
Abstract
Background:
The social, economic, and physical environments are widely recognized as important determinants of health and affect the outcome of service delivery. The differences in the patient outcomes can be inferred upon by looking into the process and content of service delivery.
Methods:
This study is a mixed-methods, prospective cohort study to be conducted at two community extension clinics run by the Central Institute of Psychiatry, Ranchi, Jharkhand. Service users diagnosed with a common mental disorder (CMDs) will be recruited during the study period of three years. The main objective is to ascertain the unmet needs of patients with CMDs. The secondary goals involve measuring the clinical outcome through the lens of process-oriented recovery, service satisfaction, and accessibility, and analyzing the barriers to access healthcare services along with the impact on the carers. Focus group discussions with participants will help understand the reasons behind their unmet needs and factors essential in service delivery.
Discussion:
Healthcare, as well as social care, aims to deliver services according to need. In a country with 15 million people with CMDs, evaluation of needs could create a platform for the rational distribution of services.
Common Mental Disorders (CMDs) are a significant source of burden in the community. Understanding their unmet needs could be significant step in addressing them. The healthcare delivery systems should reorient their services to cater to these unmet needs and aid in the recovery.Key messages:
Common mental disorders (CMDs) are as a group, more prevalent in various medical care settings as well as in the community. Depression, anxiety disorders, somatoform, and neurotic disorders are commonly considered to represent this group. 1 CMDs, as well as their subthreshold symptoms, pose a substantial risk of functional disability and absence from work. 2 About 150 million Indians need care for mental disorders and 10% have CMDs as per the estimates of National Mental Health Survey (NMHS). 3 The resources available to manage the enormous burden of mental health disorders are insufficient, inequitably distributed, and are used inadequately, leading to a treatment gap of over 75%. 4
Central Institute of Psychiatry (CIP), a tertiary healthcare teaching Institute at Ranchi, Jharkhand, initiated the community extension clinic program to address this gap. The institute has been instrumental in rendering mental health services to communities at West Bokaro, Hazaribagh, Chandankiyari, the earliest being established at Mandar near Ranchi in 1967. At two of these clinics, a clinical psychologist visits a nearby school to address the mental health concerns of students.
The communities accessing care are identified by evaluating the demographic profile of the patients visiting the institute from the nearby areas of the state. A link is established with prominent structures in the community, which could be a school, local hospital, or any known establishment, to gain better access to the people within the community. The geographical locations that do not have a local psychiatrist or a district mental health program are preferred. A team of doctors consisting of trainee psychiatrists and psychologists, along with a consultant psychiatrist, visits the community clinic on designated days established within the community. Currently, consultation at the clinic is sought for various neuropsychiatric disorders. After a brief evaluation, medications are prescribed (if needed), which are procured by the patient from the nearest pharmacy. Brief psychological interventions are provided by the psychologist when indicated. Progress is reviewed during the visit in the next month, and patients are advised to consult the nearest health facility in the case of acute problems or emergency in between follow-ups. When the identified issues are severe or require extensive management, patients are requested to visit the institute. The clinic team regularly conducts awareness programs and workshops with teachers, parents, and patients to sensitize and raise awareness of various mental health problems.
Many factors determine the health of an individual within a community. Factors such as place of living, the state of the environment, income, education, relationships, in addition to access and use of health care services, are all crucial determinants of health. A “need” in health care is the capacity to benefit. Everybody has needs, including people with mental illness. 5 The latter have the same basic needs, such as a job, transportation to a health center, proper housing, as well as specific additional needs related to mental illness. “Need” in mental health care includes broader areas of health and social functioning than most other areas of medicine. Need is subjective and the person in need might view his or her needs quite differently from how the health service professional views it. Further, some of these needs might not be recognized by the professionals due to lack of knowledge and skills. These unmet needs are essential, important priorities for improvement in quality and efficient use of resources. Adding strategies to determinate and respond to the unmet needs in a meaningful way can enhance the care quality of healthcare provided.
Access and usage of health services within a community can be variable. There could be numerous barriers that cause delay in seeking help, such as instrumental barriers (e.g., lack of information about where to avail for help), monetary barriers, or attitudinal barriers (e.g., belief that the problem will get resolved itself, preferring to solve the problem by self). 6 These care-seeking barriers can additionally impact the outcome of the services provided. Social support networks consisting of kith and kin, and neighborhood are linked to better health. Therefore, it is vital to take into account the perspectives of carers involved in caregiving. A mixed-methods approach to assess the outcome of services obtained from multiple information sources can be effectual in light of multiple health determinants.
This article presents the protocol of a community project that aims to estimate the outcome of services provided at the extension clinics by looking into the needs (met and unmet), barriers in accessing services, client satisfaction, and caregiver burden. The authors are not aware of any Indian studies on needs assessment of CMDs, while a few do exist on patients with severe mental disorders (schizophrenia and bipolar disorder).7,8
Objectives
The study has four objectives.
Objective 1: To estimate the unmet needs of patients with CMDs visiting the CIP community extension clinics.
It is not known if the services provided at the clinics address unmet resource needs that contribute to clinical recovery. There could be a situation where such an intervention may, or may not, lead to a significant change in needs.
Objective 2: To estimate the barriers to care and satisfaction with the services at the community extension clinic.
Objective 3: To estimate the involvement of carers accompanying the patients at the community extension clinics.
Objective 4: To estimate the reasons behind the unmet needs of patients with CMDs and factors involved in service delivery.
The primary outcome measure is the estimation of the needs of patients with CMDs. The secondary outcomes are the parameters of service satisfaction, recovery, and accessibility.
Materials and Methods
Design
The study will follow a mixed-methods research design conducted for three years. It is a prospective cohort study conducted on patients with CMDs attending community extension clinics. The clinical outcome of patients with CMDs will be ascertained in the domains of needs, service satisfaction, and accessibility. The perspective of the carers concerning the needs of the patients and their involvement will also be obtained. In the end, the pattern of recovery of the patients receiving treatment from the clinic will be judged at six months. There will also be a focus group discussion (FGD) of six to eight patients along with their carers to understand the reasons behind the unmet needs and lack of satisfaction with the services provided at the clinic.
Ethics
Ethical approval has been obtained from the Institute Ethics Committee, CIP.
Study Setting
The proposed plan will be conducted at the two community extension clinics run by the Institute. The General Psychiatry Clinic at West Bokaro is located 160 km away from the Institute in the Ramgarh district of Jharkhand. It is a suburban setting, and the services are provided within the Tata Central Hospital, West Bokaro. The hospital caters to the population working in the mines in a radius of 40 km in and around West Bokaro. The hospital does not have specialized mental health services, and the medical officers’ screen and the patients needing specialized services are referred to the community clinic. The community team visits the clinic on the fourth Tuesday of every month. The local St. Xavier’s School has provided its premises for another community clinic on the first Wednesday of every month. The second clinic, situated in the Hazaribagh district, is 200 km away from the Institute and is staffed by the student volunteers who manage the case record files and patient queues. The service users are ethnically heterogeneous, with a sizeable representation of tribal populations from the nearby villages.
Sample
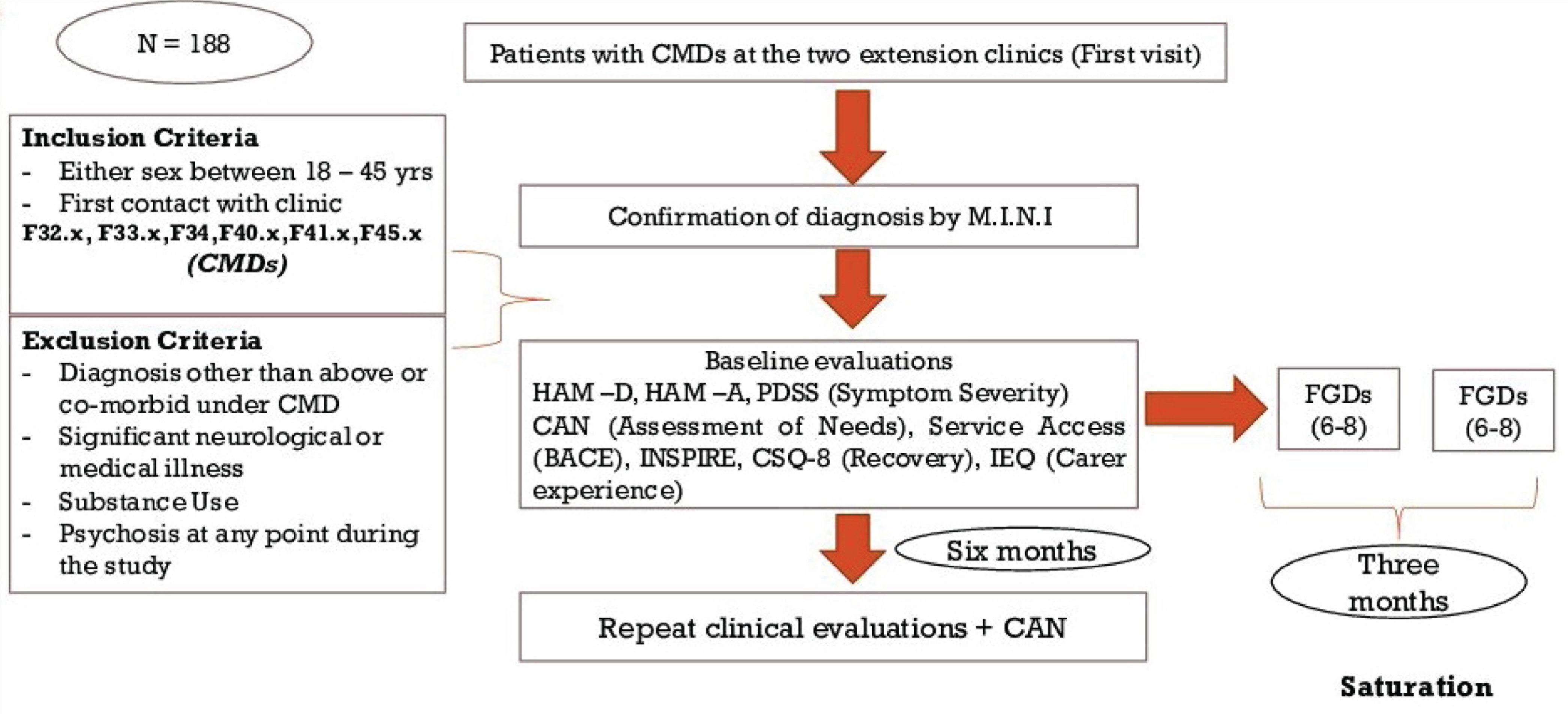
The eligible participants for the quantitative study will be those patients at the community extension clinics receiving any of the diagnoses from ICD-10 belonging to the group of CMDs (F32.x, F33.x, F34, F40.x, F41.x, F45.x) of either sex between 19 and 50 years. Those with a diagnosis other than under the inclusion criteria or co-morbid under CMDs, documented psychosis at any point of time during the study period, substance use in harmful/dependence pattern, significant neurological, or medical illness will not be included. After their first completed visit, the consenting participants recruited based on their age distribution or gender would be selected from the same community extension clinic to create a group of six to eight people for the FGD.
Sample Size
NMHS reported the prevalence of CMDs to be 10%. Using a sample size calculator, with a confidence interval of 95%, precision (d) as 0.05 without a finite population correction, and prevalence as 10%, the sample size was estimated to be 139. The dropout rates in the outpatient psychiatric services vary considerably but can be averaged around 35%. 9 Thus, the total sample size would be 188.
Recruitment
The treating team would be encouraged to refer the patients with any of the diagnoses belonging to CMDs, to the research staff stationed at the clinic. The patients would be screened for eligibility and recruited into the study after obtaining their written informed consent. The individual would continue to receive the usual care provided at the clinics while being in regular contact with the research team. The baseline assessment measures can take up to 90 minutes, so if necessary, it will be completed in two face-to-face meetings with the researchers. The assessments could either be completed at the community clinic or at the service user’s own home, at the time agreed. Since the recruitment would be done simultaneously from both the extension clinics, an attempt would be made to ensure balance in selection to allow for adequate representation of males and females. Any information about the clinical data from the research team could be obtained only with the prior consent of the patient.
Assessments
The clinical assessments will be done by an independent research team not involved in deciding the treatment strategy for the patients and their carers. The interventions would continue to be carried out as per the decision of the treating team at the clinical ethics consultations. The research team will have no role in the choice of intervention decided by the treating team.
Diagnostic assessment: The diagnosis will be ascertained using the Hindi version of the Mini International Neuropsychiatric Interview (M.I.N.I v5.0) 10 for ICD-10. Information will be corroborated from the relatives and available medical records, following which the diagnosis will be established for CMDs, according to ICD-10.
Generic assessment
Sociodemographic form: A sociodemographic sheet specifically developed by ICMR would be used for the study that records the information regarding patient’s age, gender, marital status, occupation, socioeconomic condition, details of family, duration of illness, and ongoing treatment. The team characteristics form (TC-F): This form will record the team’s key characteristics, such as number of cases seen, team composition, and support offered along with changes in any of these characteristics within the last six months.
Researcher-rated measures of symptom severity
Hamilton Depression Rating Scale (HDRS)
11
: It is widely used to assess depression, and a score of 11 on HDRS is indicative of a diagnosis of depression. Hamilton Anxiety Scale (HAM-A)
12
: This 14-item severity rating scale would be used for quantifying the symptoms of anxiety. Somatic Symptom Rating Scale: Given by DSM-5, it aids in assessment of somatic symptoms. With a score range of 0–30, higher scores indicate greater severity of somatic symptoms. Panic Disorder Severity Scale (PDSS)
13
: It is a brief 7-item clinician-rated scale to assess overall panic disorder severity with higher ratings indicating greater symptom severity.
Service User-Rated Outcome Assessments
The assessments of needs would be done using the scale of Camberwell Assessment of Needs-Research (CAN-R).
14
The CAN is an interviewer-administrated instrument for a comprehensive assessment of 22 different health and social needs of patients with severe and enduring mental illness. Given the lack of any validated tools for CMDs, this tool is being used for the population under study. However, since the domains related to “alcohol,” “psychotic symptoms” are not applicable in the current context, the patients were not assessed on these domains. CAN-R also asks the interviewee about the appropriateness of the current intervention and the satisfaction with the amount of help received. The “need” in CAN-R is stated in terms of unmet needs (current serious problems, whether or not help is offered or given) and met needs (no or moderate problems due to help given). The total number of met needs and unmet needs would give the information about the total number of needs. By aggregating the information obtained from individual patients, the estimated met needs, unmet needs, and total needs at the community level can be obtained in terms of absolute number as well as percentages. Client Satisfaction Questionnaire (CSQ-8)
15
: The 8-item scale measures the satisfaction of clients with services having a score range of 8–32 with high scores indicating greater satisfaction. Barriers to access to care evaluation (BACE v3)
16
: It appraises the barriers to access to mental health care. The user identifies problems that have ever stopped or delayed or discouraged them from getting or continuing to get professional care for the mental problem. The Involvement Evaluation Questionnaire (IEQ)
17
: This 33-item self-report tool measures the levels of burden and distress among caregivers of people with mental illness.
Process measures
The Importance of Services in Recovery (INSPIRE)
18
is a service user-rated measure of recovery. The full version has 27 items with two sections dealing with support (20 items) and relationship (7 items). The support section identifies the level of support received from the mental health professional for their recovery whereas the relationship section determines the relationship between the service user and the mental health professional.
We will use the existing Hindi translations of the tools available for symptom severity, outcome, and process measures. If the translation is required, then after the initial translation into Hindi, a bilingual researcher will back-translate the measures into English for comparison with the original.
Schedule of Evaluations
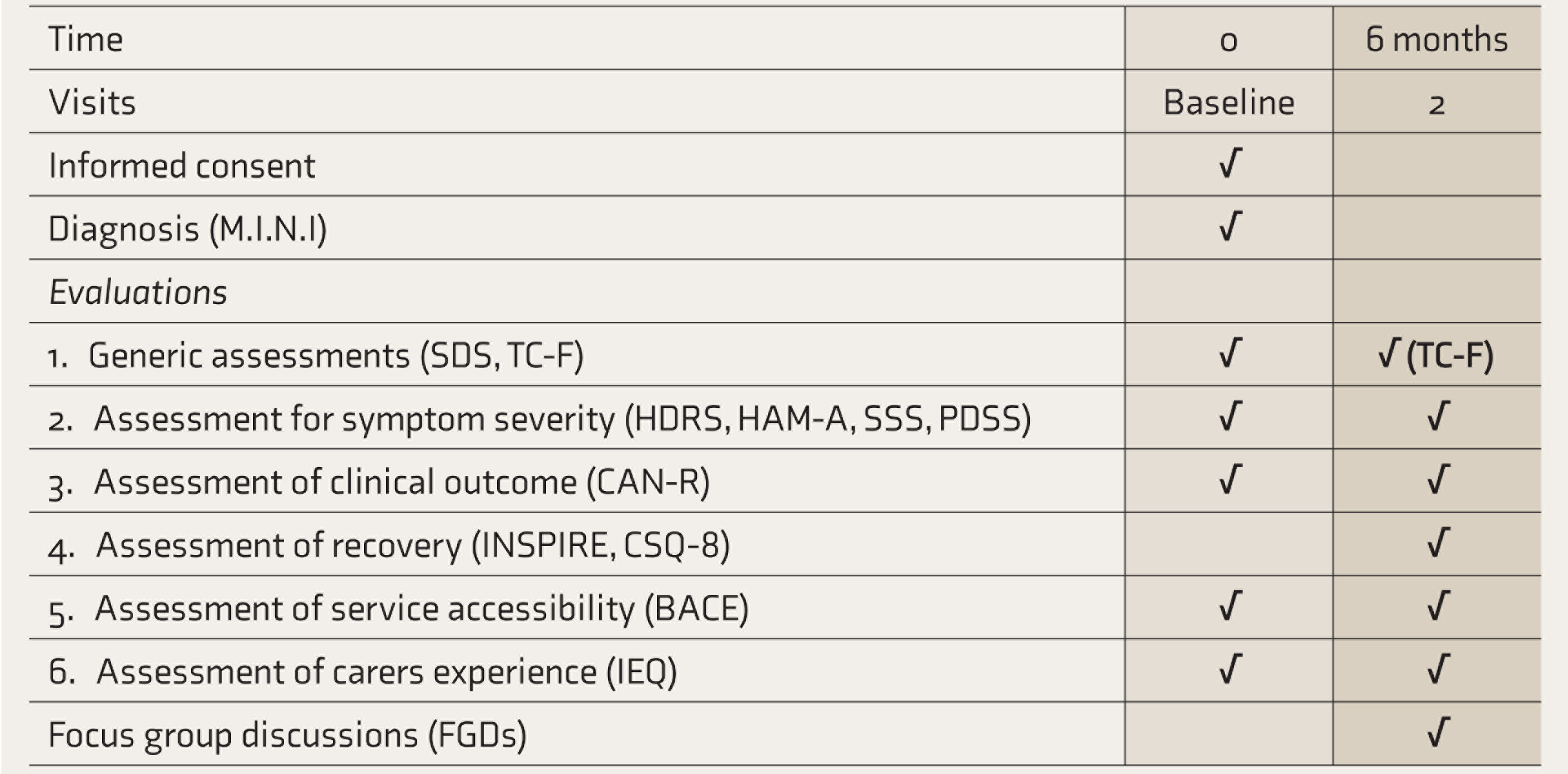
Note: TC-F: Team characteristics form.
Flow Diagram of Participant Recruitment
Procedure
The patients visiting the extension clinics will be explained about the study and asked about their willingness to participate in the study. If willing to participate, they are asked to sign a consent form. They would then complete the baseline interview comprising of symptom severity scales (HDRS, HAM-A, SSS, PDSS), CAN-R, INSPIRE, CSQ-8, BACE, and IEQ. If necessary, the baseline assessments could be spread over more than one meeting. Following baseline assessment, the service user would continue to receive the care as usual provided by the team visiting the community extension clinics. Six months after baseline data collection, the follow-up assessment will be conducted by the research worker with all the previous clinical measures. The research team member will also fill the TC-F at baseline and again at the end of six months from the first visit to the clinic. If the service user is no longer in contact with the team, efforts will still be made to contact them for a follow-up assessment through home visits or telephonic calls. After six months, the participants will be paid ₹300 for taking part in the study. A summary of the assessment measures is shown in Table 1.
In addition to the baseline and follow-up data collected, FGDs will be conducted.
FGDs: It has been seen that patients do not report needs that have not been asked. The CAN is primarily aimed at screening for met/unmet needs rather than describing in detail. These shortcomings can be overcome in FGDs. The group discussion could discern needs that have not been asked for in CAN as well as recognize the unmet needs and the likely reasons in context, depth, and detail. Additionally, the discourse aids in knowing how the needs are met while others remain unmet.
With this aim, a FGD of six to eight consenting patients purposively stratified based on age and gender will be conducted at a convenient venue within two to three months of recruitment into the study. A discussion guide will be developed for the interviewer that will have the instructions and questions related to met needs, unmet needs, stories behind the met/unmet needs, and the lack of satisfaction with the services. Every FGD would be carried out by a facilitator team comprising of two to three research members to help with asking questions and recording the discussion, including the non-verbal responses. The FGDs organized at each of the community extension clinics would be repeated every three months until theoretical saturation is obtained.
Data Analysis Plan (Quantitative and Qualitative)
The sociodemographic and clinical data obtained from the study participants will be entered into custom datasheets. All participants will be assigned a code for identification, and codes assigning files will be stored in separate places. Data will be entered in password-protected computers into password-protected databases. Data entry will be double-checked for mismatches monthly and at the end of all visits. The data will be checked for completeness and accuracy. The primary analyses will deal with identifying the total unmet needs of patients with CMDs as absolute number in terms of means as well as in percentages. This would be followed by an assessment of change in symptom severity, needs, and barriers to care at six months from baseline. The frequency analysis would be used to quantify the level of recovery and patient satisfaction from the services at the end of treatment. Regression analysis would be done to assess the potential effects of demographic or clinical covariates. For the measures that evaluated repeatedly, repeated measures mixed effect model would be used. The statistical significance would be considered as two-tailed P < 0.05.
All the group discussions would be audio-recorded and transcribed verbatim. Those carried out in Hindi will be first transcribed verbatim and then translated into English. A framework analytical approach would be used. The team will read, interpret, and identify themes and subthemes from data to develop a codebook. To ensure coding reliability, two team members will independently code all the interview transcripts. The disagreements (if any) will be resolved through consensus. After coding, thematic and content analysis will be conducted. NVIVO would be used to organize, analyze, and summarize common themes across types of participants.
Since the two settings of the community clinics could differ in terms of access and provision of health care, the participants in both the clinics would also be compared to look for the differences in their needs, barriers, and satisfaction with service delivery.
Discussion
The needs approach is considered to be one of the principal approaches to outcome assessment in mental health service evaluation. 19 The goal of the assessment would then be to inform the development of programs that determine where there may be “room for improvement” by addressing the needs and to identify specific needs for quality improvement. Patients who indicate that they would like help with any of the listed needs can inform their physician, who can refer them to a social worker and discuss their needs more fully. Help with local community services to meet needs considering factors such as eligibility, desirability, and accessibility can then be offered. The social worker could be desked at the clinic, and the patients could talk in person, or by telephone or during follow-up visits. Needs could be closed as successful when they met a set criterion or if the patient indicated that he or she has all the information needed and does not want further assistance. The World Health Organization has recommended reallocation of treatment resources to decrease the unmet treatment needs for mental disorders substantially. 20 But these needs are infinite, and resources for the health system are finite. A fundamental principle underlying community-based mental health care is that care and services should be proportional to the comprehensive and changing needs of individuals. 21 Recognizing the unmet needs could assist in the rational use of resources and help effectively improve the population’s health. So, health needs assessment could be an effective method of promoting fairness in service delivery and addressing inequalities in health. 22 In the long run, it would help develop policy decisions, interagency collaboration, and address development priorities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This protocol paper describes the methodology of a research project funded under ‘Capacity Building Task Force for Mental Health Research in India’ funded by the Indian Council of Medical Research vide file number 5/4-4/151/M/2017/NCD-1. International mentors were funded by the training program ‘Cross Fertilized Research Training for New Investigators in India and Egypt’ funded by FIC, NIH (No. D43 TW009114).