
Abstract
Background:
The studies and case reports from various parts of the world are showing discrimination and stigma associated with COVID-19. Stigma can directly worsen the mental health of people and also worsen physical health indirectly. This study is aimed to assess the anticipatory and experienced stigma associated with COVID-19 in affected individuals.
Methods:
This was a cross-sectional study conducted at Palakkad District in Kerala. Study participants were patients diagnosed with COVID-19. The sampling method was convenience sampling and snowball sampling. COVID-19 Related Stigma Survey Questionnaire was prepared by experts from the field of Psychiatry and Community Medicine. The responses were collected via an online survey and telephonic interview.
Results:
Among the total participants (N=303) 119 participants (39.3%) wanted to keep the illness a secret. Eighty-one participants (26.7%) had fear of discrimination from others. Eighty-nine participants (29.4%) had experienced stigma related to their COVID-19 infection. Seventy-five (24.8%) participants’ family members had experienced stigma. Few stigma parameters were significantly higher among the younger people. The participants belonging to the below poverty line category and the participants with lesser education showed significantly more worry about rejoining society after the isolation. Below poverty line category also had significantly more worry about discrimination towards their family members. Participants with lower education had significantly more worry about affecting their job due to the illness. Health care workers had significantly high worry regarding others attitudes towards them.
Conclusion:
There is a high level of stigma associated with COVID-19 in society. Definite measures need to be taken to reduce the stigma related to COVID-19 infection.
A significant level of stigma exists in society associated with COVID-19 infection. There is a need to improve awareness regarding illness and vaccines and to provide supportive measures to patients and health care workers. Definite regulatory measures need to be taken to reduce the untoward events related to COVID- 19 stigma.Key Message:
Social stigma is “an attribute which is deeply discrediting” that shrinks a person “from a whole and usual person to a tainted, discounted one.” 1 It is usually related to race, culture, gender, and health. Previous pandemic outbreaks had raised stigma. 2 COVID-19 also has a high potential to increase the stigma associated with the illness. Studies and case report from various parts of the world show discrimination and stigma associated with COVID-19,3–7 more against people from a specific ethnicity like East Asians, health care workers (HCW), persons under quarantine, and COVID-19 affected and recovered patients.
The pooled prevalence of stigma in the population was found to be 34%, according to a meta-analysis of all infectious disease epidemics including COVID-19. 3 A cross-sectional survey conducted among the general population in the USA and the UK showed that participants tended to discriminate against the people belonging to East Asia because of the fear of be infected with COVID-19. 4 That survey also identified several misconceptions on how to prevent the spread of COVID-19. Many other reports indicate racial bias and discrimination related to COVID-19. 5
HCW experienced significant stress because of increased workload during the pandemic. Stigma will increase the stress of the already overburdened HCW.6–8 One global study, which included 7411 participants from 173 countries, found that HCW experienced more bullying than others related to COVID-19. 9 One online survey conducted in the USA among the non-HCW found that more than one-third of participants avoided the HCW and more than one-fourth believed that HCW need more restrictions than others. 10 A study among 509 physicians in Egypt found that around 31% reported a severe level of stigma. 11 HCW were found to hold a significant negative self-image and concern about the public attitudes as per a study from Vietnam. 12 A study among HCW from May to July 2020 in North India found that 70% perceived and 20% experienced stigma. 13 Harassment from neighbors was the most common form of experienced stigma. There are many other case reports of discrimination against HCW from India. 14
These incidents are not limited to HCW. A study among discharged patients from New Delhi, India, found that more than 50% had self-perceived stigma, and more than 50% experienced quarantine-related stigma. 15 Another study from Kashmir, India, found that 98% of patients who had recovered from COVID-19 reported at least one stigma-endorsing response. 16 One study from South India found that around 7% of admitted patients with COVID-19 had a significantly high level of stigma. 17 Stigma was increased by the contact-tracing measures and the mandatory home isolation and quarantine. There were reports of significant stigma experienced by persons when notices were put outside their homes. Such incidents were reported against the flight crew members who helped to bring back hundreds of Indians home. Labeling and notifications of COVID-19 affected and quarantined people acted as a double-edged sword by increasing stigma toward them. 18
Stigma can lead to many deleterious effects on the health of affected persons and others. Persons tend to avoid testing and disclosing the information and may not seek treatment, fearing stigmatization and discrimination.19, 20 This can lead to increased spread and worsening of the health of affected persons without proper treatment. Stigma can also act as a risk factor for anxiety and depression of the affected individual.12, 21, 22 COVID-19-related stigma can also contribute to depression in nonaffected individuals. 23 Anticipatory stigma refers to the affected person’s fear about how society will react to them after their recovery. Experienced stigma is actual stigma/discrimination experienced by the persons. Both the anticipatory stigma and the experienced stigma are important as both impact the mental health and the quality of life of persons affected with COVID-19. 24
India’s first case of COVID-19 was reported in Kerala which had a high load of COVID-19 positive cases. Kerala’s parameters like education status of people and health-related indices are significantly better than the national level. We need to know the level of stigma associated with the COVID-19 infection in Kerala.
This study aimed to assess the anticipatory and experienced stigma associated with COVID-19 in affected individuals.
Materials and Methods
Study Design
This cross-sectional study was conducted at Palakkad district in Kerala from December 1, 2020, to June 21, 2021.
Participants
The study population was COVID-19-diagnosed patients older than 18 years of age and the residents of Kerala. Inclusion criteria were patients admitted at a COVID-19 hospital and a COVID-19 first-line treatment centre; patients discharged from the above two hospitals (within two weeks of negative results); patients under home isolation after getting negative COVID-19 results (within two weeks); and COVID-19-diagnosed patients under home isolation. They had to be able to read or understand Malayalam/English. Participants gave online consent (the consent form was incorporated in the Google form as a mandatory question to proceed to the stigma questionnaire) to participate in the study.
Sample Size
We did a pilot study on 30 patients to determine the sample size. The proportion of participants having anticipatory stigma and experienced stigma ranged from 24.5% to 28%. Considering this, as the prevalence with 20% precision and 95% confidence interval, the minimum required sample size was 296. The sampling method was convenience sampling from the list of COVID-19 positive patients. We also did snowball sampling by sending the form to known COVID-19 positive patients and their contacts in this district.
Study Questionnaire
As no validated scales were available to assess the COVID-19-related stigma, COVID-19-related stigma survey questionnaire was prepared by experts from the field of psychiatry and community medicine. It was validated (content validity and face validity) by experts with 10 years of experience in the field of psychiatry and community medicine. A few items of the questionnaire were adapted from the Berger HIV Stigma Scale, 25 which had eight questions each to assess anticipatory and experienced stigma. The responses were in the Likert scale format. The participants had to mark from “definitely yes” to “definitely no” in the anticipatory stigma part and “never” to “always” in the experienced stigma part. Examples of anticipatory stigma questions include “I am worried that people will discriminate against me,” “I am worried that people will judge me that I am sick because of my negligence,” and “I am worried that people will discriminate against my family members as well.” Examples of experienced stigma questions are as follows: “Have you ever experienced any act of discrimination from others?” “Have you ever experienced any social restrictions forced upon you by others apart from those advised by the government to stop the spread of COVID-19?” One open-ended question was included in the questionnaire to elaborate on the experienced stigma. After the pilot study, appropriate changes were made to the wordings of the questionnaire. The questionnaire was written in both English and Malayalam (and both the versions are available online as supplementary files). The link was created to a Google form that included the sociodemographic questions, consent form, and the stigma questionnaire.
Study Procedure
Institute Ethics Committee’s approval and permission from the COVID-19 hospital superintendent were obtained before starting the study. The phone numbers of the patients were collected from both institutes’ COVID-19 testing center and the daily list of positive patients at this district. Patients were contacted over the phone, and the link to the Google form was sent to their mobile numbers. All those patients who did not have WhatsApp or smartphones were contacted over the phone and interviewed telephonically. For older persons, considering the logistic issues, including lack of smartphone and expertise in using it, the survey questionnaire was applied by telephonic interview after obtaining verbal consent.
Statistical Analysis
Data were analyzed using the IBM SPSS version 20 (IBM SPSS 20. (SPSS Inc,Chicago, USA). For categorical variables, frequencies and percentages were applied. Chi-square test/Fisher’s exact test was used to look at the association between stigma and sociodemographic characteristics. An independent sample t-test was used to examine the association between age and stigma. P-value < 0.05 was considered significant.
Results
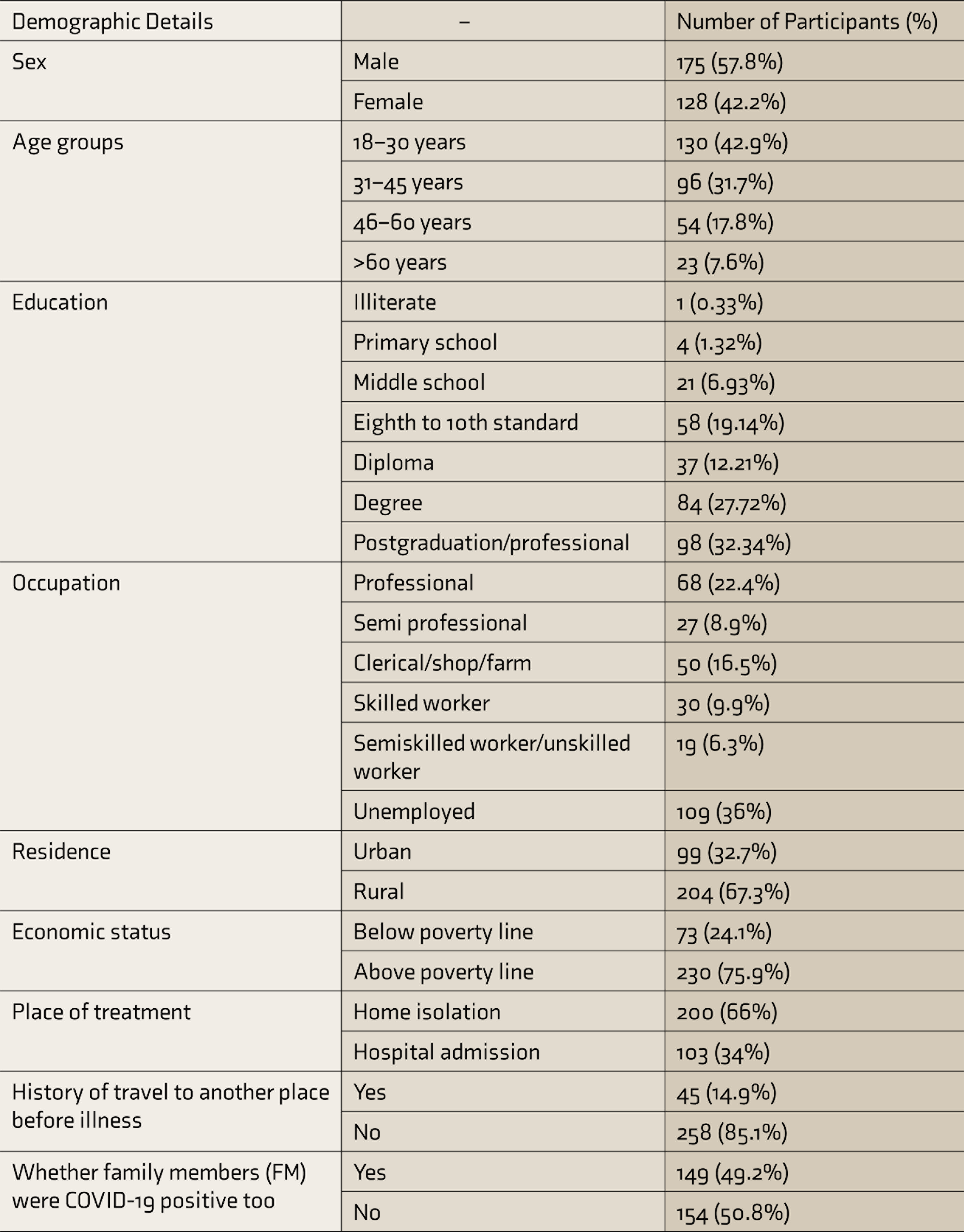
We tried to contact 1140 patients telephonically. A total of 303 participants completed the questionnaire (response rate 26.6%). The sociodemographic profile of all patients is given in Table 1. The mean (±SD) age of the participants was 36.5 (±14) years. The minimum age of the participants was 18 years, and the maximum was 81 years. Fifty-two participants were HCW. The mean number of days from the test positivity to the study was 17 ± 9 days.
Sociodemographic Profile of all Participants (N = 303)
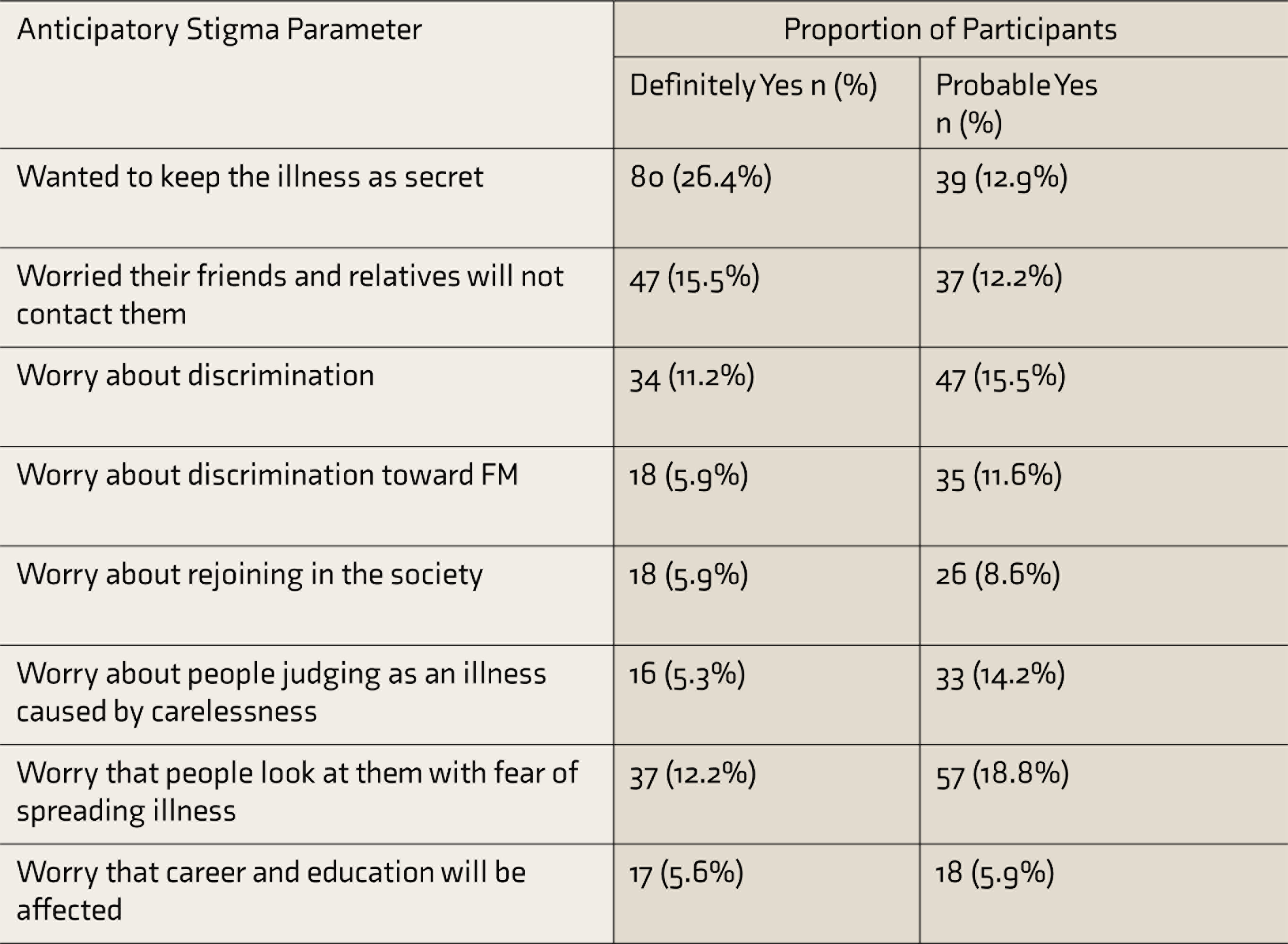
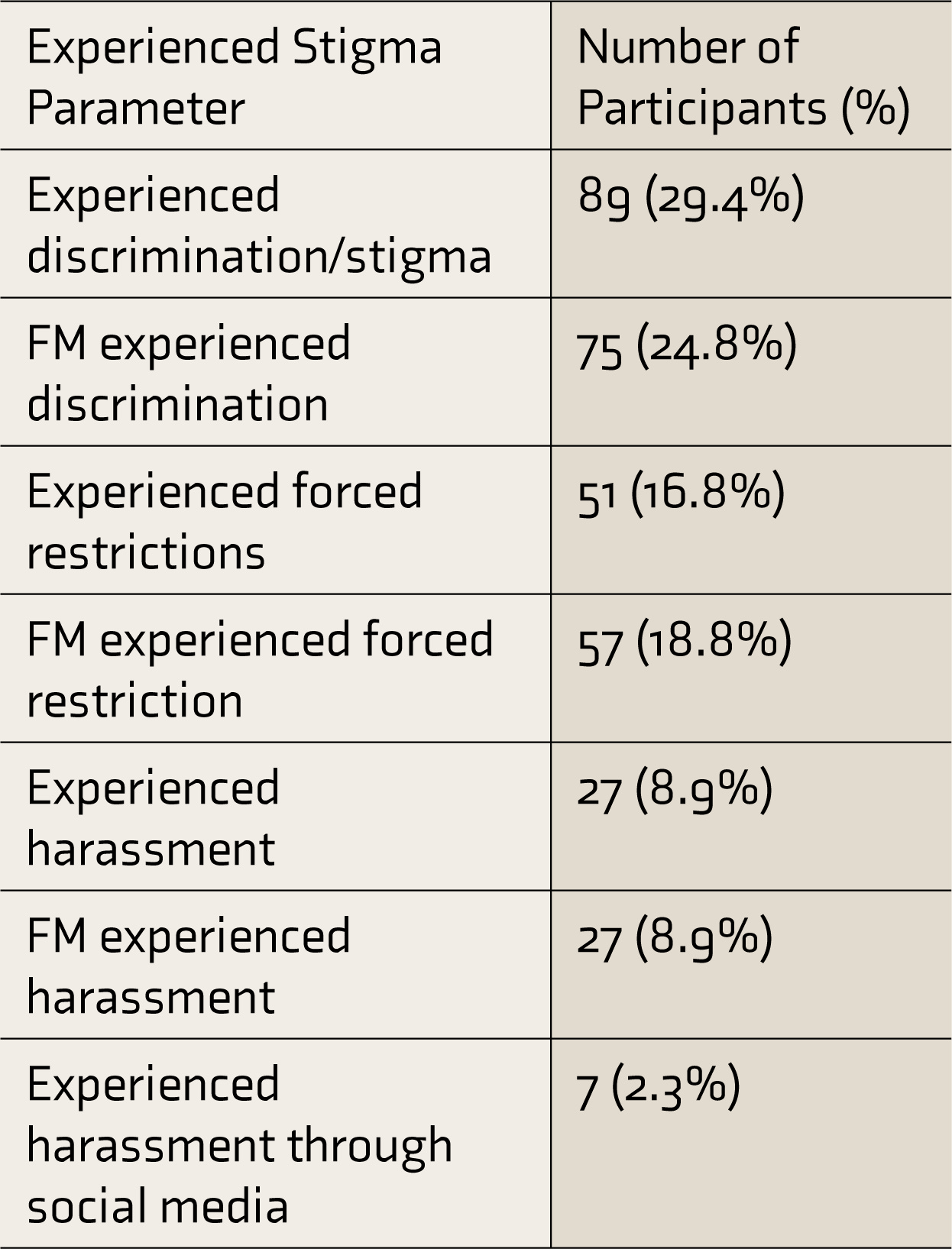
The proportions of participants having anticipatory and experienced stigma are given in Tables 2 and 3, respectively.
Proportion of Participants Having Anticipatory Stigma (N = 303)
Proportion of Participants Who Experienced Stigma (N = 303)
To look at the association of stigma with various sociodemographic factors in an exploratory manner, the neutral responses were avoided, and the responses with the same polarity were clubbed. The mean age of participants who wanted to keep the illness as the secret was significantly lesser (t = 2.76, P < 0.001) compared to others. The mean age of participants who had the fear that people will discriminate against their family members (FM) was significantly lower (t = 2.04, P = 0.04) compared to the rest of the participants. Similarly, the mean age of participants whose FM had experienced forced restriction by others was also significantly lower (t = 3.22, P < 0.001) compared to others.
Participants with education status of 10th standard or less had significantly (x= 5.68, P = 0.02) high worry about rejoining in the society after the quarantine compared to others with higher education. Less-educated participants also had significantly high (x = 5.50 P = 0.02) worry about the illness affecting their job compared to the rest of the participants. In camparison to the above poverty line patients, the below poverty line patients had significantly (x = 4.52, P = 0.03) higher fear about rejoining the society after the quarantine. They also had a significantly (x = 10.69, P < 0.001) higher fear of discrimination toward their FM. There was no significant association between stigma and factors such as sex, treatment place, urban/rural residence, history of travel, and whether FM were affected with COVID-19 or not.
Stigma parameters of HCW were compared with those of non-HCW. HCW had a significantly (x = 5.91, P = 0.02) higher worry that people would judge that their negligence caused the illness. HCW also had significantly (x = 8.67, P < 0.001) higher fear that people will look at them with the apprehension that they will spread the illness. There was no significant difference in other stigma parameters between HCW and others.
In response to the open-ended question, the participants told about the difficulties they faced from their neighbors, friends, and colleagues. The responses included allegations from others (e.g., “I was accused of knowingly going out even after being positive”). Neighbors’ attitude toward a COVID-19 positive person was also mentioned (e.g., “attitude of some of the neighbours was like if you look at a house that has positive persons, you will contract the disease”). An HCW participant reported the discrimination he faced from colleagues: “Being a COVID worker, a few of my colleagues discriminated against me even though I was not COVID positive then. It may be because of the fear of getting infected from me as I was doing COVID duty then.” Another participant also reported discrimination from close friends: “I lost my best friend after I recovered from COVID. She was afraid of me and that ruined our friendship. I was so tensed by this action.”
Discussion
Our study aimed to assess the stigma among the COVID-19-affected individuals. We found that 26.4% of patients wanted to keep the illness a secret and 29.4% faced experienced stigma in some form. Our result was similar to the studies from other parts of the world. A meta-analysis of studies of infectious disease epidemics including COVID-19 showed a stigma prevalence rate of 34%. However, the level of stigma was less compared to the other study from North India, which reported a rate of more than 50%. 15 Reasons could be the different periods of study. That study was conducted between May 15, 2020, and June 30, 2020. Our study was conducted from December 2020 to June 2021. Studies have shown that stigma tends to reduce over time.16, 26 Some of the other reasons could be the availability of more clear information about the illness, the advent of vaccinations against COVID-19, and the sociocultural differences. Clear information about the illness can reduce the stigma associated with the disease. 27 In India, vaccination started January 2021 onward.
Anticipatory stigma will prevent persons from testing, getting treatment, and disclosing the information to others. 28 The disclosure decision is an important matter of concern for the COVID-19-affected persons. 26 The decision to disclose the information is closely related to the fear of discrimination and being blamed by others. 29 Of our participants, 39.3% wished to keep the information a secret. This indicates the patients were concerned about others’ attitudes toward them and their response to the illness status.
The proportion of our participants having experienced stigma was more than that of participants having anticipatory stigma. Similarly, the proportion of participants who faced discrimination toward the FM was more than the proportion of participants with anticipated fear of discrimination toward the FM. This shows that stigma could affect people even more than they expect, exacerbating their stress related to the illness. Even though there are many reports from around the world regarding social media and online harassment, 30 harassment via social media was found to have the least proportion (2.3%) among all stigma parameters in our study.
HCW had significantly higher anticipatory stigma than others in some parameters, as found in a previous study from Vietnam. 12 They had a significantly higher worry that people would judge that their carelessness caused the illness and that people would look at them with the fear that they would spread the illness. This kind of apprehension regarding the public’s attitude toward them has also been found in another study from Egypt. 11 A high level of stigma among the HCW can lead to stress, poor job satisfaction, and absenteeism from the job; and thus, cause burnout. 31
In our study, the people who wanted to keep the illness information a secret, people with the fear of discrimination toward their FM, and people whose FM experienced forced restriction were significantly younger. This may be because the younger population are more frequently going out to society and more involved in the social situations related to their work and education compared to the older population. This result differed from one study of North India, which found the highest stigma among the 46 to 60 years age group, while other studies reported no significant association of stigma with age.15, 32, 33 But a study conducted among the general population had found more stigma among the younger persons. 34
Patients belonging to the below poverty line category had significantly higher worry about rejoining society after the isolation period than the above poverty line group. They also had significantly more worry about discrimination toward their FM. The results are similar to a previous study from North India, which found that the people living in slums, daily wagers, laborers, and vendors had higher stigma than others. 15 People with higher financial loss were found to have a higher stigma, according to a study from China. 35 Lesser educated patients had significantly more worry that the illness would affect their job/career. They also had higher anxiety regarding rejoining the society. It was in line with a study from Indonesia that reported higher stigma among the less educated people. 34 However, this was different from another study from North India, which did not find any association between stigma and educational status. 15 A study from Saudi Arabia also did not find any association between stigma and the educational or social status. 32 Illness and the isolation period lead to significant difficulty for the daily-wage workgroup and the self-employed group to make an earning. COVID-19-affected self-employed people were found to have a high stigma in a previous study from India. 15
We did not find any association of stigma with sex, treatment place (whether admitted in hospital or under home isolation), residence (urban or rural), history of travel to a different place (before being diagnosed to have COVID-19), and whether other FM affected with COVID-19, unlike a few other studies.16, 35
One of the limitations of this study includes the cross-sectional design. So the causal relationship between stigma and sociodemographic variables cannot be ascertained. Results can be generalizable to Kerala but may not be generalizable to other parts of India because of sociocultural differences. A face-to-face interview was not done considering the logistic issues of COVID-19 positive status and as we included both admitted and home care patients. Low response rate, which was probably because of the severity of COVID-19, ICU admissions, the necessity of mechanical ventilators, and the death of many patients, and the inability to contact many patients has also affected the results. Convenience and snowball sampling may have resulted in self-selection bias, where persons who felt more stigmatized chose to participate in the study.
More studies need to be conducted with larger sample sizes. Qualitative studies to understand stigma in-depth, longitudinal studies, and studies on interventions to reduce the stigma are needed too.
Conclusion
A significant level of stigma exists among the COVID-19-affected individuals. Persons with lower educational levels and persons belonging to the below poverty line category have more anticipatory stigma. HCW have significantly higher anticipatory stigma. Adequate psychological support should be provided to the COVID-19-affected persons and the HCW. Proper steps must be taken from the individual household level to the national level to reduce the stigma associated with COVID-19. Successful strategies learned from other infectious diseases can also be applied to COVID-19. Regulatory measures need to be taken against all the untoward events related to COVID-19 stigma.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We acknowledge the help received from our interns during the data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.