, among college students.1, 2 It was decided to implement the project in phases, first in the arts and sciences colleges under the Directorate of Collegiate Education and then extend the program to the Directorate of Technical Education after evaluation of feasibility and effectiveness. An expert meeting was called with the administrative officials of higher education and collegiate education and mental health experts from both Kerala and National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, the premier institute for mental health in India, in attendance. The group reviewed the mental health data and existing framework of both higher education and mental health services in the state, before deliberating on interventions. The recommendations of the expert meeting formed the framework of JEEVANI (meaning, “account of one’s life”). It was approved by the government, with an initial funding of ₹1.67 crores for the academic year 2019–2020, which included salaries of counsellors, training, infrastructure development, and administrative costs.
General Functioning
Each college had one JEEVANI unit, staffed by a full-time counsellor. The counselling center provided services to all enrolled students during working hours. In the unlikely event of services being required outside of the working hours, information on the nearest round-the-clock mental health service was provided.
Duties and Responsibilities of the Counsellor
Counsellors recruited under JEEVANI were required to have a postgraduate degree in psychology with clinical experience in counselling. Individual colleges were requested to advertise and recruit locally. Of the 66 counsellors recruited, 62 were female, most between 25 and 30 years of age, with at least one year of clinical experience. The posts were contractual for the academic year. The counsellors provided services to students enrolled in institutions under their care. These included the following.
1. Case identification and assessment
Students could “self-refer”/“walk-in” to the JEEVANI unit. Teachers, friends, or family could also initiate referrals for specific mental health concerns regarding a particular student. In third-party referrals, the counsellor was expected to elicit pertinent information and, if the concerns were tangible, reach out to the student directly or through class tutors, friends, or family, without compromising confidentiality.
Students seeking help underwent brief clinical assessment which included their clinical presentation and its history, any risk of harm to self/others, academic performance (current and historical), family circumstances (including socioeconomic status of family—above or below poverty line based on their family ration card), any additional vulnerability (disability, living in special home, sexual minorities, etc.), social supports (including friends in college) and mental status examination. Interventions were provided based on inferences made in clinical assessment.
2. Interventions
Students with significant mental health issues were provided psychoeducation and offered other evidence-based inputs, as appropriate. Students with transient situational crises, anxiety syndromes, stress-related symptoms, or mild-to-moderate depression received brief therapies (2–6 sessions) using a supportive/problem-solving/cognitive behavior therapy framework, which has been proven to reduce mental health distress.13, 14 Brief therapy using the FRAMES model was provided to those with substance use and related issues. 24 Many other intervention strategies such as mindfulness, acceptance and commitment programs, and group interventions have been shown to benefit. 13 However, it was decided at initiation, the program will focus on implementing a limited number of interventions with good evidence and on which counsellors can be effectively and easily trained.
Counsellors also facilitated assistance from the college administration/faculty when the mental health issues were precipitated or perpetuated by persistent difficulties in academics or other campus-related issues such as bullying and ragging.
Students with mental health crisis (meaning presenting with extreme emotional/behavioural disturbance or any behavior that puts the person at immediate risk of harming self or others) were provided brief crisis interventions. Family were involved wherever possible, especially if the student required clinical monitoring or was at a higher risk. Specialist referral was also initiated, if required.
The counsellors were trained to ensure that students with symptoms of Severe Mental Illness (SMI) (category in the context of this program include schizophrenia [and other psychotic disorders], bipolar affective disorder, and severe depression) presenting for the first time or who were off treatment received referral to specialist mental health services. Additionally, if symptoms of any detected mental health disorder persisted/worsened or there was a risk of harm, a referral was initiated for off-campus specialist mental health input. Consent was also taken and information was shared with the parent/guardian for all referrals.
If the student was not receptive to interventions, those with minimal symptoms were informed about “crisis signs,” “steps to keep safe,” and the need to access care if symptoms persisted/worsened. If students with significant symptoms, with risk to self/others, refused interventions and/or did not consent for a guardian to be informed, the Head of Institution/faculty in charge of the JEEVANI unit could initiate steps to contact the guardian (except in the instances where there were concerns regarding the caregiver) or ensure referral to the nearest health-care facility pending appropriate specialist mental health assessment. Referrals were also initiated if the issue required specialized long-term input that was beyond the expertise of the counsellor or the scope of the program. Counsellors also facilitated help from elsewhere if the student opted so owing to concerns of confidentiality/stigma.
3. Improving mental health awareness through promotional programs
Improving awareness about general mental health and wellbeing among young people was an important objective of the program. The awareness classes focused on promotive approaches to mental health, that is, healthy lifestyle, relaxation, healthy use of technology, study skills, and substance use prevention. Counsellors were mandated to conduct at least one program every month and used a variety of methods. Programs conducted include commemorating mental health events and conducting invited guest lectures, workshops, plays, etc. These psychoeducational approaches have been shown to improve help-seeking. 17
4. Liaison with other on-going college-based programs
Colleges in Kerala have multiple schemes/programs focused on improving student functioning and wellbeing. These include support for academically weak students under the Students’ Empowerment for Educational Development (SEED) program, fostering social interactions and responsibility (National Service Scheme), reducing bullying (Anti-ragging Cell), addressing gender issues (Women’s Cell), provision of additional academic support to students (Scholar Support Program), career guidance (Career Guidance Cell), and prevention of drug abuse (Anti-narcotic Cell). Often, these were issues underlying the mental health concerns in many students, and addressing them has been shown to be effective. 13
Training and Supervision
All counsellor-recruits received a 4-day in-house manualized training to familiarize them with the broad objectives of the program. In addition, they were oriented regarding common mental health issues, interventions to be provided, and the framework of the program.
Monthly supervision was provided to counsellors by the faculty of the Department of Psychology of the Government College for Women, Thiruvananthapuram, and the Nodal Centre, and senior mental health specialists of the Government Health Services. These supervisory meetings reviewed the counsellors’ monthly functioning, a summary of clinical duties, and targets achieved. The counsellors were themselves provided the necessary support to maintain motivation and reduce burnout.
Administrative Framework
JEEVANI had two administrative levels—at the institution level and the state level.
At the institution level, the Head of the Institution (Principal) was the administrative lead. A teacher was designated “faculty coordinator of JEEVANI” who supervised the day-to-day administrative work. A committee consisting of the college principal, faculty coordinator, college counsellor, and a parent representative ensured smooth functioning through monthly meetings that reviewed program functioning, planned activities, and addressed administrative aspects if any.
The Nodal Committee at the state level provided policy directions pertaining to the structure, finance, and implementation of the program. The Director of Collegiate Education chaired the state nodal committee. Other members were the faculty of the Department of Psychology of the Government College for Women (Thiruvananthapuram) and mental health professionals from the State Health Services and NIMHANS. The committee met every month to review the functioning of the program. The Principal Secretary for Higher Education, who was the state head of the higher education department, formed the Chief Advisor/Patron of the project.
Ethics
The program was approved by the Institute Ethical Committee of Government Medical College, Thiruvananthapuram.
Documentation
A structured case-taking pro forma was provided to all counsellors to ensure standardized assessment. Each student was assigned a unique identification number, and their clinical records were to be retained by the counsellor until the end of the academic year. After that, the records were to be transferred to the custody of the Head of the Institution for safekeeping for the subsequent four years (the entire duration of the academic course and an additional year).
The counsellors were required to provide an anonymized monthly collated report of work in their colleges.
Statistical Analysis
The monthly report provided by the counsellors for the five months between October 2019 and February 2020 were collated and analyzed using SPSS version 26. 25 Descriptive statistics have been used to describe the institutional characteristics, prevalence, and patterns of utilization of services in JEEVANI. Independent sample t-test and analysis of variance have been used to examine whether service utilization was determined by the number of students enrolled and area where the college has been situated (rural/urban).
Results
JEEVANI was launched in October 2019. Although the usual collegiate academic year in Kerala runs between June and March, in 2020, it ended abruptly in the beginning of March due to the COVID-19 pandemic. Hence, the results describe the overview of the first five months between October 2019 and February 2020.
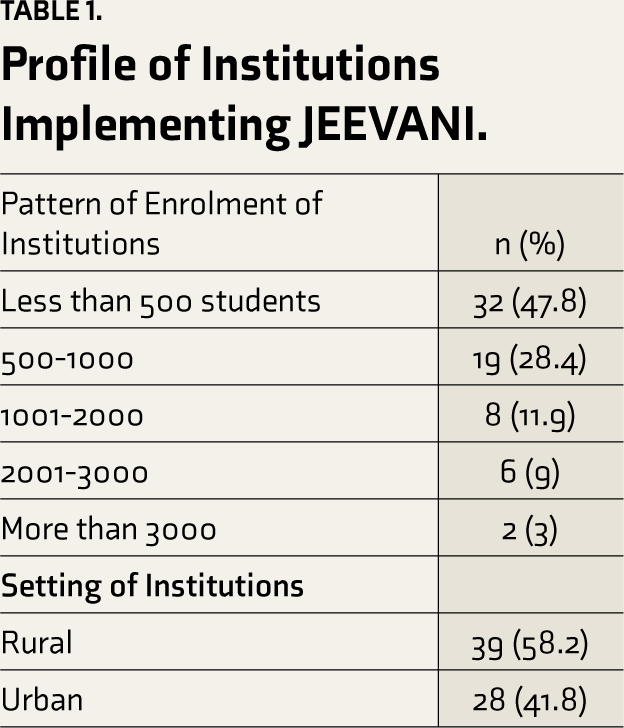
There were approximately 60,000 students across the 66 colleges under the Department of Collegiate Education were JEEVANI was implemented. The majority of these institutions are located in rural areas [38 (58.2%)], with most having less than 1,000 students (76.2%) (Table 1).
Profile of Institutions Implementing JEEVANI.
The counsellors provided 3,788 consultations for 2,315 students during the above-mentioned period. The beneficiaries were predominantly females (54.1%). Over a third (38.8%) belonged to the lower socioeconomic strata and 2.5% had significant vulnerability (disability/inmates of special homes/orphans/sexual minorities) (Table 2).
Profile of Students Seeking Consultation under JEEVANI.
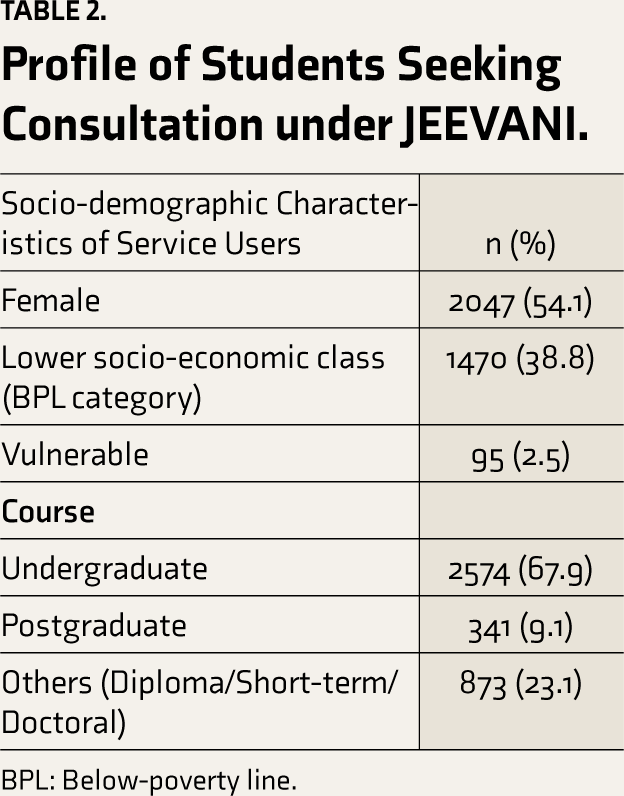
BPL: Below-poverty line.
Most students reported identifiable stressors, among which academic difficulties and interpersonal issues were the commonest. Although no syndromal diagnoses were made by the counsellors, the predominant presentations they recorded were anxiety and depression. Most students who were categorized under “others” also had a mixture of depression and anxiety symptoms. Consultations for excessive use of the internet and technology were more common than for substance use. Fifty-four students were detected to have SMI (Table 3).
Among the interventions provided, individual counselling sessions were the commonest (n = 3,758 sessions). College-level interventions mostly involved facilitating support for students with academic, financial, or interpersonal difficulties. Family involvement was required in 117 students and 68 were referred for specialist mental health inputs (Table 3). Although counsellors provided guidance for accessing specialist mental health input, parents or other caregivers were primarily involved in facilitating the same. Referral without parental/family consent were not reported during the assessment period. JEEVANI counsellors in a few institutions provided tele-support in a limited fashion.
Students in colleges in rural areas received significantly higher mean number of interventions compared to institutions in urban areas (9.36 vs 7.65, P = 0.034). However, the number of students enrolled in the institution did not determine service utilization (P = 0.16).
Discussion
The paper describes the framework of implementation and service utilization of a structured college mental health service program (JEEVANI) in the state of Kerala, India. This represents a pioneer attempt in India, as previously there were few or no avenues for campus-based mental health-care, except in a few elite institutions. The system of higher education in India is currently the third largest in the world, after USA and China. 26 Existing research on college mental health services involves high-income countries. Such findings have limited generalizability owing to differences in culture, educational policies, and political dynamics in Low and middle income countries.
Clinical Characteristics of Students who Accessed the Services and the Pattern of Interventions Provided under JEEVANI.
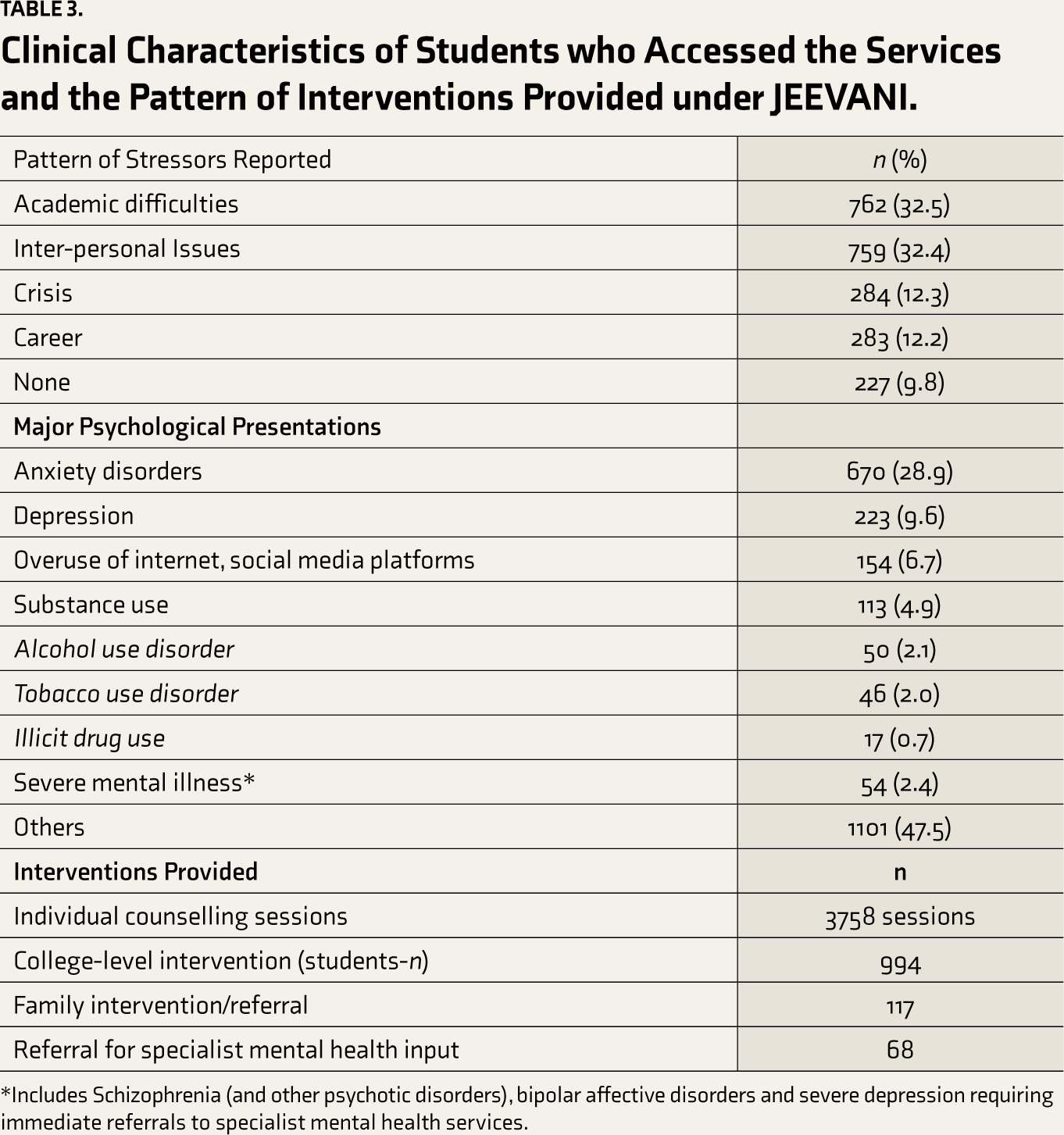
*Includes Schizophrenia (and other psychotic disorders), bipolar affective disorders and severe depression requiring immediate referrals to specialist mental health services.
JEEVANI is by far the largest structured college mental health service in India. Evidence-based measures were adopted for its implementation. These included standard protocols for the training of personnel, clinically supervised and appropriate interventions and referrals, and an administrative framework that constantly evolved based on monthly feedback and reports. This project was hence able to achieve, to a huge extent, the broader objective of delivery of minimum standards of mental health-care to college students.
A higher proportion of those who accessed services were females and those from the lower socioeconomic strata. This may, however, represent a reflection of the demographics of government colleges in Kerala. It is estimated that in Kerala, 78.64 % of students enrolled for graduation are girls, and at the postgraduation level, it is 67.01%. 18 Students with financial difficulties prefer enrolling in government institutions owing to the nominal fees and numerous scholarships. For students with economic difficulties and significant vulnerabilities (orphans/inmates of special homes), the free services through JEEVANI were possibly the only accessible mental health support. The utilization of services were also higher among students in institutions in rural areas. The reasons for this were not systematically explored. However, it could be possible that students in institutions in rural areas had relatively less access to alternate avenues for mental health-care.
The most common presentations among the students were anxiety and depression, reiterating previous reports.1, 27 Consultations for unhealthy use of the internet and technology were more frequent than for substance use, reflecting the rising tide of behavioural addictions across the world. 28 The JEEVANI counsellors were also competent to detect SMI and did so in a small group of students. This was important as SMI among college students, if unaddressed, could have a range of negative outcomes, including dropping out, substance use, and suicide.29, 30 However, there was no mechanism to evaluate effectiveness of this screening for SMI and it is possible that cases may have been missed.
The program adopted a stepped-care approach to ensure rational use of available human resources in our resource-constrained settings. Academic difficulties and interpersonal issues were the most commonly reported stressors, and the counsellors provided over 3,000 sessions of brief psychological interventions across the state. Resource-intensive interventions and referrals were initiated for those with complex mental health needs.
In the initial months, the counsellors were required to conduct monthly mental health awareness classes and be involved in the pre-existing college-based programs for students’ welfare, in order to improve acceptability and reduce stigma. Counsellors had the flexibility to promote awareness through lectures, movies, video presentations, college festivals, posters, drama, observance of World Suicide Prevention Day, World Mental Health Day, etc.
Availability of college mental health services in India is currently mostly in elite stand-alone institutions such as Indian Institute of Technology (IITs), Indian Institute of Management (IIMs), or large private institutions with counsellors/mental health professionals providing in-campus input. 31 Most of these large institutions have general health clinics with counselling services being provided within the clinics. A few have part-time psychiatrists but in almost all students with complicated mental health issues are referred externally for the specialist mental care. In contrast, in high-income countries especially the United States of America where college mental health services are more widely available, there are four structural models of mental health-care. First, in which mental health-care is integrated to university health clinic both clinically and administratively; second, being separate clinically and administratively (most common); third, providing separate services but having administrative integration, lastly being clinically integrated however with different administration. 32 It is not possible to compare both systems as they vary vastly in health-care, mental health-care, system of higher education, and culture. The reasons for seeking mental health support also vary. Consultations for substance use and polysubstance use are common in European and American universities where substance use prevalence is reported 50% to 70%. 33 In contrast, more students sought consultations in our program for behavioural addictions than substance use, reflecting the relatively lower prevalence rates of substance use in our campuses. 34
Challenges
The program faced few inception challenges. The specialist mental health personnel in the health sector, identified for the monthly group supervisory sessions of counsellors, were already burdened with numerous other programs and were unable to co-ordinate these sessions. However, as the program progressed, individual clinical supervision and referrals to the local mental health service stabilized. There were space constraints in many institutions, especially in newly established colleges that were often housed in rental buildings or shared spaces with other government institutions. In nearly a third of the institutions, providing a separate room for counselling was difficult. The necessary supportive infrastructure could be provided only towards the end of the assessment year, resulting in considerable delay in smooth functioning.
Limitations of the Study
Ideally, reporting program effectiveness requires both qualitative and quantitative assessments. The program, when envisaged, required quantitative assessment to be conducted monthly, with information being collated from counsellors’ reports. The qualitative assessment of the end-users was planned for mid-February 2020 (4–5 months after program initiation). However, the outbreak of the COVID-19 pandemic in Kerala in February/March, requirements of social distancing, and abrupt closure of all academic institutions meant this could not be done. Although this aspect was unexpected and beyond our control, this is a limitation of our reporting of program effectiveness.
Future Plans
The COVID-19 pandemic and its aftermath have seen the widespread application of technology-based platforms. 35 This has been widely used for interventions in many developed countries; however, most were deemed not culturally appropriate. Hence, developing indigenous platforms for the program after a sufficient understanding of the needs of our students is a necessary step for the immediate future. The increasing use of technology platforms also means incorporating cyber safety programs for awareness and intervention. Incorporating continuous qualitative feedback from end-users by feedback forms/suggestion boxes/anonymous surveys will also be an immediate priority. More robust indicators of program effectiveness such as substance use relapse rates, decrease in suicidality, improved functionality, and proportions of follow-up will be incorporated to examine the effectiveness of this program in the medium–long term.
To conclude, mental health issues are common among college students, and structured college mental health services ensure early detection and intervention, thus improving outcomes. Despite increased enrolment, college services providing mental health support are unavailable in most LAMI countries, including India. JEEVANI is the first structured state-wide college mental health service in India. We hope that free access to its framework and technical material will help develop similar projects in other resource-constrained settings.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The project was funded by the Department of Collegiate Education, Government of Kerala.