
Abstract
Background:
The onset of severe mental disorders (SMDs) is during adolescence or young adulthood, which affects the well-being and the educational aspirations of the students. Models of supported education practiced in the West are not culturally suitable for Indian students or the Indian education system. This study aimed to develop a Supported Education Program (SEP) for students with SMDs to help them with academic reintegration in an Indian context.
Methods and Material:
To develop the SEP, a realist review was done, followed by an in-depth interview with eight mental health professionals (MHP) and nine lecturers, using a validated interview script. After each interview, interim analysis and modifications were done to improve the rigor of the interview. After all interviews, the SEP was circulated for a second round of iteration for consensual validation by four mental health experts. The outcome of the entire process was the final version of SEP for students with SMDs.
Results:
The final SEP had two broad themes and 18 subthemes from the qualitative thematic analysis: theme 1 included issues and strategies relevant to the client or caregivers, and theme 2 was pertinent to the education system.
Conclusion:
The SEP developed and validated for people with SMDs has distinctive components: one for the individual and caregiver and the other for the educational system.
A culturally relevant Supported Education Program (SEP) is needed for individual students with SMDs in India. The SEP developed under this study is based on both a realist review and in-depth interviewing of mental health professionals (MHPs) and lecturers. The SEP encompasses two distinctive themes: one for individual students and caregivers, and the other for the educational system. The current SEP offers a comprehensive plan for the academic reintegration of students with SMDs in an Indian context.Key Messages:
The onset of Severe Mental Disorders (SMDs) is during late adolescence or young adulthood, making it difficult for students to complete their postsecondary education. Psychiatric illness affects not only the well-being of students but also the educational aspirations of students with SMDs. 1 SMDs limit the socio-occupational functioning, academic performance, and adjustment of the individuals. 2 Hence, most students with SMDs desire to complete their academic goals so that they can achieve the career of their choice. 3
The occurrence of psychiatric illness among postsecondary education students is steadily increasing and resulting in disability associated with the illness.4,5 One in four young adults having a psychiatric disability are students who experience difficulties in their educational attainment during their symptomatic phase and sometimes, even postrecovery. 6 This makes it challenging for the students to complete their educational aspirations without need-based supported education interventions.
Students with psychiatric illness face a different kind of barriers to academic attainment, such as dishonor, 7 poor understanding, 8 poor support from caregivers and peers, 9 limited traveling services, 10 problems in handling psychopathology and side effects of medications, 11 poor reasonable accommodations, 12 fear of disclosing about illness, 13 poor supported academic services, 14 poor self believe and self-respect, 15 cognitive problems, 16 previous academic failures, 17 , previous negative educational experiences, 3 financial burden, 16 , poor legislations, 18 poor attendance, and negative symptoms. 3 The above barriers to academic attainment bring out the need for developing a Supported Education Program (SEP) for students with SMDs.
As part of developing specialized services in this area, the authors examined various models on supported education that are practiced in the USA,19-22 Canada,23-25 and Australia.12,26,27 These services were not compatible with the Indian education system because they offer bridge courses, vocational skills training programs, combined SEP, supported employment programs, and cognitive remedies. Only two studies have been conducted in India in SEP: the first was a descriptive study that looked at educational difficulties, which were eight times more common among youth with schizophrenia than other psychiatric disorders. The study also detailed how these students who continued education (53.6%) faced problems, including concentration difficulties, a decline in academic performance, and breaks in schooling. 6 The second study developed a tool to assess hindering and helping factors for academic reintegration. 28 Both studies mentioned the need for the development of culture-specific SEP models for helping Indian students with SMDs. In continuation of the results of the above two studies, this study aimed to develop a culturally sensitive SEP for students with SMDs to help them in academic reintegration.
Methods and Material
This study was reviewed and approved by the Institute’s Ethics Committee. It was also registered in the Clinical Trials Registry India (CTRI): CTRI/2018/07/014828. A three-step process was followed to develop the SEP, namely (I) conducting a realist review, and (II) conducting qualitative in-depth interviews with mental health professionals (MHPs) and lecturers, and (III) validation of SEP by experts. This study used explorative design, and it was conducted from July to September 2018 in Bengaluru, India
Step I: Realist Review
The realist review was conducted through six steps advocated by RAMESES (Realist and Meta-narrative Evidence Syntheses: Evolving Standards) publication standards and guidelines 29 : (a) identifying the review questions; (b) formulate the initial program theory; (c) searching for primary studies; (d) selecting the studies and appraising their quality; (e) extracting, analyzing, and synthesizing relevant data; and (f) refining the program theory.
Step II: Qualitative In-Depth Interviews
To conduct the in-depth interviews, the researcher prepared an interview script (supplement document) based on the review of the literature, inputs from research guides, and practical experience. The interview script was evaluated by four MHPs (two psychiatric social workers, one clinical psychologist, and one psychiatrist). They examined each question to check whether they appear to be measuring the academic reintegration issues and represent all the domains of academic reintegration, and the interview script was accordingly modified. This process was to establish the face and content validity of the interview script.
A total of 17 qualitative in-depth interviews were conducted with MHPs (n = 8) and lecturers (n = 9), selected as per the study’s inclusion criteria, from July to September 2018. Purposive sampling technique was used. Lecturers involved in teaching students at the intermediate (11th and 12th standard) and graduate levels across disciplines (arts, science, medicine, commerce, engineering, education) were approached for the interview. Care was taken to approach only those lecturers who had some experience with clients with SMDs, i.e., who have observed abnormal behavior (possible symptoms of mental illness) in their students, referred students for psychiatric consultation, arranged for meeting with parents or administration for this problem, or provided some kind of relaxation in classroom setting/assignments. On interviewing, the selected lecturers did show some knowledge about the basic symptoms that students with SMDs would show as observed in the classroom. However, as the level of knowledge varied amongst the lecturers, the researcher took the initiative to educate them about SMDs in the beginning of the interview. MHPs in and around Bengaluru and those representing different mental health professions such as social work, psychiatric nursing, psychiatry, and psychology were selected.
The qualitative in-depth interviews were audiorecorded, transcribed into process recording, and coded, and themes and subthemes were derived manually for developing the SEP. The themes and subthemes were derived and collated together, independently by three MHPs (two psychiatric social workers: second and fourth authors) and one clinical psychologist (third author).
After each interview, an interim analysis was conducted to better the rigor of developing the SEP, i.e., the number of iterations the program went through in the development (n = 2). After each interview, the program was modified, and after all the experts provided their opinion, the program was circulated amongst the experts for the second round of iteration. The themes and subthemes were considered to have reached a saturation point when two consecutive interviews with experts did not elicit new themes.
The qualitative data collected from the in-depth interviews (step II) were manually analyzed following a six-step approach to thematic analysis proposed by Braun and Clarke. They included (a) familiarity with recorded data by reading and re-reading of transcripts and making important notes on the data while listening to the transcripts, (b) generating initial codes by open semantic codes and refining them through discussion, (c) searching for the themes in reference to the codes to develop SEP components, (d) reviewing the themes to collapse or cluster them based on unifying features, (e) defining and naming themes in relation to the research question and in keeping with the essence of the data collected from the experts, and (f) development of SEP, which resulted in two components (i) interventions with clients and caregivers, and (ii) intervention in academic colleges or institutions. 30 The thematic analysis was carried out mainly by the first and second authors. The third author was involved in deciding if there were any contentious differences in thematic analysis between the first two authors.
Step III: Validation of SEP
The themes elicited from the interviews conducted with MHPs and lecturers were collated, which included generating new themes and deleting repeated themes for finalizing the SEP components. The researcher utilized a Delphi method 31 for consensus building among the experts to validate the SEP. The practical importance of the Delphi method was in the rigor with which the program was developed, i.e., the number of iterations the program went through in the development. The method involved two rounds of iteration amongst all the experts where after each interview, the program was modified. After all the experts provided their opinion, the program was modified for the second round of iteration amongst the experts. During the iteration process, anonymity was maintained about the comments and names of the experts. Post the first round of iteration, there was a 70% agreement among the experts; hence, a second round of iteration was conducted with all the experts, post which there was complete agreement on the components of the SEP among all the experts.
The finalized SEP was circulated via email to all the experts for their final opinion and consensus building. Every comment was given equal importance. There were very few comments to shift themes and subthemes from one heading to another; overall, all the experts were at a consensus for the contents of the developed SEP. This helped in completing the content and consensual validity of the SEP. The outcome of the entire process was the final validated SEP for students with SMDs (Table S1, the detailed final SEP manual is available with authors on request). The experts also pointed out several practical challenges that may be experienced in delivering the SEP (Table 1).
Results
Relevant sociodemographic details of the experts who helped develop and validate the SEP are as follows: the mean (SD) age of MHPs was 52.6 (12.6) years, 62% of MHPs have Ph.D. in respective fields, and the mean year of clinical experience was 16.8 (SD 13.6). Approximately 62% of MHPs were men working in government sectors. The mean age (SD) of lecturers was 50.4 (SD 11) years, 44% of lecturers have a Ph.D. in their respective fields, and the same percentage of lecturers have postgraduation. Approximately 55% of the lecturers were men and 77% of lecturers worked in the private sector.
Realist Review
The realist review brought out 23 studies on supported education interventions that had been conducted in various countries, including the USA (n = 14), Canada (n = 6), and Australia (n = 3). The majority of the studies aimed to develop and test the effectiveness and feasibility of supported education services. The studies were explorative and augmented cognitive remediation with supported employment principles or utilized bridge SEPs. Studies used either a single group experimental or randomized control trial design. Sample sizes varied from 16 to 404, with the participants in the age range of 15–75 years. The majority of the participants were from urban backgrounds and had good social and economic support with basic educational qualification. The SEPs were longitudinal in nature, ranging from 6 weeks to 4 years in duration. All the SEP were comprehensive and focused on the psychological, social, employment, academic, and environmental aspects of participants with SMD. They were provided in medical and educational settings (college/classroom, hospital-based, occupational therapy, rehabilitation centers, community, clubhouses) by diverse professionals (e.g., occupational therapists, social workers, psychologists, certified teachers, the staff of the community colleges, agencies and community health centers, instructors, volunteers, general practitioners, and psychiatrists). To measure the effectiveness, most studies used both qualitative and quantitative assessments to measure the change/significance before and after the SEP. The study outcomes included increased enrolment in education/college, employment, or work; completion of the courses; improved self-esteem; cognitive functioning; self-efficacy; confidence; interpersonal relationships; coping; problems solving ability; community living and participation; mental health literacy; social support; social functioning; assertiveness; skills like study skills, social skills, and technical skills; college attendance; and development of personal independence. Most of the studies reported that with SEP, psychological distress, hospitalization rates, and stigma were reduced.
Several contexts–mechanism–outcome configurations were generated from the realist review to help develop the SEP. For instance, the realist review derived contexts like psychosocial support, reasonable accommodations, advocacy, networking, and coordination; multidisciplinary teams in supported education research had an opportunity to use mechanisms of integrating supported employment with supported education; bridge programs as a supported education service for higher or long-term course; augmenting cognitive remediation with supported education; mental health-related interventions in supported education programs; psychosocial interventions/support for stakeholders; collaboration among education, health, and work/employment; a combination of classroom teaching or instructions and a practical internship with and without mainstream education; recruiting or facilitating of occupational therapists, instructors and mentors for onsite one-to-one close supervision, guidance, feedback, and handholding; workshop, case-based and group-based interventions; and availability of research funding to SEPs. The above-mentioned context and mechanisms in supported education studies generated various outcomes such as academic reintegration, recovery from psychiatric illness, vocational skill training, behavioral changes, and social interactions.
Practical Difficulties in Applying Supported Education Program (SEP) as Reported by Experts (Lecturers and MHP)
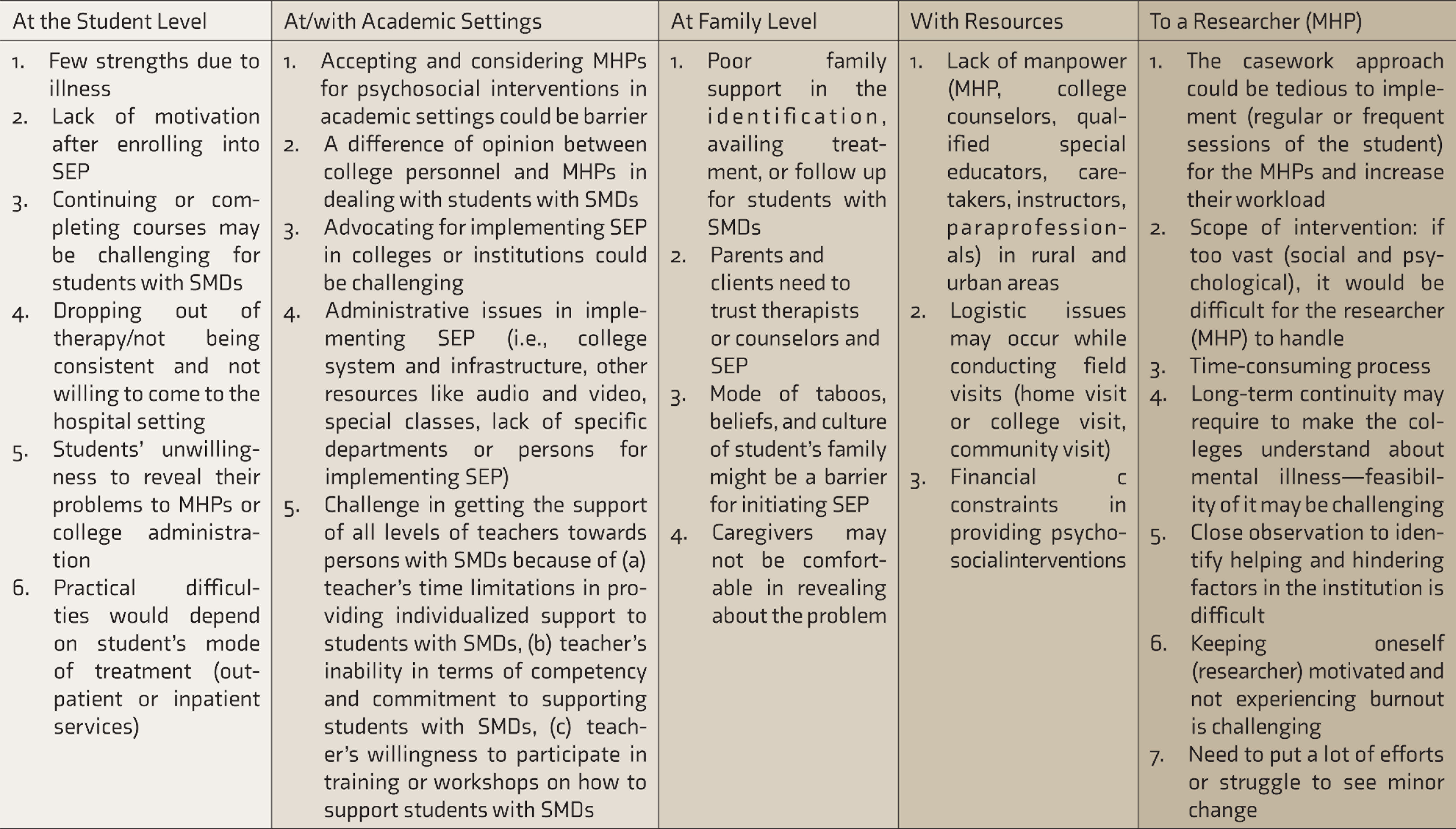
DMHP: District Mental Health Program, MHP: mental health professionals, SEP: Supported Education Program, SMD: severe mental disorders.
Final SEP
A total of two broad themes and 18 subthemes (components) emerged from the qualitative thematic analysis. The content of the sessions and quotes of the experts are described in Table S1. The themes and subthemes are listed below:
Theme 1: SEP with students and caregivers: Under this theme, the experts believed that the researcher/therapist could initiate interventions specified below, based on the need of the clients and their caregiver. A total of 13 subthemes (components of SEP) emerged that could help the students with SMDs for their academic reintegration: (a) psychoeducation about illness and its impact on academics (with client and parents), (b) motivation enhancement (with the client), (c) working on strengths and barriers (with client and family), (d) creating awareness about social welfare benefits/resources and rights (client and parents), (e) career counseling (with the client), (f) group work (with the client), (g) psychological interventions (with the client), (h) referral services (for the client), (i) family interventions (with family/caregivers), (j) liaising and coordinating with the multidisciplinary team and networking other stakeholders, (k) lifestyle modification (with the client), (l) visiting home and academic college/institutes, and (m) follow-up services. Theme II: SEP in academic colleges or institutions settings: Under this theme, the experts believed that researchers/therapists could initiate interventions based on the need at the institution level. This theme had five subthemes that could help the students with SMDs in academic reintegration: (a) working with management and the competent authority in academic settings (institutions/colleges), (b) change in the course curriculum, (c) working with lectures/faculty and college counselors, (d) working with peer groups in a college setting or environment, and (e) working with parents in a college setting.
Discussion
The SEP is an important intervention under the ambit of psychosocial rehabilitation for clients with SMDs. 32 The concept of reintegrating adults with SMDs into academics is often not considered by the family members and communities in India, due to their gap in education, stigma, and the need to earn a living instead of continuing education. 6 As education and vocation have a symbiotic relationship, families in India often try to support their children to complete their higher education so as to enable them to have economic security and more opportunities in the job market.33-36
The SEP developed is useful and applicable for multiple stakeholders: (a) for the individual with disability where the program helps him/her reintegrate into academics, (b) for the family members as it helps them understand the client’s aspirations and support him/her in pursuing his/her mainstream education, and (c) for the community as it can be utilized as a public health model where students trained in SEP can be the providers of SEP at their community level in liaison with the public health system (e.g., District Mental Health Program). The need for this synergy of stakeholders is important, especially in a country like India, where the family members and the education institutions play an active role in helping the client with disability to reintegrate and complete his/her mainstream education. Thus, the current SEP developed is culturally appropriate in keeping with the fabric of the Indian education system. The cultural differences in the education system and the differences in the stakeholders’ participation in the education of a client were a major reason why a Western model of SEP could not be adapted to the Indian context, and it warranted the development of a new SEP as in this study.
The recent legislation and policies by the Government of India, such as the Rights of Persons with Disabilities Act 2016 37 and the National Education Policy 2020, 38 advocate for an SEP model of education for persons with disabilities. The Act provides for reservations in higher education, inclusive education and equal opportunity, and reasonable accommodation in writing exams. It makes the educational institution responsible for providing disabled-friendly infrastructure and measures to help clients with SMDs reintegrate into academics. 37
The National Education Policy has also come up with different models of education for clients with disabilities, including SMDs, such as open schooling, distance education, skill-based education, and educational apps with online tutorials to help them complete their education. The essence of the Act and policy are embedded in the components of the SEP developed in this study. Furthermore, components of the SEP such as psychoeducation about the illness and welfare benefits, career counseling, neuropsychological interventions, family interventions, liaising and coordination, lifestyle modification, home and college visits, follow-up services, adapting need-based curriculum, and working with peer group, as brought out in the qualitative thematic analysis have been observed in earlier studies to be important for academic reintegration.12,20,23,24,26,39-44
The strengths of this SEP are that it has involved all stakeholders such as mental health professionals, lecturers, peer groups, and family members who are assisting in the care of the students with SMDs. Consequently, it has also helped develop an indigenous comprehensive SEP for students with SMDs in an Indian context. This program provides appropriate support during all stages of academic reintegration and beyond.
A few limitations of this study were the inclusion of only students with SMDs who were studying in mainstream education, the small sample size due to the intensive case work method adopted, and limited knowledge experience of dealing with students with SMDs among lecturers who were interviewed. Furthermore, due to a limited number of trained MHPs (NMHS, 2015–2016) in India, a multidisciplinary team approach to the provision of SEP may be feasible only in tertiary care settings situated in urban areas. Future studies can examine the feasibility of SEP across various clinical and nonclinical settings.
The SEP has far-reaching implications and can be implemented in various mental health institutions and rehabilitation and academic settings for the academic reintegration of students with SMDs. SEP as a community program can be taken up at the district level by the DMHP; psychiatric social workers and postgraduation level (Master of Social Work, Psychology) students can be trained to provide the SEP at their college/university level in their district. Furthermore, this study can act as a steppingstone for future research on SEP for other populations apart from SMDs (such as mild intellectual or developmental disabilities) and other age groups of persons with mental illness, such as children and adolescents.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.