
Abstract
Objectives:
This review aimed to evaluate all the published studies from India conducted in the consultation-liaison (CL) psychiatry setting to identify the diagnostic patterns and referral rates in this setting. Understanding the same can help in organizing the services and knowing the training needs.
Materials and Methods:
A thorough literature search was done in August 2020 using different search engines (PubMed, Medknow, and Google Scholar). This was followed by an individual search of various Indian Psychiatry journals and a hand search of references in the available articles. Only those studies that described patients referred to psychiatry services from various specialties were included.
Results:
A total of 33 studies were selected for the review. More than half of them were published in the last 5 years. Studies have primarily reported psychiatric profile medically ill inpatients referred to CL psychiatry services, with the majority of the studies reporting the number of patients seen for the duration of at least 1 year. The referral rates for inpatients across different institutes have varied from 0.01% to 3.6%. The referral rates from emergency set-ups have varied from 1.42% to 5.4%, and in outpatients, from 0.06% to 7.17%. The most commonly diagnosed psychiatric disorders across different studies include depression; organic disorders, including delirium; substance use; intentional self-harm; and anxiety disorders.
Conclusions:
A limited number of studies have reported the profile of patients seen in CL psychiatry setups. Available data from these studies suggest that referral rates to psychiatry services from other specialists are dismal. There is an urgent need to change the focus of psychiatry training at both undergraduate and the postgraduate levels to enhance the psychiatric knowledge of physicians to improve psychiatry referrals.
The referral rates to psychiatry liaison services for all the inpatients across different institutes have varied from 0.01% to 3.6%. The referral rates to consultation liaison psychiatry services in the emergency set-ups have varied from 1.42% to 5.4%, The most common diagnosed psychiatric disorders across different studies include depression, organic disorders, including delirium, substance use, intentional self-harm, and anxiety disorders.Key Messages:
In India, a major part of health care is provided through the private sector. 2 Over the years, the care model in the private sector has shifted to corporate and multispecialty hospitals. With the expansion of psychiatry in the private sector, a large proportion of psychiatrists are part of multispecialty hospitals and cater to the mental health needs of persons with various physical illnesses. 1 Addressing these needs requires a thorough knowledge of the principles of CLP.
Unfortunately, due to lack of human resources across different institutes, either in the form of the number of faculty members or the total number of trainees, CLP has not received its due importance in the postgraduate training. When one looks at the existing literature, little is understood about the service models of CLP practiced in India. 3 The available studies, which have described the referral patterns of patients seen CLP practice, are, in general, silent about the functional aspects of the services. 1 From the published data from various centers, it is evident that CLP services across the centers follow the consultation model, that is, patients are evaluated by the psychiatrists on the request of the physician/surgeon and the needful care is provided. This consultation model is followed in both inpatient and outpatient settings. 1
Although data from different institutes are available about the profile of patients with various physical illnesses seen in CLP practice, little is understood about the data from one institute compared with the other. In this background, this review aimed to evaluate the published literature for the pattern of psychiatry referrals in terms of various psychiatric diagnoses and referral rates.
Materials and Methods
For this review, published literature was searched in the month of August 2020 by using the search engines of PubMed, Medknow, and Google Scholar using terms like consultation, liaison, consultation-liaison, psychiatry referrals, emergency, and India in various permutations and combinations. Additionally, tables of content of online issues of various psychiatric journals published from India (Indian Journal of Psychiatry, Indian Journal of Social Psychiatry, Industrial Psychiatric Journal, Journal of Geriatric Mental Health, Journal of Indian Association of Child and Adolescent Mental Health, Indian Journal of Private Psychiatry, Indian Journal of Psychological Medicine, Annals of Indian Psychiatry, Journal of Mental Health and Human Behaviour, Eastern Journal of Psychiatry, Indian Journal of Behavioural Sciences, Andhra Pradesh Journal of Psychological Medicine, Kerala Journal of Psychiatry (2013 onwards), Telangana Journal of Psychiatry, Orissa Journal of Psychiatry, Bengal Journal of Psychiatry, Delhi Psychiatric Bulletin, Indian Journal of Social Work, International Journal of Psychiatry and Psychology, Journal of Psychiatric Nursing, Journal of Psychosocial Rehabilitation and Mental Health, and Indian Journal of Clinical Psychology) were specifically searched for studies evaluating psychiatry referrals. Only studies that described patients referred to psychiatry services from various specialties were included. Studies that described psychiatric morbidity in patients with various physical illnesses, but were not based on psychiatry referral pattern, were excluded. Similarly, studies describing psychiatry morbidity in patients from one specific specialty or those describing specific psychiatric disorder, but not based on psychiatry referrals, were excluded. Studies describing only patients of self-harm, seen in the CLP set-up, were also excluded. Case reports, review articles, viewpoints, etc., describing specific mental health issues in patients with various physical illnesses or in relation to CLP (such as self-harm, delirium, etc.), were excluded. Data published only as part of the abstracts of a national conference were also excluded. However, studies that reported screening of all the patients admitted to a medical/surgical ward and reported the diagnostic profile were included. The search was carried out in mid-August 2020 and encompassed the studies from 1968 to August 2020.
An initial internet search yielded 346 articles. Screening of specific journals provided an additional 20 articles. Furthermore, the reference lists of all the articles were reviewed to look for missing studies. Abstracts of these articles were initially reviewed, and the full-text articles of those relevant to CLP were collected. Finally, 33 studies were selected for this review.
Studies reporting the patient profile seen in CLP referrals were reviewed, and the following data were extracted: year of publication, study site/center, duration of data for which data was reported, number of patients, setting at which the referrals were seen, the gender distribution of patients, age categories of patients, psychiatry referral rates, and the most common diagnostic categories. Additionally, if the studies reported additional diagnosis-specific data, that was also extracted.
Results
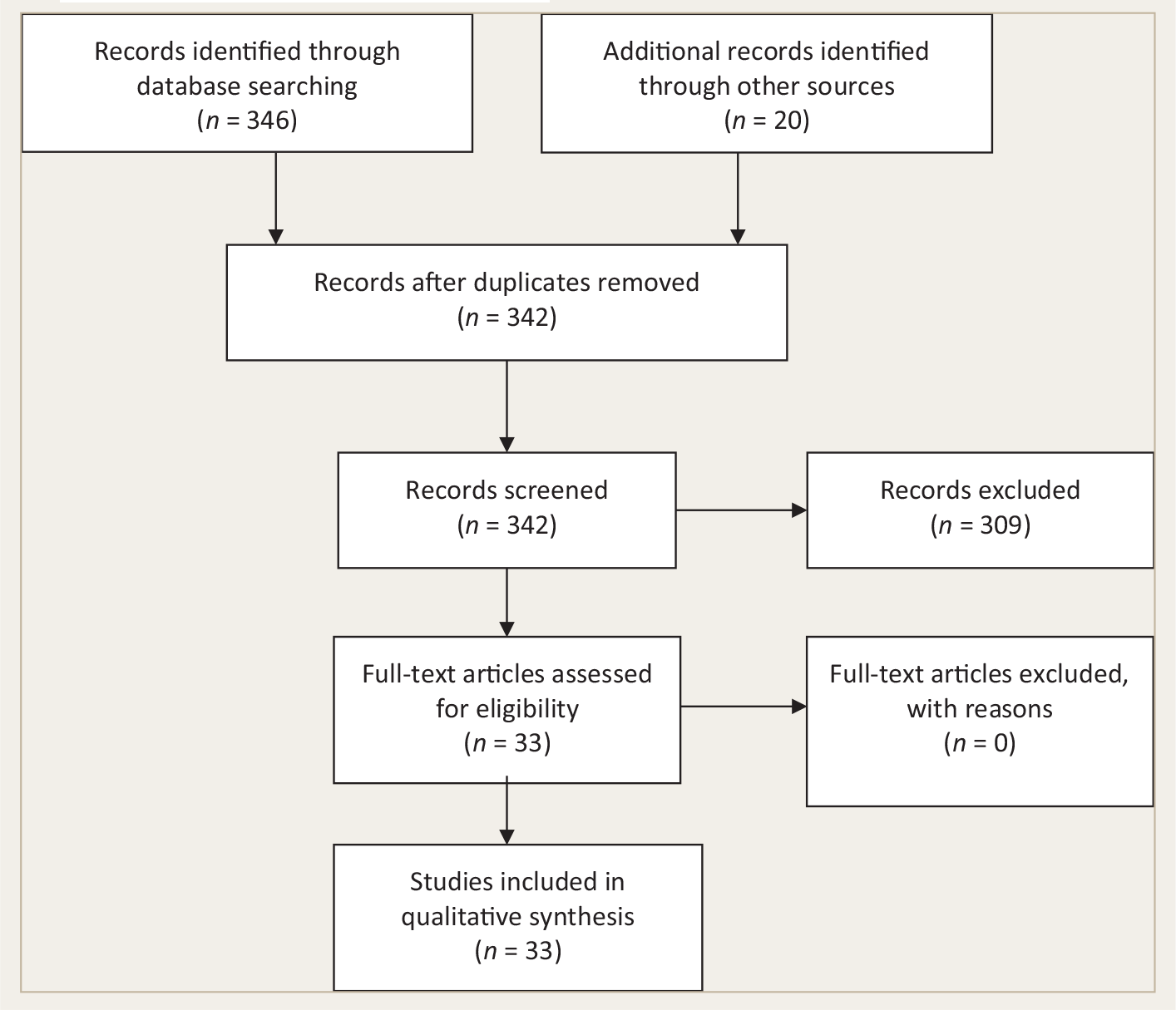
The initial search yielded 346 papers/abstracts. We screened all of them for relevance by going through the full papers. When the full papers were not available, we relied on the abstracts (n = 5). Additionally, we also checked the cross references of the papers, which yielded an additional 20 papers. After checking for duplicity, we were left with 342 papers, of which 309 were excluded as they were review articles, focused on specific issues such as delirium or self-harm, or pertained to psychiatric morbidity in a specific specialty or specific physical diseases. Finally, we were left with 33 studies, which were included in the review (
PRISMA Diagram Showing Selection of the Studies for the Review
Summary of the Studies Evaluating the Profile of Patients Seen by Psychiatry Liaison Services
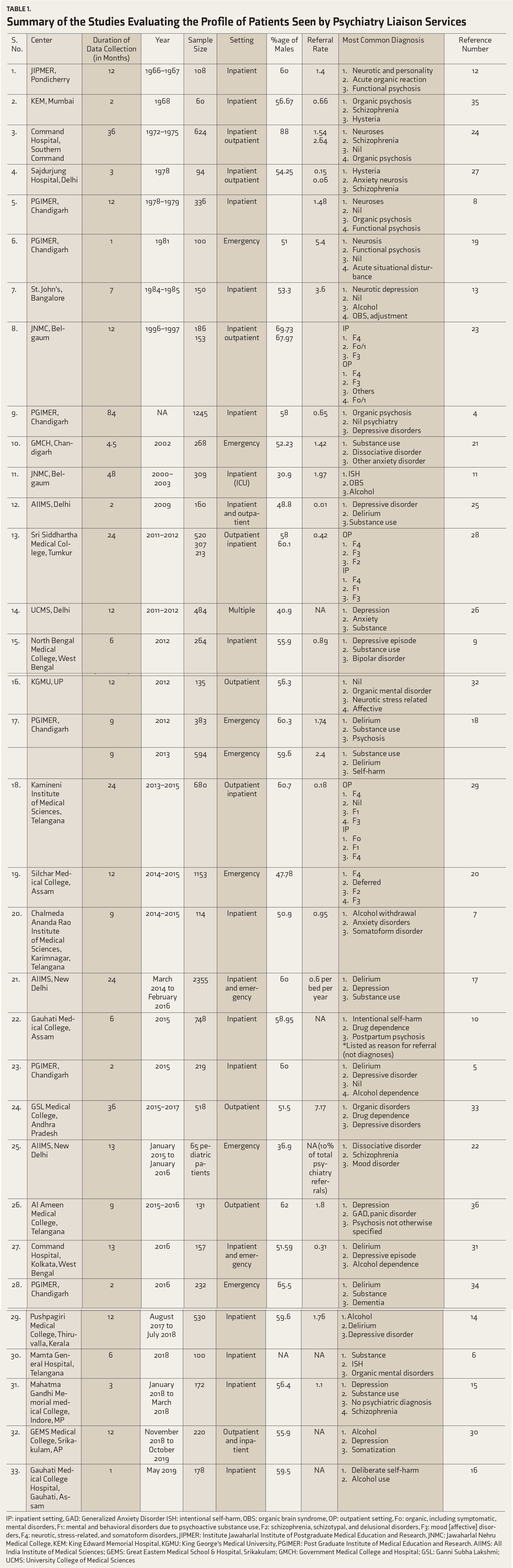
IP: inpatient setting, GAD: Generalized Anxiety Disorder ISH: intentional self-harm, OBS: organic brain syndrome, OP: outpatient setting, F0: organic, including symptomatic, mental disorders, F1: mental and behavioral disorders due to psychoactive substance use, F2: schizophrenia, schizotypal, and delusional disorders, F3: mood [affective] disorders, F4: neurotic, stress-related, and somatoform disorders, JIPMER: Institute Jawaharlal Institute of Postgraduate Medical Education and Research, JNMC: Jawaharlal Nehru Medical College, KEM: King Edward Memorial Hospital, KGMU: King George’s Medical University, PGIMER: Post Graduate Institute of Medical Education and Research. AIIMS: All India Institute of Medical Sciences; GEMS: Great Eastern Medical School & Hospital, Srikakulam; GMCH: Government Medical College and Hospital; GSL: Ganni Subha Lakshmi; UCMS: University College of Medical Sciences
In terms of diagnostic profile, there is significant heterogeneity in reporting patterns across studies, with some reporting the specific diagnosis and some reporting only the broad diagnostic categories. Furthermore, some older studies reported the diagnosis as per the International Classification of Diseases (ICD), 9th revision (ICD-9),4, 8, 19, 27 whereas recent studies used the ICD-10 criteria.5–7, 9, 11, 14, 15, 17, 18, 20–23, 25, 26, 28–33 Occasional study reported the diagnosis as per the Diagnostic and Statistical Manual (DSM) criteria.
36
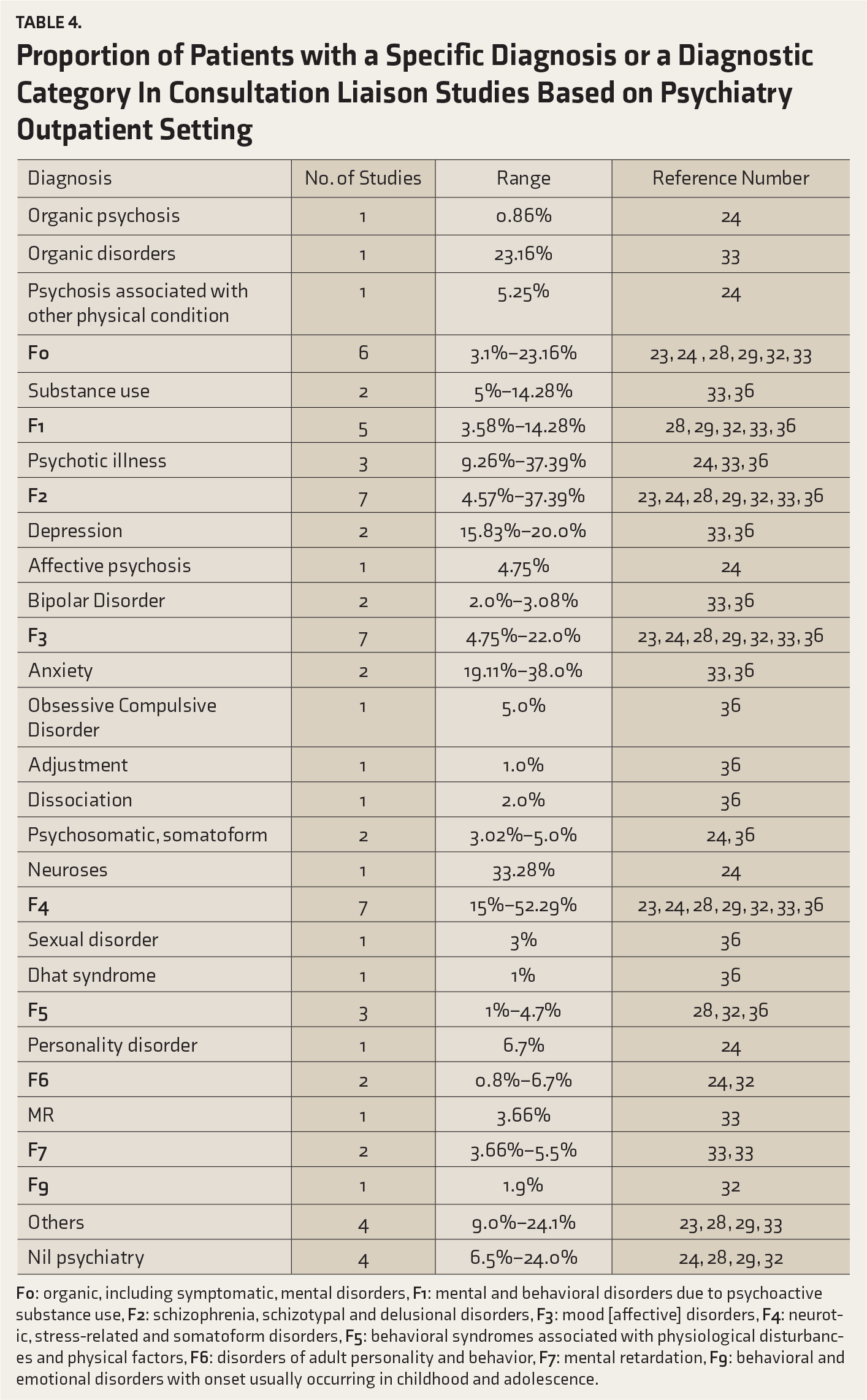
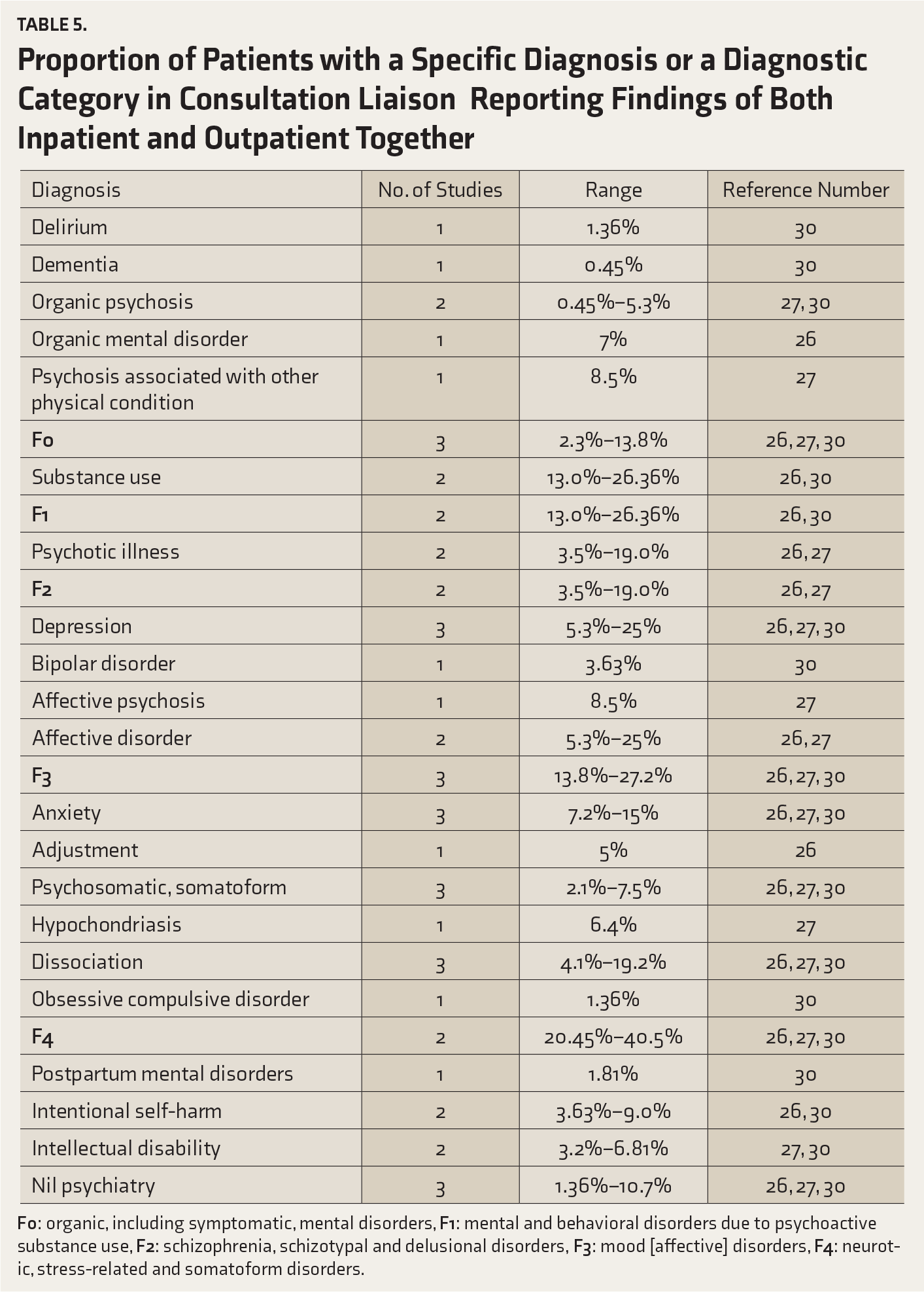
A few studies have been silent about the criteria used to make the diagnosis.12, 16 When the three most common diagnoses reported in the studies were taken into account, depression, organic disorders (including delirium), drug dependence, substance use disorder, intentional self-harm (ISH), anxiety disorders, and dissociative disorders emerged as the most common diagnostic categories. Studies that focused on patients referred to psychiatry outpatient services have, in general, reported neurotic, stress-related, and somatoform disorders to be the most common diagnostic category (
Proportion of Patients with a Specific Diagnosis or a Diagnostic Category in Studies which have focused on inpatients
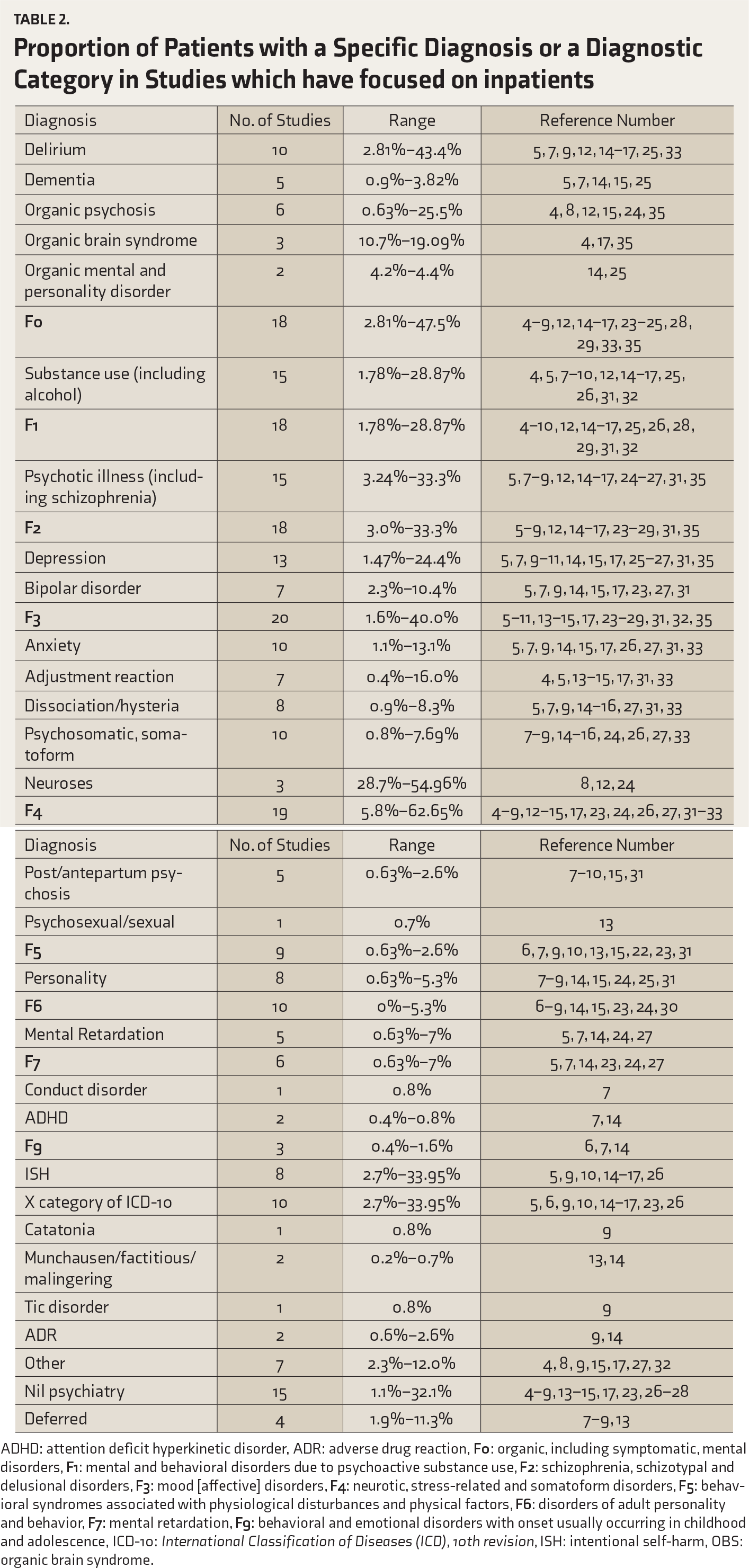
ADHD: attention deficit hyperkinetic disorder, ADR: adverse drug reaction,
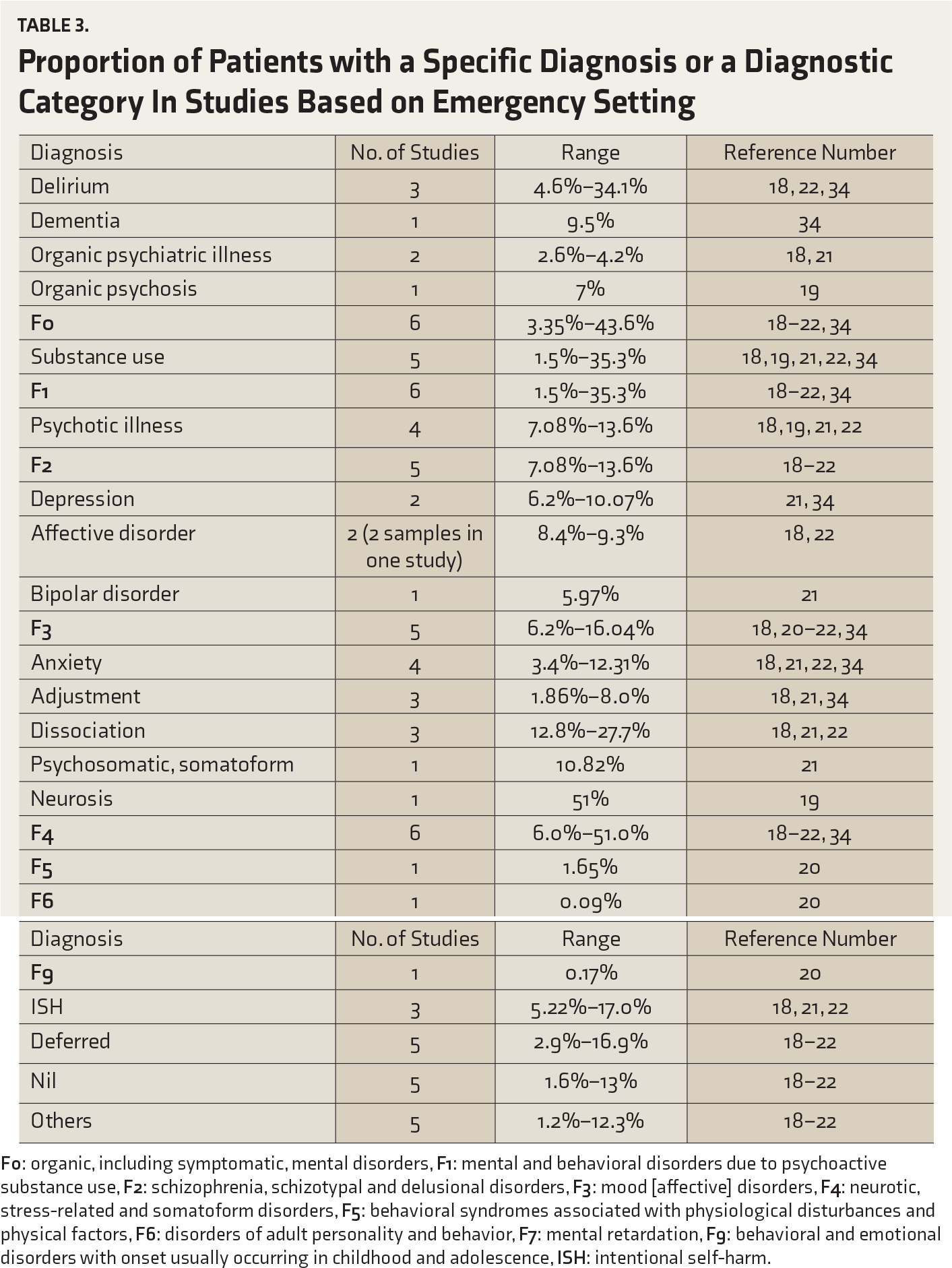
Proportion of Patients with a Specific Diagnosis or a Diagnostic Category In Studies Based on Emergency Setting
Proportion of Patients with a Specific Diagnosis or a Diagnostic Category In Consultation Liaison Studies Based on Psychiatry Outpatient Setting
Proportion of Patients with a Specific Diagnosis or a Diagnostic Category in Consultation Liaison Reporting Findings of Both Inpatient and Outpatient Together
Discussion
This review suggests that only a limited number of studies from India had evaluated the referral patterns to psychiatry and the diagnostic profile of patients referred to CLP services in various medical institutes in the country. There is significant heterogeneity across the studies in reporting patient profile and duration for which the profile was reported. Further, there is a lack of data on specific age groups, with only one study on the profile of elderly patients seen in the emergency setting 34 and one on the profile of pediatric age group referred for psychiatric evaluation. 22 Few studies focused on screening all patients admitted to various medical-surgical wards or the emergency setting. 34
If one evaluates these studies, it is apparent that at present, CLP in the country is mainly functioning on the consultation model only. Further, referral of medically ill patients to the psychiatry outpatient services highlights that there are no CLP teams that can examine the medically ill patients at the bedside. A survey that evaluated CLP services in the country reported the availability of three-tier on-call services (i.e., CLP team comprising a faculty member, a senior resident, and a junior resident) in only one-third of the institutes. Based on this data, it can be said that there is a need to develop a model for reporting patients seen in CLP setting. Further, there is a need to develop a model to collect data simultaneously from different centers, both institutes/medical colleges and corporate hospitals, to understand the training needs in CLP. This would help in evaluating and comparing the CLP services across different institutes and also help different institutes to learn from each other and a comprehensive CLP model can be developed for various institutes in the country. However, one good aspect of the research in this area is that more than half of the studies have emerged in the last 5 years, suggesting that CLP is gaining momentum in the country.
The psychiatric referral rates for inpatients of various medical and surgical wards suggest that 0.01% to 3.6% of patients are referred to psychiatry liaison services.4, 7, 9, 25, 31 The referral rates from emergency set-up varied from 1.42% to 2.4%18, 19, 21and at the outpatient level from 0.06% to 7.17%.24, 27, 33, 36 These findings suggest that the rates of psychiatry referrals are dismal. When one compares these referral rates with the available studies from India that screened patients with various physical illnesses, they suggest the prevalence rates of specific psychiatric disorders to be much higher. For example, one study that screened all the elderly patients visiting an emergency setting reported the prevalence of axis-1 diagnoses to be 47.4%. 34
Accordingly, it can be said that only a very small proportion of medically ill patients who require psychiatric help are actually referred to the psychiatry services. A possible reason for this dismal referral rates could be the stigma associated with mental illnesses. However, if one tries to hypothesize the possible reasons for these dismal rates, they can also be attributed to poor knowledge about mental illnesses among other specialists, poor psychiatry training at the undergraduate levels, and poor exposure of other specialists to the specialty of psychiatry during the postgraduate training. Other possible reasons could be confinement of psychiatry training during undergraduate and postgraduate training to the psychiatry inpatient and outpatient services only. Studies that evaluated the reasons for referral suggested that in general, there is poor concordance in the psychiatry diagnosis made by the CLP teams and other specialists.5, 14 Accordingly, it can be said that there is an urgent need to focus on the stigma associated with mental illnesses in the general public per se, but also among other specialists. 37 Additionally, there is a need to improve exposure to psychiatry during the undergraduate training and for other specialists in their postgraduate training. For undergraduate training, psychiatrists should focus on training the students in identifying various psychiatric issues in medically ill patients, rather than focusing only on those with primary psychiatric disorders. This can be done by having cases for discussion from the medical-surgical wards, rather than limiting training on those from psychiatry wards only. It can also be argued that the low referral rates could be due to the fact that the other specialists themselves manage psychiatry morbidity, rather than referring the patients to the CLP services. However, at present, there is no data to support the same.
A survey of CLP services in India showed a lack of CLP service posting for the junior and senior residents in most institutes in the country. 38 This suggests that there is a need to improve CLP training in India. If one tries to look at the implications of this review in terms of psychiatry training in the country in the background of the previous survey, it can be said that at present, psychiatry trainees are not adequately trained to manage various psychiatric disorders among the medically ill patients. This suggests that they are ill equipped to manage patients with medical comorbidities, and this can lead to improper management of such cases. Hence, there is a need to shift the focus of training, with adequate importance given to CLP. A focus on CLP can also help in improving physical health care of patients with primary psychiatric disorders by the psychiatrist.
The present review also suggests that there is significant heterogeneity in reporting of diagnostic pattern across studies, as reported earlier. 39 Further, there is also heterogeneity across studies in terms of the three most common diagnoses. This heterogeneity possibly reflects the sensitivity of other specialists in recognizing different psychiatric disorders across centers. However, when one tries to evaluate these diagnostic categories, it is apparent that clinical conditions like delirium, depression, substance use disorder, other neurotic disorders, and ISH are very common in medically ill inpatients. Accordingly, there is a need to develop treatment models for assessing and managing these disorders in the medically ill patients.
Most studies are retrospective, with only a few prospective studies. Accordingly, there is a need to carry out more prospective studies.
The present review has certain limitations. It was limited to studies that assessed psychiatric referral patterns and reported multiple diagnoses and referral rates. However, studies reporting referral patterns for specific conditions (for example, ISH, delirium) were excluded. Although efforts were made to trace all the studies, some studies that would have been published but not available on the journal websites, could have been left out. Due to heterogeneity in the reporting of data, we were unable to carry out a pooled analysis or a meta-analysis.
Conclusion
Only a few studies have reported the patient profile seen in CLP set-up. There is much heterogeneity in the reporting profile. Available data suggest that, in general, referral rates to psychiatry services from other specialists are dismal. Accordingly, there is an urgent need to change the focus of psychiatry training at both the undergraduate and postgraduate levels.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.