
Abstract
Background:
Alcohol use disorder is a serious health problem with high comorbidities. Early-onset alcohol use has been associated with greater impulsivity, increased severity of dependence, frequent alcohol withdrawal complications, externalizing symptoms, and antisocial behaviors. We aimed to evaluate the psychiatric comorbidities and severity of addiction in early- and late-onset alcohol dependence.
Methods:
This was a cross-sectional study. All patients fulfilling the diagnostic criteria of alcohol dependence as per International Classification of Diseases (10th edition) were included in it. Semi-Structured Assessment for Genetics of Alcoholism IV was applied to find the age of onset of dependence as per the lifetime frame and also to find comorbidities. Composite International Diagnostic Interview 3.0. was used to find other comorbidities. The severity of addiction was evaluated with Addiction Severity Index, 5th edition. All the sociodemographic and clinical parameters were compared between patients with the early- and late-onset alcohol dependence.
Results:
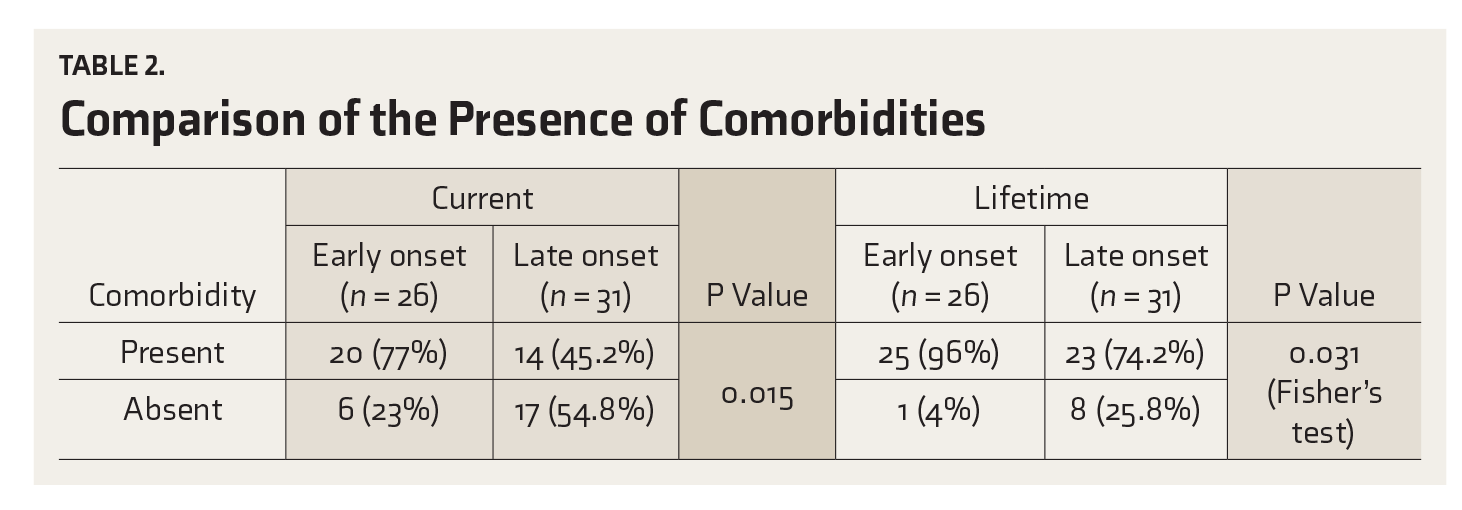
Out of the 112 patients screened, 57 met the selection criteria, 26 were with early-onset and 31 with late-onset alcohol dependence. The patients were all males. The patients with early-onset alcohol dependence had a higher family history (P = 0.006) and were nonearning (P = 0.002) in comparison to the group with late-onset dependence. The comorbidity among all patients was 59.6% and 84.2% in current and lifetime frames, respectively. It was significantly higher in the early-onset group, both for current (P = 0.015) and lifetime (P = 0.031) frames. On the domains of Addiction Severity Index 5th edition, the early-onset group had a more severe profile of addiction in all domains except the medical domain.
Conclusion:
Comorbidity is high among patients with alcohol dependence and is even higher for the early-onset group. The family history was higher in the early-onset group and they have more severe profile of substance use.
Keywords
Early-onset alcohol dependence is associated with higher family history of alcohol use. Early-onset alcohol dependence has higher psychiatric co-morbidities in comparison to late-onset alcohol dependence. Earlier the onset of alcohol use higher the severity of dependenceKey Messages:
In India, the country of our study, the total (recorded and unrecorded) per capita consumption of alcohol (in liters of pure alcohol) has increased to 4.3 (2008–2010) from 3.6 (2003–2005). 1 The largest epidemiological survey for psychiatric disorders in India had been carried out in the year 2015–2016 and the report of this National Mental Health Survey shows a prevalence of 4.65% of AUDs, which is the third most common mental disorder after tobacco use disorder and depressive disorder. 3
Higher rates of psychiatric comorbidities associated with AUDs are a matter of serious concern. The major epidemiological studies (Epidemiological Catchment Area Study, National Comorbidity Survey, and National Epidemiologic Survey on Alcohol and Related Conditions) done globally and other prevalence studies of comorbidity of AUDs done in India show a high occurrence of comorbidity. 4 Mood disorders (specifically depression), personality disorders, and anxiety disorders are common psychiatric comorbidities associated with AUDs. While a single disorder can affect the functioning of an individual, comorbidity can have an interactive and overwhelming effect. 5 This has its own diagnostic and therapeutic implications.
A typology of alcohol use is being tried from long back, dating to the 1980s. Various researchers used the “age of onset” as a classification point. Buydens-Branchy et al (1989) used it for the first time for classifying alcoholism. 6 Since then, numerous studies have been carried out for establishing this classification. Results have shown that those with EO alcoholism have more complications, more history of parental alcoholism, and a higher incidence of comorbidities. 7 An Indian study reported that adolescent-onset AUDs are increasingly associated with urban domicile, poor standard of living, and the Christian religion. This study also reported the association of adolescent-onset AUDs with psychological distress, increased vulnerability to alcohol dependence, alcohol-related injuries, and more hazardous patterns of alcohol use during adulthood. 8
This typology helps in convenient classification of the entity and early intervention. The major disadvantage of this classification lies with the elicitation of the “age of onset,” as there has been no standard definition. Various researchers have adopted different definitions of “age of onset,” such as the age at which the problem of drinking first started; the age at which alcohol was first taken, not counting sips; the age at which regular drinking started first; the age at which the heaviest drinking started; and the age at which the diagnosis of dependence was first fulfilled.9–11 It was then revealed that these various ages of onsets represent a trajectory of behaviors and that none holds more importance than the others. 12 Nevertheless, while conducting research, the “age of onset” is mostly taken by researchers as the age of onset of dependence because of its reliability, objectivity, and wide acceptability. 9 The age cut-off has been taken as 20–25 years in various studies.9–11 The age of 25 years has replicated findings, validating the typology of “age of onset” in studies conducted worldwide 13 and those conducted in India.9,10 Thus, among the various operational definitions taken, the most clinically relevant is the age at which dependence could be diagnosed for the first time with a demarcating age cut-off of 25 years.
In recent years, it has been observed in India that the age at which alcohol has been first used has declined from the age of 28 years (reported in the 1980s) to 17 years (reported in 2007). 14 In a study conducted in Kerala, the drinking population in the age group of <21 years has risen from 2% to 14% in the last 15 years. 15 If using a simple variable like “age of onset” can help in delineating subgroups that may differ in response to the treatment and long-term outcome, further studies in this field in the Indian scenario would be surely promising, taking into account the drop in the age of first alcohol use in the recent trends.
A comparison of comorbidities between EO and LO alcoholism is not available in Indian studies. The severity of addiction measured through an objective scale like Addiction Severity Index 5th edition (ASI-5), and that too comparing all domains, is also not available in the Indian scenario.
This is a part of a larger unpublished exploratory study that aimed to evaluate the psychiatric comorbidities, the severity of the addiction, externalizing psychopathology, and cognitive performance in patients with EO and LO alcohol dependence attending a tertiary-care teaching hospital of North India. In the current article, we are presenting the data (after doing secondary analysis) that focused on the psychiatric comorbidities and severity of addiction in patients of EO and LO alcohol dependence.
Materials and Methods
Study Design and Setting
This is a cross-sectional study conducted from October 2016 to July 2017 on patients visiting our outpatient de-addiction clinic. The sample consisted of all adult patients fulfilling the diagnostic criteria of alcohol dependence (active dependence) as per the International Classification of Diseases, 10th edition and Diagnostic Criteria for Research. 16
Inclusion and Exclusion Criteria
Patients willing to give written informed consent, and accompanied by relatives who could corroborate the history provided by the patient, were included in the study. Subjects with serious medical comorbidities or too ill to cooperate for the interview were excluded. Other exclusion criteria were age <18 or >60 years and years of formal education <8 years, as another part of the study assessed cognitive performance. Patients in severe intoxication or severe withdrawal were followed-up and made part of the study once the conditions stabilized. Patients abstinent from alcohol for the last one month were also excluded.
Assessment Tools
The patients were assessed with a semi-structured pro forma for sociodemographic and clinical details, details of substance use (onset, course, duration, pattern, and other relevant details), past history, family history, personal history, pre-morbid personality, and mental status examination. International Classification of Diseases, 10th edition, and Diagnostic Criteria for Research were used to make the diagnosis, Semi-Structured Assessment for the Genetics of Alcoholism-IV version (SSAGA-IV) 17 was used to find the comorbidity and also the age of onset by its lifetime interview section. Composite International Diagnostic Interview (CIDI) 3.0 18 was used to assess the comorbidities not present in SSAGA-IV, and ASI-5 19 was applied to find the severity of addiction in various domains.
Procedure
Ethical clearance for the study was obtained from the Institutional Ethics Committee. Patients attending the de-addiction clinic and fulfilling the selection criteria were made part of the study. Written informed consents were taken from the patients. After obtaining sociodemographic details in a semi-structured pro forma, SSAGA-IV was applied to get a detailed history of substance abuse, including the age at which the patient first fulfilled the diagnosis of alcohol dependence in the lifetime section of the diagnostic interview. A reliable informant, which included any of the parents or an older sibling, had to be present during the interview with the patient so that the age could be confirmed to avoid any false reporting and to give details of childhood behavior. For the study, “age of onset” was operationally defined as “the age at which the patient first fulfilled the diagnosis of alcohol dependence (as per self-report and cross-checking from the available attendant in the lifetime interview schedule of SSAGA-IV).” SSAGA-IV was used to assess the common comorbid psychiatric disorders associated with it through its diagnostic interview. (It includes the disorders occurring with greater frequency in those with alcoholism.)
CIDI 3.0 screener was applied, and specific modules of CIDI 3.0 were applied to diagnose any other comorbidity not present in SSAGA-IV and which was apparent in the clinical interview. ASI-5 was applied to find out the severity in different domains, both through patient and interviewer severity ratings and also to calculate the composite score.
The patients were divided into two groups as EO alcohol dependence and LO alcohol dependence on the basis of the age of onset of dependence in SSAGA-IV. The age of 25 years was taken as a cut-off to divide the above two groups. The two groups were then compared on sociodemographic profiles, presence of comorbidities, various clinical parameters, and the severity of the addiction. The data were then analyzed using appropriate statistical tests or using Statistical Package for the Social Sciences (SPSS) version 16.20 For categorical variables such as sociodemographic details, chi-square test or Fischer’s test were used. For comparing means, Mann–Whitney U test was applied as the distribution of the data was not normal.
Results
Sociodemographic and Clinical Variables
A total of 112 patients were screened, out of which 21 were excluded. The various reasons for exclusion were age <18 years (n = 1), age >60 years (n = 2), refusal to give consent (n = 1), years of formal education <8 years (n = 9), presence of serious comorbid medical illness (n = 3), and not being accompanied by a relative who could provide correct history of the patient (n = 5). Out of the 91 patients included in the study, 34 did not turn up for the cognitive assessment (which was part of the larger study). So, 57 patients finally formed the study population, out of which 26 belonged to the EO group and 31 to the LO group.
Sociodemographic and Clinical Profile of the Patients
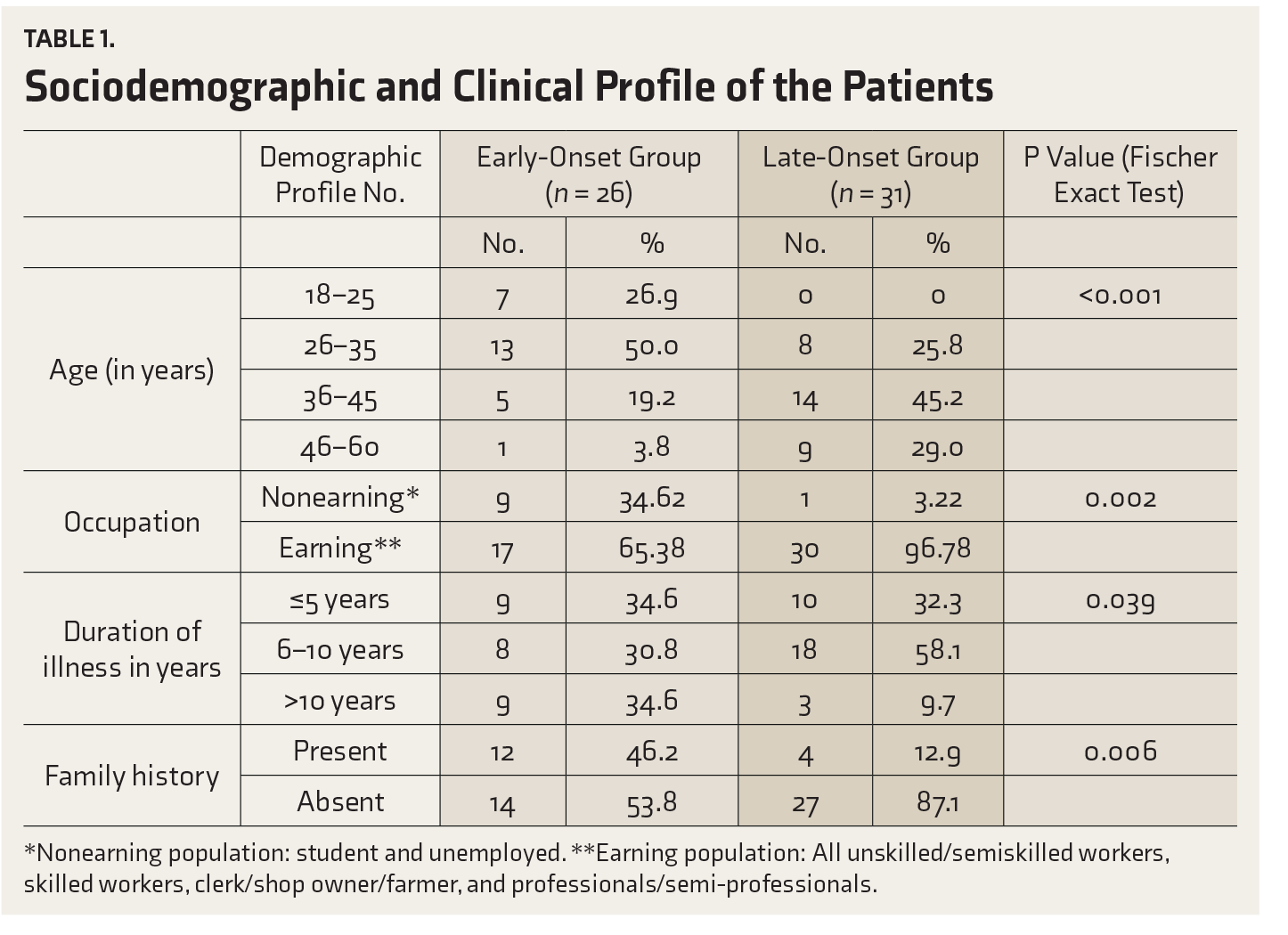
*Nonearning population: student and unemployed.
**Earning population: All unskilled/semiskilled workers, skilled workers, clerk/shop owner/farmer, and professionals/semi-professionals.
Comorbidities
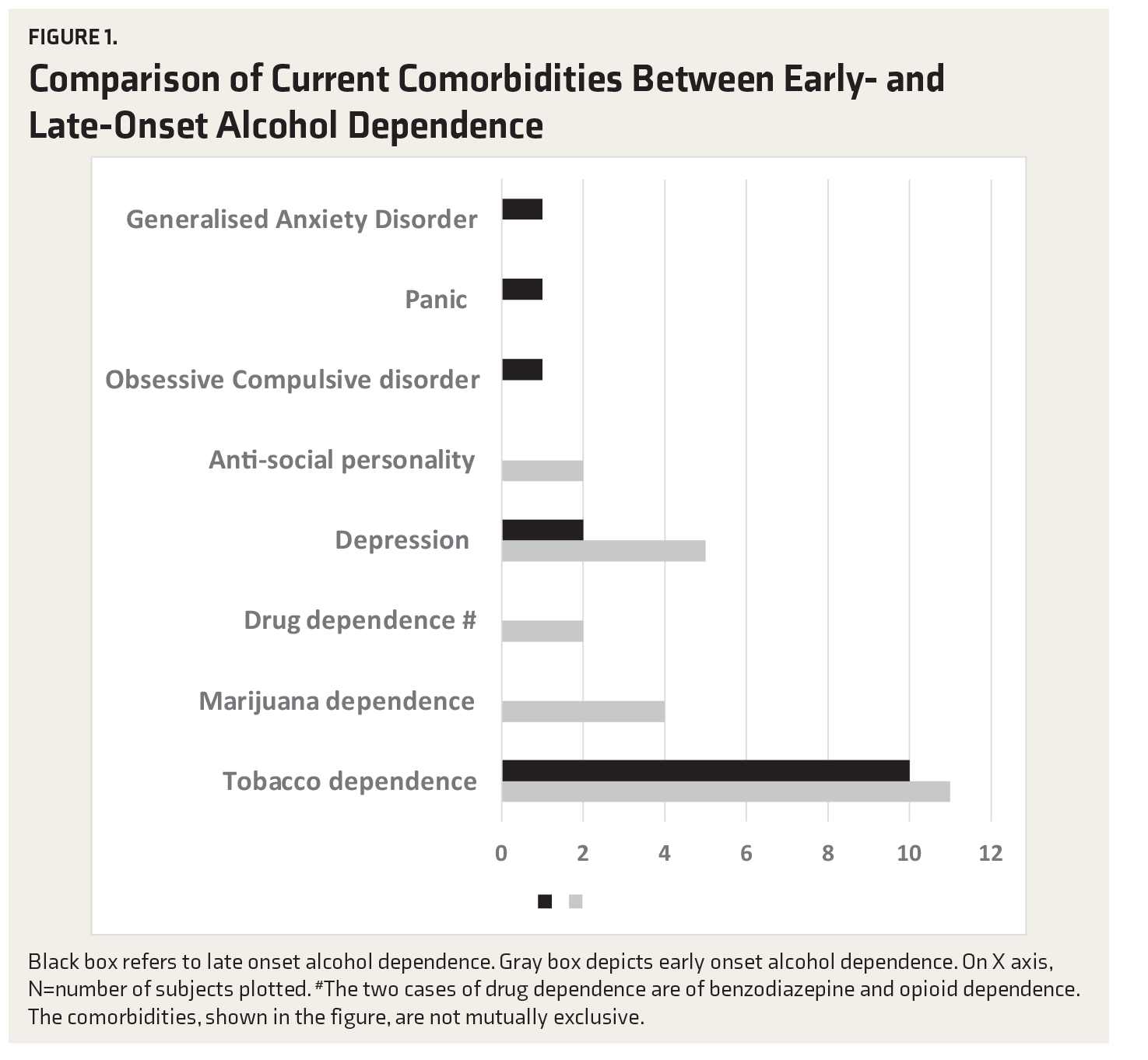
Comparison of Current Comorbidities Between Early- and Late-Onset Alcohol Dependence
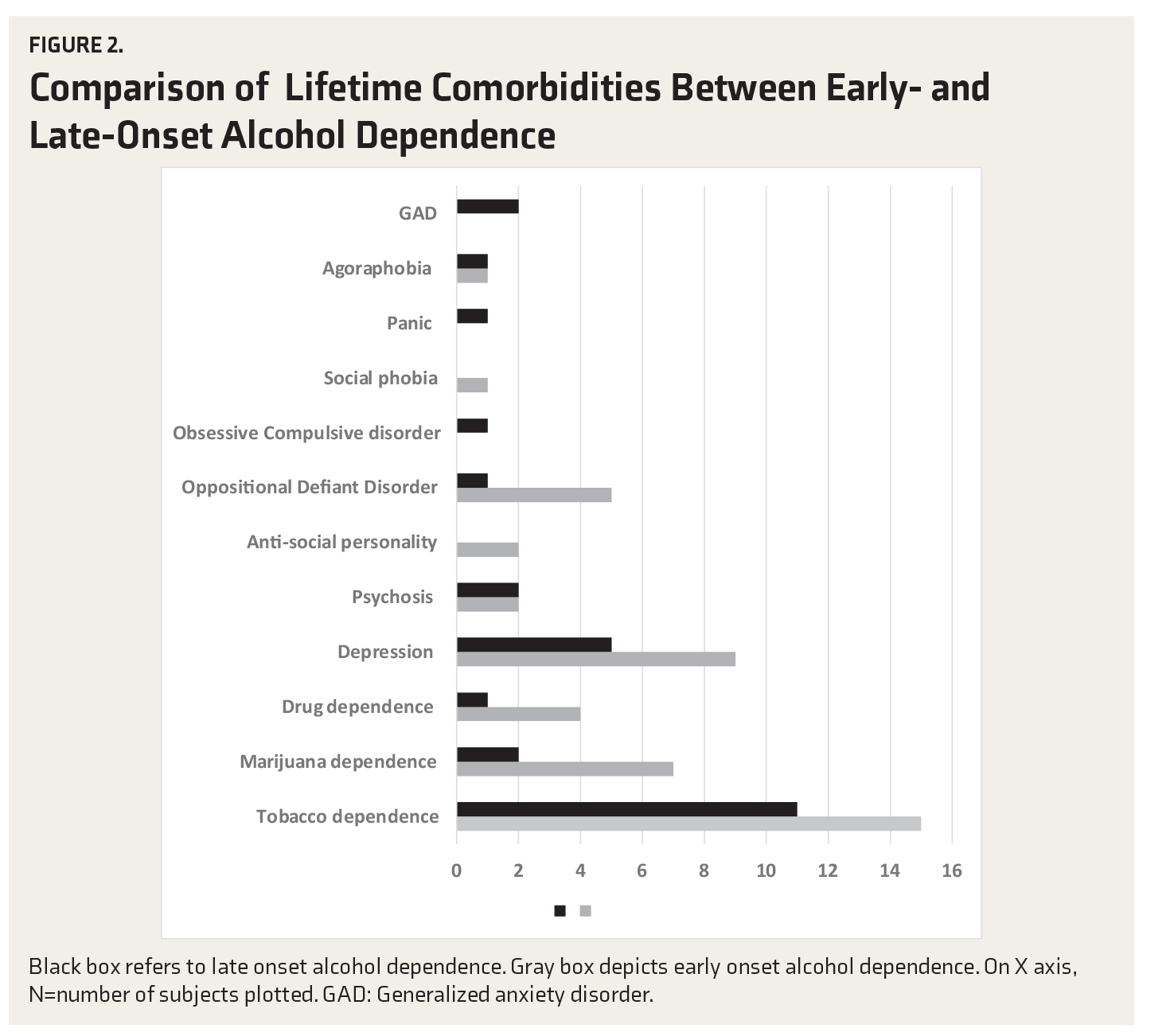
Comparison of Lifetime Comorbidities Between Early- and Late-Onset Alcohol Dependence
Comparison of the Presence of Comorbidities
Severity of Addiction
Comparison of Mean Scores, Median, and Interquartile Range (IQR) of ASI Domains—Interviewer Severity Rating and Composite Severity Rating Scores Between the Two Groups
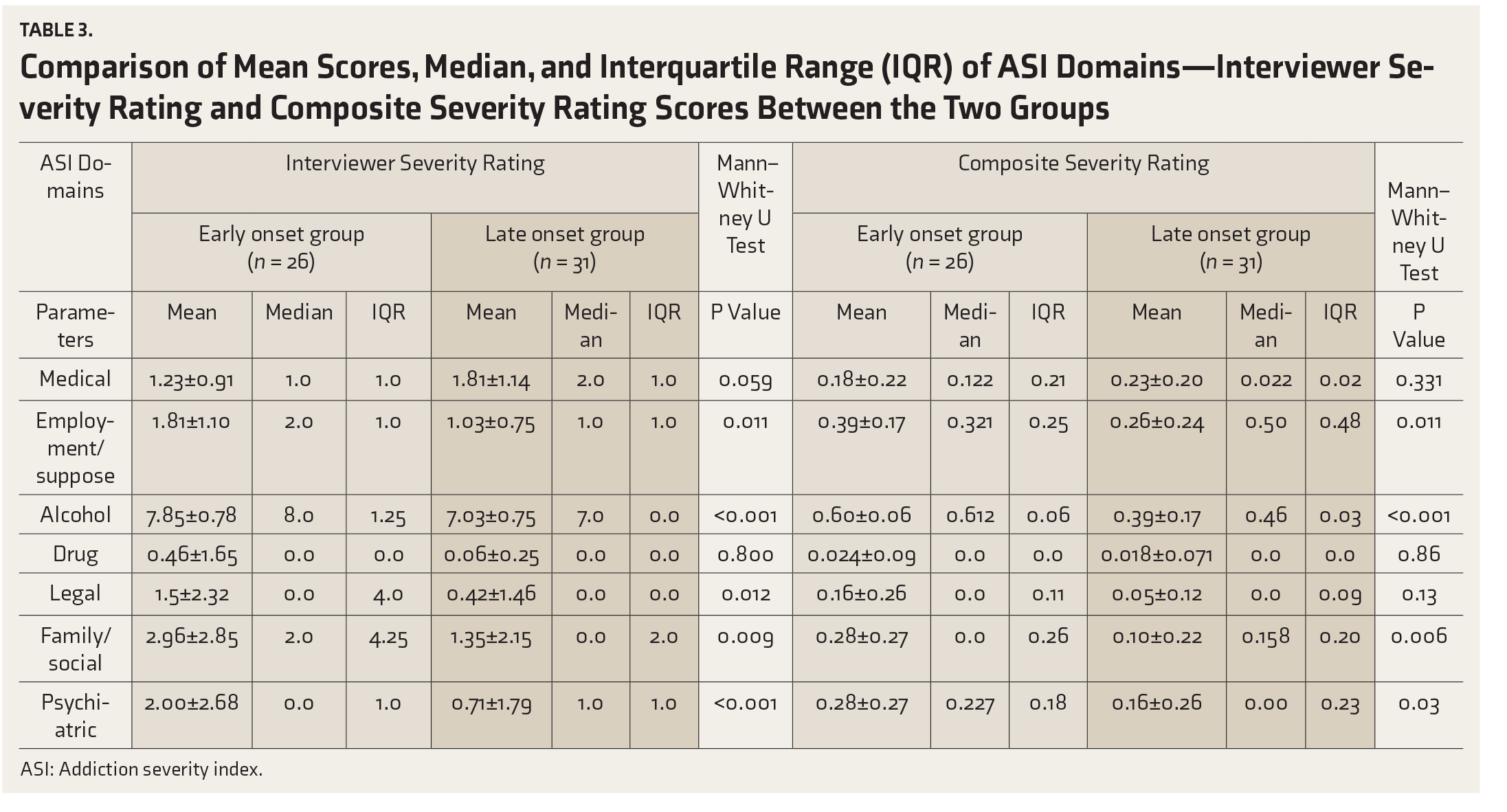
ASI: Addiction severity index.
Discussion
This was a cross-sectional, noninterventional study carried out over a period of approximately one year, in a tertiary care general hospital of North India. SSAGA-IV can be used with reliability and validity to assess the comorbidities commonly associated with alcohol use. Because of its timeline representation of diseases, it is easy to find the age of onset of alcohol dependence, which is the most crucial construct of our study.
The National Mental Health Survey 2015–2016 showed that the prevalence of AUDs is the highest (6.72%) in the age group of 40–49 years. 3 The mean age of our LO group fell in this range, while the EO group had patients with the age of onset of dependence being less than 25 years; the mean age of the EO group was lower. Previous studies also show that the mean age of EO patients was significantly lower (the mean ranging from 35 to 42.43 years) than that of the LO patients (the mean ranging from 40.1 to 47.61 years).9,13
The family history of AUDs was significantly higher in the EO group than the LO group. This has been seen in earlier studies too.9,10 Varma et al, in their study, showed that there is a family loading of alcohol use/dependence in the EO group. 9 This study also showed that it is not the use of all substances but rather only alcohol use which is high in family members of the patients, suggesting a clustering of alcohol use in families. 9 The association between the presence of family history and EO alcohol use seems to be because of having opportunities of earlier initiation of drinking. This difference can have 2 explanations: Firstly, there may be a genetic influence on the dopaminergic and serotonergic pathways, which has given rise to the concept of familial alcoholism. Secondly, it may be environmental influence because of the presence of family members around who are taking alcohol. 21 It has been already found after extensive research that those with familial alcoholism have an earlier age of onset and show more structural and functional brain abnormalities. 22
The comorbidity profile of the patients shows that both the current and the lifetime comorbidities are significantly higher in the EO group (Tables 2 and 3). Tobacco dependence was the most common comorbidity in both the groups. It is a known fact that tobacco use and alcohol use commonly coexist. They serve as the gateway to the use of more serious drugs. A number of studies indicate that cigarette smoking is a strong predictor of subsequent alcohol use. 23
After tobacco dependence, the most common comorbidity is depression in both EO and LO groups. Previous Indian studies have also shown depression to be one of the most common comorbidity in AUDs.24,25 The occurrence of depression is higher in the EO group (19.2% vs. 6.4% for the LO group) for current diagnosis as well as lifetime diagnosis (34.6% vs. 16.1%). Trajectories showing the relation of EO and LO alcohol use with depression show that EO of alcohol consumption is related to higher levels of depressive symptoms. 26 A study has shown that there is a reduction in depression in the <25 years age group, which the authors explained by the hypothesis that the group consisted of more mature individuals who have better coping skills. This possibility was supported in the study by the finding that the people who belonged to <25 years age group also had better social functioning than the EO group. 11 It is also seen that early life depressive symptoms may also give rise to EO alcohol use, thus increasing the lifetime prevalence of depressive disorders in the EO group. 27
The relationship between AUDs and depression as a comorbidity is well known. The distinction between the cause and the effect between the two entities had always been a point of interest. It has always been problematic to distinguish between the two entities of substance-induced mood disorders and independent mood disorders. Firstly, the years and age are all retrospective reports. Secondly, there are chances of missing independent psychiatric disorders if we only take into account the status of substance use rather than the duration of substance use. Thirdly, the episodes which intermingle with substance use but continue even after cessation can be missed.5 Because of the above-mentioned possibilities, SSAGA-IV was used, which is a specialized diagnostic tool that specifically takes into account the time periods and, thus, helps delineate the two disorders. The only disadvantage that remains is the retrospective recall of the age, which is inevitable.
The other comorbidity which needs discussion is antisocial/dissocial personality disorder. The prevalence in the EO group was 8%, while the LO group had no such patients. The link of EO alcohol use with antisocial personality disorder (ASPD) is a well-known entity that gets validated more. Various studies have shown the presence of antisocial traits and criminality in the EO group.11,13 This takes into account that antisocial behavior is a continuum in externalizing behaviors and is thus more prevalent in the EO group. 11 It has been discussed whether ASPD is primary or secondary to the categorization of EO alcoholism, i.e., whether a group of individuals exists with ASPD, and because of the personality construct, does EO alcoholism develop secondarily. On the other hand, antisocial traits may be a part of a total heritable constellation. 11 A longitudinal study needs to be done in this regard to get the cause–effect model.
Similarly, the lifetime rate of Oppositional Defiant Disorder in our study was 19.2%. Literature review shows a wider prevalence of all externalizing disorders in EO alcohol use. An Indian study evaluated the association of ADHD with the age of onset of AUDs. It revealed that individuals with EO AUDs have significantly higher childhood history of ADHD than those with LO AUD. 28 In our study, the LO group had higher comorbid anxiety disorder than the EO group. Anxiety disorder is more of an internalizing psychopathology. There is a need to see the presence of internalizing psychopathologies like anxiety disorder in a larger sample.
The lifetime comorbidity after combining the EO and LO groups was 84.2%. This is similar to the range of comorbidity rates, i.e., 62% to 92%, found in other Indian studies.24,25 Community samples had shown a somewhat lower rate of comorbidity. 29 It has been seen that the comorbidity rate in the clinical population is higher than that in the community samples because of Berkson’s fallacy, which states that the presence of comorbidity gives an added motivation to patients to seek treatment. 25
On comparing the severity of addiction or the extent of problematic substance use by using the ASI, it was found that the EO group had a significantly higher score (i.e., more severe problem) in the interviewer severity rating in multiple domains (employment/support status, alcohol, legal, family/social relationships, and psychiatric status). In the medical domain, the LO group had a higher score as there were more patients with medical comorbidity in the LO group (two suffered from diabetes mellitus, three from hypertension, and one from ascites). In the drug domain, two patients of the EO group had drug dependence, but no patient from the LO group did; thus, the score did not show a statistical difference. In the composite score, the EO group had a significantly higher score (i.e., more severe problem) in the domains of employment/support status, alcohol, family/social relationships, and psychiatric status (Table 3). The composite score gives a weightage to the patient’s need for treatment in that aspect. The explanation for the legal domain not reaching significance can be that the patient did not perceive the problem as severe as deemed by the interviewer. Previous studies have already shown that the severity of alcoholism and the associated psychopathology increase as the age of onset decreases. 11 A study was done where the ASI was applied in the age groups of alcoholism onset <20 years, 20–25 years, and >25 years. It was found out that the lower age group had a higher score in employment, alcohol, legal, family/social status, and psychiatric status, showing more alcohol-related problems in the EO age group. The study also showed that there is a preponderance of legal, social, family, and psychiatric problems in the <20 years onset group. The effects may also be due to the duration of illness. The prolonged illness can affect the employment status, social relationships, family relationships, and even legal status. This implies that the longer a patient has been addicted to alcohol, the more it is likely that he/she would have more psychosocial impairments. So, this observation can be due to the higher duration of illness in the EO group. 11 It has also been seen that the antisocial traits also form an essential element of the EO construct 11 and, thus, may contribute to higher legal problems.
All these findings support the concept of an endophenotype model. We can see that in our study, the EO group had a higher family history of alcohol use, more problematic alcohol use, and higher comorbidities. Ongoing research, including our study, has shown that these constructs are interrelated. Identification of the subjects who are at a higher risk of acquiring the endophenotype can help early intervention and possible approaches to mitigate AUDs as early as possible. So, finding out any of the deficits, such as a family history of alcohol use, any comorbidity (especially ASPD), or higher alcohol-related problems at any point should alert the clinicians. A thorough assessment of all other domains should be done in all such patients.
It has been seen that AUDs contribute to morbidity and disability in a huge proportion, irrespective of the age of onset. Taking alcohol and continuing using it at any level of problematic use is harmful to the individual and society as a whole. If a simple entity like “age of onset” can be applied to the clinical population to stratify risk groups, it can be highly useful. Our study shows valid evidence that the “EO versus LO” concept exists and that the EO group falls in the higher risk strata than the LO group. The comorbidity profile, which has been elaborately studied and compared for the first time in an Indian study, also supports the above assumption. It was also evident through the domain scores of ASI-5, and its use to compare the addiction profile is new in the study. Identification of patients with “EO” in a proximal phase of the trajectory can serve as a helpful measure in the prevention of further problems in the individual. Even from a perspective of public health, a systematic study of the effects of age of first alcohol use are important to be known. Prevention programs such as delaying the first use of alcohol can be an important step. A wholesome management in this viewpoint can help reduce individual suffering by mitigating social, economic, and health-related costs.
The study has limitations. The sample was drawn from individuals attending a De-addiction clinic outpatient department for treatment rather than from alcohol-dependent subjects from the community, limiting its generalizability to the general population. It also resulted in a smaller sample size. The basis for determination of the presence of ADHD/CD/Oppositional Defiant Disorder was essentially and necessarily retrospective in nature. Hence, the influence of factors such as recall bias, selective forgetting, and retrospective falsification cannot be ruled out. To minimize the effect of these factors, information put forth by the individuals was corroborated from the available informants whenever feasible. The investigator was not blind to the outcome. Hence, the possibility of ascertainment bias could not be ruled out. Subjects with serious medical comorbidities were excluded; this could explain why the EO group had a less severe profile of addiction in the medical domain.
Steps were taken to overcome some of these limitations. The onset of alcohol dependence was determined later after interpreting SSAGA-IV, and that was done after the individuals were interviewed on the later sections of SSAGA-IV that included the presence of externalizing disorders. Hence, the interviewer was not aware of the patients’ onset of alcohol dependence status during the time of assessment. This must have reduced the interviewer’s bias.
Conclusion
The study found that comorbidity is high in patients with alcohol dependence (59.6% and 84.2% in the current and lifetime frames) and is higher in the EO group. The EO group also had a higher family history and a more severe profile of substance use. So, this group forms a more vulnerable population, and special attention needs to be given to them to find out any comorbidity and to manage the severity of their problems.
Footnotes
Acknowledgments
The authors would like to thank Victor M. Hesselbrock, PhD Chairperson, Collaborative Study on the Genetics of Alcoholism (COGA) Assessment Committee, for allowing them to use Semi-Structured Assessment for the Genetics of Alcoholism IV. It has been provided by COGA, supported by NIH Grant U10AA08401 from the NIAAA. We would like to thank Dr Abhishek Ghosh, Assistant Professor, Department of Psychiatry, PGI, Chandigarh, India.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.