
Abstract
Background:
Common mental health disorders (CMDs) affect nearly 10% of the population, with the majority (80%) remaining untreated. Culturally relevant counseling approaches can be a means to reach many untreated persons. We describe the development and validation of a socioculturally relevant counseling module based on the Ramayana for persons with CMDs.
Methods:
The study employed an exploratory research framework to design the counseling module. The module underwent a comprehensive review of the Valmiki Ramayana to ensure its cultural relevance. Content validation was performed by mental health professionals from the field of Indian psychology. Concurrently, a panel of 15 experts from diverse backgrounds in Indian psychology validated the counseling module based on the Ramayana.
Results:
Based on the results of expert interviews (n = 15), the counseling techniques, encompassing concepts, anecdotes, and narratives, were finalized. These interviews also contributed to the refinement of the counseling module. The primary objective of the content validation process was to systematically assess the appropriateness, accuracy, and practicality of the various components within the module. The content validation demonstrated that all items contained within the module exceeded the established threshold of p = .59.
Conclusions:
The developed counseling module based on the Ramayana is feasible to be implemented as a sociocultural intervention for persons with CMDs. By assisting persons to enhance coping abilities and improve overall well-being, this module offers a valuable resource for mental health intervention in the Indian sociocultural context. It fosters a culturally sensitive and practical approach to address the diverse mental health needs of the population.
This study represents one of the first-ever attempts to develop a module for Ramayana-based counseling interventions in the field of psychiatry in India. It provides a comprehensive guideline on how to implement the Ramayana based counseling module in clinical setting for persons with common mental health disorders in the relevant contexts. The feasibility and efficacy testing of this module will help to establish its worthiness and practical application in the future.Key Messages:
Common mental health disorders (CMDs) are characterized by significant difficulties experienced in emotion regulation. Persons diagnosed with CMDs manifest heightened levels of psychological distress, exerting deleterious effects on their personal, social, and occupational dimensions. 1 The substantial treatment gap of 80.4% indicates that the majority of CMDs remain untreated due to various psychosocial factors such as stigma, lack of awareness, socioeconomic status, and help-seeking behaviors, among others.2,3
Several therapeutic approaches are evidence based in the context of CMDs. Different psychotherapies have demonstrated efficacy and cost-effectiveness in treating CMD conditions such as depression, anxiety, stress-related disorders, and somatoform disorder. 4 These gold standard psychotherapies include psychoanalytical therapy, cognitive behavioral therapy (CBT), emotional-focused therapy (EFT), brief dynamic therapy (BDT), and interpersonal therapy (IT). Over the past few decades, numerous brief psychotherapies and culturally relevant counseling techniques have emerged for the treatment of CMDs. While these psychotherapies and counseling share the common goal of assisting distressed persons, they differ in the delivery of concepts, methodologies, and techniques. 5 As most of these therapies emphasize the emotional regulation process of persons experiencing distress, they are often effective in helping them cope with various challenges.
Similarly, Indian texts exhibit qualities akin to counseling, offering concepts applicable in clinical and therapeutic settings for the benefit of clients. 6 These therapeutic elements, rooted in Indian scriptures, serve as guiding principles for morality, values, and life management. For example, one of the renowned discourses in Hindu philosophy and psychotherapy comes from the Bhagavad Gita, which continues to serve as a spiritual guide to the vast majority of the population across the globe. 7
Some researchers have suggested that narratives and concepts derived from ancient mythology possess therapeutic potential8–11 and can prove effective when used in “appropriate” clinical contexts.6,12,13 An extensive body of literature asserts that the essence of psychotherapy and counseling is embedded within our Indian texts.6,9,14–25 Researchers have delved into Indian epics such as the Bhagavad Gita and Ramayana, revealing numerous aspects parallel to Indian culture.19,26 However, the Bhagavad Gita has been extensively explored, and since there are only two Indian epics, Ramayana was considered for the study. It is more about what each character tells others and the lessons we learn from them than the characters themselves. These concepts, narratives, and anecdotes could be helpful in cultural contexts and improving the coping as well as the well-being of the clients. For instance, when Sita is abducted by the demon king Ravana in the Ramayana, Rama expresses anger and helplessness. In response, Lakshmana advises Rama to identify the responsible individual rather than reacting impulsively with destructive anger toward others. This counseling approach by Lakshmana exhibits techniques akin to those described in Gestalt therapy, emphasizing a perspective focused on the “here and now”—directing attention to the task of finding Sita instead of self-blame for her abduction. Lakshmana also reinforces Rama’s strength of character and self-regulation, highlighting his typical ability to handle situations appropriately. 26 Counseling techniques consisting of selected anecdotes, concepts, and narratives from the Ramayana for persons with CMDs in India could be culture sensitive and easily applicable as people living in India would be familiar with Indian literature.6,23,27–31 Further, a systematic method of iterations to identify the anecdotes, narratives, and concepts from the Ramayana to address issues faced by persons with CMDs could add to the Indian counseling literature. In this context, we aimed to develop and validate the counseling techniques based on the Ramayana for persons with CMDs in India.
Methods
The Institute Ethics Committee (IEC) of the National Institute of Mental Health and Neurosciences reviewed and approved the study. Written informed consent was obtained from expert mental health professionals. The study is registered in the Clinical Trials Registry India (CTRI) under the registration number CTRI/2020/06/025572.
Study Design
The study employed an exploratory research design. The development and validation of the Ramayana-based counseling module were conducted in two phases: (a) Phase I: review of the Ramayana- based counseling module for CMDs and (b) Phase II: validation and finalization of the Ramayana module for persons with CMDs. Data collection took place between December 2018 and July 2021. Further details of each phase are provided below.
Phase I—Review of Ramayana
The first author extensively examined both the English and vernacular language (Marathi) versions of the Ramayana to gain an in-depth understanding of the content of the texts. The first author conducted several reviews of the Ramayana to compile verses that illustrate counseling techniques akin to anecdotes, concepts, and narratives. According to Pepisky and Pepisky, counseling is an interaction between two individuals called counselor and client, takes place in a professional setting, and is initiated and maintained to facilitate changes in a client’s behavior.
32
Based on this definition, we have formulated an operational definition to serve as a tool or method to extract anecdotes, concepts, and narratives from the Ramayana, as given below. The following counseling definition guided these reviews:
Interaction or dialogues between two individuals Distressful situations Behavioral outcomes result from counseling provided by the characters in Ramayana
Each review had specific objectives for selecting relevant anecdotes. After each review, the authors, along with their guide and co-guide, rigorously evaluated the outcomes, which included counseling techniques such as anecdotes, narratives, and concepts. These counseling techniques underwent a comprehensive review and consolidation process. Initially grouped into general themes (GT) based on shared emotional contexts, they were further refined by an internal committee member (PS), who merged closely related themes to form specific themes (ST). These specific themes were then carefully examined by external doctoral committee members (DCM) and co-guides to highlight closely associated concepts. Subsequently, the 14 themes, comprising anecdotes, narratives, and concepts, were presented to a panel of experts who needed to be made aware of thematic similarities. This process aimed to ensure clarity and objectivity in the evaluation.
Phase II—Validation from Experts and Finalizing the Techniques
The authors prepared a list and approached mental health professionals using snowball sampling in this study. The inclusion criteria involved mental health professionals with at least five years of clinical experience in Indian psychology and proficiency in English. Maximum variation sampling was employed to ensure a diverse representation of mental health professionals within the sample. A total of 23 experts were contacted, with eight citing busy schedules as the reason for non-participation. Nevertheless, 15 experts consented to participate, comprising three psychiatrists, three clinical psychologists, two psychiatric social workers, and seven professionals with specialized knowledge in Indian psychology and scripture, along with a background in yoga. No incentives or compensation was provided to the expert participants during the data collection process. For the content validity assessment, data were collected from experts through an iterative process, employing two methods: (a) in-depth interviews and (b) content Validation.
In-depth interviews: This qualitative research design employed structured qualitative interviews to facilitate and guide discussions with experts. This phase aims to conduct a content validation process on the culled counseling techniques (anecdotes, narratives, and concepts) from the Ramayana.
It is imperative to emphasize that this phase does not entail data generation, as the cull-out counseling techniques were already identified through an iterative review process in Phase I. Mental health professionals with specialized clinical experience and expertise in Indian psychology and scripture were pivotal in facilitating consensus on themes and refining anecdotes during this phase. Expert (N = 4) interviews were conducted online and audio-recorded, and each lasted for two to four hours. Experts were provided with a script containing collected anecdotes, concepts, and narratives from the Ramayana to aid in conducting in-depth interviews. A structured PowerPoint presentation was also prepared, outlining the study’s title, aims and objectives and the organization of the five stages of the counseling process, which was explained to the experts. The 14 themes were categorized according to shared contexts and assigned numerical codes. Each theme comprised six to nine anecdotes accompanied by associated images. Although the themes were grouped based on everyday contexts and coded with numbers, the specific codes remained unknown to the experts. After completing each theme, the experts were presented with targeted questions for assessment.
What is the context/theme?
What emotions are brought forth in the anecdote from the Ramayana?
Do the listed anecdotes, concepts, and narratives from the Ramayana depict any counseling techniques? If so, which ones? In what contexts can these counseling techniques be used?
What is the process for delivering/providing these techniques? How will these particular techniques help individuals with CMD? Which specific outcomes are likely to improve?
Are there any other concepts, anecdotes, or narratives in the Ramayana that the list does not include and needs to be included?
The interviews, which lasted two to four hours, were conducted over multiple sessions to facilitate comprehensive discussions and collect experts’ perspectives on the applicability of anecdotes in modern counseling. Due to time constraints, all four experts specializing in Indian psychology had to schedule appointments twice each to complete the refinement and validation of the anecdotes. Following these sessions, experts recommended a quantitative approach for content validation of the module, citing the time-consuming nature of in-depth interviews and the potential scheduling difficulties for experts required to attend multiple appointments for refining anecdotes.
Furthermore, these interviews were transcribed and reviewed for consensus on anecdotes. As previously mentioned, each counseling technique (anecdotes, concepts, and narratives) was categorized into 14 themes unfamiliar to the experts. These techniques underwent scrutiny and analysis to assess their agreement with the pre-established themes proposed by the authors before the interviews. The in-depth interview analysis suggests the removal of several anecdotes from the module due to their limited relevance to contemporary illness contexts.
The remaining anecdotes were classified into four groups using the International Classification of Diseases-10 (ICD-10), which included conditions such as depression, anxiety disorders, somatoform disorders, and stress-related disorders. Each diagnosis was associated with an everyday context, followed by supporting anecdotes corresponding to the ICD-10 diagnostic criteria. After refining the anecdotes, the module was structured according to the five phases of the counseling process recommended by the guide. These phases are: Phase I: understanding the problem, which consists of (i) relationship building and (ii) problem assessment; Phase II: goal setting; Phase III: counseling techniques; Phase IV: implementation and change; and Phase V: termination. These phases of the counseling process serve as a valuable framework and guidance in the therapy setting when working with clients.
Content validation: The objective of this phase was to validate the module’s content. To achieve this, a structured Google Form and the Ramayana-based counseling module were sent to experts (n = 11) who agreed to participate in the study. The questionnaire consisted of seven sections, each containing five questions. Each question was rated on a 5-point Likert scale, assessing the appropriateness, adequacy, and practicality of implementing the module. Additionally, the fifth question in each section was open ended, allowing experts to provide suggestions for any necessary changes to the module. These seven sections were organized into sections based on the module’s framework as follows: (a) introduction to Ramayana module and consent of experts; (b) understanding the problem; (c) goal setting; (d) counseling techniques; (e) implementation and change; (f) termination; and (g) overall suggestions. To calculate the content validity ratio (CVR), the responses on the 5-point Likert scale were combined as follows:
Positive rating: very appropriate + appropriate = 1 Neutral rating: neither appropriate nor inappropriate = 2 Negative rating: inappropriate + very inappropriate = 3
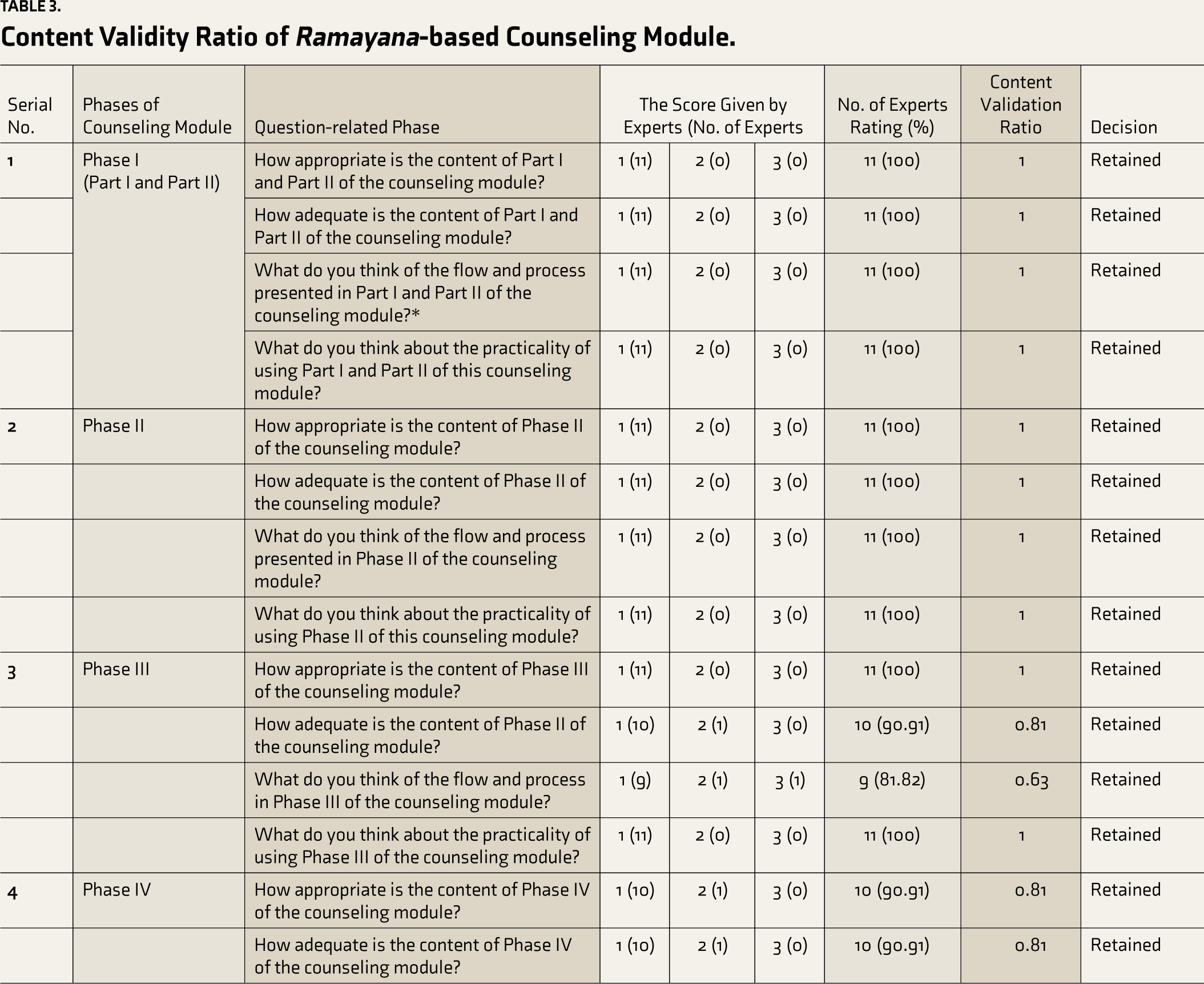
Content validity was established through input from 11 experts who evaluated the appropriateness, adequacy, and practicality of calculating the CVR. Lawshe’s CVR table was used to compute each item in the module, with each item achieving a CVR of 0.5 or higher, demonstrating agreement beyond chance among the 11 experts. 33
Results
This study phase encompasses data analysis from in-depth interviews and content validation provided by experts in Indian psychology.
Phase I: Review of Ramayana
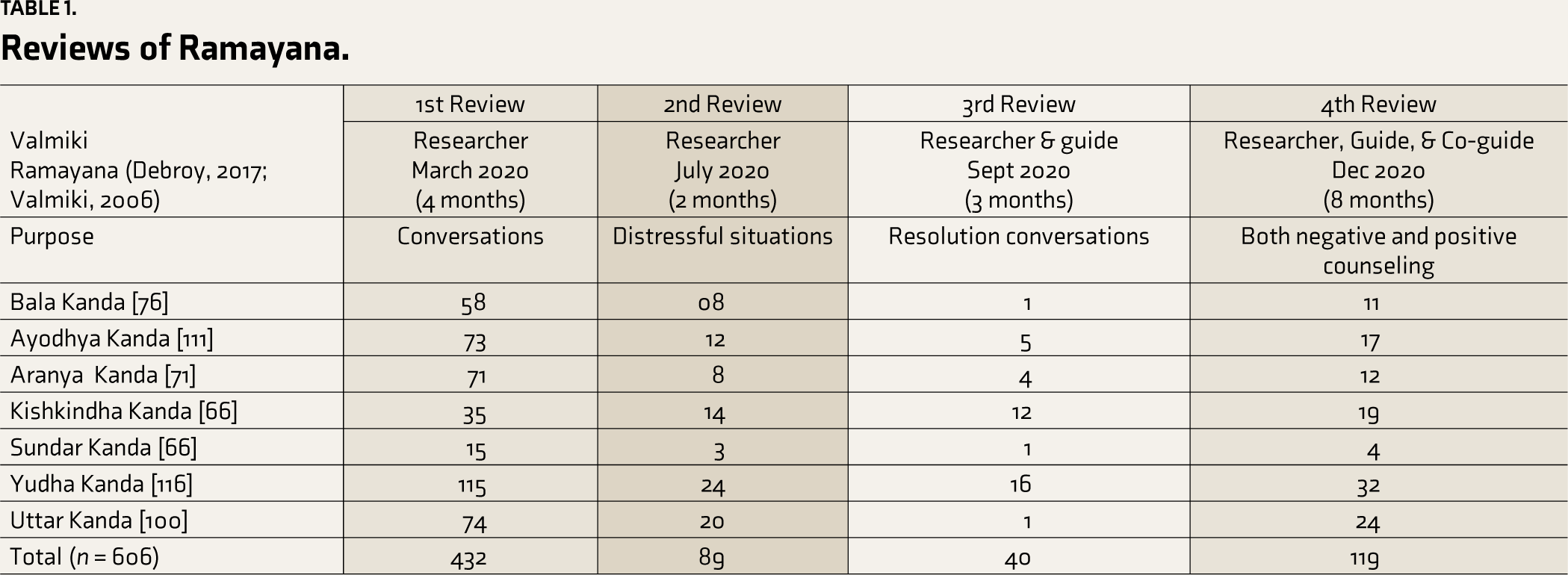
A total of n = 5 reviews were conducted, with each review having distinct goals to extract Ramayana-based counseling techniques. In the first review, the objective was to extract conversations depicted in the Ramayana. The results of this review revealed a total of n = 432 counseling techniques (anecdotes, concepts, and narratives), representing conversations from the Ramayana across its seven Kandas: Bala Kanda (n = 49), Ayodhya Kanda (n = 73), Aranya Kanda (n = 71), Kishkindha Kanda (n = 35), Sundar Kanda (n = 15), Yudha Kanda (n = 115), and Uttar Kanda (n = 74).
Similarly, the second review of Ramayana aimed to identify counseling techniques that involved distressful situations and counseling provided to the characters in the Ramayana. This review also resulted in a total of n = 89 counseling techniques (anecdotes, concepts, and narratives) encompassing distressful situations (anecdotes, narratives, and concepts) that contained the counseling techniques across the seven Kandas of Ramayana.
The objective of the third review was to assess whether the selected anecdotes aligned with the inclusion criteria of counseling definitions, which encompassed interaction or dialogues between two people, distressful situations and the presentation of effective outcomes based on counseling provided by others. The results of this review suggested n = 40 anecdotes out of the previously identified n = 89 counseling techniques based on the inclusion criteria for counseling.
In the fourth review, under the guidance of a primary guide and a co-guide (experts in Ramayana), the researcher read the Ramayana to extract anecdotes. To ensure thorough oversight, both the guide and co-guide decided to read the Valmiki Ramayana independently alongside the researcher, carefully monitoring and supervising the adaptation of counseling techniques from the epic to develop the counseling module. During the process of revisiting and revising counseling techniques, encompassing both negative and positive elements of counseling outcomes such as physical, cognitive, or spiritual changes depicted within the verses of the Ramayana, this review was conducted. Additionally, this review helped minimize bias and identify potential anecdotes that may have been overlooked or neglected while compiling previous reviews to extract counseling techniques. The four reviews presented n = 119 counseling techniques (anecdotes, narratives, and concepts), with details provided in Table 1.
Reviews of Ramayana.
In the fifth review, the researchers aimed to eliminate counseling techniques related to group counseling, as the study focused solely on individual conversations (dialogues between two people). This review decided to maintain the study’s focus on the dynamics and nuances of one-on-one interactions, ensuring a more targeted analysis of individual counseling scenarios. The results of the fifth review are presented as follows: Bala Kanda had 1 group counseling technique out of 11, Ayodhya Kanda had no group counseling techniques out of 17, Aranya Kanda had 1 out of 12, Kishkindha Kanda had 2 group counseling techniques out of 19, Sundar Kanda had none out of 4, Yudha Kanda had 2 out of 32, and Uttar Kanda had 6 out of 24. Therefore, as a result of this review, the 12 group counseling techniques were excluded from the n = 119 anecdotes.
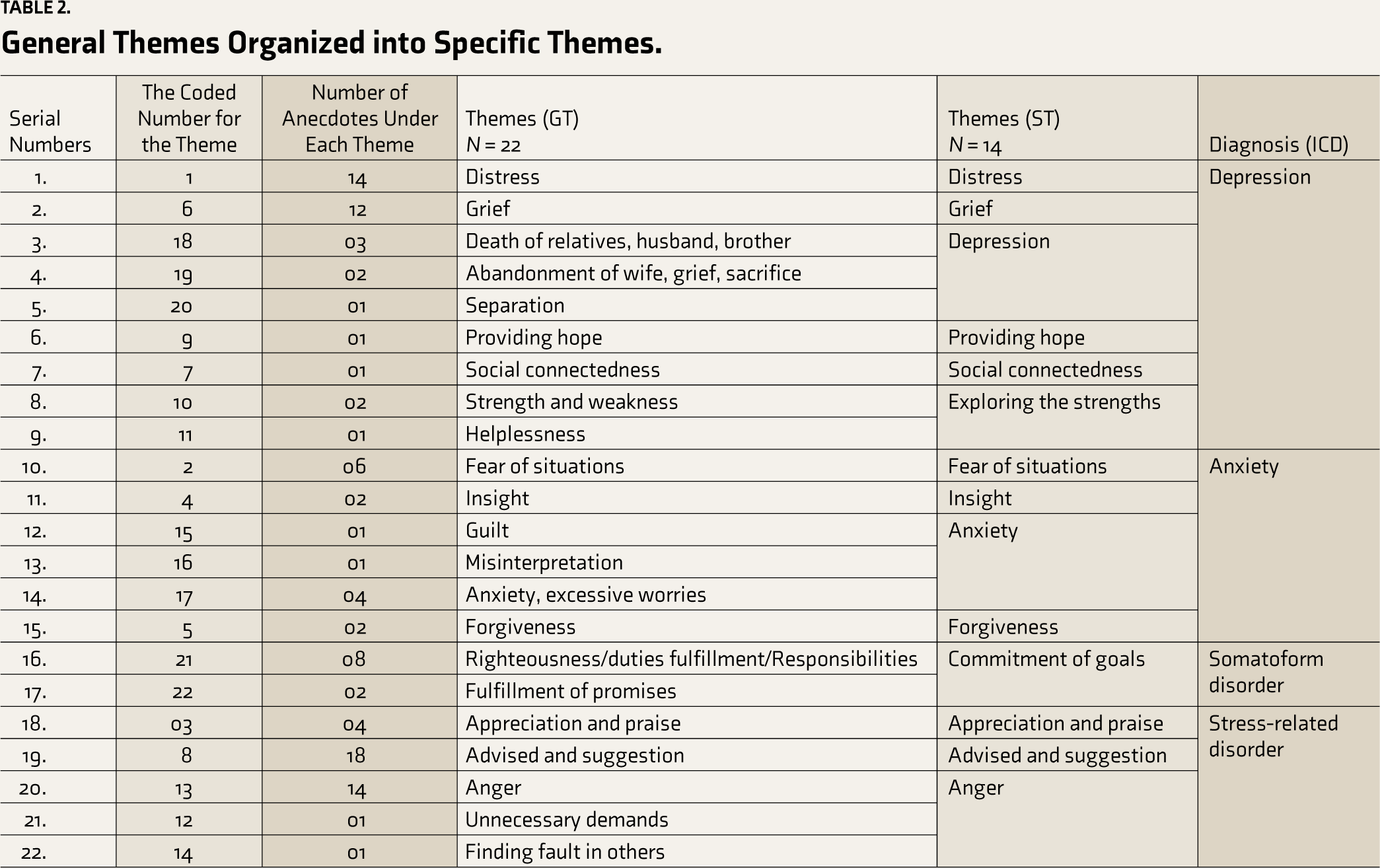
Furthermore, 107 anecdotes were retained and are depicted in Table 2. This table illustrates the themes derived through consensus among the authors and two additional experts during the review of anecdotes. Initially, these anecdotes were categorized into general themes (n = 22) based on shared contexts of emotion, situations, or events. Later, they were further refined into specific themes (n = 14) based on these shared everyday contexts (broader themes) with the assistance of the study’s internal doctoral committee member. Details of the themes are provided in Table 2.
General Themes Organized into Specific Themes.
Phase II: Validation from Experts and Finalizing the Techniques
This study phase included results from in-depth interviews and content validation from experts in Indian psychology. These mental health professionals had expertise in Indian psychology. Four experts consented to in-depth interviews (n = 4) to understand the relevance and accuracy of the listed anecdotes from the Ramayana, and 11 experts consented to content validation of the module. The demographic details of the experts involved in the validation process for developing Ramayana-based counseling are as follows: the average age was 45.33 years (SD = 6.9), the experts had an average of 16.73 years of education (SD = 1.9), and their total years of work experience averaged 17.33 (SD = 8.8). The mean (SD) years of clinical experience was 14.13 (SD =7.0). There were male (n = 11) experts and female experts (n = 4) in Indian psychology. Out of these 15 experts, 7 had a background in Sanskrit, Yoga, and Indian scriptures, 3 were psychiatrists, 3 were clinical psychologists, and 2 were psychiatric social workers. These experts were from different states such as Karnataka (n = 10), Maharashtra (n = 2), Tamil Nadu (n = 2), and West Bengal (n = 1). Similarly, the experts belonged to various universities and institutes such as the National Institute of Mental Health and Neurosciences (NIMHANS) (n = 8), Swami Vivekananda Yoga Anusandhana Samsthana (SVYASA) (n = 2), and other institutes, including the Indian Institute of Technology (IIT) Kharagpur (n = 1) and MIT School of Vedic Sciences (n = 4). We elucidated the expert’s responses obtained during the content validation process listed in the paragraphs. These results are shown from the (a) in-depth interview and (b) content validation recorded below.
In-depth Interview
An in-depth interview involving four mental health professionals with expertise in Indian psychology was conducted. A total of 107 anecdotes, categorized into 14 themes based on everyday contexts such as emotions, situations, or events, were presented to the experts. This interview aimed to understand the relevance and accuracy of the listed counseling techniques (anecdotes, concepts, and narratives) from the Ramayana for individuals with CMDs. Experts recommended removing 55 counseling techniques (anecdotes, concepts, and narratives) due to their irrelevance in present clinical contexts. These included results from Bala Kanda (n = 5; not relevant to current contexts), Ayodhya Kanda (n = 6; not relevant to current contexts), Aranya Kanda (n = 6; not relevant to current contexts), Kishkindha Kanda (n = 6; not relevant to current contexts), Sundar Kanda (n = 2; not relevant to current contexts), Yudha Kanda (n = 12; not relevant to current contexts), n = 6 (counseling was not successful), and Uttar Kanda (n = 11; not relevant to current contexts; n = 1; counseling was not practical). After eliminating these 55 techniques, 52 counseling techniques were retained out of the initial 107.
A total of 52 remaining anecdotes were categorized into four groups as associated with disorders such as depression, anxiety disorder, somatoform, and stress-related disorders using ICD-10 diagnosis criteria. Each diagnosis had everyday contexts, followed by anecdotes supporting the diagnostic criteria per the ICD-10. Depression had 11 everyday contexts followed by 22 anecdotes; anxiety had 10 familiar contexts followed by 11 anecdotes; somatoform disorder had 6 contexts followed by 6 anecdotes; and stress-related disorder had 13 contexts followed by 13 anecdotes. Furthermore, the structure of the counseling module was organized into five phases and forwarded to experts (n = 11) for the evaluation of the content of the module.
Content Validation
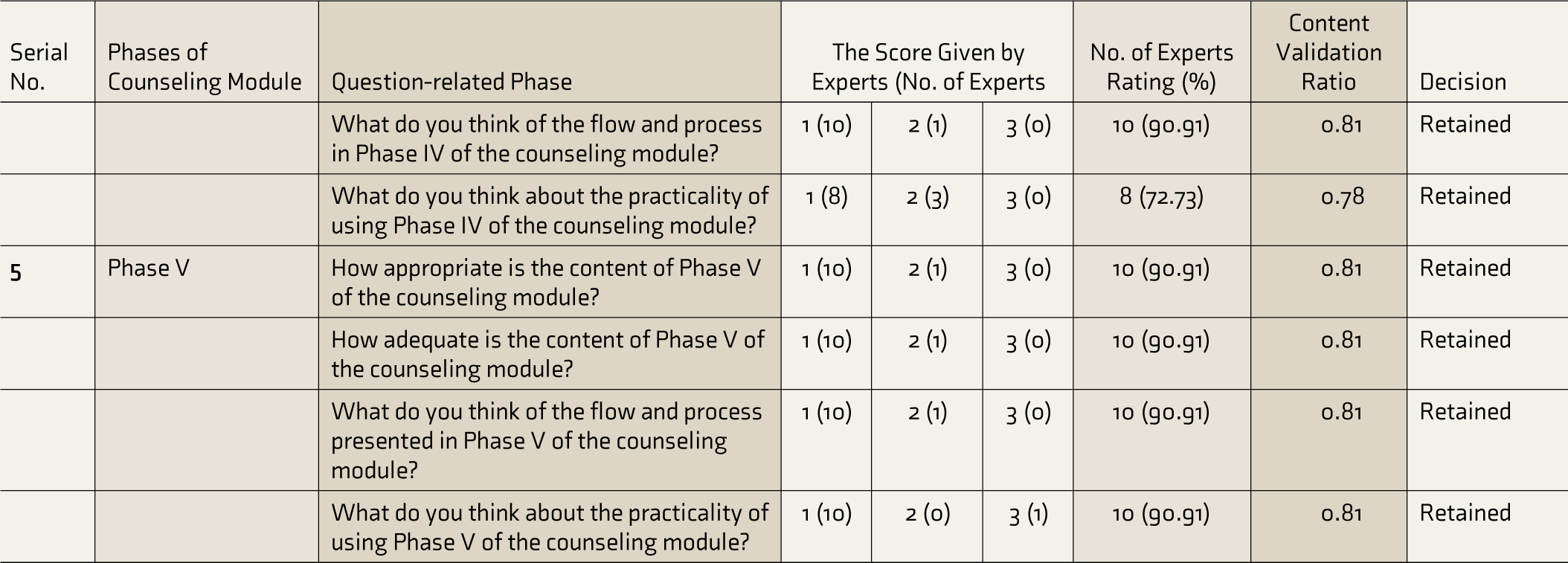
A panel of mental health experts conducted the content validation of the Ramayana-based counseling module (n = 11). The components of the Ramayana- based counseling technique module were assessed using the CVR, as proposed by C. H. Lawshe. 33 The CVR was calculated using the formula (Ne − N/2 divided by N/2), where Ne represents the number of panelists indicating “essential,” and N is the total number of panelists. The numeric values of the CVR were determined according to the Lawshe table. The scores for each phase obtained from experts and the calculated CVR are shown in Table 3.
Content Validity Ratio of Ramayana-based Counseling Module.
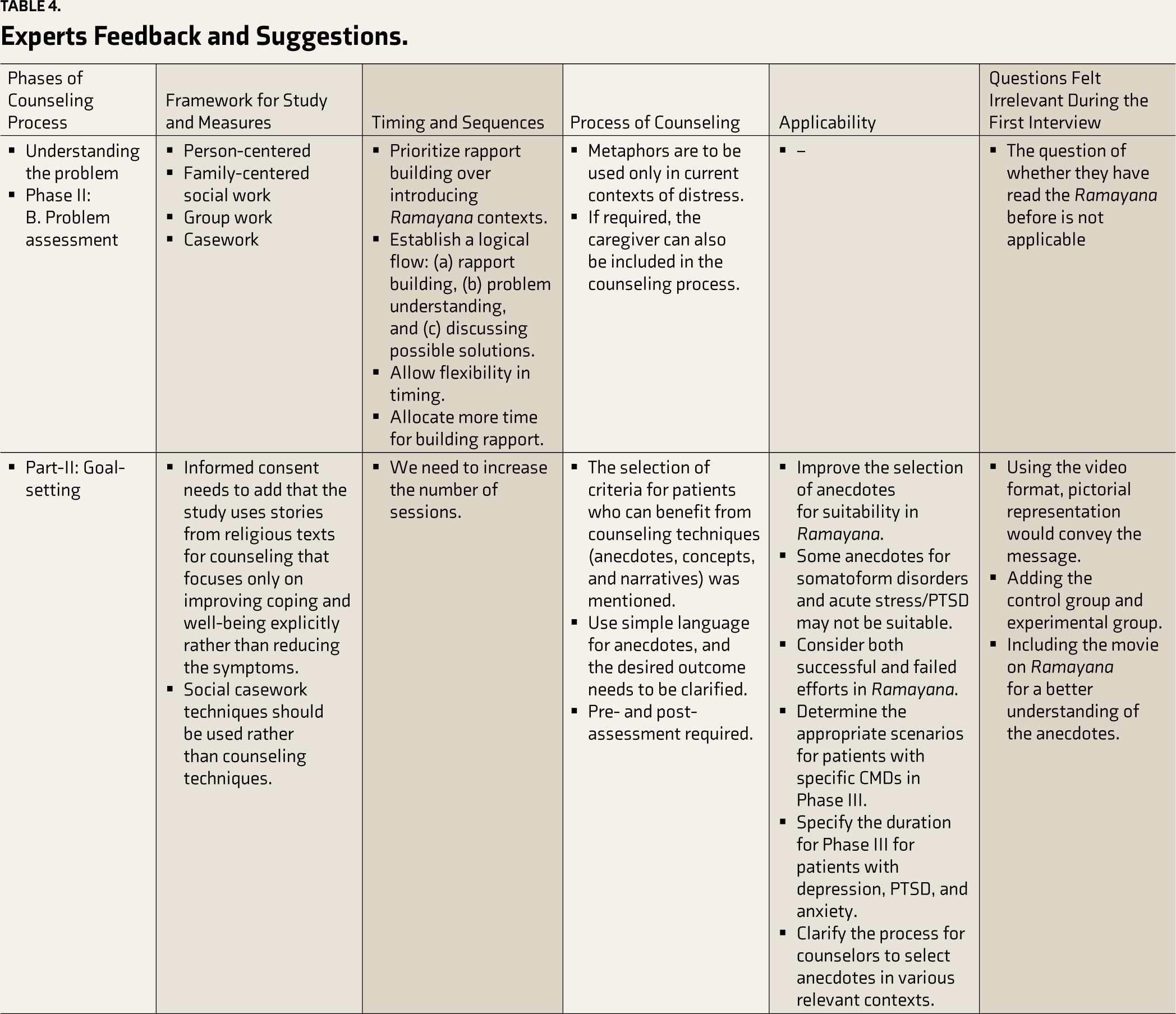
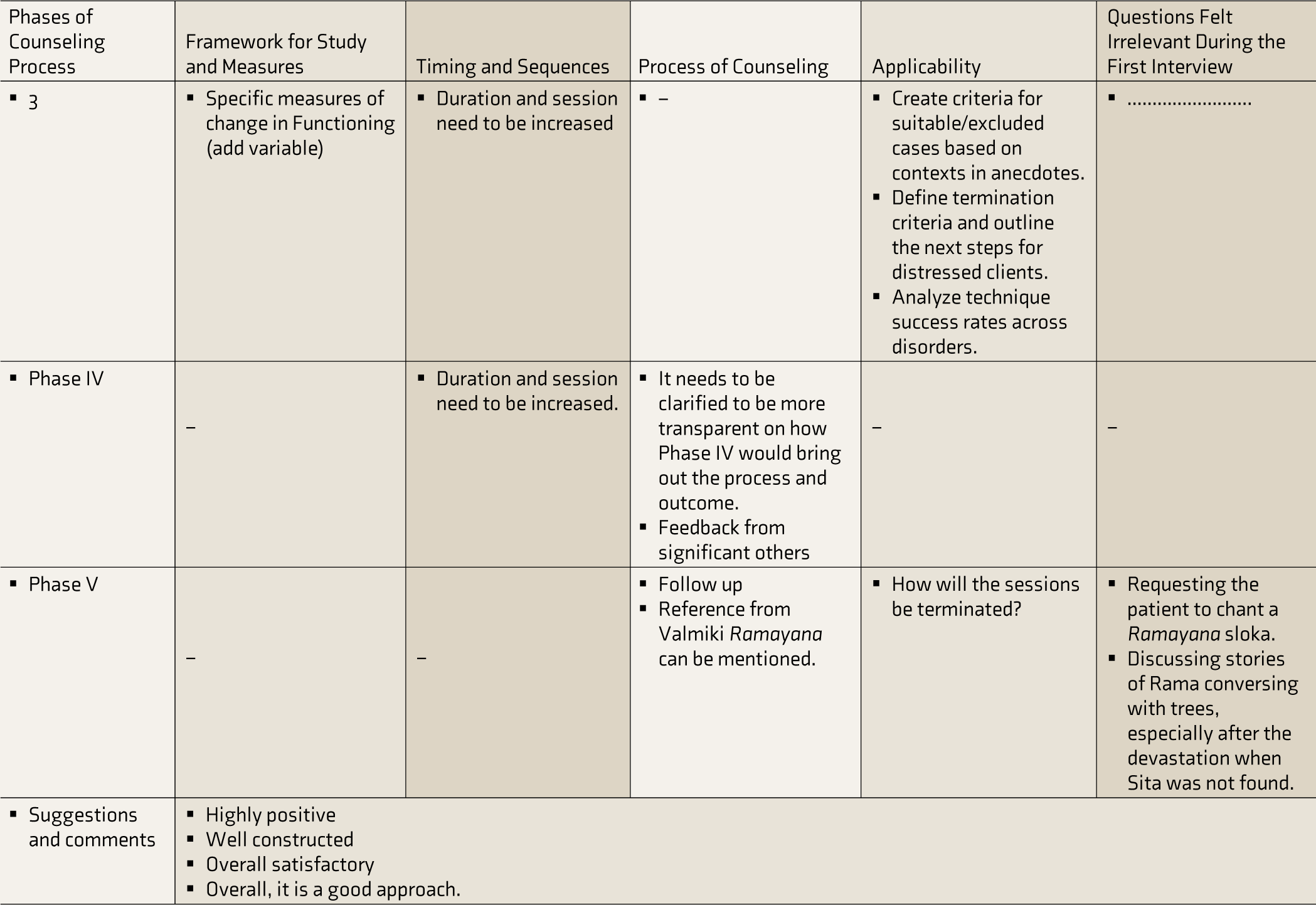
During validation, experts provided suggestions and comments in a tabular format, organized according to counseling phases. These inputs were carefully considered for incorporation into the module, and the comments provided by the experts are presented in Table 4. Relevant comments were integrated into the module, while irrelevant ones were excluded.
Experts Feedback and Suggestions.
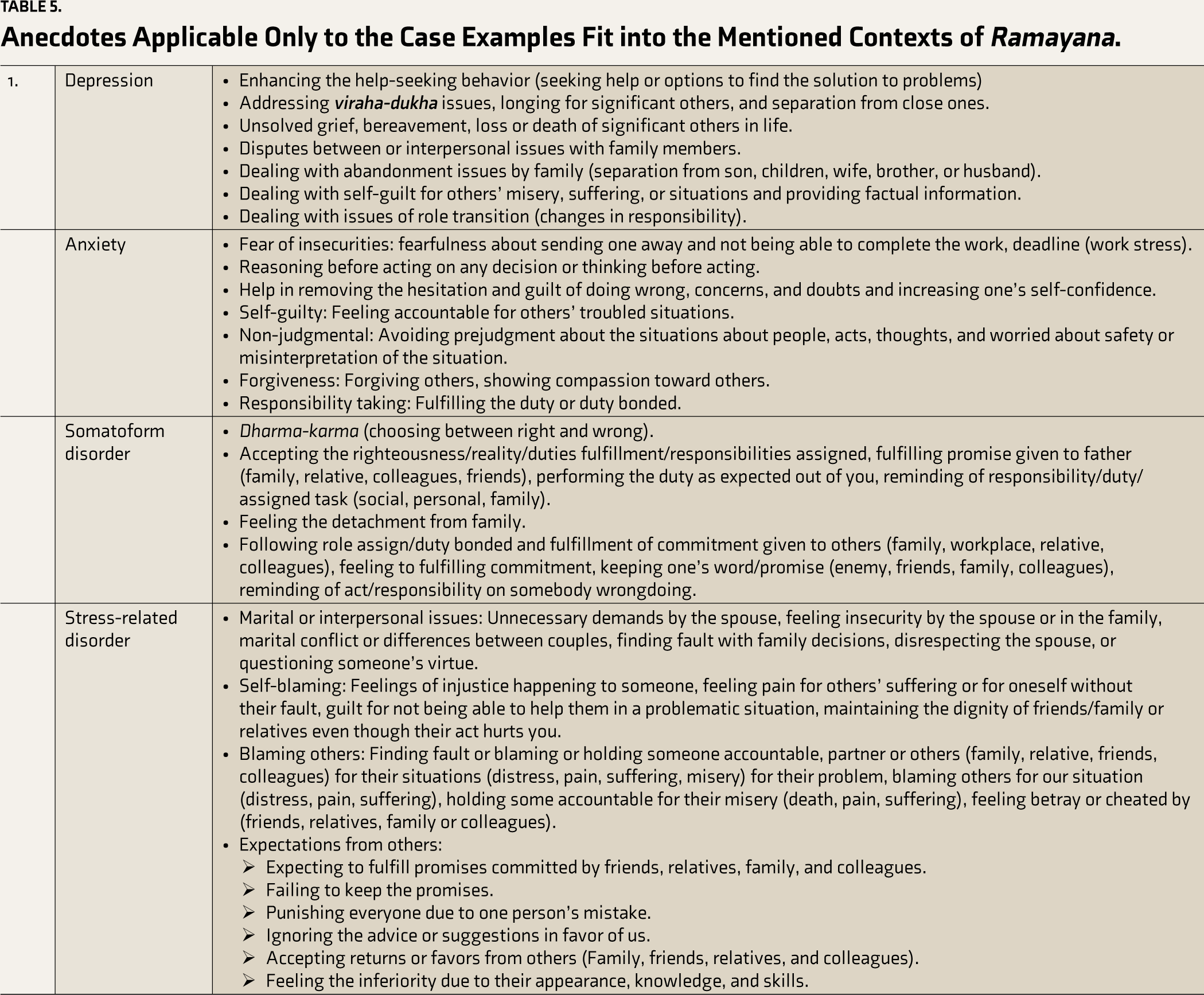
This module is organized to suit various everyday contexts based on ICD-10 diagnosis criteria for persons facing common mental health issues. The counseling techniques were specifically designed for the following diagnoses: F32.0 to F32.1—mild to moderate depression, F41 to F41.9—other anxiety disorders including panic disorder, generalized anxiety disorder, social phobias, mixed anxiety disorder, F45—somatoform disorder, F43—reaction to severe stress, F43.2—adjustment disorder–acute stress reaction, and F43.1—post-traumatic stress disorder. Table 5 shows the anecdotes applicable only to the case examples that fit into the mentioned everyday contexts of the Ramayana. The module will be available upon request from the author.
Anecdotes Applicable Only to the Case Examples Fit into the Mentioned Contexts of Ramayana.
Discussion
The present study focuses on developing and validating a comprehensive counseling module grounded in the Ramayana, intended for application in clinical settings for individuals experiencing common mental health issues. Sociocultural factors are essential in understanding and forming perceptions, attitudes, and behaviors in therapeutic engagement. Psychotherapeutic constructs originating in the West, such as integrity, autonomy, and confidentiality, are often associated with various standardized therapies such as CBT, EFT, schema therapy, and acceptance and commitment therapy. In contrast, sociocultural factors intrinsic to the Indian context, including belief systems such as karma (deeds) and dharma (duties) and faith in superstitions, rituals, and mythology, often lead individuals to seek the sources of their problems external to themselves. 18 While many Western psychotherapeutic approaches have demonstrated efficacy, their applicability to the sociocultural complexities of the Indian population remains limited.
Several studies have shed light on the challenges of standardized psychotherapy in cultural contexts,18,34-37 highlighting the differences between Indian philosophical constructs and traditional psychotherapy based on sociocultural factors. The cultural context in India, including factors such as a client’s dependency on the therapist, faith and religion, beliefs in rebirth and fatalism, social hierarchy, confidentiality, decision-making, and personal responsibility, significantly influences the implementation of Western psychotherapy principles. According to experts, an individual’s personality emerges as a significant determinant in the trajectory of mental health disorders and therapeutic outcomes. Consequently, it is critical to adapt psychological interventions in alignment with the unique social and cultural factors inherent to a given society and culture.9,25,38,39
In the context of our research, we developed a Ramayana-based counseling module by drawing upon its concepts, narratives, and anecdotes, collectively referred to as counseling techniques. This endeavor represents a pioneering effort in India, as no such module has been formulated before. This module can offer valuable support to healthcare professionals addressing mental health issues by enhancing their ability to educate individuals, resolve interpersonal conflicts, facilitate coping mechanisms, and promote overall well-being. Indian scriptures like the Ramayana serve as reservoirs of profound wisdom, effectively guiding individuals in managing negative emotions and fostering psychological resilience. To ensure cultural relevance, emphasis on cross-cultural adaptations is imperative, considering the disparities highlighted by various researchers when comparing Western psychotherapy with Indian cultural contexts. 5 Additionally, systematic reviews have illustrated the efficacy of religion-based interventions in addressing mental health concerns, particularly CMDs, when compared to standardized therapeutic approaches.40-42
Furthermore, the study’s strength lies in using a systematic methodology comprising five iterative analyses, as detailed in the methodology section. This rigorous process led to identifying 107 relevant anecdotes, with active collaboration between the researcher, primary guide, and co-guide. Several other studies have also employed similar qualitative methods to incorporate religious elements into interventions, such as using focus groups, 43 conducting in-depth interviews, relying on existing literature, 44 conducting narrative reviews, 45 employing CBT frameworks, 46 and using various survey methods, 47 including the examination of published literature and conducting narrative reviews of sacred texts. Additionally, one study employed a series of approaches, including focused group discussions, in-depth stakeholder interviews, and active patient engagement, as central components in their intervention development strategies. 48 These approaches have collectively played a significant role in shaping interventions during the module development process in other studies. Importantly, our study also aligns with the qualitative methods employed for module development, reflecting a perspective that advocates for a bottom-up methodology to establish a comprehensive theoretical and practical foundation for treatment strategies, thereby promoting a holistic understanding.
The development of the Ramayana- based counseling module represents a meticulously executed and multifaceted process. It combines various research methods and expert insights to ensure its robustness and clinical applicability. The in-depth interviews with mental health experts played a crucial role in conceptualizing the Ramayana-based counseling module. These interviews contributed to the module’s conceptualization and brought essential practical knowledge into its development. Multiple reviews of anecdotes and narratives have enhanced the clarity and relevance of the counseling techniques, making them more effective in clinical contexts. Furthermore, the qualitative analysis, conducted manually, enabled a comprehensive examination of numerous anecdotes, narratives, and concepts found in the Valmiki Ramayana.
One significant aspect of this module’s development lies in its alignment with diagnostic criteria for CMDs as per the ICD-10. This alignment enhances the clinical applicability of the module by tailoring interventions to address the specific challenges posed by each CMD category. The module addresses core components such as emotion regulation, grief issues, and intra-personal or interpersonal relations. The aim is to target these challenges through Ramayana-based counseling effectively. Overall, these symptoms are commonly presented in diagnoses such as depression, anxiety disorders, stress-related disorders, and somatoform disorders. Categorizing anecdotes based on these diagnostic criteria facilitates a targeted and practical approach. The involvement of experts in organizing and contextualizing situations, coupled with the meticulous refinement of the module, exemplifies the commitment to excellence in its development. The rigorous content validation process also serves as a testament to the module’s quality assurance. The systematic assessment of appropriateness, accuracy, and practicality, guided by expert feedback, further refines the module’s applicability in clinical settings. This comprehensive approach to development and validation demonstrates its readiness for practical application and emphasizes its significance in mental health counseling.
Across these diverse studies, the initial stages consistently emphasize rapport building and issue understanding, followed by phases involving problem formulation and therapeutic goal establishment. This uniformity underscores the structured progression prevalent in various intervention approaches.49-51 The delivery structure in Ramayana- based counseling entails a session count ranging from 10 to 15, depending on the patient’s specific objectives as suggested by experts during the validations. Each session is allocated a duration of 40–50 minutes and occurs weekly or biweekly. A consistent pattern was observed in various religious-based studies, consisting of 10–12 sessions per participant.44-46,50,51 Remarkably, these religious-based studies show no discernible timing, duration, goals, and expected outcome disparities. This study consistently applies the principles outlined in the literature to develop modules incorporating religious components for therapeutic benefits in managing mental health disorders.
This study describes the development of a socioculturally relevant Ramayana-based counseling technique module designed to assist individuals with CMDs in coping better and enhancing their well-being. The module addresses the psychosocial needs of individuals with CMDs, facilitating understanding and resolving interpersonal issues while promoting self-regulation. In the Indian context, the Ramayana-based counseling module may be more acceptable, appropriate, and contextualized within the client’s social-cultural milieu, potentially aiding in managing daily life difficulties more effectively.
Limitations
One limitation of this study is the lack of prior research or scientific data to establish a framework to guide the development of the module based on Indian scriptures. Consequently, we had to formulate our framework for developing and validating the module, relying solely on our expertise and inputs from several experts.
Conclusion
This study has outlined the comprehensive development and validation process of a Ramayana-based counseling technique with the potential to enhance mental healthcare for individuals with CMDs. However, further research and testing are crucial to evaluate the applicability and effectiveness of these techniques in addressing issues related to CMDs in clinical practice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval and Informed Consent
The Institute Ethics Committee (IEC) of the National Institute of Mental Health and Neurosciences reviewed and approved the study. Written informed consent was obtained from expert mental health professionals.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.