
Abstract
Background:
The cost of illness (COI) for common mental disorders (CMDs) that include depression, anxiety, and somatoform disorder is less studied in India. Hence, we studied the COI and disability of CMDs and their relationship in patients with depression, anxiety, and somatoform disorders.
Methods:
In this cross-sectional study, we recruited 220 patients (110 with depression, 58 with anxiety disorders, and 52 with somatoform disorders) and evaluated disability using the Sheehan Disability Scale (SDS). The schedule for the cost of illness (S-COI) was used for evaluating COI for the last year.
Results:
The annual COI of CMDs from the patient perspective was ₹21,620 (interquartile range [IQR], ₹47,761; ≈US$290). The median annual direct COI was ₹4,907 (IQR ₹7,502), and indirect COI was ₹12,900 (IQR ₹37744). The direct COI was 18%, whereas the indirect COI was 82%. The direct and indirect COI in the three groups were similar. In all three groups with ongoing treatment, the mean scores indicated a mild level of disability. Total and indirect COI, but not the direct COI, correlated positively with the severity of illness and disability.
Conclusion:
All the CMDs with ongoing treatment are associated with a mild level of disability and are a significant financial burden, with higher indirect costs.
Common mental disorders (CMDs) are associated with mild to moderate levels of disability. Indirect costs of the diseases are much higher than direct costs. Regular treatment and compliance may positively influence the cost of illness.Key Message:
Depressive, anxiety, and somatoform disorders are classified separately in the tenth revision of the International Classification of Diseases (ICD-10). 1 From the perspective of public health and primary care interventions, they are often grouped as common mental disorders (CMDs) because of their higher degree of comorbidity, similar epidemiological profile, and transdiagnostically similar treatment approach.2–4 The consequences of CMDs are not just limited to patients and their social milieu, they affect the entire social fabric, particularly through economic burden. Also, depression is ranked as the single largest contributor to global disability (7.5%), and anxiety disorders are ranked sixth (3.4%). 5 The number of persons having CMDs is increasing, specifically in the low- and middle-income countries such as India. 5 Somatic symptom disorder (somatoform disorders) also has a high prevalence of 5% to 7% in the general population, 6 and together with depression and anxiety disorders, poses significant societal burden and health challenges. Depression, anxiety disorders, and somatoform disorders often co-occur together (also known as the SAD triad), are highly prevalent in society, and constitute major part of CMDs. 7
In India, two-thirds of the population with depression have a disability across domains of work-life (67.3%), social life (68.6%), and family life (70.2%). 8 Anxiety disorders cause disadvantages throughout the lifespan in areas such as income, education, and interpersonal relationships. 9 In somatoform disorders, because of the unexplained medical symptoms and the patient preference to see a general practitioner rather than a psychiatrist, there can be inappropriate and/or excessive use of medical services, which can further increase the health care cost in these patients. 6
The cost of illness (COI) covers the varied aspects of the disease burden on society. It extends beyond the mere cost of treatment to its effect on life expectancy, morbidity, reduced quality of life, cost of premature death, and disability from the illness. COI studies are regarded as a fundamental evaluation technique in health care systems that help find proper preventive and treatment strategies to reduce the economic burden of health problems. 10 Based on the data from 2010, the global direct costs (consultation fee, inpatient charges, medication, and transportation) and indirect costs (loss because of absence from work, unemployment, early retirement, and family burden) of mental disorders were estimated at US$2.5 trillion. 11 However, research on cost analysis of depression and other CMDs in developing countries such as India is scarce.5,12,13 COI studies are considered essential for better policymaking, efficient health resources utilization, effective management of health problems, and the maintenance of the health of the economy, both at the household level and national level.14–16 Hence, we aimed to study the economic burden and societal cost of CMDs. The objectives were (a) to study the COI and disability of CMDs, (b) to study the association between COI and disability in CMDs, and (c) to explore if the COI and disability differ between depression, anxiety, and somatoform disorders.
Methods
Participants
This was a cross-sectional, observational study undertaken from April 2018 to January 2019 at the follow-up outpatient clinic of the Department of Psychiatry, National Institute of Mental health and Neurosciences, Bengaluru, a tertiary care academic neuropsychiatric hospital in South India. The Institutional Ethics Committee approved the study. Convenient sampling was used. Male and female patients in the age group 18 to 65 years, diagnosed with depressive disorder (without psychotic symptoms), anxiety disorders (generalized anxiety disorder, panic disorder, social phobia, anxiety disorder unspecified), or somatoform disorders (somatization disorder and somatoform pain disorder) as per ICD 10 criteria, 1 functioning normally before the onset of the illness, and visiting the psychiatry follow-up outpatient department (OPD) were screened for the study after getting their written consent. Patients with severe symptoms affecting cooperation for the study, presence of psychotic symptoms, comorbid major psychiatric disorders, personality disorders, substance use disorders (except tobacco dependence), or comorbid severe medical disorders were excluded. However, patients with well-controlled medical disorders, as inferred by their self-report of regularity in following up with their physician and regular treatment, were not excluded.
Assuming a frequency (p) of 25% of CMDs in the hospital-based population, ±10% confidence limits, and a design effect of 1.5, the sample size at 95% CI was 110 patients with CMDs. We recruited a total of 220 patients—110 patients with depression, 58 patients with anxiety disorders, and 52 patients with somatoform disorders.
Measures
Sociodemographic and clinical details were recorded using a pro forma designed for the study. Mini-International Neuropsychiatric Interview (MINI) Plus 5.0, 17 a short, structured diagnostic interview developed based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) and International Classification of Diseases (ICD-10), was administered to confirm the diagnosis. Clinical global impression-severity (CGI-S) 18 was used to rate the severity of illness. CGI has been validated for use in CMDs. 19 Sheehan Disability Scale (SDS) 20 was used for assessing disability. SDS is a brief, subjective measure to rate the extent of impairment in three domains—work, social, and family life—on a 10-point visual analog scale. The three domains can be summed up to obtain global functional impairment, with a score ranging from 1 to 30. A higher score is suggestive of higher impairment. A score of ≥5 in any domain indicates significant impairment in the respective domain. 21 The “Schedule for Cost of Illness” (S-COI) was used for evaluating the COI for the last year. S-COI was developed for this study based on the bottom-up approach of the human capital method, taking cues from the cost of dementia care study. 22 It was used after pilot testing on 10 patients.
The study assessment was conducted in the follow-up OPD of the hospital. It took about 45 min for the assessment of one study subject. Information was obtained directly from the subject and the caregiver, and all the study-related assessments of a subject were completed on a single day.
COI calculation using S-COI
Health economics broadly classifies COI as direct and indirect costs. The direct costs consist of health care costs (direct medical) and nonhealth care costs (direct nonmedical). Direct medical costs are defined as medical care expenditures for diagnosis, treatment, rehabilitation, etc. 10 The direct medical costs considered for calculation in this study included consultation fees, costs of diagnostic tests, hospitalization costs, costs of medications, and cost of psychotherapy and other services in the last year. The direct nonmedical costs are related to the consumption of nonhealth care resources like transportation, household expenditures, relocating, property losses, and informal care. 10 In this study, it included the cost of travel, food, accommodation (if any), and other costs incurred during hospital visits. The indirect costs refer to the productivity losses and social welfare losses because of the diseases. 10 Under indirect costs of illness, we covered the cost of leaves/absence from work for health visits of both patient and caregivers, cost of loss of job in last one year of both patient and caregivers, cost of special care, cost of magico-religious practices for illness, and other costs indirectly related to the illness that could be quantified.
To calculate the cost of a particular medicine/tablet spent by the patient, the average value of the cost of the commonly used brands of the drug was considered. The cost of free drugs, which were distributed by the study venue for the poor patients, was calculated from the official price list of the institution obtained from the chief pharmacy and drug dispensary. The cost of psychotherapy provided on-site was not considered, as most patients who receive psychotherapy were exempted from paying for the sessions. Details of the number of visits and treatment over the last year were obtained from the patients’ files in the medical records section. The cost of free medicines and other free services the patients received in other government and charity hospitals was not included as it was not available. For those patients on treatment for less than one year, the projected drug cost was estimated. This was based on the clinical decision made by considering the need for treatment, treatment duration, treatment response, the need for a change of treatment, regularity of patient visits, and treatment adherence. For example, if a patient has been on treatment for the last four months with drug X, the projected drug cost was calculated as the cost of four months divided by 4, then multiplied by 12 to get the total cost of medication for one year. The projected cost was estimated for medication and other medical costs and not for nonmedical and indirect costs. Projected drug cost was also not included in calculating total costs, as indirect cost (actual loss) was already calculated for the last year. For calculating the nonmedical direct cost for one year, the travel and food cost of the current visit was multiplied by the number of hospital visits in the last year. Direct medical and nonmedical costs incurred outside the study site were calculated as per the patient’s recall from memory. Indirect COI was calculated by multiplying the daily income of the patient/bystander by the number of days of loss of work from illness in the last year. For those with no fixed earnings (e.g., farmers), the daily income was calculated based on their overall annual income. The daily income of homemakers was calculated based on how much money they would spend if they had hired a maid to replace patients’ daily household chores. If the patient could not cook food because of illness, their spending on the hotel was also taken into consideration for calculating indirect costs. If the patient was unemployed for a long time or had no fixed job, his/her daily income was calculated based on the earnings of a person of the same locality with characteristics similar to the patient.
Statistical Analysis
Data obtained were analyzed using IBM SPSS Statistics 20.0 (IBM Corp., Armonk, NY, USA) for Windows. Descriptive statistics such as n (%), mean (SD), or median (IQR) were used to summarize data. Pearson’s chi-square test (or likelihood ratio or Fisher–Freeman–Halton exact test) was used to compare the proportions between groups. Kruskal–Wallis test was used to compare the continuous variables, with post hoc Mann–Whitney tests. P values <0.05 (two-tailed) were considered significant.
Results
Of the 220 patients, the majority (66%) belonged to the age group of 30 to 50 years, 63% were women, the majority (65%) were illiterate, and most (45%) did unskilled/semiskilled jobs (Table 1). Among the subjects, 75% were married, 70% belonged to lower socioeconomic status, and 68% lived in nuclear families. Insurance coverage was by Government health scheme for 12%, whereas 8% had employer-sponsored insurance, 2% had private insurance, and the rest did not have any insurance cover. The mean age of patients with somatoform disorders was higher than those with depressive disorder, which was higher than that of anxiety disorder patients. The proportion of females was higher in depression and somatoform disorder groups, whereas males were more in the anxiety disorders group. Lower education levels and lower socioeconomic status were more frequent in patients with somatoform disorders than in the other two groups (Table 1).
Sociodemographic Characteristics
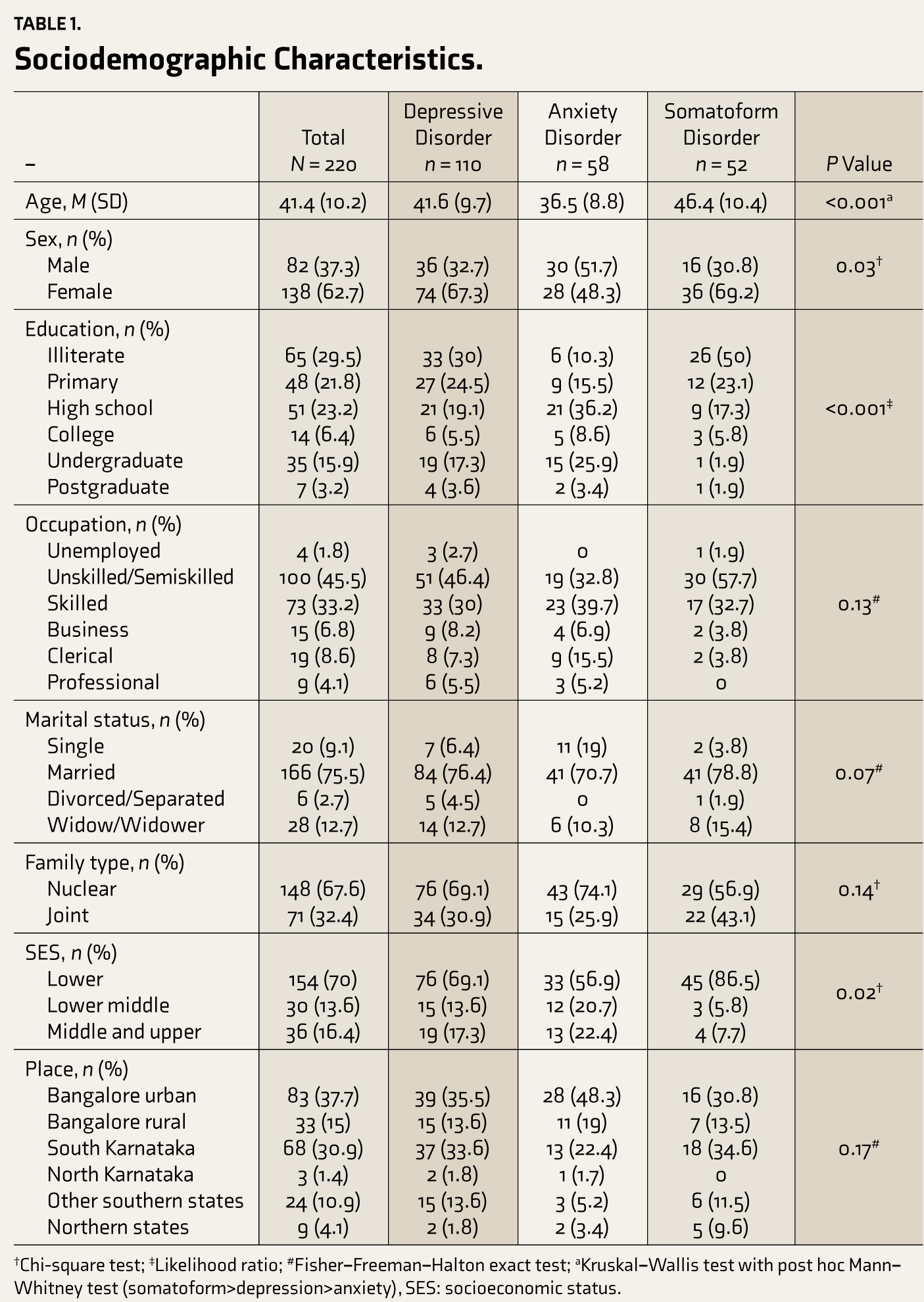
The mean duration of illness in the sample was 6.3 (SD = 6.4) years, and the mean duration of treatment was 4.1 (SD = 5.4) years. Almost 38% of patients had another CMD as a comorbid condition. The common psychosocial stressors reported were financial problems (21%), interpersonal problems (22%), death of a close relative (12%), and neglect by family members (10%), among others. The participants were receiving antidepressants such as amitriptyline (43%), escitalopram (33%), fluoxetine (19%), venlafaxine (5%), mirtazapine (5%), sertraline (3%), and paroxetine (2.5%). The median number of hospital visits in one year was 7 (IQR 6), and the total time spent was 28 (IQR 40) h. The median distance traveled by the patients was 50 (IQR 109) km. Among the patients, 57% were accompanied by others, and the common mode of travel was public transport bus (73%).
The median direct medical cost of the sample in one year was ₹3,705 (IQR ₹5,483), and the median direct nonmedical cost was ₹1,600 (IQR ₹3,275). The direct medical cost included costs at other hospitals (49%), cost of medicines borne by patients (22%), projected drug cost (22%), cost of medicines incurred by the hospital (4%), diagnostic tests (2%), and registration (1%). The direct medical cost was 66%, whereas the nonmedical cost included the cost of travel (27%) and the cost of food and accommodation (7%). The total annual indirect COI for the sample was ₹12,900 (IQR ₹37,744). The breakup of indirect costs included the cost of loss of work of the patient (73%), cost of loss of work of the caregiver (10%), cost of religious practices (7%), cost of leaves for consultation (5%), cost of caregiver’s leaves (5%), and cost of alternative practices (<1%). The direct COI was 18%, whereas the indirect COI was 82%. The direct and indirect costs of illness in the three groups were similar (Table 2). The indirect costs were much higher than the direct costs overall and in all three groups. The median cost of psychotropic medication for a single CMD (₹842, IQR ₹2,538) was significantly less than that for multiple CMDs (₹1564, IQR ₹2,431; P = 0.03). Also, 44% of the study subjects were on irregular medication, and the median cost of medicines in those having irregular treatment (₹554, IQR ₹1,286) was significantly less than that of those on regular treatment (₹1,387, IQR ₹2,923; P = 0.028).
COI for One Year
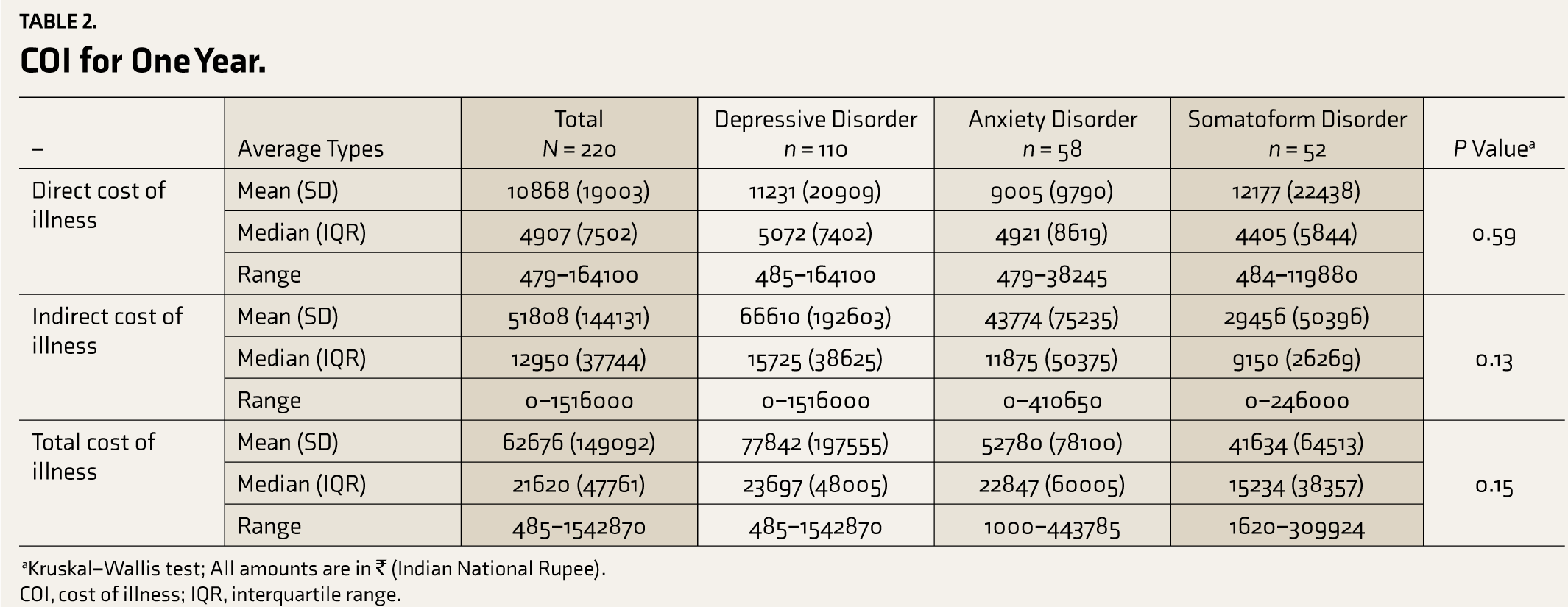
COI, cost of illness; IQR, interquartile range.
The mean (SD) CGI-S score was 3.12 (1.08), 3.35 (0.97), and 3.15 (0.89) in those with depression, anxiety, and somatoform disorders, respectively, and there was no difference between the groups (P = 0.42; Table 3). There was no difference between the three groups on SDS scores as well (P = 0.55). In all three groups, most of the subjects had a moderate level of disability. None of the study subjects with somatoform disorders had a severe level of disability.
Severity of Illness and Disability of CMDs

CGI-S, clinical global impression-severity; SDS, Sheehan Disability Scale; CMDs, common mental disorders.
Discussion
In our study, the annual average direct cost (medical and nonmedical) per person was approximately ₹11,000 (US$160) and the annual average indirect cost amounted to ₹53,000 (US$760). The total annual cost was about ₹64,000 (US$920). Indirect costs were much higher than direct costs. The annual indirect costs were six times higher than direct costs in the case of depression, five times higher in anxiety disorders, and 2.5 times higher in somatoform disorders, indicating that patients with somatoform disorders tend to spend relatively more on direct costs because of doctor shopping. Overall, indirect costs in CMDs were five times higher than direct costs.
Correlations Between the Cost of Illness, Severity, and Disability in Common Mental Disorders (
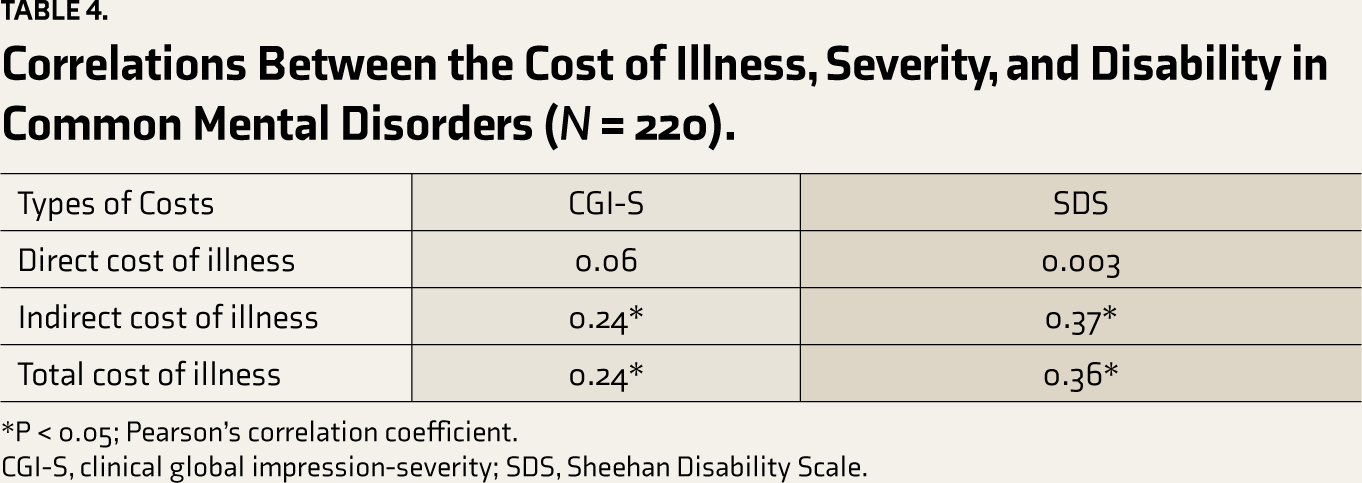
CGI-S, clinical global impression-severity; SDS, Sheehan Disability Scale.
A systematic review of the COI in depression involving 24 studies showed that indirect (morbidity) costs were higher than direct costs and that depression was associated with a high economic burden. 23 Another meta-analysis that studied the COI in depression across different age groups (adolescence, adults, and older adults) reported that depression was associated with higher direct costs in all age groups, though most studies included in this meta-analysis did not emphasize indirect costs. However, the study reported higher indirect costs in adults, and further research on indirect costs was suggested. 24
A meta-analysis on economic burden reported that anxiety disorders were associated with a low proportion of health care costs on a population level but significantly increased health care costs on an individual level. 25 Furthermore, the authors reported that the COI was higher for generalized anxiety disorders than for social phobia. They conclude that further COI research is needed in less studied disorders such as panic disorder. 26 Another systematic review of 20 COI studies in anxiety disorders focused on generalized anxiety disorders and panic disorders (though they also included phobias) and reported that anxiety disorders cause considerable direct costs. However, they identified that differing inclusion of cost categories limited the comparability of COI. 27
A review on COI in medically unexplained symptoms (MUS) reported that MUS can cause excess annual costs in health care comparable to disorders like depression or anxiety disorders. The authors also found a lack of research on indirect costs, which they consider high in MUS, and hence, it should be a focus for further research. 27 A retrospective cross-sectional study involving 294 patients with MUS studied the association of costs with somatic symptom severity. The authors concluded that MUS is associated with relevant direct and about seven times higher indirect costs that strongly depend on somatic symptom severity. The direct costs primarily increased in severe cases, whereas the indirect costs increased continuously from mild through moderate to severe cases of MUS. However, the authors opined that this latter fact needs further research, though they suggested early interventions for mild MUS itself, given the economic burden. 28
We did not come across original studies with a methodology similar to ours that had compared direct and indirect costs. Most previous research is on direct costs, and the studies had inferred that the costs are high. Although the studies on indirect costs in CMDs are limited, our study replicates the findings from the existing studies that indirect costs are significantly higher than direct costs in all CMDs including somatoform disorders23,24,25,28 and hence supports intervention at early stages.
The average total monthly cost per person exceeded ₹5,000 (equivalent to US$73 in 2018) in our study, and 80% of this was attributable to indirect costs. In that, the proportion of direct monthly cost was ₹635 (US$9), which is similar to a recent Indian study that quoted a direct cost of ₹790 for recurrent depressive disorder. 29 Furthermore, the longer the duration of treatment, the lesser the indirect COI, i.e., continuing treatment for more than one year significantly reduced the indirect cost in our study. Thus, though they cost more, regular medication resulted in better recovery, thus causing less financial burden in the long run than in those having irregular treatment. Quicker recovery resulted in better income because of consistent work, which led to decreased indirect costs. It indicates that a decrease in indirect costs is the key to reduced COI.
We compared depression, anxiety disorders, and somatoform disorders for COI as well as disability, and they were evenly matched in terms of both COI and disability. We did not find other studies that compared different CMDs head-to-head for COI and disability. The indirect and total costs correlated positively with the severity of CMDs and the level of disability but not the direct cost. All our patients rated mild on CGI-S for severity. Depression and somatoform disorders were seen more in females than males, which is the difference in their prevalence rate in the general population. Also, most subjects with somatoform disorders belonged to lower socioeconomic strata, a finding common to somatoform disorders. 30 CMDs are associated with disability, though their severity level is less compared to the major mental disorders. In our study, the average total scores on SDS were in the range of 9 to 10, for the whole sample as well as each disorder group, indicating a mild level of disability. There was no statistically significant difference across diagnoses. A recent study from Portugal reported disability in 14.6% of the study sample of CMDs, using the modified World Health Organization Disability Assessment Schedule for the World Mental Health Survey (WMHS) Initiative. The specific disorders assessed were PTSD, depression, generalized anxiety disorder, and bipolar disorder. The authors inferred that such assessments contribute to mental health efforts in developing interventions to reduce the burden of disability associated with CMDs. 31 Although in India patients with CMDs are not eligible for disability benefits, the mild level of disability measured was possibly because of the ongoing treatment. Thus, timely interventions can be considered essential to reducing the burden of disability associated with CMDs. Further, our study has shown that the economic burden can worsen if the illness is untreated, as the illness can worsen further because of the lack of treatment.
Carer burden is a significant issue in the care of mentally ill persons. The unpaid carers (family members) may have to spend substantial time caring for mentally ill relatives. Caregivers of patients with somatization disorder and depression have also been reported to experience a burden comparable to that seen in schizophrenia. It involves different domains like finances and family routine. 32 Developed countries like Australia and the UK provide financial aid to carers, in the form of carer allowance. In India, unpaid carers are not formally recognized and do not get separate financial support. The Right to Persons with Disability Act 2016 has a provision for a carer allowance, but that provision has not yet been implemented. 33 Although patients in India receive a disability pension of ₹1,500 per month, it is available only for major mental disorders, and patients still end up with high out-of-pocket expenses. These are the areas that need major policy changes to enhance mental health funding in India.
The cross-sectional design is a limitation of our study. Further, the sample size calculation for estimating the COI need not be based on the prevalence of that particular illness. Hence, we consider this also as a limitation. Nevertheless, we used standardized, validated tools for assessing disability and severity of illness. A longitudinal study can be more accurate for the precise calculation of costs. However, dropouts are inevitable in such designs, which can sometimes be too high. Because it was a cross-sectional study, we relied upon patient recall for some findings. Therefore, there is a possibility of over-estimation of intended measures because of possible recall bias. This recall bias could have affected the scientific validity of our study, and hence, we recognize this as a limitation. Also, we could not include the cost of free medications received from other government/charity institutions because of the nonavailability of their price. Further, the cost estimated for patients who were on treatment for less than one year may not be accurate. Because this is not a multicentric study, the findings from one government-sector tertiary psychiatric referral hospital will be difficult to generalize, especially to the population that belongs to the higher socioeconomic strata, which prefers treatment from the private sector, though it comprises less than 20% of the total Indian population. Issues of stigma and privacy may make most patients with CMDs seek treatment from private clinics. Nevertheless, the estimated cost might have been higher if there was equal representation from all socioeconomic strata. Also, though convenient sampling is not an inappropriate sampling method for such hospital-based studies, it has its limitations because of selection bias. We may have missed some diagnostic categories with a high COI, as we relied on those patients visiting the hospital OPD. Depression seems to be overrepresented compared to other CMDs in our study, but it is also highly prevalent. Besides, from the broader management perspective, it may be practical to view CMDs as transdiagnostic. Nevertheless, estimation of COI with an emphasis on both direct and indirect costs and comparing different CMDs for disability and costs is a unique work. The outcome of this study should encourage further refined research to overcome its limitations.
Conclusion
CMDs are associated with a significant financial burden to the person and family, though the level of disability can be mild, because of ongoing treatment. Indirect cost was almost five times higher than the direct cost in all CMDs, and it did not differ across diagnoses. The indirect and total costs correlated positively with the severity of CMDs and level of disability, but not the direct cost. The authors suggest a multicenter, longitudinal study with a larger sample size and uniform distribution of all categories of CMDs, to get results that would be more generalizable. Nevertheless, the authors consider that early intervention and regular treatment have an important role in reducing the COI in CMDs.
Footnotes
Acknowledgements
We are grateful to the faculty and scholars of the Department of Biostatistics at NIMHANS, Bengaluru, for their role in guiding the study tools.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning this article’s research, authorship, and publication.
Funding
The authors received no financial support for the research, authorship, and publication of this article.